

Abstract
Purpose: This study surveyed physiotherapists working at Canadian cystic fibrosis (CF) specialized centres to investigate the current practice, barriers to, and facilitators of exercise testing and training. Method: Physiotherapists were recruited from 42 Canadian CF centres. They responded to an e-questionnaire regarding their practice. The data were analyzed using descriptive statistics. Results: Eighteen physiotherapists responded (estimated response rate of 23%); median years of clinical experience was 15 (range, min-max, 3–30) years. Aerobic testing was administered by 44% of respondents, strength testing by 39%, aerobic training by 78%, and strength training by 67%. The most frequently reported barriers across all four types of exercise testing and training were insufficient funding (reported by 56%–67% of respondents), time (50%–61%) and staff availability (56%). More late career than early career physiotherapists reported utilizing aerobic testing (50% vs. 33% of respondents), strength testing (75% vs. 33%), aerobic training (100% vs. 67%), and strength training (100% vs. 33%). Conclusions: Exercise testing and training is underutilized in Canadian CF centres. Experienced physiotherapists reported utilizing exercise testing and training more than less-experienced physiotherapists. Post-graduate education and mentorship, especially for less-experienced clinicians, are recommended to emphasize the importance of exercise testing and training. Barriers of funding, time, and staff availability should be addressed to further improve quality of care.
Key Words: cystic fibrosis, endurance training, professional practice gaps, rehabilitation, resistance training
Abstract
Objectif :sondage auprès de physiothérapeutes qui travaillent dans des centres canadiens spécialisés en fibrose kystique (FK) pour examiner les pratiques, les obstacles et les incitations actuels liés aux épreuves et aux entraînements à l’exercice. Méthodologie: les physiothérapeutes ont été recrutés dans 42 centres canadiens spécialisés en FK. Ils ont répondu à un questionnaire en ligne au sujet de leur pratique. Les données ont été analysées au moyen de statistiques descriptives. Résultats: les 18 physiothérapeutes qui ont répondu (taux de réponse estimatif de 23 %) avaient une médiane de 15 années d’expérience clinique (plage minimale-maximale de trois à 30 ans). Ainsi, 44 % des répondants effectuaient des épreuves d’endurance aérobique, 39 %, des épreuves en résistance, 78 %, un entraînement aérobique et 67 %, un entraînement en résistance. Les obstacles les plus signalés dans les quatre types d’épreuves et d’entraînement à l’exercice étaient un financement insuffisant (par 56 % à 67 % des répondants), le manque de temps (50 % à 61 %) et le peu de disponibilité du personnel (56 %). Plus de physiothérapeutes en fin de carrière qu’en début de carrière ont déclaré utiliser les épreuves d’endurance aérobique (50 % par rapport à 33 % des répondants), les épreuves de résistance (75 % par rapport à 33 %), l’entraînement aérobique (100 % par rapport à 67 %) et l’entraînement en résistance (100 % par rapport à 33 %). Conclusions: l’épreuve et l’entraînement à l’exercice sont sous-utilisés dans les centres canadiens spécialisés en FK. Les physiothérapeutes d’expérience étaient plus nombreux à avoir déclaré utiliser l’épreuve et l’entraînement à l’exercice que les physiothérapeutes moins expérimentés. Les études supérieures et le mentorat, particulièrement chez les cliniciens moins expérimentés, sont recommandés pour insister sur l’importance de l’épreuve et de l’entraînement à l’exercice. Il faut corriger les obstacles au financement, au temps et à la disponibilité du personnel pour améliorer encore davantage la qualité des soins.
Mots-clés : : entraînement en endurance, entraînement en résistance, fibrose kystique, lacunes de la pratique professionnelle, réadaptation
Cystic fibrosis (CF) is the most common fatal genetic disease. It predominantly affects Caucasias and impacts multiple body systems, including the respiratory systems.1,2 There are over 4,370 people with CF in Canada.1 Individuals with CF have decreased aerobic capacity2 and peripheral muscle strength,3 higher rates of depression and anxiety,4 and lower health related quality of life (QOL).1
In Canada, this multisystem disease is managed by CF specialized centres. In these centres, various health care professionals with in-depth knowledge of CF and experience in CF care provide interdisciplinary care. In general, it is recommended that individuals with CF attend a CF centre every three months; however this interval varies depending on the individual’s health status. The role of physiotherapists in CF care has evolved from mainly facilitating airway clearance to incorporating different types of exercise in assessment and treatment.5,6 The main role of physiotherapists in CF care, as outlined in the International Physiotherapy Group’s practice guidelines, are airway clearance therapy, inhalation therapy, exercise testing and training, musculoskeletal physiotherapy management, and pre- and post- lung transplant care.5–7 To our knowledge, the extent of exercise testing and training being performed in Canadian CF centres is unknown.
