

Abstract
Objective
Among persons with immune-mediated inflammatory diseases (IMIDs) who received SARS-CoV-2 vaccines, we compared postvaccine antibody responses and IMID disease activity/states.
Design
Single-centre prospective cohort study.
Setting
Specialty ambulatory clinics in central Canada.
Participants
People with inflammatory arthritis (n=78; 77% rheumatoid arthritis), systemic autoimmune rheumatic diseases (n=84; 57% lupus), inflammatory bowel disease (n=93; 43% Crohn’s) and multiple sclerosis (n=72; 71% relapsing-remitting) (female 79.4%, white 84.7%, mean (SD) age 56.0 (14.3) years) received COVID-19 vaccinations between March 2021 and September 2022.
Primary outcome
Postvaccination anti-spike, anti-receptor binding domain (anti-RBD) and anti-nucleocapsid (anti-NC) IgG antibodies tested by multiplex immunoassays compared across vaccine regimens and with responses in 370 age-matched and sex-matched vaccinated controls.
Secondary outcomes
COVID-19 infection and self-reported IMID disease activity/state.
Results
Most (216/327, 66.1%) received homologous messenger RNA (mRNA) (BNT162b2 or mRNA1273) vaccines, 2.4% received homologous ChAdOx1 and 30.6% received heterologous vaccines (23.9% ChAdOx1/mRNA, 6.4% heterologous mRNA) for their first two vaccines (V1, V2). Seroconversion rates were 52.0% (91/175) for post-V1 anti-spike and 58.9% (103/175) for anti-RBD; 91.5% (214/234) for post-V2 anti-spike and 90.2% (211/234) for anti-RBD; and were lower than controls (post-V2 anti-spike 98.1% (360/370), p<0.0001). Antibody titres decreased 3 months after V2 but increased 1 month after the third vaccine (V3) and 1 month after the fourth vaccine (V4) (BAU/mL median (IQR), anti-spike 1835 (2448) 1 month post-V2, 629.1 (883.4) 3 months post-V2, 4757.5 (7033.1) 1 month post-V3 and 4356.0 (9393.4) 1 month post-V4; anti-RBD 1686.8 (2199.44) 1 month post-V2, 555.8 (809.3) 3 months post-V2, 4280.3 (6380.6) 1 month post-V3 and 4792.2 (11 673.78) 1 month post-V4). If primed with a vector vaccine, an mRNA vaccine increased antibody titres to those comparable to homologous mRNA vaccines. Anti-RBD and anti-spike titres were higher in anti-NC seropositive (n=31; 25 participants) versus seronegative samples (BAU/mL median (IQR) anti-RBD 11 755.3 (20 373.1) vs 1248.0 (53 278.7); anti-spike 11 254.4 (15 352.6) vs 1313.1 (3106.6); both p<0.001). IMID disease activity/state and rates of self-reported moderate or severe IMID flare were similar across vaccinations.
Conclusion
Heterologous COVID-19 vaccination improves seroconversion rates following a vector vaccine and does not lead to IMID disease flare. IMIDs benefit from at least three vaccines.
Keywords: COVID-19, RHEUMATOLOGY, GASTROENTEROLOGY, NEUROLOGY, IMMUNOLOGY
STRENGTHS AND LIMITATIONS OF THIS STUDY.
This is a longitudinal cohort study with systematic collection of data on COVID-19 infection, immune-mediated inflammatory disease (IMID) activity and paired biosamples for anti-SARS-CoV-2 IgG assays following each vaccine, for up to four vaccines.
The study is a cross-disease comparisons of four IMIDs from different medical specialties that are treated with immunocompromising medications.
Validated measures of self-report IMID disease activity/state were used to assess vaccine safety and risk of postvaccine IMID disease flare.
The relatively small sample size for each IMID and the predominantly female population (as expected for these IMIDs) limit the analysis of sex and gender effects.
Introduction
COVID-19 vaccines have reduced the rates of serious SARS-CoV-2 infection and mortality in the general population.1–4 However, information on optimal vaccine strategies for immunocompromised individuals who are at increased risk of serious COVID-19 infection is limited.
Immune-mediated inflammatory diseases (IMIDs), such as autoimmune inflammatory arthritis (IA), systemic autoimmune rheumatic disease (SARD), inflammatory bowel disease (IBD) and multiple sclerosis (MS), affect 5% of the general population and share an autoimmune phenotype that affects multiple organ systems and treatment with immune therapies.5 Due to immune-mediated disease and treatment, some people with IMIDs are at increased risk of vaccine-preventable disease, including serious COVID-19 infection.6–10 While COVID-19 vaccines are effective in the general population, immune dysregulation from disease or treatment may impair vaccine responses in people with IMIDs. Due to evolving regional vaccination strategies in our region11 (online supplemental figure 1), a high proportion of individuals with immunocompromised conditions received heterologous vaccine courses. Although available data on immunogenicity of these mixed vaccine courses in the general population are reassuring,12–14 data are limited regarding the safety and immunogenicity of this strategy for immunocompromised patients, as are data comparing these outcomes across diseases.
bmjopen-2022-071397supp001.pdf (1.9MB, pdf)
We established a cohort of patients diagnosed with any of IA, SARDs, IBD or MS to determine the safety (IMID flare) and humoral immunogenicity following COVID-19 vaccination and to assess the impact of mixing COVID-19 vaccine types. Herein, we report the clinical safety results and seroconversion results obtained after four vaccinations and compare the seroconversion rates across initial vaccine combinations.
Methods
Study design
This single-centre prospective cohort from Manitoba, Canada, was established in March 2021 and enrolled people diagnosed with any of IA, SARDs, IBD or MS. Data were collected until 30 October 2022. Vaccines were administered in accordance with provincial public health recommendations. Study participants were followed 1 and 3 months after each vaccine for up to four vaccines.
Study objectives
The primary study objective was to compare postvaccination anti-spike (S1), anti-receptor binding domain (anti-RBD) and anti-nucleocapsid (anti-NC) IgG antibody seroconversion and titres across vaccine regimens. The secondary study objectives were to determine the kinetics of seropositivity and titres across vaccine doses, to compare immunogenicity across IMIDs, to determine the effect of vaccination on COVID-19 infection (efficacy), and to determine postvaccine IMID disease activity/state and self-reported IMID flare (safety).
Recruitment
We approached potential participants attending ambulatory clinics using multiple methods with an aim to enrol 400 individuals with a diagnosed IMID. Our sample size was limited by recruitment.
