

Abstract
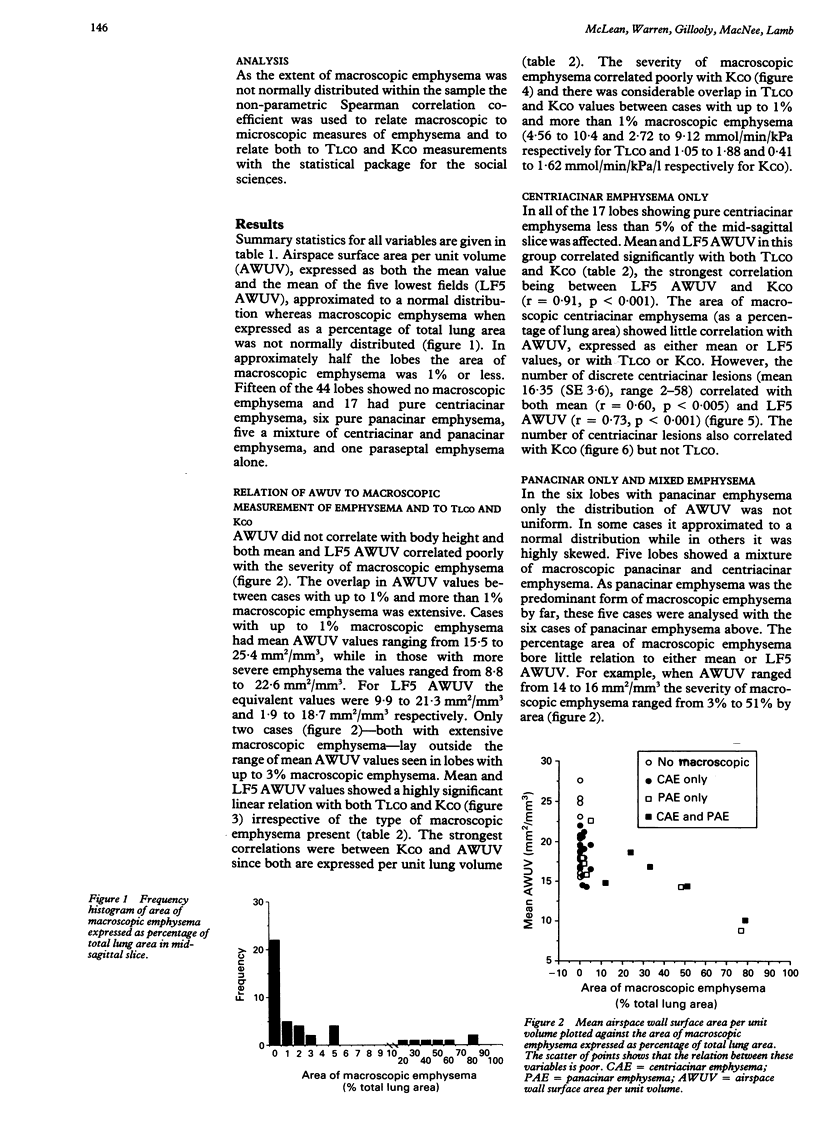
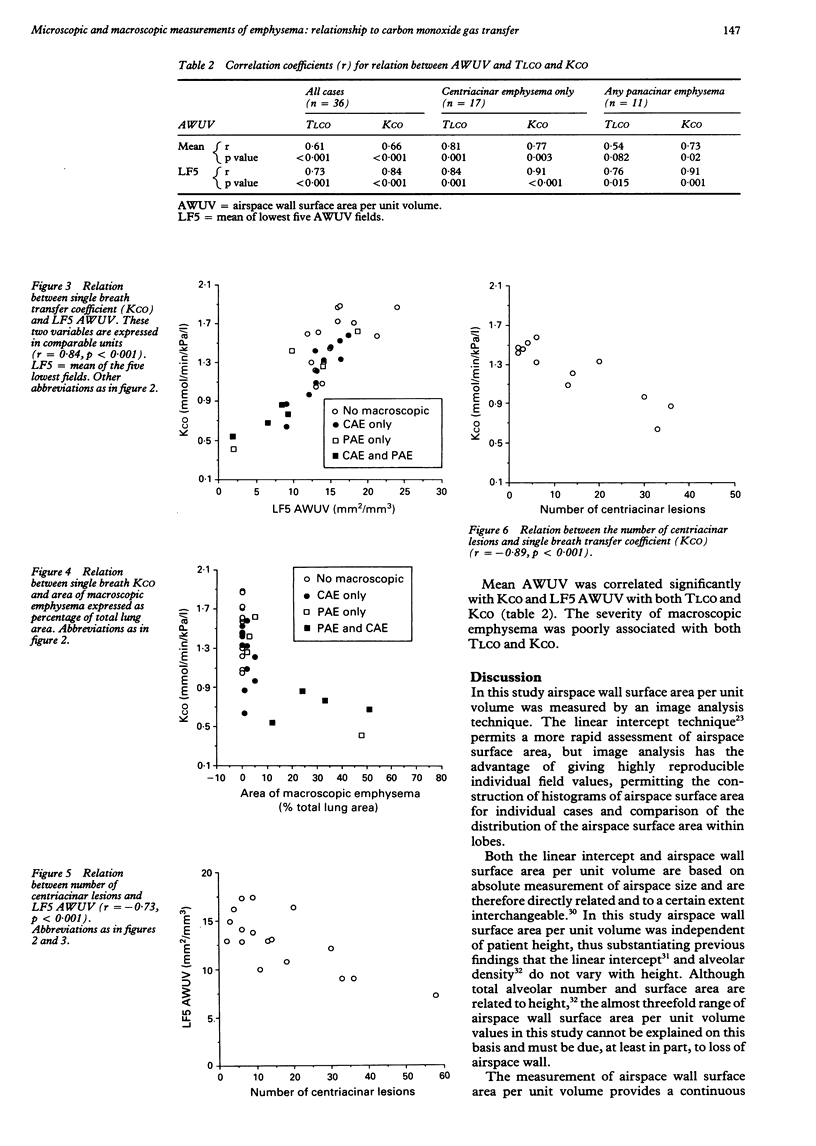
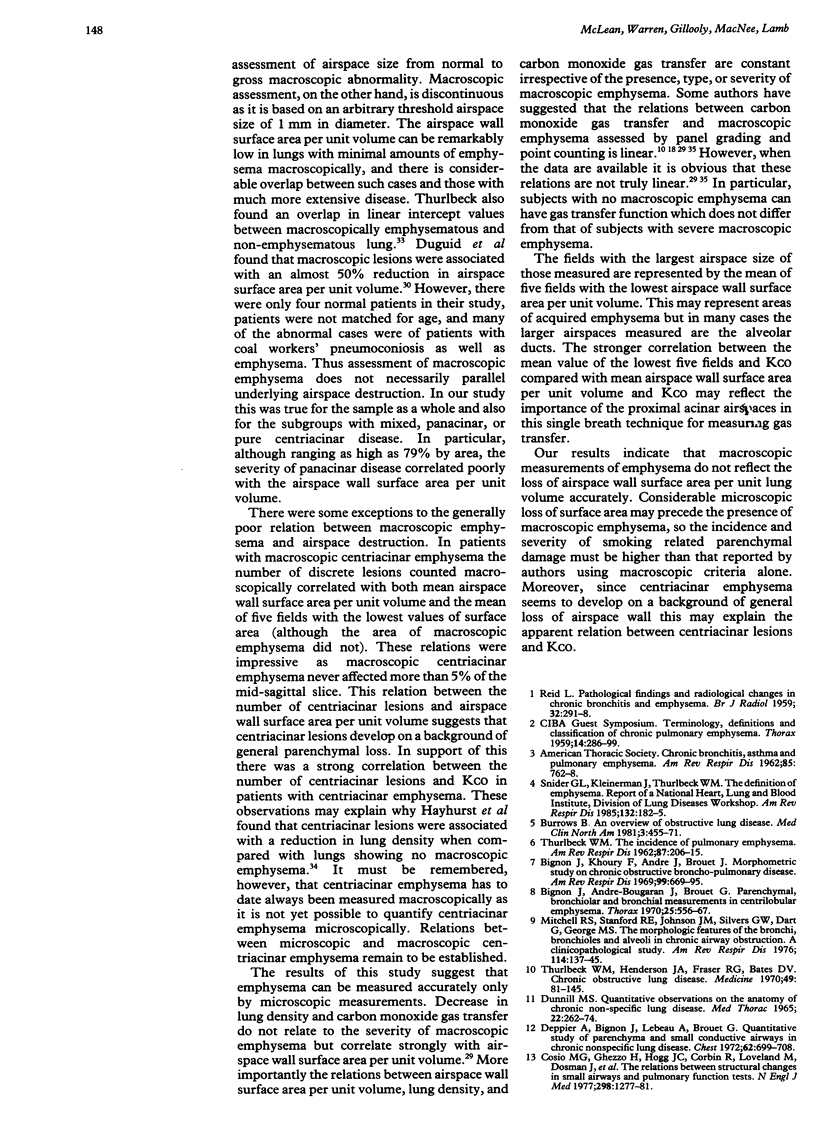
BACKGROUND: Studies of the relation between the severity of structural change in emphysema and physiological abnormality have been based on macroscopic assessments, which have not been truly quantitative or sensitive enough to detect early changes. With a highly reproducible method for measuring emphysema using histological sections and a semiautomatic image analysis system, this quantitative assessment of emphysema was compared with a semiquantitative macroscopic assessment of emphysema and measurements of carbon monoxide gas transfer. METHODS: Microscopic and macroscopic measurements of emphysema on 44 thoracotomy specimens were compared; only two were from non-smokers. Airspace wall surface area per unit volume was measured microscopically with an automatic image analyser and expressed as both the mean airspace wall surface area per unit volume and the mean value of the five fields with the lowest values. Macroscopic emphysema was measured directly on a tracing of the midsagittal slice using a digitising tablet attached to a microcomputer and expressed as a percentage of the total area of lung. In cases with centriacinar emphysema the number of discrete lesions was counted. RESULTS: The area of macroscopic emphysema ranged from 0 to 78% of the total area of lung examined, but most patients had less than 1% involvement so that the distribution was highly skewed. Both mean airspace wall surface area per unit volume and the mean of five fields with the lowest airspace wall surface area per unit volume were normally distributed, with mean airspace areas ranging from 8.8 to 25.4 mm2/mm3 (mean 18.1 mm2/mm3). In lobes with centriacinar emphysema the number of discrete