Aerobic testing is defined as an assessment for an individual’s cardiopulmonary status; it is measured by maximal, submaximal, laboratory-based or field-based tests. Measures derived from aerobic testing, (e.g., Vo2max) are prognostic indicators for individuals with CF.8 Aerobic testing and strength testing also provide a baseline of general physical health and can inform exercise prescription.9 For individuals with CF, studies show that aerobic training can improve pulmonary function, aerobic capacity, physical activity levels; ameliorate symptoms of anxiety and depression; and enhance health related QOL.5,10,11 Strength training helps increasing force production, fosters a lean body mass, and improves pulmonary function for individuals with CF.11,13
Studies conducted in the United Kingdom, Germany, and the United States have found that general exercise testing and training are underutilized in CF centres.13–15 While these studies addressed general exercise, a study in Australia and New Zealand specifically looked at the extent of strength testing in CF centres and reported that only 20% of centres included strength testing.16 These results, however, cannot be generalized to Canadian CF centres because of inherent differences in the health care systems.
Multiple studies report that a barrier to incorporating exercise testing and training in clinical practice is the lack of resource availability, including the lack of trained personnel, time, equipment, facilities, and infection control precautions.13–16 In contrast, another study found that a lack of equipment was not a barrier; these researchers reported a quantity of available equipment was not being used.13 Previous studies have not investigated facilitators, specifically, of exercises testing and training. Rather they report that the rationale, specifically, for conducting exercise testing and training is based on disease severity, in response to patients reporting decreased exercise tolerance, or conducted immediately post-discharge from acute care, and for the purpose of pre-transplant assessment.16 It is unknown what barriers and facilitators CF centres in Canada encounter with exercise testing and training. Identifying specific barriers and facilitators within CF centres may help strategize ways to enhance incorporating exercise testing and training in clinical practice.
In most studies on exercise testing and training, physicians were the main respondents to surveys, followed by physiotherapists and nurses.13,15 Although physicians may provide a general insight into the practice, it would be beneficial to have physiotherapists as the primary respondents because they would have a first-hand experience with exercise testing and training, and would be able to provide a different perspective.
Many entry-level health care graduates doubt their level of competence and readiness to practise.17 It can be more challenging for them when working in a specialized clinical area, such as CF care. Previous studies have shown that the cognitive processes between novice and expert physiotherapists differ.18–20 It is unknown whether there is a difference in utilization of exercise testing and training by physiotherapists with less experience relative to physiotherapists with more experience in CF centres. If there are discrepancies, it may highlight the need to improve the learning experiences for physiotherapists in CF care to support utilization of exercise testing and training.
The knowledge-to-action model21 describes a process by which knowledge (e.g., practice guidelines recommendations for exercise testing and training) can be turned into action in clinical practice. The model involves identifying a gap between knowledge and practice, and assessing barriers to implementating the knowledge. Following that, the model involves implementing changes, monitoring and evaluating outcomes, and sustaining change. As current physiotherapy practice regarding exercise testing and training in Canadian CF centres is unknown, and in consideration of the knowledge-to-action model, the objectives of this study were to (1) determine the utilization of aerobic testing, strength testing, aerobic training, and strength training in Canadian CF centres, (2) identify the barriers and facilitators for implementing exercise testing and training; and (3) investigate the relationship between physiotherapist’s year of clinical experience and utilization of exercise testing and training in CF centres.
Methods
Study design
A quantitative cross-sectional web-based survey was administered to physiotherapists practicing in Canadian CF centres. To be eligible, participants had to be a physiotherapist working in one of the 42 Canadian CF centres, defined as a clinic that provides specialized interdisciplinary care for individuals with CF and is accredited and supported financially by Cystic Fibrosis Canada. Participants were excluded if they provided only weekend and/or holiday coverage. Ethics approval was obtained from the University of Toronto (REB 00038507).
Recruitment
The secretary for the Canadian CF Physiotherapy Advisory Group emailed all of the physiotherapists working at Canadian CF centres to request their participation. The email included a brief description of this study, an informed consent letter containing information on the purpose of the study, risks, benefits, consent, confidentiality, and publication, a link to the questionnaire including an initial page to indicate consent, and the authors’ email address for questions and to request study results. Two additional emails, spaced two weeks apart, were sent to remind physiotherapists to complete the questionnaire.
Data collection
The 40-item questionnaire was developed based on previous similar studies.13–16 The questionnaire examined the proportion of physiotherapists surveyed who perform aerobic testing, strength testing, aerobic training, and strength training with their CF caseload; the barriers and facilitators to incorporating exercise testing and training as measured by the 5 point-Likert scale; and the demographics of the physiotherapists. To reduce self-report bias and protect participant privacy, the demographic information was collected in a manner that would keep the physiotherapists and CF centres anonymous. The questionnaire was administered through Research Electronic Data Capture (REDCap), version 7.4.1.22,23 The questionnaire piloted with physiotherapists on the cardiorespiratory team at St. Michael’s Hospital, modified based on feedback, and then administered to study participants between March to April 2020.