Clinical data
Demographic data including birth date, sex, self-reported ethnic group according to the Canadian Institute for Health Information guidelines,15 highest education level achieved, self-reported comorbidity and health behaviours such as smoking history were collected at baseline. Clinical data including IMID treatment, IMID-specific disease activity/state measures, participant-reported interval COVID-19 infections with type of confirmatory test and biosamples were collected at each visit. IMID treatment was subcategorised as anti-inflammatories and immunomodulators such as 5-aminosalicylic acid (5-ASA), sulfasalazine, hydroxychloroquine, glatiramer and interferon therapies; traditional immunosuppressants such as methotrexate, leflunomide, azathioprine and mycophenolate; biologic or advanced therapies such as antitumour necrosis factor (anti-TNF) agents, B cell-depleting agents, vedolizumab, fingolimod, anticytokine therapies, other biologics and Janus kinase inhibitors; and corticosteroids (online supplemental table 1). Self-reported IMID disease activity/status was assessed with disease-relevant validated measures (IA: Routine Assessment of Patient Index Data 3 and Rheumatoid Arthritis Flare Core domain indices; SARD: Systemic Lupus Activity Questionnaire; IBD: Inflammatory Bowel Symptoms Severity Index-Short Form and Manitoba IBD Flare Question; MS: self-report disease activity and Expanded Disability Status Scale).16–20 These disease-related questionnaires were fully completed for IBD (248/255, 97% visits), IA (208/215, 97% visits), SARDs (239/260, 92% visits) and MS (291/327, 89% visits). Data were not imputed. Individuals could attend a study visit in person or submit their data by mailed paper forms or direct entry into a REDCap electronic database hosted at the University of Manitoba.21 Participants had the option to participate in the safety study component only.
Biosamples
Participants not attending the clinic were provided kits to collect blood by finger poke on dried blood spot (DBS) cards for postal submission.22 Participants attending the clinic had blood collected by venipuncture, and DBS was prepared before processing blood for serum. Aliquoted serum and DBS cards were stored at −20°C for batch testing.
Regional population control biosample data were obtained from 370 vaccinated Canadian Blood Services blood donors who were age-matched and sex-matched to the clinical cohort. Data on vaccine type administered were not available.
Serology
A bead-based multiplexed immunoassay was used to detect IgG anti-S1, RBD (reflecting response to vaccine) and NC antibodies (reflecting response to infection) (Bio-Rad BioPlex 2200 SARS-CoV-2 IgG assay). This assay was chosen based on an evaluation of several multiplex platforms using a large panel of well-pedigreed plasma DBS specimens.22 The quantitative measurement of the antibody response used the WHO International Standard for anti-SARS-CoV-2 antibody detection. Cut-offs for seropositivity for DBS samples were established using receiver operating characteristic (ROC) curve analysis. Cut-offs for plasma from the company were used. Sera from patients with IA (n=19) and patients with lupus (n=31) collected before the pandemic were tested to evaluate the potential for false-positive SARS-CoV-2 antibody tests in IMIDs with known autoantibodies. Concordance of antibody assays in paired DBS and serum samples was assessed using the Kendall’s tau b test. The controls were tested using the Roche Elecsys anti-SARS-CoV-2 spike protein semiquantitative immunoassay (Roche Diagnostics International, Rotkreuz, Switzerland), which measures total antibodies (including IgA, IgM and IgG) to the SARS-CoV-2 spike protein (anti-S), and the Roche Elecsys anti-SARS-CoV-2 qualitative immunoassay (Roche Diagnostics International), which measures total antibodies (including IgA, IgM and IgG) to SARS-CoV-2 recombinant protein, nucleocapsid antigen (anti-NC).
Analysis
Demographic information of participants is reported using descriptive statistics, including mean (SD), median (range or IQR) and counts (%). Non-parametric tests (Mann-Whitney U or Kruskal-Wallis tests with Bonferroni adjustment for multiple comparisons) were used to compare antibody levels across groups and visits. Wilcoxon signed-rank tests were used to compare antibody levels across visits within individuals. Binary logistic regression was used to evaluate predictors of seroconversion 1 month following the second vaccine (V2). Variables included sex, age greater than 65 years, IMID diagnosis, treatment category (none vs biologics and advanced therapies vs immunosuppressants vs other agents) and vaccine mix (vector–messenger RNA (mRNA) vs mRNA–mRNA). Statistical analysis was conducted using IBM SPSS Statistics V.27 for Windows.
Consent
All subjects provided informed consent.
Patient and public involvement
Patients or the public were not involved in the study design or in the conduct or reporting of the research. Participants were informed of their serological results.
Results
Between 12 March 2021 and 30 July 2022, we recruited 339 participants (online supplemental figure 2). Vaccination and disease activity data for the time points reported herein were available for 327 participants (78 IA: 77% rheumatoid arthritis; 84 SARDs: 57% lupus; 93 IBD: 43% Crohn’s; and 72 MS: 71% relapsing-remitting) (table 1). Most were female (79.4%) and white (84.7%), with a mean (SD) age of 56.0 (14.3) years. Nearly one-third (30.6%) of participants with IMID were taking biologics or advanced therapies.
Table 1.
Demographics, vaccines administered, self-reported IMID flare and COVID-19 history of participants
| IA n=78 | SARD n=84 | IBD n=93 | MS n=72 | All IMIDs n=327 | |
| Age, years, mean (SD) | 61.9 (11.8) | 55.7 (13.4) | 53.7 (16.4) | 53.1 (13.5) | 56.0 (14.3) |
| Female, n (%) | 66 (84.6) | 75 (89.3) | 59 (63.4) | 59 (81.9) | 259 (79.4) |
| White, n (%) | 66 (84.6) | 64 (76.2) | 79 (84.9) | 68 (94.4) | 277 (84.7) |
| Education | |||||
| Years of school, median (IQR) | 15.0 (4.5) | 16.0 (4.3) | 16.0 (4.0) | 16.0 (5.0) | 16.0 (4.0) |