lesions correlated with airspace wall surface area per unit volume and with preoperative carbon monoxide transfer factor (TLCO) per unit lung volume. However, other measurements of macroscopic emphysema did not correlate with loss of alveolar wall surface area, and there was considerable overlap between subjects with no or minimal macroscopic emphysema and those with more severe disease. TLCO correlated with both mean airspace wall surface area per unit volume and the mean of five fields with the lowest airspace wall surface area per unit volume but not with the severity of macroscopic emphysema. CONCLUSION: If emphysema is to be quantified it must be measured microscopically; macroscopic measurements do not, in general, reflect the microscopic loss of airspace wall.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Angus G. E., Thurlbeck W. M. Number of alveoli in the human lung. J Appl Physiol. 1972 Apr;32(4):483–485. doi: 10.1152/jappl.1972.32.4.483. [DOI] [PubMed] [Google Scholar]
- BLAKEMORE W. S., FORSTER R. E., MORTON J. W., OGILVIE C. M. A standardized breath holding technique for the clinical measurement of the diffusing capacity of the lung for carbon monoxide. J Clin Invest. 1957 Jan;36(1 Pt 1):1–17. doi: 10.1172/JCI103402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berend N., Woolcock A. J., Marlin G. E. Correlation between the function and structure of the lung in smokers. Am Rev Respir Dis. 1979 May;119(5):695–705. doi: 10.1164/arrd.1979.119.5.695. [DOI] [PubMed] [Google Scholar]
- Bergin C., Müller N., Nichols D. M., Lillington G., Hogg J. C., Mullen B., Grymaloski M. R., Osborne S., Paré P. D. The diagnosis of emphysema. A computed tomographic-pathologic correlation. Am Rev Respir Dis. 1986 Apr;133(4):541–546. doi: 10.1164/arrd.1986.133.4.541. [DOI] [PubMed] [Google Scholar]