Statistical analysis
Descriptive statistics were computed, including medians, ranges and frequencies, using IBM SPSS Statistics, version 26.0 (IBM Corporation, Armnok, NY). To geographically present the data relating to objective 3, participants were categorized into the following groups: (1) early career, those with <10 years of experience, (2) mid career, those with >10 and <20 years of experience; and (3) late career, those with >20 years of experience.
Results
A total of 18 physiotherapists responded out of an estimated 84 physiotherapists working in Canadian CF centres, with there being between 1–3 physiotherapists per centre. The median years of clinical experience was 15 (range, min-max, 3–30) years, with a median full-time equivalence of 0.30 (range, min-max, 0.05–1.00) hours worked/ full-time hours working at the CF centre. There were 67% (12) respondents from Western Canada, 17% (3) from Ontario, and 17% (3) from Quebec and Eastern Canada. Table 1 summarizes the demographic data.
Table 1 .
Characteristics of Physiotherapists Working in CF Centres Across Canada (N = 18)
| Characteristic (N = 18) | No. (%) of respondents |
|---|---|
| % of caseload that is patients with CF | |
| <40% | 10 (56) |
| 40% to <80% | 3 (17) |
| 80%–100% | 5 (28) |
| Practice region | |
| Western Canada (BC/AB/SK/MB) | 12 (67) |
| Ontario | 3 (17) |
| Quebec and Eastern Canada (NB/NS/NL) | 3 (17) |
| Clinical practice setting | |
| Outpatient only | 4 (22) |
| Inpatient and outpatient | 14 (78) |
| Clinical practice population | |
| Paediatric only | 12 (67) |
| Adult and paediatric | 6 (33) |
CF = cystic fibrosis; BC = British Columbia; AB = Alberta; SK = Saskatchewan; MB = Manitoba; NB = New Brunswick; NS = Nova Scotia; NL = Newfoundland and Labrador.
Utilization of exercise testing and training
Table 2 summarizes utilization of exercise testing and training: 44% (8) administered aerobic testing, 39% (7) administered strength testing, 78% (14) prescribed aerobic training, and 67% (12) prescribed strength training. Additionally, 39% (7) administered both aerobic testing and aerobic training, and 33% (6) administered both strength testing and training.
Table 2 .
Implementation of Aerobic and Strength Testing, and Aerobic and Strength Training in CF Centres in Canada
| Type of testing or training | No. of PTs who implement (N = 18) | Proportion of CF caseload for whom testing/training is implemented*
|
||||
|---|---|---|---|---|---|---|
| Small† | Medium† | Large† | ||||
| Aerobic testing | 8 | 7 | 1 | – | ||
| Strength testing | 7 | 7 | – | – | ||
| Aerobic training | 14 | 6 | 1 | 7 | ||
| Strength training | 12 | 9 | 1 | 2 | ||
| Aerobic testing and training | 7 | |||||
| Strength testing and training | 6 | |||||
Of physiotherapists who implement testing/training.
Small = 0 to <40% of CF caseload; medium = 40% to <60% of CF caseload; large = 60–100% of CF caseload.
CF = cystic fibrosis; PT = physiotherapist.
Among those who administer aerobic testing, 88% (7 out of 8) use the six minute walk test, 25% (2 out of 8) use the incremental shuttle walk test, and 13% (1 out of 8) utilized the Bruce protocol. Annual aerobic testing was reported by 75% (6 out of 8). For aerobic training, 92% (13 out of 14) of respondents recommended that their patients engage in aerobic training more than three times per week. Comparatively, 58% (7 out of 12) of respondents recommended that strength training to be performed three to four times per week. With respect to prescribing an aerobic home exercise programme, 71% (10 out of 14) respondents reported prescribing such a programme more than 50% of the time. In contrast, 58% (7 out of 12) respondents reported prescribing a strength-based home exercise programme less than 25% of the time. Regarding referring to other health care professionals for exercise training, 86% (12 out of 14) of respondents reported never or rarely (0%–25% of the time) referring out for aerobic training, while 67% (8 out of 12) of respondents reported never or rarely (0%–25% of the time) referring out for strength training, and 25% (3 out of 12) of respondents reported sometimes (50% of the time) referring out for strength training. All but one of the respondents who prescribed aerobic or strength training reported encouraging participation in recreational sports and fitness classes.