| Comorbidity*, n (%) | |||||
| Cardiovascular | 35 (44.9) | 31 (36.9) | 26 (28.0) | 22 (30.5) | 115 (35.1) |
| Pulmonary | 8 (10.2) | 24 (28.6) | 15 (16.1) | 8 (11.1) | 55 (16.8) |
| Diabetes | 13 (19.7) | 3 (3.7) | 3 (3.4) | 5 (6.9) | 24 (7.3) |
| Other endocrine | 25 (32.1) | 24 (28.6) | 20 (21.5) | 20 (27.8) | 90 (27.4) |
| Renal disease | 2 (3.0) | 9 (11.0) | 4 (4.3) | 0 (0.0) | 15 (4.6) |
| Cancer | 15 (19.2) | 10 (11.9) | 12 (12.9) | 5 (6.9) | 43 (13.10) |
| Mental health | 17 (21.8) | 27 (32.9) | 27 (29.0) | 22 (30.6) | 94 (28.7) |
| Total, median (range) | 2.5 (0–10) | 3 (0–10) | 2 (0–10) | 2 (0–6) | 2 (0–10) |
| BMI, mean (SD) | 27 (6.6) | 28.0 (7.8) | 27.2 (6.1) | 28.0 (6.2) | 27.7 (6.7) |
| IMID treatment level†, n (%) | |||||
| Immunomodulators | 4 (5.1) | 25 (30.5) | 21 (22.6) | 28 (38.9) | 78 (23.9) |
| Immunosuppressants | 27 (34.6) | 42 (51.2) | 10 (10.8) | 0 (0.0) | 79 (24.2) |
| Biologics/JAKi | 37 (47.4) | 7 (8.5) | 41 (44.1) | 14 (19.4) | 99 (30.3) |
| Anti-TNF, n | 22 | 2 | 28 | 0 | 52 |
| Anti-B cell, n | 5 | 6 | 0 | 10 | 21 |
| Other or JAKi, n | 9 | 0 | 13 | 4 | 26 |
| None | 11 (14.1) | 9 (10.7) | 21 (22.6) | 30 (41.7) | 71 (21.7) |
| Vaccine type, V1‡, n (%) | |||||
| ChAdOx1 | 15 (19.5) | 28 (33.3) | 17 (18.3) | 26 (36.1) | 86 (26.4) |
| BNT | 60 (77.9) | 56 (66.7) | 66 (71.0) | 39 (54.2) | 221 (67.8) |
| mRNA1273 | 2 (2.6) | 6 (7.1) | 10 (10.8) | 7 (9.7) | 25 (7.7) |
| Vaccine type, V2‡, n (%) | |||||
| ChAdOx1 | 2 (2.6) | 3 (3.6) | 3 (3.2) | 1 (1.4) | 9 (2.7) |
| BNT | 65 (84.4) | 58 (68.7) | 60 (65.2) | 54 (75.0) | 236 (72.8) |
| mRNA1273 | 16 (13.0) | 23 (27.7) | 29 (31.5) | 17 (23.6) | 79 (24.4) |
| Vaccine type, V3‡, n/N (%) | |||||
| ChAdOx1 | 0 | 0 | 1 (1.3) | 1 (1.6) | 2 (0.7) |
| BNT | 54 (71) | 58 (78.4) | 49 (66.2) | 39 (61.9) | 200 (71.2) |
| mRNA1273 | 16 (21.1) | 16 (21.6) | 24 (32.4) | 23 (36.5) | 79 (28.1) |
| Other | 0 | 0 (0) | 1 (1.4) | 1 (1.6) | 2 (0.7) |
| Vaccine type, V4‡, n/N (%) | |||||
| ChAdOx1 | 0 (0) | 1 (2.7) | 0 (0) | 0 (0) | 1 (0.8) |
| BNT | 25 (69.4) | 28 (75.7) | 25 (64.1) | 12 (70.6) | 90 (69.8) |
| mRNA1273 | 10 (27.8) | 8 (21.6) | 14 (35.9) | 2 (11.8) | 34 (26.4) |
| Other | – | – | – | 3 (17.6) | 3 (2.3) |
| Vaccines for V1 and V2, n (%) | |||||
| ChAdOx1–BNT | 9 (11.5) | 10 (11.9) | 4 (4.3) | 17 (23.6) | 40 (12.2) |
| ChAdOx1–mRNA1287 | 4 (5.1) | 15 (17.9) | 11 (11.8) | 8 (11.1) | 38 (11.6) |
| BNT–mRNA1273 or mRNA1273–BNT | 4 (5.1) | 5 (6.0) | 10 (10.8) | 2 (2.8) | 21 (6.4) |
| BNT–ChAdOx1 | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 1 (0.3) |
| ChAdOx1–ChAdOx1 | 2 (2.6) | 3 (3.6) | 2 (2.2) | 1 (1.4) | 8 (2.4) |
| BNT–BNT | 56 (71.8) | 46 (54.8) | 55 (59.1) | 37 (51.4) | 194 (59.3) |
| mRNA1273–mRNA1273 | 2 (2.6) | 4 (4.8) | 9 (9.7) | 7 (9.7) | 22 (6.7) |
| Vaccine interval | |||||
| Days between V1 and V2, median (range) | 66 (21–97) | 62 (20–188) | 57 (20–98) | 59 (26–97) | 60 (20–188) |
| Self-report IMID flare§,¶, n/N (%) | |||||
| 1 month post-V1 | 12/44 (27.3) | 10/44 (22.7) | 0/44 (0) | 1/41 (2.4) | 23/173 (13.3) |
| 1 month post-V2 | 9/56 (16.1) | 9/58 (8.6) | 0/67 (0) | 2/69 (2.9) | 20/250 (8.0) |
| 1 month post-V3 | 11/57 (19.3) | 19/63 (30.2) | 2/62 (3.3) | 1/61 (1.6) | 33/243 (13.6) |
| 1 month post-V4 | 6/38 (15.8) | 12/57 (21.1) | 4/38 (8.3) | 1/24 (4.2) | 23/157 (14.6) |
| 1 month post any vaccine | 38/195 (19.5) | 50/202 (24.8) | 6/211 (2.8) | 5/129 (3.9) | 99/803 (12.2) |
| COVID-19 illness, ever¶, n (%) | |||||
| None | 43 (55.1) | 38 (46.3) | 46 (50.0) | 31 (43.1) | 158 (48.8) |
| Suspected but not tested | 27 (34.6) | 29 (35.4) | 22 (23.9) | 24 (33.3) | 112 (34.6) |
| COVID-19 PCR-positive | 8 (10.3) | 13 (15.9) | 14 (15.2) | 17 (23.6) | 52 (16.0) |
| COVID-19-positive, hospitalised | 0 (0.0) | 2 (2.4) | 0 (0.0) | 0 (0.0) | 2 (0.6) |
IA: rheumatoid arthritis (RA), n=60; psoriatic arthritis, n=8; other spondyloarthropathy, n=3; other IA, n=7. SARDs: systemic lupus erythematosus, n=48; myopathy, n=5; vasculitis, n=7; other or unknown SARDs, n=24. IBD: Crohn’s disease n=43. MS: relapsing-remitting, n=51; secondary progressive, n=11; primary progressive, n=4; unknown, n=2.
*Cardiovascular disease includes ischaemic heart disease, congestive heart failure, valvular heart disease, peripheral vascular disease, stroke or transient ischaemic attack, or hypertension; respiratory disease includes asthma or chronic obstructive pulmonary disease; other endocrine includes thyroid disease and hypercholesterolaemia.
†IMID treatment based on the most aggressive combination if on multiple agents. One subject with RA on only prednisone monotherapy. Medication data missing for two subjects with SARD. Other therapy: n=26 (ustekinumab n=6, vedolizumab n=7, abatacept n=1, tofacitinib n=4, tocilizumab n=3, fingolimod n=2, alemtuzumab n=1, natalizumab n=1, upadacitinib n=1).
‡Vaccine data available for V1: n=326 (77 IA, 84 SARD, 72 MS, 93 IBD); V2: n=324 (77 IA, 83 SARD, 72 MS, 92 IBD); V3: n=281 (76 IA, 74 SARD, 63 MS, 74 IBD); V4: n=128 (35 IA, 37 SARD, 39 IBD, 17 MS).
§Flare assessed by the following questions and reponses: IA: ‘Are you having a flare?’ Yes; SARDs: ‘In the past 3 months have you had a disease flare (A flare is when your disease gets worse)?’ Yes moderate or severe flare; IBD: ‘In the past 6 months my disease has been: Constantly active, giving me symptoms every day, or often active, giving me symptoms most days or sometimes active, giving me symptoms on some days (for instance 1–2 days/week)’; MS: ‘Do you feel there has been a change in your MS since your last visit?’ My multiple sclerosis is much worse and in a flare. Flare rate across IMIDs 1 month after any vaccine: χ2=72.9, p<0.001; flare rate post-V1 across IMIDs: χ2=21.8, p<0.001; flare rate post-V2 across IMIDs: χ2=17.7, p<0.001; flare rate post-V3 across IMIDs χ2=29.4, p<0.001; flare rate post-V4 across IMIDs: χ2=10.3, p=0.02. IMID flare rate across vaccination visits: χ2=7.4, p=0.06.
¶Self-reported over the course of the study. COVID-19 illness data missing for two participants with SARDs and one with IBD.