- Bignon J., Andre-Bougaran J., Brouet G. Parenchymal, bronchiolar, and bronchial measurements in centrilobular emphysema. Relation to weight of right ventricle. Thorax. 1970 Sep;25(5):556–567. doi: 10.1136/thx.25.5.556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bignon J., Khoury F., Even P., Andre J., Brouet G. Morphometric study in chronic obstructive bronchopulmonary disease. Pathologic, clinical, and physiologic correlations. Am Rev Respir Dis. 1969 May;99(5):669–695. doi: 10.1164/arrd.1969.99.5.669. [DOI] [PubMed] [Google Scholar]
- Burrows B. An overview of obstructive lung diseases. Med Clin North Am. 1981 May;65(3):455–471. doi: 10.1016/s0025-7125(16)31509-7. [DOI] [PubMed] [Google Scholar]
- CAMPBELL H., TOMKEIEFF S. I. Calculation of the internal surface of a lung. Nature. 1952 Jul 19;170(4316):116–117. [PubMed] [Google Scholar]
- Cosio M. G., Hale K. A., Niewoehner D. E. Morphologic and morphometric effects of prolonged cigarette smoking on the small airways. Am Rev Respir Dis. 1980 Aug;122(2):265–221. doi: 10.1164/arrd.1980.122.2.265. [DOI] [PubMed] [Google Scholar]
- Cosio M., Ghezzo H., Hogg J. C., Corbin R., Loveland M., Dosman J., Macklem P. T. The relations between structural changes in small airways and pulmonary-function tests. N Engl J Med. 1978 Jun 8;298(23):1277–1281. doi: 10.1056/NEJM197806082982303. [DOI] [PubMed] [Google Scholar]
- DUGUID J. B., YOUNG A., CAUNA D., LAMBERT M. W. THE INTERNAL SURFACE AREA OF THE LUNG IN EMPHYSEMA. J Pathol Bacteriol. 1964 Oct;88:405–421. doi: 10.1002/path.1700880204. [DOI] [PubMed] [Google Scholar]
- Depierre A., Bignon J., Lebeau A., Brouet G. Quantitative study of parenchyma and small conductive airways in chronic nonspecific lung disease. Use of histologic stereology and bronchial casts. Chest. 1972 Dec;62(6):699–708. doi: 10.1378/chest.62.6.699. [DOI] [PubMed] [Google Scholar]