Rationale for, facilitators of, and barriers to exercise testing and training
Tables 3, 4 and 5 summarize the rationale for, facilitators of, and barriers to exercise testing and training. The most commonly reported reason for performing aerobic testing was to establish baseline values for patients, 88% (7 out of 8); followed by establishing eligibility for transplant, 75% (6 out of 8); responding to the request of physicians/nurse practitioners, 75% (6 out of 8); informing exercise prescription, 50% (4 out of 5); and estimating functional independence, 50% (4 out of 8). Of those who perform strength testing, their rationale included informing exercise prescription 86% (6 out of 7); establishing baseline values for patients 71% (5 out of 7); and estimating functional independence 71% (5 out of 7). No participants reported aerobic or strength testing as requirements by their place of work.
Table 3 .
Rationale for the Administration of Aerobic Testing and Strength Testing Utilized by Physiotherapists Working in CF Centres in Canada
| Aerobic testing, % (n = 8) | Strength testing, % (n = 7) | |
|---|---|---|
| Establishing baseline values | 88 | 72 |
| Informing exercise prescription | 50 | 86 |
| Estimating functional independence | 50 | 71 |
| Requested by physician/nurse practitioner | 75 | 14 |
| Establishing eligibility for transplant | 75 | N/A |
Note: Participants could select one or more response(s).
CF = cystic fibrosis.
Table 4 .
Facilitators for the Implementation of Aerobic and Strength Testing, Aerobic and Strength Training as Determined by Physiotherapists Working in CF Centres in Canada
| Aerobic testing, % | Strength testing, % | Aerobic training, % | Strength training, % | |
|---|---|---|---|---|
| Sufficient infection control | 72 | 72 | 67 | 56 |
| Sufficient knowledge | 44 | 61 | 72 | 61 |
| Sufficient equipment | 44 | 33 | 50 | 44 |
| Patient(s) willing to participate | 39 | 33 | 17 | 11 |
| Sufficient staff availability | 22 | 22 | 33 | 22 |
| Sufficient time | 17 | 22 | 17 | 17 |
| Sufficient funding | 6 | 6 | 6 | 17 |
Note: Participants could select one or more response(s).
CF = cystic fibrosis.
Table 5 .
Barriers to the Implementation of Aerobic and Strength Testing, and Aerobic and Strength Training as Determined by Physiotherapists Working in CF Centres in Canada
| Aerobic testing, % | Strength testing, % | Aerobic training, % | Strength training, % | |
|---|---|---|---|---|
| Insufficient funding | 67 | 61 | 56 | 61 |
| Insufficient time | 61 | 61 | 50 | 61 |
| Insufficient staff availability | 56 | 56 | 56 | 56 |
| Insufficient equipment | 39 | 45 | 28 | 28 |
| Patient(s) unwilling to participate | 17 | 17 | 11 | 17 |
| Insufficient infection control | 6 | 6 | 11 | 22 |
| Insufficient knowledge | 17 | 11 | – | 6 |
Note: Participants could select one or more response(s).
CF = cystic fibrosis.
The most frequently reported facilitator for aerobic testing and strength testing was sufficient infection control, 72% (13 out of 18). The most frequently reported facilitator for aerobic and strength training was the physiotherapist having sufficient knowledge to prescribe training programmes, 72% (13 out of 18) and 61% (11 out of 18), respectively.
Among the participants, 67% (12) reported insufficient funding as the primary barrier to administering aerobic testing; 56% (10) reported insufficient funding and staff availability as the main barriers to the implementing aerobic training; 61% (11) reported insufficient funding and time as main barriers to strength testing and strength training.
Years of experience and utilization of exercise testing and training
Figure 1 depicts the utilization of exercise testing and training among physiotherapists based on their years of experience in CF care. Of the early-career group, 33% (2 out of 6) of physiotherapists reported performing aerobic testing, strength testing, and strength training, while aerobic training was reported by 67% (4 out of 6). In the mid-career group, aerobic testing was reported by 50% (4 out of 8), strength testing by 25% (2 out of 8), and aerobic and strength training by 75% (6 out of 8). For the late-career group, aerobic testing was reported by 50% (2 out of 4), strength testing by 75% (3 out of 4). All of the late-career physiotherapists reported prescribing aerobic and strength training to their patients in the last 12 months.
Figure 1 .
Proportion of respondents implementing exercise testing and training by category (aerobic testing, strength testing, aerobic training, and strength training).
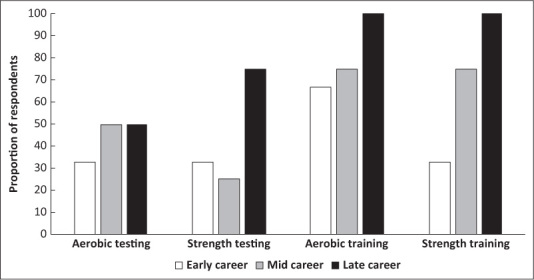
Note: Early career (≤10 years experience) n = 6, mid career (>10 years and <20 years of experience) n = 8, late career (≥20 years experience) n = 4.