BMI, body mass index; BNT, BNT162b2 vaccine; IA, inflammatory arthritis; IBD, inflammatory bowel disease; IMID, immune-mediated inflammatory disease; JAKi, Janus kinase inhibitor; MS, multiple sclerosis; RA, rheumatoid arthritis; SARD, systemic autoimmune rheumatic disease; TNF, tumour necrosis factor inhibitor; V1, first vaccine; V2, second vaccine; V3, third vaccine; V4, fourth vaccine.
Samples of adequate quality were obtained following the first vaccine (V1) at 1 month (n=175) and 3 months (n=44), following the second vaccine at 1 month (n=234) and 3 months (n=246), following the third vaccine at 1 month (n=215), and following the fourth vaccine at 1 month (n=85). For 31 participants, DBS samples were of inadequate quality and a serum sample from the same day was substituted. In paired DBS and serum tests from 208 subjects, seroconversion and titres were highly concordant (Kendall’s tau b correlation coefficient: anti-RBD 0.93 BAU/mL; anti-S1 0.92 BAU/mL) (online supplemental figure 3). Prepandemic sera were seronegative for anti-SARS-CoV-2 antibodies.
Following the first vaccine, 60% of participants with IMID seroconverted (table 2). Following the second vaccine, seroconversion rates increased to 91% (p=0.1 across IMIDs for both anti-S1 and anti-RBD). The change in anti-S1 seropositivity between the first and second vaccines was significant (anti-S1: all IMIDs χ2=82.2, p<0.0001; IA χ2=40.5, p<0.0001; SARDs χ2=18.5, p<0.0001; IBD χ2=16.9, p<0.0001; MS, χ2=4.1, p=0.04; and anti-RBD: all IMIDs χ2=55.1, p<0.0001; IA χ2=31.6, p<0.0001; SARDs χ2=18.8, p<0.0001; IBD χ2=8.4, p<0.01; MS χ2=5.1, p=0.02). Of the 20 participants who were seronegative after the second vaccine and had data following the third vaccine, 8 of 15 (53.3) seroconverted after the third vaccine. Seroconversion rates for both anti-S1 and anti-RBD after the third and fourth vaccines were greater than 95%.
Table 2.
Seroconversion rates 1 month following each COVID-19 vaccine
| Seroconversion | IA, n/N (%) | SARDs, n/N (%) | IBD, n/N (%) | MS, n/N (%) | All IMIDs, n/N (%) |
| Post-V1 | |||||
| Anti-S1 | 14/47 (29.8) | 21/47 (44.7) | 33/48 (68.8) | 23/33 (69.7) | 91/175 (52.0) |
| Anti-RBD | 18/47 (38.2) | 22/47 (46.8) | 40/48 (83.3) | 23/33 (69.7) | 103/175 (58.9) |
| Anti-NC | 1/47 (2.1) | 0/48 (0) | 0/47 (0) | 1/33 (3) | 2/175 (1.1) |
| Post-V2* | |||||
| Anti-S1† | 50/55 (90.9) | 46/54 (85.1) | 62/64 (96.9) | 53/61 (86.9) | 214/234 (91.5) |
| Anti-RBD‡ | 50/55 (90.9) | 47/54 (87.0) | 63/64 (98.4) | 54/61 (88.5) | 211/234 (90.2) |
| Anti-NC | 1/55 (1.8) | 0/57 (0) | 1/64 (1.6) | 1/61 (1.6) | 3/234 (1.3) |
| Post-V3 | |||||
| Anti-S1 | 51/52 (98.1) | 57/62 (91.9) | 56/56 (100.0) | 41/45 (91.1) | 205/215 (95.3) |
| Anti-RBD | 51/52 (98.1) | 56/62 (90.3) | 56/56 (100.0) | 41/45 (91.1) | 204/215 (94.9) |
| Anti-NC | 2/52 (3.8) | 3/62 (4.8) | 2/56 (3.6) | 2/45 (4.4) | 9/215 (4.2) |
| Post-V4 | |||||
| Anti-S1 | 31/32 (96.9) | 21/23 (91.3) | 27/27 (100) | 3/3 (100) | 82/85 (96.5) |
| Anti-RBD | 31/32 (96.9) | 21/23 (91.3) | 27/27 (100) | 3/3 (100) | 82/85 (96.5) |
| Anti-NC | 3/32 (9.4) | 4/23 (17.4) | 3/27 (11.1) | 0/3 (0.0) | 10/85 (11.8) |
*Seroconversion V1 to V2 across IMIDs: anti-S1 χ2=82.2, p<0.0001; anti-RBD χ2=55.1, p<0.0001.
†Change in anti-S1 seropositivity V1 to V2: IA χ2=40.5, p<0.0001; SARDs χ2=18.5, p<0.0001; IBD χ2=16.9, p<0.0001; MS χ2=4.1, p=0.04.
‡Change in anti-RBD seropositivity V1 to V2: IA χ2=31.6, p<0.0001; SARDs χ2=18.8, p<0.0001; IBD χ2=8.4, p<0.01; MS χ2=5.1, p=0.02.
IA, inflammatory arthritis; IBD, inflammatory bowel disease; IMID, immune-mediated inflammatory disease; MS, multiple sclerosis; NC, nucleocapsid; RBD, receptor binding domain; S1, spike protein; SARD, systemic autoimmune rheumatic disease; V1, first vaccine; V2, second vaccine; V3, third vaccine; V4, fourth vaccine.
Post-V2 anti-S1 seroconversion rates for IMIDs were lower compared with those of age-matched and sex-matched controls (anti-S1 seropositive controls (363/370, 98.1%) vs IMIDs Χ2=14.5, p<0.0001) but similar for anti-NC (anti-NC seropositive controls (13/370, 3.5%) vs IMIDs χ2=2.9, p=0.1). Matched population-based estimates were not available for subsequent vaccinations.
Anti-RBD and anti-S1 IgG titres of those who seroconverted increased between the 1 month post-V1 and 1 month post-V2 time points for combined IMIDs and for each IMID individually (figure 1) (all p<0.0001). Anti-RBD and anti-S1 titres declined by 3 months after the second vaccine (p values for combined IMIDs p<0.0001, SARDs p<0.001, IBD p<0.001, IA p<0.001 and MS p<0.001) but increased 1 month after the third vaccine (all p<0.0001). Titres of anti-RBD and anti-S1 were similar between 1 month after the third vaccine and 1 month after the fourth vaccine. Within individuals, paired analysis of titres across visits yielded similar findings.
Figure 1.

Titres of anti-spike and anti-receptor binding domain IgG levels following first, second, third and fourth vaccinations: (A) All IMIDs, (B) IA, (C) SARDs, (D) IBD and (E) MS. Data for seroconverters only. IgG levels natural log-transformed (LN). Unadjusted p values: *p<0.0001, **p≤0.001, ***p≤0.00, ****p<0.05. IA, inflammatory arthritis; IBD, inflammatory bowel disease; IMIDs, immune-mediated inflammatory disease; MS, multiple sclerosis; RBD, receptor binding domain; SARD, systemic autoimmune rheumatic disease; V1, first vaccine; V2, second vaccine; V3, third vaccine; V4, fourth vaccine.
