

Abstract
Background
Many patients hospitalized for COVID-19 experience prolonged symptoms months after discharge. Little is known abou t patients’ personal experiences recovering from COVID-19 in the United States (US), where medically underserved populations are at particular risk of adverse outcomes.
Objective
To explore patients’ perspectives on the impact of COVID-19 hospitalization and barriers to and facilitators of recovery 1 year after hospital discharge in a predominantly Black American study population with high neighborhood-level socioeconomic disadvantage.
Design
Qualitative study utilizing individual, semi-structured interviews.
Participants
Adult patients hospitalized for COVID-19 approximately 1 year after discharge home who were engaged in a COVID-19 longitudinal cohort study.
Approach
The interview guide was developed and piloted by a multidisciplinary team. Interviews were audio-recorded and transcribed. Data were coded and organized into discrete themes using qualitative content analysis with constant comparison techniques.
Key Results
Of 24 participants, 17 (71%) self-identified as Black, and 13 (54%) resided in neighborhoods with the most severe neighborhood-level socioeconomic disadvantage. One year after discharge, participants described persistent deficits in physical, cognitive, or psychological health that impacted their current lives. Repercussions included financial suffering and a loss of identity. Participants reported that clinicians often focused on physical health over cognitive and psychological health, an emphasis that posed a barrier to recovering holistically. Facilitators of recovery included robust financial or social support systems and personal agency in health maintenance. Spirituality and gratitude were common coping mechanisms.
Conclusions
Persistent health deficits after COVID-19 resulted in downstream consequences in participants’ lives. Though participants received adequate care to address physical needs, many described persistent unmet cognitive and psychological needs. A more comprehensive understanding of barriers and facilitators for COVID-19 recovery, contextualized by specific healthcare and socioeconomic needs related to socioeconomic disadvantage, is needed to better inform intervention delivery to patients that experience long-term sequelae of COVID-19 hospitalization.
Supplementary Information
The online version contains supplementary material available at 10.1007/s11606-023-08246-9.
KEY WORDS: COVID-19, outcomes, recovery, qualitative research, health disparities
INTRODUCTION
For many patients experiencing severe COVID-19, hospital discharge is only the first step in recovery. Nearly half of those hospitalized with COVID-19 experience prolonged physical, cognitive, or psychological symptoms such as fatigue, dyspnea, memory loss, anxiety, or depression lasting at least 1 year after their initial diagnosis.1 Longitudinal cohort studies have increased our understanding of the broad range of persistent symptoms and their prevalence in different populations.2–4 The emergence of post-acute sequelae of COVID-19, commonly called “long COVID,” has been described across the spectrum of people infected with COVID-19, from those with very mild acute disease to those with life-threatening critical illness.5 However, patients’ perspectives on how COVID-19 hospitalization and persistent symptoms impact their daily lived experience are less well understood.
Prior qualitative studies on COVID-19, all conducted outside the United States (US), have suggested unique challenges for COVID-19 survivors in their physical, cognitive, and psychological recovery.6–8 Many characteristics of the US healthcare system are likely to introduce healthcare access, healthcare delivery, and multiple post-hospitalization challenges for patients, especially for racially and ethnically minoritized populations that experience COVID-19.9 However, few previous qualitative studies have highlighted the experiences of minoritized patients recovering from COVID-19. To address this gap in the literature, we aimed to explore the perspectives of a predominantly Black American population that survived a COVID-19 hospitalization and identify barriers to and facilitators of recovery 1 year following hospital discharge.
METHODS
Design
We conducted an exploratory qualitative study. We report this study in accordance with the Consolidated Reporting of Qualitative Research checklist (Appendix A).10 The University of Pennsylvania’s Institutional Review Board approved this study.
Setting and Participants
Participants were recruited from those already enrolled in the Molecular Epidemiology of Severe Sepsis in the ICU COVID-19 (MESSI-COVID) study, a prospective cohort study of adult survivors of severe COVID-19.11,12 Enrollment in the parent cohort required hospitalization for COVID-1913 as defined by a PCR-confirmed SARS-CoV-2 infection at one of two urban hospitals in our health system. Participants were enrolled in MESSI-COVID during their hospital stay and then contacted at or following hospital discharge for enrollment in longitudinal follow-up. Approximately 1 year following hospital discharge, we contacted consecutive MESSI-COVID patients who had consented to longitudinal follow-up and invited them to participate in this qualitative sub-study from August 13, 2021, to January 17, 2022. Eligibility for this qualitative study required English proficiency by telephone.