Discussion
In this study, we investigated the current practice of, barriers to, and facilitators of, exercise testing and training by physiotherapists at Canadian CF centres. The main findings were that aerobic testing, strength testing, aerobic training and strength training are underutilized, with aerobic training being the most utilized. The most frequently reported barriers to exercise testing and training were insufficient funding, time, and staff availability. The most frequently reported facilitators were physiotherapists having appropriate knowledge to perform testing and training, and sufficient infection control practices. Mid- and late-career physiotherapists tend to utilize exercise testing and training more than their early-career colleagues.
The results of our study regarding the utilization of exercise testing and training were aligned with previous studies conducted in the United Kingdom, Germany, and the United States.13–15 The UK study also demonstrated that aerobic training was more commonly utilized than aerobic testing,15 which is similar to our study results. The previously mentioned studies focused solely on aerobic testing and aerobic training. In contrast, the study in Australia and New Zealand is uniquely similar to ours in that it looked at strength testing in addition to aerobic testing. That study reported a higher utilization of aerobic testing than our study, but similar preferential use of field-based exercise tests over lab-based tests, and similar underutilization of strength testing.16
We postulate that the underutilization of strength testing and training may be due to CF care historically focusing on managing respiratory function. However, there has been a recent increase in focus on muscle impairments in people with CF. In particular, a study found that altered expression of the CF transmembrane conductance regulator (CFTR) gene in skeletal muscle results in disruption of cell electrochemical gradients, which may impact the excitation-coupling necessary for skeletal muscle function.24 On a macroscopic level, individuals with CF have small thigh muscles and diminished hand grip strength.25 Given these physiological impairments, there is a need to optimize functional strength testing and prescribe strength training to ameliorate these impairments. It is estimated to take 17 years for research to translate into practice,26 which may help explain the underutilization of strength testing and training. As the average lifespan of individuals with CF lengthens due to advances in health care, such as a new class of drugs, CFTR modulator therapies, that modulate the function of CFTR proteins that are defective due to mutations the CFTR gene, musculoskeletal issues will become more prominent, resulting in an increased need for exercise, such as strength training, to improve physical functioning and QOL.12
Our study found aerobic testing to be less utilized than aerobic training. This raises the question of what background information physiotherapists use to prescribe aerobic training. It is plausible that other health care professionals (e.g., respiratory therapists) conduct the exercise testing, and that physiotherapists conduct informal exercise testing (e.g., observing patients’ mobility) and then prescribe exercise training. Or, exercise may be prescribed within the general parameters of intensity by using the Borg Dyspnea Scale or a range of predicted heart rates. However, our participants did not indicate the above alternative methods to inform exercise training in the questionnaire. Further, standardized aerobic testing is important for determining exercise capacity, symptoms related to exercise, the need for oxygen supplementation, and to monitor the efficacy of a training programme, all crucial for aerobic exercise prescription according to best practice guidelines.6 Additionally, due to COVID-19, many patients may be exercising independently, without medical supervision. This further emphasizes the need for initial exercise testing as a basis for safe exercise prescription, especially for patients with a history of adverse effects during exercise. There appears to be a lack of aerobic testing performed by physiotherapists at Canadian CF centres, and while understandable considering barriers (e.g., insufficient funding, time, and staff availability) it is a significant issue that should be addressed.
One of our objectives was to investigate facilitators for exercise testing and training. Within this objective, we further investigated the clinicians’ rationales for implementing exercise testing. Our study found that the most frequently reported facilitators for exercise testing and training are sufficient infection control practices, and physiotherapists possessing adequate knowledge for testing protocols. Infection control practices are essential to minimize patient-to-patient spread of pathogens, which is crucial for individuals with CF at all times. The rationale for performing testing procedures was to establish baseline values of patients and guide exercise prescription. Similarly, the study in Australia and New Zealand, which discussed only the rationale for exercise testing, reported that it is conducted for patient annual assessments and in response to reduced exercise tolerance.16
With respect to the barriers for exercise testing and training, our study had similar findings to research conducted in the United Kingdom, and Australia and New Zealand; that is, the most common barriers that hinder the utilization of exercise testing and training are insufficient funding, time, and staff availability at CF centres.15,16 A possible explanation for the commonalities in barriers that CF physiotherapists in the United Kingdom, Australia and New Zealand, and Canada,15,16 encounter may be that they all have universal, publicly funded health care systems. Thus, barriers such as insufficient funding must be examined at a health systems level as opposed to studying individual CF centres.