Over the study, 99 (30.6%) participants with IMID received heterologous/mixed vaccines for their first two vaccines (table 1). For those with 1-month post-V2 serology data, individuals receiving homologous vector vaccines had the lowest seroconversion rates and titres for both anti-RBD and anti-S1 responses. Individuals receiving either mRNA vaccine following a vector vaccine had comparable anti-RBD and anti-S1 titres as those receiving two mRNA vaccines (figure 2). Anti-RBD and anti-S1 seropositivity and titres 1 month following the third vaccine were similar among individuals receiving different combinations of vaccines for their first two vaccines (online supplemental table 2, online supplemental figure 4).
Figure 2.
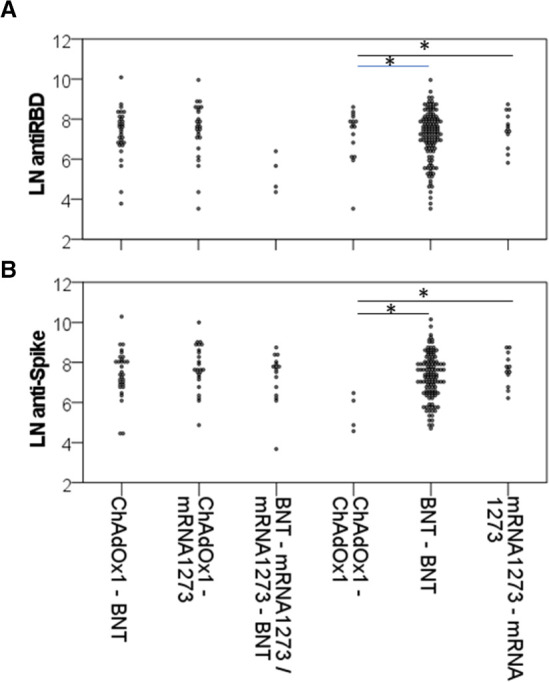
Titres of anti-spike and anti-RBD IgG levels 1 month following second vaccination by vaccine mixture: (A) log anti-RBD and (B) log anti-spike. Data for seroconverters only. IgG levels natural log-transformed (LN). Unadjusted p value: *p<0.01. BNT, BNT162b2; RBD, receptor binding domain.
Participants over 65 years of age, diagnosed with MS or taking biologics were less likely to seroconvert by the second vaccine in multivariable models (table 3). The results were similar if seroconversion was defined as seropositivity to anti-RBD and/or anti-S1. Vaccine mix (vector–mRNA vs mRNA–mRNA) did not impact seroconversion when included in the regression models. Most of the 20 individuals who did not seroconvert after the second vaccine were taking immunosuppressives (mycophenolate n=5, methotrexate n=2, azathioprine n=1) or biologics (B cell-targeting currently or previously n=8, anti-TNF n=2, other n=2) (online supplemental table 3).
Table 3.
Clinical variables associated with seroconversion 1 month following second vaccine
| Post second vaccine OR (95% CI) |
P value | |
| RBD seroconversion | ||
| Sex | ||
| Male | Ref | 1.0 |
| Female | 1.0 (0.21 to 4.71) | |
| Age (years) | ||
| >65 | Ref | 0.002 |
| ≤65 | 7.4 (2.04 to 27.06) | |
| IMID | ||
| IBD | Ref | <0.001 |
| IA | 0.2 (0.02 to 2.65) | |
| SARD | 0.05 (0.003 to 0.79) | |
| MS | 0.009 (0.001 to 0.13) | |
| Immune therapy | ||
| None | Ref | 0.004 |
| Other immunomodulator | NA | |
| Immunosuppressant | 0.03 (0.002 to 0.33) | |
| Biologic | 0.02 (0.002 to 0.16) | |
| S1 seroconversion | ||
| Sex | ||
| Male | Ref | 0.85 |
| Female | 1.1 (0.29 to 4.52) | |
| Age (years) | ||
| >65 | Ref | 0.02 |
| ≤65 | 3.9 (1.29 to 11.62) | |
| IMID | ||
| IBD | Ref | <0.001 |
| RA | 0.5 (0.07 to 3.02) | |
| SARD | 0.1 (0.01 to 0.91) | |
| MS | 0.03 (0.003 to 0.20) | |
| Immune therapy | ||
| None | Ref | 0.01 |
| Other immunomodulator | NA | |
| Immunosuppressant | 0.06 (0.006 to 0.51) | |
| Biologic | 0.04 (0.007 to 0.27) |
Biologics: tumour necrosis factor antagonists, abatacept, tocilizumab, tofacitinib, upadacitinib, ustekinumab, apremilast, rituximab, anakinra and B cell-targeted therapies (rituximab, belimumab, ocrelizumab); immunosuppressants: methotrexate, leflunomide and mycophenolate; immunomodulators: hydroxychloroquine and sulfasalazine.
IA, inflammatory arthritis; IBD, inflammatory bowel disease; IMID, immune-mediated inflammatory disease; MS, multiple sclerosis; NA, not able to compute; RBD, receptor binding domain; Ref, reference category; S1, spike protein; SARD, systemic autoimmune rheumatic disease.
We evaluated the impact of vaccine mix and treatment on waning of anti-SARS-CoV-2 titres between 1 and 3 months following the second vaccination. In paired analysis, the decline in titres between 1 month post-V2 and 3 months post-V2 for anti-RBD and anti-S1 differed across vaccine mixtures (anti-RBD p=0.026, anti-S1 p=0.02); however, this was mainly due to minimal titre changes for individuals receiving homologous vector vaccines who had lower titres overall. We observed greater titre change between those who received vector–mRNA and mRNA–mRNA combinations for S1, but did not see differences in RBD titre change between those who received vector–mRNA and those who received mRNA–mRNA combinations: median (IQR) anti-S1 mixed 1591.6 (3002.7) vs homologous mRNA 1086.3 (1608.8), p=0.021; anti-RBD mixed 1469.9 (2086.5) vs homologous mRNA 1124.5 (1402.4), p=0.051. For individuals receiving homologous mRNA (BNT162b2–BNT162b2 (BNT–BNT) vs mRNA1273–mRNA1273), there was no difference in waning for anti-RBD or anti-S1: RBD titre change anti-RBD: BNT–BNT 1080.6 (2405) vs mRNA1273–mRNA1273 1434.9 (2465.1), p=0.58; anti-S1 BNT–BNT 1051.9 (1674.1) vs mRNA1273–mRNA1273 1567.5 (2481.9), p=0.39. There was no difference in waning for individuals receiving homologous mRNA versus mixed vector–mRNA of the same type for anti-RBD or anti-S1. There was no difference in titre change across different biologic categories (anti-TNF vs Bell depletion vs other biologic; anti-RBD p=0.30, anti-S1 p=0.14) (online supplemental figure 5).
Of the participants, 25 were seropositive for anti-NC antibodies on at least one visit (8 IA, 8 SARDs, 3 MS, 6 IBD), and for 4 of these individuals seropositivity persisted with declining titres across consecutive visits, spanning 3–6 months. All but one participant with MS were also anti-RBD and anti-S1 seropositive. Anti-RBD and anti-S1 titres were higher in anti-NC positive compared with anti-NC negative samples: median (range; IQR): anti-RBD 11 755.3 (20 373.1) vs 1248.0 (27–78 936.2; 53 278.7); anti-S1 11 254.4 (77.3–68 157.0; 15 352.6) vs 1313.1 (37.4–87 401.3; 3106.6) (online supplemental figure 6). Of the 25 seropositive individuals, 9 were asymptomatic, 10 were taking biologics (5 anti-TNFs, 3 current or past B cell depletion, 4 other biologics/advanced therapies), 7 immunosuppressives (5 methotrexate, 2 azathioprine), 7 immunomodulating agents alone and 1 MS participant was on no IMID (online supplemental table 4). Although the rates of anti-NC positivity increased over the course of the study, anti-NC titres did not vary by vaccine status (heterologous or homologous) nor by date tested (table 2, online supplemental figure 7).
