

Abstract
Chondroid syringomas are rare, benign tumors originating from sweat glands occurring as singular lesions of the head and neck. This case report presents a patient in whom multiple chondroid syringoma lesions were found. Thus illuminating the possibility for such occurrences in the future of which physicians should be aware.
Keywords: Chondroid syringoma, Mixed tumor, Pleomorphic adenoma, Sweat gland, Head, Neck
Introduction
Chondroid syringomas (CS) are rare, benign cutaneous mixed tumors derived from sweat glands. These tumors manifest as firm, well-circumscribed masses located within the dermis and subcutis. CS are infrequent and unusual diagnoses about which exist a paucity of literature. Within the literature that does exist, CS are invariably reported to be solitary lesions. The original description of CS was even, in part, dependent upon there being no more than a single identifiable lesion [1]. As such, there do not appear to be any cases in the literature detailing the presentation of multifocal CS found on a singular patient prior to this case. This case report will elaborate on the presentation of a patient who was diagnosed with multiple CS of the face.
Case Presentation
A 54-year-old woman presented with painful facial masses in the right malar region with slowly, but progressively worsening symptoms. On physical examination, a 2-cm, firm subcutaneous mass was palpated around the nasolabial fold. The mass was tender to palpation. There were two additional subcutaneous masses measuring 2 cm and 1.5 cm overlying the right masseter muscle. Nasal endoscopy revealed a 1.5-cm submucosal mass emanating from the right anterior septum. Computed tomography (CT) revealed a heterogenous soft tissue mass superficial to the right premaxilla, measuring 1.9 × 1.4 × 2.3 cm, and exhibiting no evidence of bone invasion (Fig. 1A). CT imaging also revealed two round, soft tissue masses superficial to the right masseter muscle, measuring 2.0 × 1.4 × 1.4 cm and 1.5 × 1.1 × 1.0 cm (one visualized in Fig. 1A). Another mass, measuring 1.4 × 1.0 × 1.4 cm, was noted on the right anterior nasal septum, associated with leftward deviation of the septum (Fig. 1B). Pre-surgical fine needle aspiration of the right nasolabial mass was reported as a neoplasm of uncertain etiology and complete excision was recommended. A discussion was had with the patient about the unclear origin of the nasolabial mass as well as the findings on CT of multiple other masses. The patient elected for surgical removal of the lesions. Surgical excision of all masses was performed and full recovery was expected. At follow up, the patient reported complete resolution of previous symptoms. Microscopic evaluation of each excised mass revealed multiple CS—otherwise known as benign mixed tumors—morphologically identical to pleomorphic adenomas that arise from salivary glands. No major or minor salivary gland tissue was present in any of the specimens in this case. Thereby ruling out pleomorphic adenomas from the differential diagnosis in favor of CS. Histologically, the tumors displayed bland epithelial and myoepithelial cells intermixed with chondromyxoid stroma (Fig. 2) typical of a CS [2, 4]. One of the skin-based tumors showed clear-cut histologic evidence of origination from skin adnexa (i.e. eccrine glands).
Fig. 1.

Axial view of Computed Tomography images. A Nasolabial mass & Right cheek mass and B Mass on right anterior nasal septum
Fig. 2.