It is widely acknowledged that the health care systems in many Canadian provinces struggle to procure sufficient funding.–27,28 Previous Canadian research highlights the costs associated with hospitalization of individuals with CF, citing an average of $21,000 per hospitalization in 2014 for pulmonary exacerbation.29 Research has also shown that individuals who undertake aerobic training have lower risks of hospitalization due to their higher aerobic fitness.30 Taken together, it is imperative that physiotherapists working in Canadian CF centres advocate for additional funding for exercise testing and training to help mitigate hospitalization costs but more importantly, to improve patient outcomes.
Our study reports that a substantially higher proportion of experienced physiotherapists, those with greater than 10 years of experience, perform exercise testing and training compared to their less experienced colleagues. To our knowledge, there are no previous studies examining the association between physiotherapists’ clinical experience and utilization of exercise testing and training in their CF practice in Canada. However, clinical experience has been previously shown to be related with clinical decision-making. Novice clinicians tend to prioritize their academic knowledge, while experienced clinicians transition towards using their clinical experience when making clinical decisions.20 Studies show that physiotherapists with less clinical experience prefer to seek assistance when making clinical decisions, as they report less self-efficacy and confidence in their decisions.19,20 Additionally, another study noted that experienced physiotherapists were more confident in managing uncertainty during decision-making and felt they could balance risks and benefits in their practice.31 Less experienced physiotherapists also demonstrated having lower confidence with assessment and treatment.32 When taken together, a lack of clinical experience and confidence may translate into less experienced physiotherapists underutilizing exercise testing and training in their practice; however, this requires further investigation to confirm. Wainwright and colleagues noted that both novice and experienced physiotherapists working in neurologic physiotherapy valued mentorship in developing clinical decision-making.20 Furthermore, students and novice physiotherapists felt that learning from peers was essential when developing clinical skills.33 This highlights the benefits of mentorship in specialized practice areas, such as CF centres, and the value it would provide less experienced physiotherapists in developing their skills. Further, online resources tailored towards enhancing practice of novice CF physiotherapists such as Australia’s CFphysio.com, may be a good supplement to mentorship sessions. Many workplaces also offer educational grants that may incentivize physiotherapists to further their professional development.
This study investigated the physiotherapy practices in CF Centres prior to the COVID-19 pandemic; however, it is imperative to highlight the impact of the pandemic on current and future practice. As many in-person services were disrupted, physiotherapists modified their practice by incorporating telerehabilitation. While the efficacy of telerehabilitation during the pandemic is still being investigated, a previous study investigating the remote administration of exercise training for individuals with chronic lung conditions concluded that individuals receiving supervised remote aerobic training demonstrated improvements in endurance exercise capacity as measured by increased shuttle walk test times.34 This needs to be confirmed with the CF population. The COVID-19 pandemic and subsequent research of efficacy of practice during that time may provide a unique opportunity to expand CF care, including exercise testing and training, to virtual platforms, making CF care more accessible to Canadians who live far from a CF centre.
Based on the knowledge-to-action model created by Graham and colleagues, our study identified a knowledge-practice gap between practice guidelines’ recommendations for exercise testing and training and its clinical utilization, and barriers and facilitators to utiliza- tion.21 To overcome the gap between practice guidelines and clinical practice, we propose the following recommendations.
We recommend education regarding the importance and benefits of aerobic testing, strength testing, aerobic training and strength training in CF care. More specifically, with regards to early-career physiotherapists, literature supports continued educational opportunities and men- torship to increase confidence and skills, which translates into improved decision-making in clinical practice.
Additionally, we recommend increased funding and staffing to minimize the barriers that physiotherapists encounter utilizing exercise testing and training. Future studies may investigate how increased funding can be allocated to best enable increased exercise testing and training.
A limitation of our study is that other health care professionals may have conducted exercise testing or training with the patients of physiotherapists responding to our study, which was not reflected in our questionnaire. However, we specifically directed our study towards physiotherapists working at CF centres to elucidate their current practice. We had a smaller sample size than expected, which may have been due to the following: the timeframe for data collection was reduced due to data collection occurring during the COVID-19 pandemic. Also physiotherapists may have been focused on their clinical work secondary to changes in personal protective equipment policy, redeployment, and prioritizing patients; therefore, had less opportunity to respond to our questionnaire.
Furthermore, a large proportion of our respondents were from Western Canada, limiting the generalizability of our findings to physiotherapist practice across all Canadian CF centres. Another limitation is that we do not know how many of Canada’s 42 CF centres represented in the response. This is because we ensured complete anonymity of all respondents, including which CF centres they worked at, to reduce response bias.
As our study did not examine the specific testing and training protocols used at Canadian CF centres, future studies should investigate the protocols used. This may help inform a future Canadian best practice guideline that CF centres could follow to standardize the high level of care they provide. Future studies should also continue the application of the knowledge-to-practice model through its subsequent stages of monitoring the change in utilization of exercise testing and training, evaluating patient outcomes, and ensuring sustainability of increased exercise testing and training in CF centres.