Most participants reported no COVID-19 infection symptoms during the study, including 9 individuals who tested seropositive for anti-NC antibodies, whereas 113 (35.7%) participants reported mild symptoms consistent with COVID-19 infection but did not have community-based confirmatory testing by either polymerase chain testing before December 2021 or self-administered testing after December 2021. All COVID-19 infections with positive community-based testing were also anti-NC positive. Only two confirmed COVID-19 infections required hospitalisation. Both had received three vaccines and had moderate levels of anti-NC (69.4 BAU/mL and 22.8 BAU/mL) (table 1).
Self-reported disease activity/status scores were similar across visits for each IMID (figure 3). Rates of moderate or severe self-reported IMID flares were similar across vaccines. Participants with MS and IBD had lower rates of self-reported flare compared with IA and SARDs (n/N (%) with self-reported flare after any vaccine: MS 5/129 (3.9), IA 38/195 (19.5), SARDs 50/202 (24.8), IBD 6/211 (2.8); χ2=72.9, p<0.001). IA and SARDs tended to have greater rates of self-reported flare (table 1).
Figure 3.

Disease activity before and after each vaccine: (A) inflammatory arthritis, (B) systemic autoimmune rheumatic disease, (C) inflammatory bowel disease and (D) multiple Sclerosis. EDSS, Expanded Disability Status Scale; IBDSI-SF, Inflammatory Bowel Disease Symptom Inventory-Short Form; RAPID-3, Routine Assessment of Patient Index Data 3; SLAQ, Systemic Lupus Activity Questionnaire; V1, first vaccine; V2, second vaccine; V3, third vaccine; V4, fourth vaccine.
Discussion
This single-centre cohort study evaluated the safety and immunogenicity of SARS-CoV-2 vaccines in IMIDs and confirmed relative safety with no increase in IMID disease activity despite self-reported disease flare rates of 12% following four vaccinations. Fewer than two-thirds seroconverted after the first vaccine. Seroconversion rates differed by vaccine type, with higher titres of anti-RBD and anti-S1 responses generated by mRNA vaccines compared with the available vector vaccine. Individuals who received an initial vector vaccine followed by an mRNA vaccine had vaccine-induced titres that were comparable to those following a homologous mRNA vaccine course and were higher than those who received homologous vector vaccines. Anti-SARS-CoV-2 antibody titres declined 3 months after the second vaccine but improved after the third and fourth vaccines. Most individuals who did not produce adequate humoral responses to the vaccine were taking immunosuppressants or biologics.
Our findings are consistent with emerging clinical trial and cohort data from the general population and other immunocompromised groups. Prior studies of rheumatic disease flare post-COVID-19 vaccination have produced mixed results; however, most found no major concerns.7 Data for IBD and MS are also reassuring.23 24 Several studies have found lower seroconversion rates and anti-SARS-CoV-2 titres in IMIDs compared with the general population.25 26 While older age plays a role, the primary reason for reduced responses appears due to medication use, with the greatest impact from biologics, especially B cell-depleting therapies, fingolimod, anti-TNF agents and Janus kinase inhibitors, and with conventional disease-modifying antirheumatic drugs (cDMARDs) such as mycophenolate and methotrexate. Hydroxychloroquine does not impair vaccine responses. Proposed strategies to optimise responses for patients on these medications include holding medication around the time of vaccination and delaying vaccination following infusion of B cell-targeted therapies.27 28 For B cell therapies, humoral immune responses remain suboptimal even after the third dose, especially for individuals with low prevaccination cell counts.29–31 Reassuringly, T cell responses are induced, although possibly impaired.26 31 32
Heterologous vaccine administration increased as vaccine availability and data on safety and immunogenicity evolved, thereby allowing evaluation of the role of homologous versus heterologous vaccine administration for people with IMIDs. In the general population, clinical trials and cohort studies of mixing vaccine types that compared homologous vector, homologous mRNA and heterologous vector–mRNA vaccine courses observed greater immune responses (humoral and cellular) with mRNA vaccines than vector vaccines, and that in individuals receiving a vector vaccine first an mRNA vaccine improved vaccine responses to levels comparable to those of homologous mRNA vaccines.12–14 33 Our observations in IMIDs confirm that second, and at least third, vaccination courses are needed to generate acceptable humoral immunogenicity, that mRNA vaccines can overcome limited responses to vector vaccines and that the type of mRNA administered has minimal impact on waning antibody titres following the second vaccination.
The clinical findings of this report reflect data collected during intermittent public health-mandated societal restrictions, before and during the early period when the Omicron variant was circulating in our region and before bivalent vaccines were available.11 Over one-third reported mild symptoms or were suspected to have had COVID-19 illness but less than 10% had confirmed COVID-19 infection. Despite complete vaccination, infection and concerning symptoms increased as public health restrictions were relaxed, the prevalence of SARS-CoV-2 virus increased and new variants of concern emerged. This emphasises the need for ongoing COVID-19 surveillance to inform personal health practices given the real concerns expressed by many people with IMIDs, even those who are fully vaccinated. Recent studies have described reduced sensitivity of the anti-NC assay following vaccination that is only partially explained by viral load.34 In this study, all participants with COVID-19 infection confirmed with community-based testing were also anti-NC positive, and while the number of anti-NC positive participants increased over the study we did not see any difference in anti-NC IgG levels with the number of vaccines or by calendar month.
We acknowledge limitations of this work. Our sample size was relatively small for each IMID; however, we have collected extensive patient-reported data combined with biologic samples from individuals representing four common IMID groups, allowing cross-disease and cross-specialty comparisons which are not widely reported. We assessed IMID disease activity using validated patient self-reported, disease-specific indices and flare questions, although these questionnaires can be subject to recall bias. Ideally patient-reported IMID activity would be supplemented with clinician-assessed measures; however, both patient preferences and COVID-19 pandemic travel restrictions impacted the feasibility of inperson clinical assessments for all participants. Self-reported disease activity/state measures correlate with clinical assessment measures.19 35–37 As expected for these IMIDs, our population was predominantly female; thus, we lack power to detect sex-based differences in our outcomes and there is uncertainty as to how they would reflect a male-predominant cohort. We focused on humoral vaccine-induced immunogenicity using antibody seropositivity and titres as surrogates for vaccine-induced protection. Antibody binding titres have been shown to correlate with neutralising and cellular responses, which in turn correlate with vaccine efficacy, although the titres needed to achieve good vaccine efficacy may differ for anti-S1 and anti-RBD.38 Further work is needed to evaluate the neutralisation capacity of vaccine-induced antibodies to SARS-CoV-2 and emerging variants of concern including Omicron. We did not evaluate cellular immune responses, yet these are critical for long-term antiviral protection especially for individuals without robust antibody responses. We were not able to confirm prior reports of the impact of different biologic categories on antibody titres; however, our study was not powered for this question. Additional studies are needed to evaluate if there are important differences across mRNA vaccines and vaccine intervals for optimal protection against variants of concern to inform recommendations for additional vaccinations in IMIDs. Importantly, it is still unclear what level of humoral or cellular immunogenicity is optimal to protect IMIDs against serious COVID-19 infection, although population-based vaccine efficacy data are emerging for some immunocompromised groups.39
We conclude that most individuals with IMID can safely receive COVID-19 vaccines without risk of disease flare. At least two doses that include an mRNA vaccine, either homologous or mixed vaccine types, are needed to generate humoral immunity comparable to the general population. The observed decline in humoral responses supports the use of third and subsequent vaccine doses for IMIDs. These data can be used to direct vaccine policies in countries where vaccine rates have been lagging or where supply has been limited.
