

Reason for posting: Health professionals are being warned of potentially fatal myocarditis, cardiomyopathy and heart failure associated with the antipsychotic drug clozapine.1 Clozapine-associated myocarditis has been previously estimated to occur at rates ranging from 1 in 10 0002 to 1 in 5003 patients. The drug's manufacturer has reported 213 international cases of myocarditis (including 50 deaths), 85% of which developed in the first 2 months of therapy.1 Most of the patients were prescribed the drug in recommended doses. Forty percent were under 30 years of age (64% under 49). In Canada 16 cases (including 3 deaths) of myocarditis, pericarditis or pericardial effusion have been reported, some occurring as early as 2 weeks after the start of treatment; patients were 19–37 years of age. Consistent with previous studies3 many of the international cases occurred in the presence of cardiac and peripheral blood eosinophilia, which indicates a possible IgE-mediated hypersensitivity reaction.1,3
There have been 178 international reports (including 32 deaths) of clozapine-associated cardiomyopathy; 7 cases occurred in Canada.1 Most (80%) of the patients in the international cases were under 50 years of age. Cardiomyopathy has occurred more often in clozapine-treated patients than in similar patients in the general population not taking clozapine for their illness.1,3 Dilated cardiomyopathy accounted for two-thirds of the cases and over one-third of deaths from cardiomyopathy.1 From a small number of cases in which follow-up data were provided, there is some evidence that withdrawal of the drug may result in improvement of the cardiomyopathy.1
Myocardial infarction has been reported in Canada in 30 clozapine-treated patients, 15 of whom died; however, no causal link to the drug has been firmly established.1
The drug: Clozapine is a dibenzodiazepine antipsychotic with strong affinity for D4-dopaminergic receptors and potent serotonergic, noradrenergic,3 histamine4 and cholinergic M2 receptor5 blocking ability. It differs from traditional antipsychotic drugs in that it has relatively weak D2-receptor activity and few extrapyramidal side effects, and it is effective in treating resistant schizophrenia.2,4
A common and serious adverse effect requiring regular hematologic monitoring is agranulocytosis, occurring in about 1% of patients in the first year of treatment.4,6 Other severe adverse reactions include seizures,4 venous thromboembolism,7 and severe hyperglycemia and diabetic ketoacidosis in previously nonobese, nondiabetic patients.8,9 Physicians should be aware of the challenge of distinguishing the signs and symptoms of myocarditis from more common, benign changes that can accompany rapid changes in dose, including tachycardia (occurring in about 25% of patients), lethargy and orthostatic hypotension.4
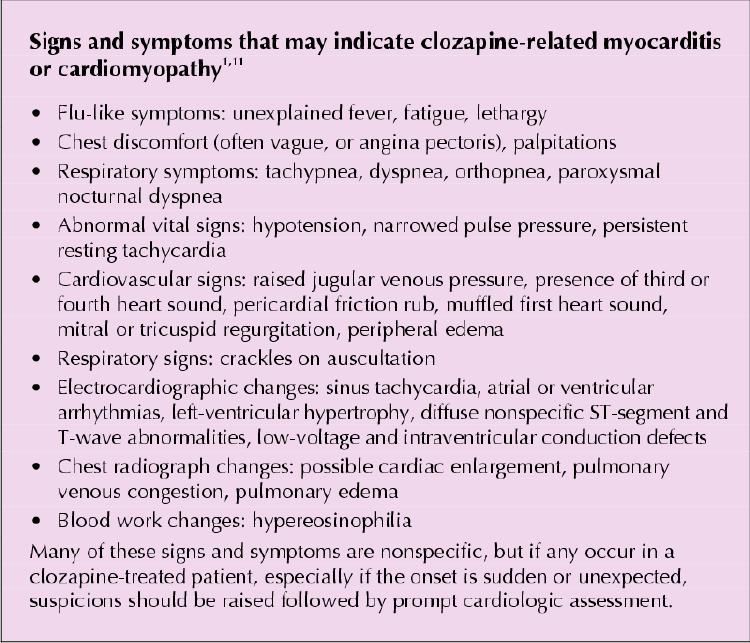
What to do: Patients should be warned of these uncommon but potentially fatal cardiovascular adverse effects associated with clozapine. Before treatment, a cardiac evaluation should be considered for patients with a personal or family history of heart disease; clozapine is contraindicated in patients with severe cardiac disease. Although patients are at greatest risk in the first month of therapy, the risk may persist as long as they are taking the drug. Clinicians caring for schizophrenic patients who are taking clozapine should maintain a high degree of suspicion if signs or symptoms consistent with cardiac toxicity develop (see side box). The drug should promptly and permanently be stopped in patients with myocarditis; discontinuation of the drug should be considered in patients with cardiomyopathy. Bayesian analyses of data from several international adverse reaction databases suggest that other antipsychotic drugs may also be associated with episodes of myocarditis or cardiomyopathy, but not to the same degree as clozapine.10
Box 1.
Eric Wooltorton Editorial Fellow, CMAJ
References
- 1.Association of Clozaril (clozapine) with cardiovascular toxicity [Dear Healthcare Professional letter]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2002 Jan 14. Available: www.hc-sc.gc.ca/hpb-dgps/therapeut/zfiles/english/advisory/industry/clozaril_e.html (accessed 2002 Mar 29).
- 2.Warner B, Alphs L, Schaedelin J, Koestler T. Clozapine and sudden death [letter]. Lancet 2000;355:842. [DOI] [PubMed]
- 3.Kilian JG, Kerr K, Lawrence C, Celermajer DS. Myocarditis and cardiomyopathy associated with clozapine. Lancet 1999;354:1841-5. [DOI] [PubMed]
- 4.Clozaril (clozapine tablets) [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc; 2000 Jun 16.
- 5.Devarajan S, Kutcher SP, Dursun SM. Clozapine and sudden death [letter]. Lancet 2000;355:841. [DOI] [PubMed]
- 6.Alvir JM, Lieberman JA, Safferman AZ, Schwimmer JL, Schaaf JA. Clozapine induced agranulocytosis: incidence and risk factors in the United States. N Engl J Med 1993;329:162-7. [DOI] [PubMed]
- 7.Hagg S, Spigset O, Soderstrom TG. Association of venous thromboembolism and clozapine. Lancet 2000;355:1155-6. [DOI] [PubMed]
- 8.Chan NN. Clozapine and sudden death [letter]. Lancet 2000;355:841-2. [DOI] [PubMed]
- 9.Griffiths J, Springuel P. Atypical antipsychotics: impaired glucose metabolism. Can Adverse Drug Reaction Newsl 2001;11(4):2-3. [Also in CMAJ 2001; 165(7):943-4]. [PubMed]
- 10.Coulter DM, Bate A, Meyboom RHB, Lindquist M, Edwards IR. Antipsychotic drugs and heart muscle disorder in international pharmacovigilance: data mining study. BMJ 2001; 322: 1207-9. [DOI] [PMC free article] [PubMed]
- 11.Wynne J, Braunwald E. The cardiomyopathies and myocarditides. In: Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL, editors. Harrison's principles of internal medicine. 15th ed. New York: McGraw-Hill; 2001. p. 1359-65.