Sampling
Consistent with standard qualitative research techniques, a sample size was not set a priori; rather, enrollment continued until thematic saturation was achieved.14 Thematic saturation was achieved when additional interviews ceased to yield new information about participants’ perceptions of recovery from COVID-19.
Recruitment
The research team contacted eligible patients approximately 1 year after hospital discharge by telephone, obtained verbal informed consent, and scheduled telephone interviews at a time convenient for the participant. Patients were considered unreachable after three unsuccessful attempts at contact. Participants were given $40 as an incentive for participation.
Interview Structure and Data Collection
A multidisciplinary study team developed and piloted a semi-structured interview guide based on domains identified in previous research and in consultation with health equity, pulmonology, neurology, critical care, rehabilitation, and serious illness experts. The interview guide included open-ended questions about interactions with healthcare and activities of daily living since being hospitalized (Appendix B). Participants also provided demographic information, including gender and self-identified race, assessments of financial security, and social isolation.15 Age, insurance status, baseline comorbidities, World Health Organization (WHO) clinical progression scale,16 intensive care unit (ICU) admission, need for respiratory support, and hospital length of stay were abstracted from the electronic health record. The area deprivation index (ADI), a composite measure of 17 indicators of neighborhood-level socioeconomic disadvantage, was determined for each participant based on 9-digit zipcode.17,18 To quantitatively assess persistent functional deficits and symptoms that would indicate presence of the long COVID syndrome,13 participants completed the EuroQoL5D instrument (EQ-5D), WHO Disability Assessment Schedule 2 (WHODAS-2), and Modified Research Council (MRC) Dyspnea Scale by phone with trained research personnel. Individual, 30–45-min telephone interviews were conducted by the principal investigator (C.P.C.). All interviews were audio-recorded and professionally transcribed. Field notes were made during each interview. All personal identifiers were removed from transcripts, and subject codes were assigned to protect confidentiality. De-identified transcripts were uploaded into NVivo (version 12; QSR International) for coding and analysis.
Analysis
The analytic team included a medical student and a physician with qualitative research experience and formal training (C.P.C., C.A.), a physician with expertise in disparities research (C.F.C.), a physician and an epidemiologist with expertise in ICU survivorship (R.K., M.H.), and two experienced qualitative coders (R.N., M.W.), none of whom had a relationship with study participants before enrollment. A close reading of four transcripts was conducted to develop a codebook that combined deductive codes based on the structure of the interview guide and inductive codes that emerged through open coding. Two coders (M.W., R.N.) established strong inter-rater reliability (ĸ = 0.90 [range 0.46–0.90]) with nine interviews (38%) double-coded and the remaining interviews divided and coded independently. Inter-rater reliability queries were run periodically to ensure ongoing agreement and to facilitate analysis.
The team performed qualitative content analysis with constant comparison techniques to code and organize data into discrete themes.19,20 Coded data were reviewed and analyzed by identifying patterns within participants’ experiences that suggested relationships between the deductive and inductive codes. Field notes were referenced to incorporate contextual information, such as participant emotional responses, that were not apparent in transcripts. The research team held regular consensus meetings in which they reviewed emergent themes within transcripts, resolved coding discrepancies by consensus, and agreed when thematic saturation was achieved.
RESULTS
Recruitment flow is presented in Fig. 1. We identified 42 patients engaged in longitudinal follow-up for the parent cohort study and were approximately 1-year post-hospital discharge. We successfully contacted 27 patients, of whom 24 consented to participate. Thematic saturation was achieved after 24 interviews. Participant demographic and clinical characteristics are presented in Table 1 and Appendix C. The majority of participants (71%) identified as Black. Median ADI was 82.5 (interquartile range 50.5, 91), corresponding to severe neighborhood-level disadvantage, with over half of participants (54%) living in neighborhoods with the highest ADI. Baseline comorbidities were reflective of known risk factors for developing severe COVID-19. During hospitalization, most participants (75%) required some form of respiratory support and 33% were admitted to an ICU. Among the 19 participants who completed full functional assessments 1 year after hospital discharge, 15 (79%) reported moderate to severe dysfunction or persistent symptoms on the EQ-5D, WHODAS-2, or MRC, thereby meeting criteria for long COVID.21
Fig. 1.