Conclusion
Aerobic testing, strength testing, aerobic training and strength training are underutilized at Canadian CF centres. Insufficient funding, time, and staff availability are the most reported barriers to the implementation of exercise testing and training. Additionally, a greater proportion of physiotherapists with more clinical experience in CF care tend to implement exercise testing and training. We recommend that the barriers of time and funding be addressed; physiotherapists continue to learn about the importance of testing and training for people with CF; and physiotherapists support one another, especially early-career clinicians, to increase the utilization of exercise testing and training in CF care.
Key Messages
What is already known on this topic
To improve patient outcomes, exercise testing and training are an important aspect of the physiotherapists’ role in CF care. However, studies show that exercise testing and training is underutilized at CF centres outside of Canada.
What this study adds
Exercise testing and training is underutilized in Canadian CF centres, with the most reported barriers being insufficient funding, time, and staff availability. This study recommends continuing education opportunities on the importance of exercise testing and training in CF care, and that the barriers to exercise testing and training be addressed to enable improved quality of care and outcomes for individuals with CF.
References
- 1.Cystic Fibrosis Canada . The Canadian Cystic Fibrosis Registry: 2017 annual data report [Internet]. Cystic Fibrosis Canada; 2018. Dec [cited 2020 May 18]. Available from: https://www.cysticfibrosis.ca/uploads/Registry%20Report%202017/2017%20Registry%20Annual%20Data%20Report.pdf
- 2.Troosters T, Langer D, Vrijsen B, et al. Skeletal muscle weakness, exercise tolerance and physical activity in adults with cystic fibrosis. Eur Respir J. 2009. Jan;33(1):99–106. [DOI] [PubMed] [Google Scholar]
- 3.Elkin SL, Williams L, Moore M, et al. Relationship of skeletal muscle mass, muscle strength and bone mineral density in adults with cystic fibrosis. Cyst Fibros. 2000;6. [PubMed]
- 4.Quittner AL, Goldbeck L, Abbott J, et al. Prevalence of depression and anxiety in patients with cystic fibrosis and parent caregivers: results of The International Depression Epidemiological Study across nine countries. Thorax. 2014. Dec;69(12):1090–7. [DOI] [PubMed] [Google Scholar]
- 5.Button BM, Wilson C, Dentice R, et al. Physiotherapy for cystic fibrosis in Australia and New Zealand: A clinical practice guideline. Respirol Carlton Vic. 2016. May;21(4):656–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Morrison L, Parrott H. Standards of care and good clinical practice for the physiotherapy management of cystic fibrosis [on the internet]. Cystic Fibrosis Trust; 2020. Nov [cited 2022 Sept 18] Available from: https://www.cysticfibrosis.org.uk/the-work-we-do/resources-for-cf-professionals/consensus-documents
- 7.International Physiotherapy Group for Cystic Fibrosis . Physiotherapy for People with Cystic Fibrosis: from Infant to Adult. 7th ed. 2019. [cited 2022 Sept 20]. Available from: https://www.ecfs.eu/sites/default/files/general-content-files/working-groups/IPG%20CF_Blue%20Booklet_7th%20edition%202019.pdf
- 8.Urquhart DS, Saynor ZL. Exercise testing in cystic fibrosis: Who and why? Paediatr Respir Rev. 2018. Jun;27:28–32. [DOI] [PubMed] [Google Scholar]
- 9.Martin C, Chapron J, Hubert D, et al. Prognostic value of six minute walk test in cystic fibrosis adults. Respir Med. 2013. Dec;107(12):1881–7. [DOI] [PubMed] [Google Scholar]
- 10.Radtke T, Nolan SJ, Hebestreit H, et al. Physical exercise training for cystic fibrosis. Cochrane Database Syst Rev. 2015. Jun 28;(6):CD002768. [DOI] [PubMed] [Google Scholar]
- 11.Selvadurai HC, Blimkie CJ, Meyers N, et al. Randomized controlled study of in-hospital exercise training programs in children with cystic fibrosis. Pediatr Pulmonol. 2002. Mar;33(3):194–200. [DOI] [PubMed] [Google Scholar]
- 12.Shaw I, Kinsey JE, Richards R, et al. Individualized supervised resistance training during nebulization in adults with cystic fibrosis. Pak J Med Sci. 2016. Oct; 32(5):1152–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Barker M, Hebestreit A, Gruber W, et al. Exercise testing and training in German CF centers. Pediatr Pulmonol. 2004. Apr;37(4):351–5. [DOI] [PubMed] [Google Scholar]
