

Dear Editor,
A 19-year-old male without any known illnesses presented with slowly enlarging asymptomatic plaques over his right cheek, noticed since the age of 4 years. On examination, there were grouped well-defined dull red-brownish, soft, compressible, non-tender papules and plaques of size ranging from 1.5 × 1 cm to 4 × 3 cm over the right pre-auricular area, with smaller lesions extending onto the right post-auricular area and upper neck. There was loss of hair on the skin overlying these plaques and a separate linear band of non-scarring alopecia below these plaques, running obliquely across the right mandible [Figure 1]. The right temple and the upper cheek appeared depressed, producing mild facial asymmetry. Examination of the left side of the head and neck was unremarkable. A skin biopsy from one of the plaques showed an ill-defined spindle cell proliferation with a loose myxoid stroma in the mid- and deep dermis [Figure 2a], encasing the hair follicles and arrector pili muscle [Figure 2b]. The nuclei of the spindle cells were short and wavy [Figure 2c]. These histological features were those of a diffuse neurofibroma, which was further confirmed by positive immunohistochemistry for S-100 [Figure 2d]. Biopsy from the linear band of alopecia was histologically unremarkable. A non-contrast computerized tomographic scan of the head showed a nodular thickening of the skin and subcutaneous tissue in the right cheek and temporal region. The underlying mandibular condyle, ramus, coronoid process, and body of the right hemimandible were hypoplastic compared to the opposite side. The right zygomatic arch and pterygoid plates also appeared smaller and thinned out [Figure 3]. An ophthalmological evaluation revealed Lisch nodules in both eyes. There were no café-au-lait macules, axillary, inguinal, or palmar freckling, or any other bony deformity. Family history was negative. Based on these findings, a diagnosis of diffuse neurofibroma, with hypoplasia of ipsilateral mandible and zygomatic arch, and Lisch nodules (Neurofibromatosis 1) was made, and the patient was referred to the plastic surgery department.
Figure 1.
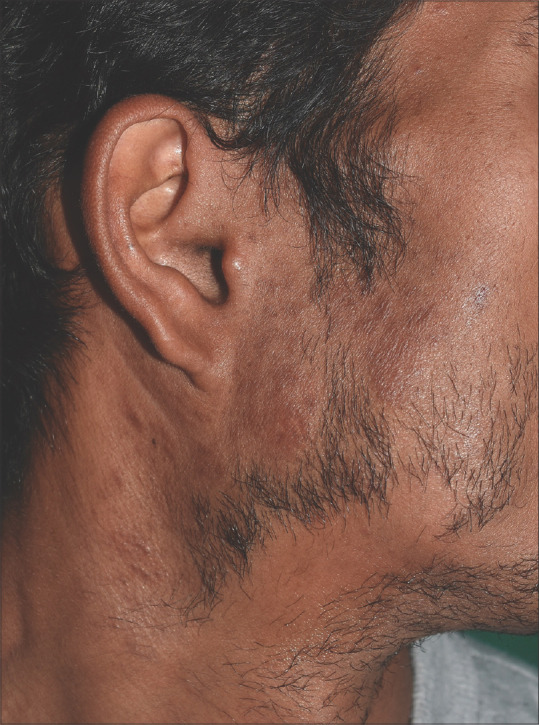
Grouped, well-defined, dull red, soft, compressible, non-tender papules and plaques with overlying alopecia over the right preauricular area and upper neck
Figure 2.

(a) Ill-defined spindle cell proliferation with a loose myxoid stroma in the mid- and deep dermis (40x). (b) Spindle cell proliferation encasing the hair follicles and arrector pili muscle (100x). (c) The nuclei of the spindle cells are short and wavy (200x). (d) Spindle cells showing positive immunohistochemistry for S-100 (200x)
Figure 3.

(a) Non-contrast computerized tomographic scan of the head: Coronal maximum-intensity projection bone window image shows hypoplasia of condyle and ramus of right hemimandible. (b) Volume rendering technique image shows hypoplasia of right hemimandible and thinning of the right zygomatic arch
Neurofibromas can be classified into three types, namely localized, plexiform, and diffuse. Of these, localized and plexiform neurofibromas are well-characterized, while diffuse neurofibroma is a rare and unusual variant.
Diffuse neurofibroma clinically presents as a single gradually progressive dermal and/or subcutaneous plaque in children and young adults. Although classically reported to occur on the head and neck region, other sites such as trunk and extremities can also be affected. Histopathologically, it shows a neural proliferation occupying the dermis and subcutaneous tissue, with an infiltrative growth pattern enveloping, but not destroying, the normal adnexal structures such as hair follicles; this finding may explain the alopecia overlying diffuse neurofibromas that was seen in our case and has been reported previously as well.[1-4] Meissner bodies are characteristic, but not always present.
About 10% of diffuse neurofibromas may be associated with neurofibromatosis type 1. A higher incidence of 61% was reported by Megahed et al. in their series of 13 patients with diffuse neurofibroma.[5] Our patient satisfied the criteria for neurofibromatosis type 1 as he also had bony hypoplasia and Lisch nodules in both eyes. An argument could also be made for the diagnosis of segmental neurofibromatosis, given the clustering of diffuse neurofibromas on one side of the face.
Malignant transformation of neurofibromas is rare. The risk is more in patients with associated neurofibromatosis, particularly in plexiform neurofibromas. The reported prevalence of malignant peripheral nerve sheath tumors in NF-1 is 2–13%, as compared to 0.001% in the general population.[6] However, we did not come across any reports of malignant transformation in diffuse neurofibromas.
The main differential diagnosis of facial plaques with overlying hair loss includes tuberculoid leprosy and alopecia mucinosa; however, these are typically not unilateral or grouped as was seen in our patient. Diffuse neurofibroma may be added to the list of differential diagnoses of alopecic plaques affecting the head and neck region.
To conclude, diffuse neurofibroma is a rare neurofibroma variant with distinctive histological features. Through this case, we wish to increase the awareness among our colleagues about this unusual entity. Overlying alopecia may be a clue to the clinical diagnosis. Patients should be screened for associated systemic features.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Kumar BS, Gopal MG, Talwar A, Ramesh M. Diffuse neurofibroma of the scalp presenting as circumscribed alopecic patch. Int J Trichology. 2010;2:60. doi: 10.4103/0974-7753.66919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Macias VC, Rafael M, Fernandes C, Rosa JC. Diffuse neurofibroma - an uncommon cause of alopecia. An Bras Dermatol. 2013;88:166–9. doi: 10.1590/abd1806-4841.20132170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lee IT, Chang JM, Fu Y. Diffuse neurofibroma:An uncommon cause of alopecia. Skin Appendage Disord. 2020;6:151–4. doi: 10.1159/000505438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sritanyarat T, Thanomkitti K. Diffuse neurofibroma of the scalp with alopecia:A case report. Thai J Dermatol. 2019;35:49–54. [Google Scholar]
- 5.Megahed M. Histopathological variants of neurofibroma. A study of 114 lesions. Am J Dermatopathol. 1994;16:486–95. doi: 10.1097/00000372-199410000-00003. [DOI] [PubMed] [Google Scholar]
- 6.Ducatman BS, Scheithauer BW, Piepgras DG, Reiman HM, Ilstrup DM. Malignant peripheral nerve sheath tumors. A clinicopathologic study of 120 cases. Cancer. 1986;57:2006–21. doi: 10.1002/1097-0142(19860515)57:10<2006::aid-cncr2820571022>3.0.co;2-6. [DOI] [PubMed] [Google Scholar]