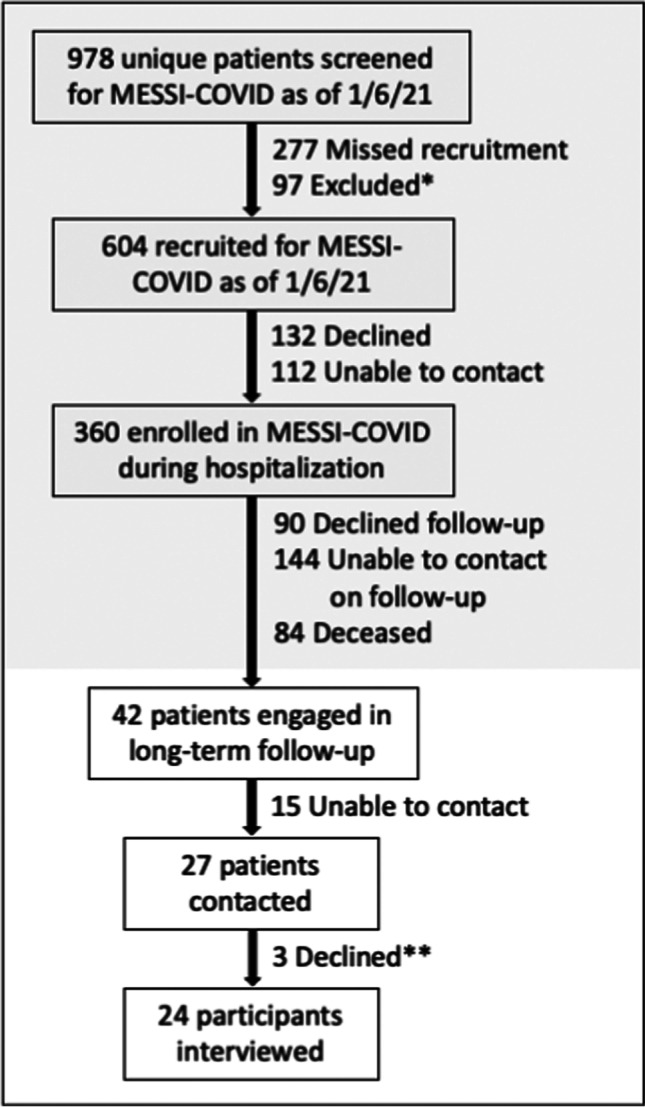
Recruitment of study participants. While the MESSI-COVID study continued to enroll and engage participants in follow-up, recruitment for this qualitative study was stopped at the time of confirming data saturation. Recruitment flow includes only those participants eligible at the conclusion of this qualitative study. *Exclusion criteria for the MESSI-COVID parent cohort included no proxy or necessary interpreter available at time of recruitment (n = 39), desire for exclusively palliative care (n = 38), active enrollment in a clinical trial (n = 14), age under 18 (n = 2), pregnancy (n = 2), severe anemia (n = 2). **Reasons for declining qualitative study participation: “not interested” (n = 1), “insufficient time” (n = 1), “not ready to tell my story” (n = 1).
Table 1.
Participant Characteristics
| Characteristic | Participants (n = 24) |
|---|---|
| Age, median (IQR) | 60.5 (49, 64.5) |
| Women, n (%) | 50 |
| Race, n (%) | |
| Black | 17 (71) |
| White | 6 (25) |
| Native American | 1 (4) |
| Insurance type, n (%) | |
| Commercial | 11 (46) |
| Medicaid | 7 (29) |
| Medicare | 5 (21) |
| Veterans affairs | 1 (4) |
| Chronic illness, n (%) | |
| Obesity | 14 (58) |
| Hypertension | 13 (54) |
| Diabetes | 11 (46) |
| Respiratory disease (asthma or chronic obstructive pulmonary disease) | 7 (29) |
| Cardiac disease | 2 (8) |
| Leukemia or lymphoma | 1 (4) |
| End stage renal disease | 1 (4) |
| Area deprivation index national rank, quintile, n (%) | |
| 1st (1–20): least disadvantaged | 2 (8) |
| 2nd (21–40) | 1 (4) |
| 3rd (41–60) | 6 (25) |
| 4th (61–80) | 2 (8) |
| 5th (81–100) | 13 (54) |
| Highest level of respiratory support while hospitalized, n (%) | |
| No oxygen support | 6 (25) |
| Nasal cannula oxygen ≤ 6 L per minute | 10 (42) |
| Non-invasive ventilation or high-flow nasal cannula (oxygen > 6L per minute) | 5 (21) |
| Invasive mechanical ventilation | 3 (13) |
| Intensive care unit admission, n (%) | 8 (33) |
| Hospital length of stay in days, median (IQR) | 6 (6, 9) |
| One-year functional and symptom assessments | Median (IQR) |
| EQ-5D | |
| Mobility (5-point scale, 1 being no problems, 5 being unable to walk about) | 3 (1, 3.75) |
| Usual activities (5-point scale, 1 being no problems, 5 being unable to do usual activities) | 2 (1, 3) |
| Anxiety, depression (5-point scale, 1 being no anxiety or depression, 5 being extreme anxiety or depression) | 2 (1, 2.75) |
| MRC dyspnea scale (5-point scale, 0 being breathless only with strenuous exercise, 5 being too breathless to leave the house or breathless with dressing) | 1 (0, 1.5) |
| WHODAS-2 (5-point scale with 5 being extreme difficulty) | |
| Item 3: Difficulty learning a new task | 1 (0, 2.5) |
| Item 6: Difficulty concentrating for 10 min | 2 (1, 3) |
| Other measures | Median (IQR) |