Supplementary Material
Acknowledgments
We acknowledge the technical expertise of the NLHRS, including A Harris, R Fabia, K Cachero, H Ellis, S Simon, K Peladeau and J Walker, and the assistance of M Moyen, M Sevilla, S Nanayakkara, T Shcholok and J Remple.
Footnotes
Contributors: CAH contributed to study conceptualisation, funding acquisition, recruitment of participants, data curation, data analysis, writing of original and final manuscript drafts and is responsible for the overall content as the guarantor. CM contributed to data curation by conducting and analysing the SARS-CoV-2 assays and reviewed the draft manuscript. CNB and RAM contributed to study conceptualisation, funding acquisition, recruitment of participants, and both review and editing of the manuscript. CC contributed to the review and editing of the manuscript. SFO'B contributed resources including data for the controls, and both review and editing of the manuscript. JK contributed to study conceptualisation, funding acquisition, provided resources for conducting and interpreting the SARS-CoV-2 assays, and contributed to the review and editing of the manuscript. All authors contributed to critical review of the manuscript and approved the final version.
Funding: The study received funding from Research Manitoba. The Public Health Agency of Canada provided funding for the Kim lab. The study sponsors had no role in study design, data collection, analysis, interpretation, writing or in the decision to submit the manuscript.
Competing interests: CAH: unrelated grant funding from Pfizer; advisory board for AstraZeneca Canada for unrelated product; unrelated research funds from Research Manitoba, Health Science Center Foundation and International League of Associations for Rheumatology; and unrelated educational funds from the Royal College of Physicians and Surgeons of Canada. RAM: receives research funding from CIHR, Research Manitoba, Multiple Sclerosis Society of Canada, Multiple Sclerosis Scientific Foundation, Crohn’s and Colitis Canada, National Multiple Sclerosis Society, CMSC, Arthritis Society, Brain Canada, and US Department of Defense; coinvestigator on a study funded in part by Biogen Idec and Roche Canada; and supported by the Waugh Family Chair in Multiple Sclerosis. CNB: supported by the Bingham Chair in Gastroenterology; has served on advisory boards for AbbVie Canada, Amgen Canada, Bristol Myers Squibb Canada, Roche Canada, Janssen Canada, Sandoz Canada, Takeda Canada and Pfizer Canada; consultant for Mylan Pharmaceuticals and Takeda; educational grants from AbbVie Canada, Pfizer Canada, Takeda Canada and Janssen Canada; speaker’s panel for AbbVie Canada, Janssen Canada, Pfizer Canada and Takeda Canada; and received research funding from AbbVie Canada, Bristol Myers Squibb Canada, Sandoz Canada and Pfizer Canada. CC: receives grant funding from PHAC and CITF through internal research funding streams at PHAC. JK: receives grant funding from PHAC through internal research funding streams at PHAC.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Not required.
Ethics approval
This study involves human participants and was approved by the University of Manitoba Health Research Ethics Board (HS24647-H2021-005), Manitoba Shared Health (SH2021:009), and Health Canada and Public Health Agency of Canada Research Ethics Board (REB 2021-018P). Participants gave informed consent to participate in the study before taking part.
References
- 1. Krammer F. SARS-Cov-2 vaccines in development. Nature 2020;586:516–27. 10.1038/s41586-020-2798-3 [DOI] [PubMed] [Google Scholar]
- 2. Baden LR, El Sahly HM, Essink B, et al. Efficacy and safety of the mRNA-1273 SARS-Cov-2 vaccine. N Engl J Med 2021;384:403–16. 10.1056/NEJMoa2035389 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med 2020;383:2603–15. 10.1056/NEJMoa2034577 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Falsey AR, Sobieszczyk ME, Hirsch I, et al. Phase 3 safety and efficacy of Azd1222 (Chadox1 nCoV-19) COVID-19 vaccine. N Engl J Med 2021;385:2348–60. 10.1056/NEJMoa2105290 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. El-gabalawy H, Guenther LC, Bernstein CN. Epidemiology of immune-mediated inflammatory diseases: incidence, prevalence, natural history, and Comorbidities. The Journal of Rheumatology Supplement 2010;85:2–10. 10.3899/jrheum.091461 [DOI] [PubMed] [Google Scholar]
- 6. Maddur MS, Vani J, Lacroix-Desmazes S, et al. Autoimmunity as a predisposition for infectious diseases. PLoS Pathog 2010;6:e1001077. 10.1371/journal.ppat.1001077 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Grainger R, Kim AHJ, Conway R, et al. COVID-19 in people with rheumatic diseases: risks, outcomes, treatment considerations. Nat Rev Rheumatol 2022;18:191–204. 10.1038/s41584-022-00755-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Conway R, Grimshaw AA, Konig MF, et al. SARS-Cov-2 infection and COVID-19 outcomes in rheumatic diseases: A systematic literature review and meta-analysis. Arthritis Rheumatol 2022;74:766–75. 10.1002/art.42030 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Schiavetti I, Ponzano M, Signori A, et al. Severe outcomes of COVID-19 among patients with multiple sclerosis under anti-CD-20 therapies: A systematic review and meta-analysis. Multiple Sclerosis and Related Disorders 2022;57:103358. 10.1016/j.msard.2021.103358 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Tripathi K, Godoy Brewer G, Thu Nguyen M, et al. COVID-19 and outcomes in patients with inflammatory bowel disease: systematic review and meta-analysis. Inflamm Bowel Dis 2022;28:1265–79.:izab236. 10.1093/ibd/izab236 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Aboulatta L, Kowalec K, Delaney J, et al. Trends of COVID-19 incidence in Manitoba and public health measures: March 2020 to February 2022. BMC Res Notes 2022;15:162. 10.1186/s13104-022-06049-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Borobia AM, Carcas AJ, Pérez-Olmeda M, et al. Immunogenicity and Reactogenicity of BNT162b2 booster in Chadox1-S-primed participants (Combivacs): a Multicentre, open-label, randomised, controlled, phase 2 trial. The Lancet 2021;398:121–30. 10.1016/S0140-6736(21)01420-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Barros-Martins J, Hammerschmidt SI, Cossmann A, et al. Immune responses against SARS-Cov-2 variants after heterologous and Homologous Chadox1 nCoV-19/BNT162b2 vaccination. Nat Med 2021;27:1525–9. 10.1038/s41591-021-01449-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Schmidt T, Klemis V, Schub D, et al. Immunogenicity and Reactogenicity of heterologous Chadox1 nCoV-19/mRNA vaccination. Nat Med 2021;27:1530–5. 10.1038/s41591-021-01464-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Information CIfH . Guidance on the Use of Standards for Race-Based and Indigenous Identity Data Collection and Health Reporting in Canada. Ottawa, ON, 2022. [Google Scholar]