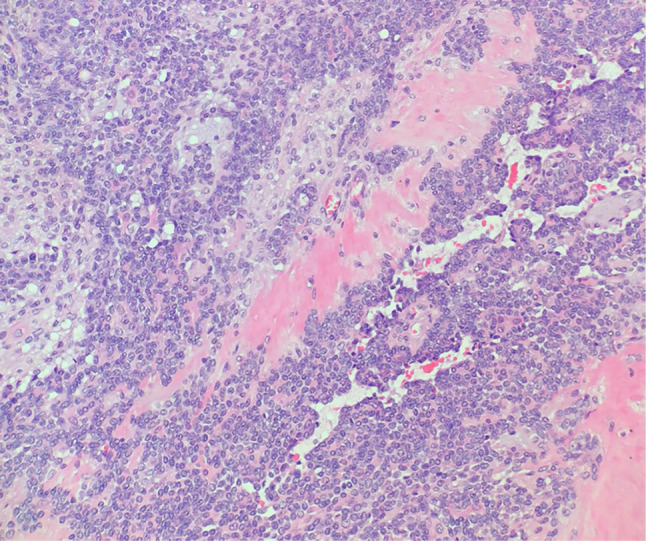
Histomicrograph of one of the excised chondroid syringomas (hematoxylin–eosin stain; original magnification × 200)
Discussion
Chondroid syringomas are rare adnexal skin lesions with a predilection for the nose, cheeks, and lips [2, 3, 5]. They are histologically identical to pleomorphic adenomas, containing a combination of epithelial and mesenchymal tissues, but derive from sweat glands [5]. Clinically, they present as firm, intradermal or subcutaneous nodules, requiring biopsy and histologic examination for definitive diagnosis [3]. CS comprise < 1% of all known skin lesions. They occur with higher incidence in males than females, are most prevalent in persons of middle and older age, though they have been documented to occur in other age groups, and have an indolent clinical course. Definitive treatment involves complete tumor excision [2]. The sporadic and infrequent nature of CS lesions has made it difficult to determine if there are specific causes or risk factors of the lesions. Furthermore, the available literature has not elaborated on the existence of any known risk factors. One might expect that a plurality of CS lesions would warrant additional concern for management and treatment. However complete excision is curative. Therefore, complete excision of all lesions with close follow up to assess for recurrence is still the ideal mode of treatment in a patient with multiple chondroid syringomas.
Historically, patients have presented with an isolated CS lesion largely confined to the head and neck with some reports of patients experiencing these benign lesions in other body regions, such as the thigh or shoulder [6, 7]. Current literature, prior to this article, has yet to identify any patient with multiple CS lesions. Our patient’s presentation of multiple simultaneous lesions clinically presenting as benign CS and histologically diagnosed as CS lesions sheds light on the possibility of such an occurrence. Thus, CS should be considered in the differential diagnosis in a patient presenting with multiple skin lesions. They should not be ruled out of a differential diagnosis solely on the basis of there being more than one presenting lesion since, as this case report demonstrates, it is possible for multiple CS lesions to be present contrary to previous belief.
Declarations
Conflict of interest
The authors have no conflicts of interest to report, including financial or non-financial interests that may otherwise be directly or indirectly related to this work.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Hirsch P, Helwig EB. Chondroid syringoma. Mixed tumor of skin, salivary gland type. Arch Dermatol. 1961;84:835–47. doi: 10.1001/archderm.1961.01580170129018. [DOI] [PubMed] [Google Scholar]
- 2.Ayala-Cortes A, Martinez-Cabriales S, Vazquez-Martinez O, et al. Chondroid syringoma: a challenging clinical diagnosis. J Am Acad Dermatol. 2015;72(5):AB42. doi: 10.1016/j.jaad.2015.02.178. [DOI] [Google Scholar]
- 3.Bekerecioglu M, Tercan M, Karakok M, Atik B. Benign chondroid syringoma: a confusing clinical diagnosis. Eur J Plast Surg. 2002;25:316–318. doi: 10.1007/s00238-002-0385-5. [DOI] [Google Scholar]
- 4.Sundling RA, So E, Logan DB. Chondroid syringoma. Foot Ankle Spec. 2017;10(2):167–169. doi: 10.1177/1938640016666927. [DOI] [PubMed] [Google Scholar]
- 5.Pal S, Sengupta S, Jana S, Bose K. Fine-needle aspiration cytology of chondroid syringoma of fore arm: report of a rare case. J Cytol Indian Acad Cytol. 2014;31(3):171–3. doi: 10.4103/0970-9371.145659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sulochana S, Manoharan M. Chondroid syringoma-an unusual presentation. J Clin Diagn Res. 2014;8(7):FD13–4. doi: 10.7860/JCDR/2014/7567.4627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sungur N, Uysal A, Gümüş M, Koçer U. An unusual chondroid syringoma. Dermatol Surg. 2003;29(9):977–979. [PubMed] [Google Scholar]