| How confident are you that you could find the money to pay for a financial emergency that costs about $1000? (rated on scale 1–10, 1 being no confidence, 4 being little confidence, 7 some confidence, and 10 high confidence) | 8 (4, 10) |
| 5-point social isolation measure adapted from National Health and Aging Trends Study (rated on scale 0–5 based on marital status, engagement with friends, family, religious services, and organized activities) (n = 18) | 3 (2, 4) |
IQR, interquartile range; EQ-5D, EuroQol-5 Dimensions: assesses self-reported limitations in various domains; MRC, Medical Research Council: assesses self-reported degree of breathlessness; WHODAS-2, WHO Disability Assessment Schedule 2: assesses self-reported degree of difficulty with tasks
Qualitative findings are organized into four major sections: (1) persistent symptoms, (2) impact on well-being, (3) longitudinal assessments of recovery, and (4) barriers to and facilitators of recovery.
Persistent Symptoms
The majority of participants (88%) described limitations in physical, cognitive, and psychological function during semi-structured interviews. New physical symptoms or changes in functional status included breathlessness, mobility limitations, and fatigue. Some participants also experienced new sexual dysfunction, such as lack of interest in sexual activity, following their COVID-19 hospitalization. Participants described how new symptoms made it difficult to carry out tasks they had easily performed before COVID-19 hospitalization.
The other day, I was sitting down trying to prepare food, and I ran out of breath. I can’t stand at the sink and do my dishes, I run short of breath. These are all common things that I never thought I would have a problem with. (Participant 7)
Ongoing cognitive symptoms, such memory deficits and “brain fog,” were also common. Memory deficits included problems recalling specific information.
I can’t remember stuff at all…If somebody told me something 10 minutes ago, I may forget until they bring it back to my attention. (Participant 15)
“Brain fog” included difficulty focusing and processing new information.
Even now, as you can tell in my conversation, the focus is really bad. You can’t focus. It does something to your mind with focusing. (Participant 22)
Psychological changes included new depressive symptoms such as hopelessness, sadness, and irritability. Others described new feelings of fear, worry, and anxiety. Participants discussed fears specific to their health and mortality and broader fears about the spread of COVID-19. Some participants also described frustration over how changes in their physical and psychological health resulted in lifestyle and relationship changes.
Impact on Well-being
When exploring how physical, cognitive, and psychological changes impacted current life and well-being, analysis yielded three major themes: financial hardship, loss of a sense of self, and loss of social connectedness (Table 2).
Table 2.