- 16. Johnson TM, Michaud K, England BR. Measures of rheumatoid arthritis disease activity. Arthritis Care Res 2020;72:4–26. 10.1002/acr.24336 Available: https://onlinelibrary.wiley.com/toc/21514658/72/S10 [DOI] [PubMed] [Google Scholar]
- 17. Arora S, Isenberg DA, Castrejon I. Measures of adult systemic lupus erythematosus: disease activity and damage. Arthritis Care Res 2020;72:27–46. 10.1002/acr.24221 Available: https://onlinelibrary.wiley.com/toc/21514658/72/S10 [DOI] [PubMed] [Google Scholar]
- 18. Witges K, Sexton K, Graff LA, et al. What is a flare? the Manitoba living with IBD study. Inflamm Bowel Dis 2022;28:862–9. 10.1093/ibd/izab192 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Sexton KA, Walker JR, Targownik LE, et al. The inflammatory bowel disease symptom inventory: A patient-report scale for research and clinical application. Inflamm Bowel Dis 2019;25:1277–90. 10.1093/ibd/izz038 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 1983;33:1444–52. 10.1212/wnl.33.11.1444 [DOI] [PubMed] [Google Scholar]
- 21. Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (Redcap) – A Metadata-driven methodology and Workflow process for providing Translational research Informatics support J Biomed inform. J Biomed Inform 2009;42:377–81. 10.1016/j.jbi.2008.08.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Cholette F, Mesa C, Harris A, et al. Dried blood spot specimens for SARS-Cov-2 antibody testing: A multi-site, multi-assay comparison. PLoS One 2021;16:e0261003. 10.1371/journal.pone.0261003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Botwin GJ, Li D, Figueiredo J, et al. Adverse events after SARS-Cov-2 mRNA vaccination among patients with inflammatory bowel disease. Am J Gastroenterol 2021;116:1746–51. 10.14309/ajg.0000000000001342 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Ciampi E, Uribe-San-Martin R, Soler B, et al. Safety and humoral response rate of Inactivated and mRNA vaccines against SARS-Cov-2 in patients with multiple sclerosis. Mult Scler Relat Disord 2022;59:103690.:S2211-0348(22)00205-X. 10.1016/j.msard.2022.103690 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Jena A, Mishra S, Deepak P, et al. Response to SARS-Cov-2 vaccination in immune mediated inflammatory diseases: systematic review and meta-analysis. Autoimmun Rev 2022;21:102927.:S1568-9972(21)00202-0. 10.1016/j.autrev.2021.102927 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Tortorella C, Aiello A, Gasperini C, et al. Humoral- and T-cell-specific immune responses to SARS-Cov-2 mRNA vaccination in patients with MS using different disease-modifying therapies. Neurology 2022;98:e541–54. 10.1212/WNL.0000000000013108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Skaria TG, Sreeprakash A, Umesh R, et al. Withholding methotrexate after vaccination with Chadox1 Ncov19 in patients with rheumatoid or Psoriatic arthritis in India (MIVAC I and II): results of two, parallel, assessor-masked, randomised controlled trials. The Lancet Rheumatology 2022;4:e755–64. 10.1016/S2665-9913(22)00228-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Curtis JR, Johnson SR, Anthony DD, et al. American college of rheumatology guidance for COVID-19 vaccination in patients with rheumatic and musculoskeletal diseases: version 3. Arthritis & Rheumatology 2021;73:e60–75. 10.1002/art.41928 Available: https://onlinelibrary.wiley.com/toc/23265205/73/10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Bajwa HM, Novak F, Nilsson AC, et al. Persistently reduced humoral and sustained cellular immune response from first to third SARS-Cov-2 mRNA vaccination in anti-Cd20-treated multiple sclerosis patients. Mult Scler Relat Disord 2022;60:103729.:S2211-0348(22)00244-9. 10.1016/j.msard.2022.103729 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Stefanski A-L, Rincon-Arevalo H, Schrezenmeier E, et al. B cell numbers predict humoral and cellular response upon SARS-Cov-2 vaccination among patients treated with Rituximab. Rheumatology [Preprint] 2021. 10.1101/2021.07.19.21260803 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Jyssum I, Kared H, Tran TT, et al. Humoral and cellular immune responses to two and three doses of SARS-Cov-2 vaccines in Rituximab-treated patients with rheumatoid arthritis: a prospective, cohort study. The Lancet Rheumatology 2022;4:e177–87. 10.1016/S2665-9913(21)00394-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Apostolidis SA, Kakara M, Painter MM, et al. Cellular and humoral immune responses following SARS-Cov-2 mRNA vaccination in patients with multiple sclerosis on anti-Cd20 therapy. Nat Med 2021;27:1990–2001. 10.1038/s41591-021-01507-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Stuart ASV, Shaw RH, Liu X, et al. Immunogenicity, safety, and Reactogenicity of heterologous COVID-19 primary vaccination incorporating mRNA, viral-vector, and protein-adjuvant vaccines in the UK (Com-Cov2): a single-blind, randomised, phase 2, non-inferiority trial. The Lancet 2022;399:36–49. 10.1016/S0140-6736(21)02718-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Follmann D, Janes HE, Buhule OD, et al. Antinucleocapsid antibodies after SARS-Cov-2 infection in the blinded phase of the randomized, placebo-controlled mRNA-1273 COVID-19 vaccine efficacy clinical trial. Ann Intern Med 2022;175:1258–65. 10.7326/M22-1300 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Pincus T, Yazici Y, Bergman MJ. Rapid3, an index to assess and monitor patients with rheumatoid arthritis, without formal joint counts: similar results to Das28 and CDAI in clinical trials and clinical care. Rheumatic Disease Clinics of North America 2009;35:773–8. 10.1016/j.rdc.2009.10.008 [DOI] [PubMed] [Google Scholar]
- 36. Svenungsson E, Gunnarsson I, Illescas-Bäckelin V, et al. Quick systemic lupus activity questionnaire (Q-SLAQ): a simplified version of SLAQ for patient-reported disease activity. Lupus Sci Med 2021;8:e000471. 10.1136/lupus-2020-000471 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Koch MW, Mostert JP, Wolinsky JS, et al. Comparison of the EDSS, timed 25-foot walk, and the 9-hole peg test as clinical trial outcomes in Relapsing-Remitting multiple sclerosis. Neurology 2021;97:e1560–70. 10.1212/WNL.0000000000012690 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Feng S, Phillips DJ, White T, et al. Correlates of protection against symptomatic and asymptomatic SARS-Cov-2 infection. Nat Med 2021;27:2032–40. 10.1038/s41591-021-01540-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Widdifield J, Kwong JC, Chen S, et al. Vaccine effectiveness against SARS-Cov-2 infection and severe outcomes among individuals with immune-mediated inflammatory diseases. Lancet Rheumatology 2022. 10.1016/S2665-9913(22)00096-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2022-071397supp001.pdf (1.9MB, pdf)
Data Availability Statement
All data relevant to the study are included in the article or uploaded as supplementary information.