- 14.Kaplan TA, ZeBranek JD, McKey RM. Use of exercise in the management of cystic fibrosis: short communication about a survey of cystic fibrosis referral centers. Pediatr Pulmonol. 1991;10(3):205–7. [DOI] [PubMed] [Google Scholar]
- 15.Stevens D, Oades PJ, Armstrong N, et al. A survey of exercise testing and training in UK cystic fibrosis clinics. J Cyst Fibros Off J Eur Cyst Fibros Soc. 2010. Sep;9(5):302–6. [DOI] [PubMed] [Google Scholar]
- 16.Sawyer A, Cavalheri V, Wood J, et al. Exercise testing and exercise training within cystic fibrosis centres across Australia and New Zealand: what is considered important and what is current practice? Intern Med J. 2019. Aug 6. [DOI] [PubMed]
- 17.Reagor JK. Perceived readiness for practice of senior baccalaureate nursing students [dissertation]. University of Kansas, Lawrence KS; 2010. [Google Scholar]
- 18.Riolo L. Skill Differences in Novice and Expert Clinicians in Neurologic Physical Therapy. Neurol Rep. 1996; 20(1):60–63. [Google Scholar]
- 19.Smith M, Higgs J, Ellis E. Physiotherapy decision making in acute cardiorespiratory care is influenced by factors related to the physiotherapist and the nature and context of the decision: a qualitative study. Aust J Physiother. 2007. Jan 1;53(4):261–7. [DOI] [PubMed] [Google Scholar]
- 20.Wainwright SF, Shepard KF, Harman LB, et al. Factors That Influence the Clinical Decision Making of Novice and Experienced Physical Therapists. Phys Ther. 2011. Jan 1; 91(1):87–101. [DOI] [PubMed] [Google Scholar]
- 21.Graham ID, Logan J, Harrison MB, et al. Lost in knowledge translation: time for a map? J Contin Educ Health Prof. 2006;26(1):13–24. [DOI] [PubMed] [Google Scholar]
- 22.Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009. Apr;42(2):377–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform. 2019. Jul;95:103208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lamhonwah AM, Bear CE, Huan LJ, et al. Cystic fibrosis transmembrane conductance regulator in human muscle: Dysfunction causes abnormal metabolic recovery in exercise. Ann Neurol. 2010. Jun;67(6):802–8. [DOI] [PubMed] [Google Scholar]
- 25.Wu K, Mendes PL, Sykes J, et al. Limb muscle size and contractile function in adults with cystic fibrosis: A systematic review and meta-analysis. J Cyst Fibros. 2021. Feb;S1569–1993(21):00045–X. [DOI] [PubMed] [Google Scholar]
- 26.Green LW, Ottoson JM, García C, et al. Diffusion theory and knowledge dissemination, utilization and integration. Front Public Health Serv Syst Res. 2014;3(1):3. [PMC free article] [PubMed] [Google Scholar]
- 27.Valle VM. An Assessment of Canada’s Healthcare System Weighing Achievements and Challenges. Norteamérica. 2016. Jul 1;11(2):193–218. [Google Scholar]
- 28.Financial Accountability Office of Ontario . Comparing Ontario’s Fiscal Position with Other Provinces [On the internet]. Financial Accountability Office of Ontario; 2019. Feb [cited 2020 May 18]. Available from: https://www.fao-on.org/en/Blog/Publications/inter-prov-comparisons-feb-2019
- 29.Skolnik K, Ronksley P, Pendharkar SR, et al. Hospital costs of Canadian cystic fibrosis patients. Canadian Journal of Respiratory, Critical Care, and Sleep Medicine. 2021;6(2):145–152. [Google Scholar]
- 30.Perez M, Groeneveld IF, Santana-Sosa E, et al. Aerobic fitness is associated with lower risk of hospitalization in children with cystic fibrosis. Pediatr Pulmonol. 2014. Jul;49(7):641–9. [DOI] [PubMed] [Google Scholar]
- 31.Smith M, Higgs J, Ellis E. Characteristics and processes of physiotherapy clinical decision making: a study of acute care cardiorespiratory physiotherapy. Physiother Res Int. 2008. Dec;13(4):209–22. [DOI] [PubMed] [Google Scholar]
- 32.Ackerman IN, Soh S-E, Barker AL. Physical therapists’ falls prevention knowledge, beliefs and practices in osteoarthritis care: A national cross-sectional study. Arthritis Care Res (Hoboken). 2020. Aug; 72(8):1087–95 [DOI] [PubMed] [Google Scholar]
- 33.Rappolt S, Tassone M. How rehabilitation therapists gather, evaluate, and implement new knowledge. J Contin Educ Health Prof. 2002;22(3):170–80. [DOI] [PubMed] [Google Scholar]
- 34.Tsai LL, McNamara RJ, Moddel C, et al. Home-based telerehabilitation via real-time videoconferencing improves endurance exercise capacity in patients with COPD: the randomized controlled TeleR Study. Respirology. 2016. Dec 19;22(4):699–707. [DOI] [PubMed] [Google Scholar]