Relationship Between Persistent Symptoms and Domain of Well-being
| Symptom category | Well-being domain | Representative quotes | Participant number |
|---|---|---|---|
| Physical | Financial well-being | I lost my job in September of last year… I fell asleep on night shift, and I blame myself…I still wasn’t a hundred percent from having COVID in May. This was in September. Lost my job. | 11 |
| Sense of self | Well, before hospitalization, I was very energetic. I ran my boss’ businesses for them, and the office…I handled everything from A to Z for them. And I had energy. I raised six children, worked the whole time while I had my children. And was in organizations and did different things. And now it’s just a whole different world to me. And I don’t like it because my mind wants to be the person that I used to be. And now I can’t be. | 12 | |
| Social connectedness | I want to go on vacation. I can’t do that, get on a plane. My girlfriend made a, it wasn’t a joke, but she said, ‘We going to Vegas…’ I laughed it off, but I’m like, ‘I don’t want to spoil nobody’s fun.’ I’m not the same as I used to be. I’m very outgoing, love to dance. I can’t do that. I call myself old now. I’m just a old lady riding this old car because I can’t keep up with my breathing. | 3 | |
| Cognitive | Financial well-being | I can’t even go back to work. People think, ‘Oh, it’s so easy,’ but it’s not. I never thought of it that way. A little bit of brain fog, [and at work] I forget where a guy is and he calls for help, I got a problem, he’s got a problem…it affects me to a point that I can’t even go back to work. | 7 |
| Sense of self | A little bit of brain fog affects me to a point that…you can’t do anything that you’re used to. Your whole life changes, you know what I mean? I used to be able to get away from people, do this, do that, go out on my own. Now I have somebody with me, my wife and I, we’re here constantly together. | 7 | |
| Social connectedness | But integrating just the details of everyday life, appointments, things with friends…I have a large family, seven children, 11 grandchildren. Remembering appointments, commitments, simple things. I call it the matrix, that’s really, really hard still | 24 | |
| Psychological | Financial well-being | Well, before COVID, I had two jobs. I let one go because I just don’t have the energy. I don’t have the strength…And I think it’s a side effect of COVID. I’m not always cognitive of what’s going on…Something’s just not there. I can’t explain it. I just don’t feel like things sometime. I have less interest. Like I just don’t even care. I just want to lay in bed all day. | 5 |
| Sense of self | I understand having fun, but that’s not part of my vocabulary now. I don’t look to have that. Some people look to have a funny moment, or look at their laugh, and laugh until they hurt. Not me. I don’t find a lot of humor in anything now. Everything is serious now. | 20 | |
| Social connectedness | I know the difference between laying down when you’re depressed and laying down when you’re tired. I call it the dark place. When I feel myself going to the dark place I pull myself up out of it. A lot of times I’m just fearful that I have to pull myself out of it sometimes. I try not to go there, I try to catch myself. Then I isolate. I mean I will isolate. | 9 |
New physical and cognitive limitations often resulted in financial challenges. For many participants, absence from work during the acute illness and increased medical bills negatively impacted financial well-being. Participants who were able to return to work felt optimistic their financial hardships would be temporary. However, some participants described ongoing inability to work the job they had before hospitalization due to lingering health effects (often, breathlessness or memory deficits). This resulted in more persistent and profound financial impact and worries about the future.
I still have issues and there’s no way I could do my job right now…Because the focus isn’t there. And as you saw, I just automatically blank out sometimes. (Participant 12)
Participants also described changes in their sense of self. Physical health impairments, like decreased mobility or low energy, and cognitive impairments, like brain fog, meant participants could no longer function in the same occupational or social roles they held before their hospitalization.
I had to have a talk with my children like, I need you all to pick up more and help me out. I just can’t do it. I just don’t have it in me anymore. I’m not the same woman I was before COVID. (Participant 5)
This loss resulted in downstream effects on participants’ occupations and personal lives. For example, one participant who used to take pride in organizational and communication skills described how cognitive changes resulted in feeling out of place and insecure at work. Although they described a supportive work environment in which accommodations could be made, the newly reduced level of function was nonetheless unsettling and insurmountable.
While many participants spoke positively of how their loved ones supported them through recovery, COVID-19 negatively impacted social and relational health for others. This was often because physical and cognitive symptoms limited participants’ ability to interact meaningfully with others.
It’s like [I’m] fearful. I’ve been feeling so [fearful] in my friendships. I have girlfriends, but everybody backed off because I can’t do as much as they do. It’s a little depressing. (Participant 3)
Longitudinal Assessments of Recovery
Participants described various trajectories of recovery over the year since hospitalization. While many emphasized that they had not fully recovered, most reported they were getting better overall, albeit slowly.
Like I said, I have been getting stronger. I can walk a little more than I used to be able to and so I am getting better. It’s just such a slow process. It’s frustrating. (Participant 13)
Notably, five participants described complete recovery and no persistent impact on their lives. These participants’ EQ-5D, WHODAS-2, and MRC dyspnea scale scores aligned with these qualitative findings.
I don’t have any long lasting [impacts] from physical issues because I worked very hard to resolve them. (Participant 8)
Barriers to and Facilitators of Recovery
Participants described factors that either hindered or helped recovery. These barriers and facilitators were grouped into system-, clinician-, and individual-level factors (Table 3).
Table 3.