- Gould G. A., MacNee W., McLean A., Warren P. M., Redpath A., Best J. J., Lamb D., Flenley D. C. CT measurements of lung density in life can quantitate distal airspace enlargement--an essential defining feature of human emphysema. Am Rev Respir Dis. 1988 Feb;137(2):380–392. doi: 10.1164/ajrccm/137.2.380. [DOI] [PubMed] [Google Scholar]
- Greaves I. A., Colebatch H. J. Observations on the pathogenesis of chronic airflow obstruction in smokers: implications for the detection of "early" lung disease. Thorax. 1986 Feb;41(2):81–87. doi: 10.1136/thx.41.2.81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayhurst M. D., MacNee W., Flenley D. C., Wright D., McLean A., Lamb D., Wightman A. J., Best J. Diagnosis of pulmonary emphysema by computerised tomography. Lancet. 1984 Aug 11;2(8398):320–322. doi: 10.1016/s0140-6736(84)92689-8. [DOI] [PubMed] [Google Scholar]
- Mitchell R. S., Stanford R. E., Johnson J. M., Silvers G. W., Dart G., George M. S. The morphologic features of the bronchi, bronchioles, and alveoli in chronic airway obstruction: a clinicopathologic study. Am Rev Respir Dis. 1976 Jul;114(1):137–145. doi: 10.1164/arrd.1976.114.1.137. [DOI] [PubMed] [Google Scholar]
- Pare P. D., Brooks L. A., Bates J., Lawson L. M., Nelems J. M., Wright J. L., Hogg J. C. Exponential analysis of the lung pressure-volume curve as a predictor of pulmonary emphysema. Am Rev Respir Dis. 1982 Jul;126(1):54–61. doi: 10.1164/arrd.1982.126.1.54. [DOI] [PubMed] [Google Scholar]
- Petty T. L., Silvers G. W., Stanford R. E. Functional correlations with mild and moderate emphysema in excised human lungs. Am Rev Respir Dis. 1981 Dec;124(6):700–704. doi: 10.1164/arrd.1981.124.6.700. [DOI] [PubMed] [Google Scholar]