Barriers and Facilitators of Recovery at the System-, Clinician-, and Individual-Levels with Exemplary Quotes
| Barriers | Facilitators | |
|---|---|---|
| System-level |
• Transportation • High insurance co-pays, lack of insurance coverage for rehabilitation needs • Misinformation in the media • Interruption of home care during early pandemic |
• Insurance coverage • Telemedicine video appointments • Automated hospital discharge follow-up |
| Yeah. I wished I had more therapy… It wasn’t their fault. It’s just that the COVID, so they wasn’t allowed to come back into the homes no more. (Participant 3) | Well, I guess I’m more willing to call the doctors now because the insurance that I have makes it more affordable, where before I would not necessarily go to the doc…even if I should have because money was a part of it. | |
| Clinician-level |
• Clinicians dismissing persistent COVID-19 symptoms • Prioritization of physical well-being over psychological well-being |
• Clinician trust, e.g., having clinicians who the patient can trust • Patient trust, e.g., having clinicians who trust patients or take patient concerns seriously • Increased clinician access via patient messaging portals |
| Emotionally, I probably need to see a therapist. It’s been suggested. A friend of mine said, ‘You might have long haulers’, and I don’t mean physically either. Long haulers emotional... I probably could benefit from therapy. Really I haven’t looked into it, how to go about it, would my health insurance pay for it? I don’t know, you know. That probably would help, but as I said I’m tired. (Participant 9) | [My doctor] shared a lot with me. You know how they tell you, ‘Make sure you do this. Make sure you do that. Don’t worry about this. That’ll pass.’ Like the anxiety, ‘That’ll pass.’…Medical advice is good. Medical advice the best, besides spiritually. Those are the two things I can really say. (Participant 10) | |
| Individual-level |
• Lack of knowledge, specifically regarding what types of clinicians to see for persistent COVID-19 symptoms, how to access subspecialty care or rehabilitation services • Lack of familial support system |
• Supportive friends and family • Increased personal agency, e.g., taking on a more active role in healthcare • Increased attention to diet, exercise, and medication adherence • Faith, religion, spirituality • Attitude shift/gratitude |
| Oh, they don’t support me with my health at all, because they smoke. They smoke marijuana, and they smoke too much marijuana…it bothers my lungs. (Participant 6) | It made you look at life where you appreciate and you don’t take anything for granted…I want to experience some things on my bucket list…It’s no more, ‘I’ll get around to it.’ It’s no more going to bed angry…Because you just might not wake up. (Participant 21) |
System-level barriers to recovery included social infrastructure deficiencies, such as difficulty securing transportation to appointments and concerns about office accessibility. A main system-level facilitator to recovery was the coverage afforded by participants’ insurance plans, private and public alike, that enabled participants to seek and access necessary healthcare services. Participants also valued the convenience of the hospital system’s patient e-messaging platform during the recovery process.
Many participants felt their clinicians did not address their COVID-19-specific concerns appropriately, communicate with them clearly, or help them to identify effective resources (e.g., diagnostic testing or rehabilitation for persistent symptoms) for follow-up care. There was a general sense that more information should be shared by health professionals about what to expect and how to manage the recovery process, leaving participants feeling alone in seeking out external support. In particular, participants reported their cognitive and psychological needs were under-prioritized relative to their physical health needs.
I don’t know how to access [the care I need]... And I think it’s important this neurological piece, I don’t know in a general sense who would be appropriate or how to access that. (Participant 24)
Some participants reported a high degree of trust in a specific clinician as a facilitator. For such participants, this positive relationship with an individual provider was an outlier relative to their other interactions with the healthcare system. This relationship was critical to their recovery and ability to navigate an otherwise unwelcoming healthcare system.
Participants also reported experiencing stigma about having had COVID-19 in their social circles and skepticism about the legitimacy of persistent symptoms. Some noted that family members lacked consideration for their health. For others, positive family and social relationships facilitated recovery. Positive relationships provided both emotional support and assistance with basic needs and activities of daily living. Out of necessity, many participants took an active role in their own healthcare as a strategy for coping physically and psychologically during their recovery, which involved close monitoring of their own symptoms and intentional engagement with healthcare providers.
Having COVID made me more conscious of my health. I make sure I make appointments that I probably would never have made before…I have to stay up on my health because I want to live... It’s my responsibility. You can’t put that on anyone else. (Participant 5)
Some drew on faith and spirituality as sources of comfort and strength through recovery. Others adopted new mindsets or attitudes which helped them process and cope with their experiences, most notably increased gratitude for life and loved ones.
It made you look at life where you appreciate, and you don’t take anything for granted...I want to experience some things on my bucket list…It’s no more, ‘I’ll get around to it.’ It’s no more going to bed angry... Because you just might not wake up. (Participant 21)
Across participants, there was an emphasis placed on the importance of the individual-level facilitators, as these were the only facilitators to recovery that participants felt they had any control over.
DISCUSSION
This qualitative study provides insight into the recovery experiences of US patients 1 year after hospitalization for COVID-19. Most participants reported persistent symptoms and functional deficits, as assessed by both our qualitative interviews and patient-reported outcome measures, thereby meeting broad definitions of long COVID.21 Notably, the few participants with no functional deficits or objective symptoms at 1 year were the same individuals who qualitatively reported full recovery and minimal persistent life impact. Together, these findings highlight relationships between long-term deficits in physical, cognitive, and psychological health and consequent financial hardship, loss of self, and social impairments and suggest that many of the persistent negative impacts of a COVID-19 hospitalization may be driven by the development of long COVID. In addition, we identify barriers and facilitators to recovery on the system-, clinician-, and individual-levels. This work enriches prior knowledge of COVID-19 survivorship, long COVID–related health burdens, and specific challenges that Black American patients face during the process of COVID-19 survivorship.
Prior qualitative studies of recovery after COVID-19 have been conducted primarily outside the US, have had low representation of Black participants, and do not contextualize patient outcomes with socioeconomic factors.6–8 Given the disproportionate impact of COVID-19 on Black and socioeconomically disadvantaged Americans, 22 our goal was to highlight their experiences through this research. While this study was not designed to identify differences in post-COVID experiences between racial groups or related to socioeconomic status, most participants identified as Black and resided in areas with severe neighborhood-level disadvantage. This study advances COVID-19 survivorship research through inclusion of perspectives previously underrepresented in this field. Future work is needed to determine whether the themes our study identified apply to patients of other backgrounds, including race, ethnicity, rural residence, and how intersecting aspects of these identities impact healthcare and social experiences during and after COVID-19 hospitalization.
While most participants reported satisfaction with how their physical symptoms were addressed since their hospitalization, there was consensus of inadequate care for cognitive and psychological health. This may be driven by the lack of robust tools for identifying and quantifying the impact of COVID-19 on important cognitive outcomes, such as “brain fog.” In considering how to best serve the needs of patients recovering from severe COVID-19, health systems and clinicians should consider allocating resources to support patients’ overall health, including psychological and cognitive health. Previous work has shown that physicians are more likely to overlook psychological health in men and patients of Black and Hispanic backgrounds, necessitating even more awareness of this topic in these populations.23 There is additionally need for ongoing work to develop and validate tools for diagnosing brain fog and other cognitive and psychological impacts of COVID-19.
Clinicians should also be aware of how financial consequences of severe COVID-19 compound patients’ physical and psychological impairments. In a prior study on financial toxicity in patients recovering from acute respiratory distress syndrome (ARDS), two-thirds of participants reported at least some degree of ARDS-related financial strain with noted downstream impacts on physical and psychological health.24 Similar concepts emerged in our study through participants’ comments on increased financial burden after COVID-19. While it may be challenging to quantify the financial impact of COVID-19 on individuals, identifying ongoing financial hardship, particularly among individuals already residing in the most disadvantaged neighborhoods, is troubling. Though some argue that social determinants of health are beyond the scope of practice for individual clinicians,25 our study demonstrates that patients look to healthcare providers to provide guidance for problems related to the social context of health, both at a system- and clinician-level.26 While clinicians can take more active roles in stewarding resources and referring patients to supportive services in cases of financial strain,27 more durable policy interventions must also be explored. Increased federal investment in high-quality, interdisciplinary care for COVID-19 survivors, including specialized recovery clinics,28 could improve care delivery, provide support for vulnerable patients, promote rapid knowledge acquisition of mechanisms behind long COVID, and facilitate intervention development.
Of note, there was outsized importance placed on individual-level facilitators to recovery relative to system- or clinician-level facilitators. While this finding is emblematic of the resilience of the study population, it more importantly highlights the shortcomings of the system- and clinician-level supports that could better assist patients after severe COVID-19, and particularly those who have already faced significant socioeconomic disadvantage.
Limitations
Our study should be interpreted in the context of several limitations. First, participants were recruited from a single, urban, academic health system and were engaged in a longitudinal cohort study. The recovery experiences of patients in other settings and regions may diverge from those described in this study and these findings should not be considered definitive for the experience of all Black or socioeconomically disadvantaged survivors of COVID-19. Second, while our study population resided in disadvantaged neighborhoods, every participant interviewed in this study had active health insurance. Our study does not capture the experiences of uninsured patients, who are more likely to face difficulties in healthcare access and suffer worse health outcomes than their insured counterparts.29,30 Third, all interviews in this study were conducted in English. Findings may not encompass patients’ views from other cultural backgrounds and likely do not fully capture the unique barriers faced by patients with limited English proficiency.31 Finally, potential selection bias may have been introduced by recruiting participants from a sample of patients already engaged in a prospective cohort study. Our study sample includes patients most inclined to participate in research and only those successfully contacted following hospital discharge.