- Petty T. L., Silvers G. W., Stanford R. E. Small airway disease is associated with elastic recoil changes in excised human lungs. Am Rev Respir Dis. 1984 Jul;130(1):42–45. doi: 10.1164/arrd.1984.130.1.42. [DOI] [PubMed] [Google Scholar]
- REID L., SIMON G. III. Pathological findings and radiological changes in chronic bronchitis and emphysema. Br J Radiol. 1959 May;32(377):291–305. doi: 10.1259/0007-1285-32-377-291. [DOI] [PubMed] [Google Scholar]
- Ryder R. C., Thurlbeck WM GOUGH J. A study of interobserver variation in the assessment of the amount of pulmonary emphysema in paper-mounted whole lung sections. Am Rev Respir Dis. 1969 Mar;99(3):354–364. doi: 10.1164/arrd.1969.99.3.354. [DOI] [PubMed] [Google Scholar]
- THURLBECK W. M. The incidence of pulmonary emphysema, with observations on the relative incidence and spatial distribution of various types of emphysema. Am Rev Respir Dis. 1963 Feb;87:206–215. doi: 10.1164/arrd.1963.87.2.206. [DOI] [PubMed] [Google Scholar]
- The definition of emphysema. Report of a National Heart, Lung, and Blood Institute, Division of Lung Diseases workshop. Am Rev Respir Dis. 1985 Jul;132(1):182–185. doi: 10.1164/arrd.1985.132.1.182. [DOI] [PubMed] [Google Scholar]
- Thurlbeck W. M., Horowitz I., Siemiatycki J., Dunnill M. S., Maisel J. C., Pratt P., Ryder R. Intra- and inter-observer variations in the assessment of emphysema. Arch Environ Health. 1969 Apr;18(4):646–659. doi: 10.1080/00039896.1969.10665467. [DOI] [PubMed] [Google Scholar]
- Thurlbeck W. M. Internal surface area and other measurements in emphysema. Thorax. 1967 Nov;22(6):483–496. doi: 10.1136/thx.22.6.483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thurlbeck W. M. The internal surface area of nonemphysematous lungs. Am Rev Respir Dis. 1967 May;95(5):765–773. doi: 10.1164/arrd.1967.95.5.765. [DOI] [PubMed] [Google Scholar]