CONCLUSIONS
This exploratory study highlights the complex patient experiences of recovery 1 year post-hospitalization for severe COVID-19 in a predominantly Black and socioeconomically disadvantaged population. Our findings suggest interconnected relationships between persistent physical, cognitive, and psychological symptoms and their impact on socioeconomic and relational well-being. Further work is needed to understand how specific barriers and facilitators to COVID-19 illness recovery elicited by our cohort may serve as opportunities for future intervention development.
Supplementary Information
Below is the link to the electronic supplementary material.
Acknowledgements
We would like to thank the patients who agreed to participate in this study and generously shared their time and perspectives.
Funding
Financial support for this study was provided through a pilot program sponsored by the University of Pennsylvania Institute for Translational Medicine and Therapeutics and Kings College London. Subjects were initially recruited with funding to Dr. Meyer (National Institutes of Health [NIH] HL161196). Dr. Sandsmark is supported by an NIH)/National Institutes of Neurological Diseases and Stroke Career Development Award (K23 NS104239) and U01 NS114140. Dr. Kohn is supported by an NIH/National Heart, Lung, and Blood Institute Career Development Award (K23 HL146894). Dr. Auriemma is supported by an NIH/NHLBI Career Development Award (K23 HL163402) and an NIH Loan Repayment Program Award (L30 HL154185). Dr. Harhay is supported by NIH/NHLBI R00 HL141678.
Declarations
Conflict of Interest
N.J.M. has received funding from Endpoint Health, Inc and Janssen Inc for advising and consulting. She has received funding from the CAVIARDS (Careful Ventilation in ARDS) trial and SPIROMICS II cohort study to serve on a Data Safety Monitoring Board. M.O.H. has received funding from Elsevier, Guidepoint Advisors, and the American Thoracic Society for consulting and has received honoraria from Trinity Life Sciences. He has received funding from the University of California, San Francisco to serve on a Data Safety Monitoring Board.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Huang L, Yao Q, Gu X, et al. 1-Year Outcomes in Hospital Survivors with COVID-19: a Longitudinal Cohort Study. Lancet. 2021;398(10302):747. doi: 10.1016/S0140-6736(21)01755-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Taniguchi LU, Avelino-Silva TJ, Dias MB, Jacob-Filho W, Aliberti MJR. Patient-Centered Outcomes Following COVID-19: Frailty and Disability Transitions in Critical Care Survivors. Crit Care Med. 2022;50(6):955–963. doi: 10.1097/CCM.0000000000005488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Heesakkers H, van der Hoeven JG, Corsten S, et al. Clinical Outcomes Among Patients With 1-Year Survival Following Intensive Care Unit Treatment for COVID-19. JAMA. 2022;327(6):559–565. doi: 10.1001/JAMA.2022.0040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Iwashyna TJ, Kamphuis LA, Gundel SJ, et al. Continuing Cardiopulmonary Symptoms, Disability, and Financial Toxicity 1 Month After Hospitalization for Third-Wave COVID-19: Early Results From a US Nationwide Cohort. J Hosp Med. 2021;16(9):531–537. doi: 10.12788/JHM.3660. [DOI] [PubMed] [Google Scholar]
- 5.Crook H, Raza S, Nowell J, Young M, Edison P. Long COVID-Mechanisms, Risk Factors, and Management. BMJ. 2021;374. doi:10.1136/BMJ.N1648. [DOI] [PubMed]
- 6.Guo M, Kong M, Shi W, Wang M, Yang H. Listening to COVID-19 Survivors: What They Need After Early Discharge from Hospital - a Qualitative Study. Int J Qual Stud Health Well-being. 2022;17(1). doi:10.1080/17482631.2022.2030001. [DOI] [PMC free article] [PubMed]
- 7.Wu D, Ding H, Lin J, et al. Fighting COVID-19: a Qualitative Study into the Lives of Intensive Care Unit Survivors in Wuhan, China. BMJ Open. 2022;12(3):e055365. doi: 10.1136/BMJOPEN-2021-055365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Missel M, Bernild C, Westh Christensen S, Dagyaran I, Kikkenborg Berg S. The Marked Body - a Qualitative Study on Survivors Embodied Experiences of a COVID-19 Illness Trajectory. Scand J Caring Sci. 2022;36(1):183–191. doi: 10.1111/SCS.12975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mackey K, Ayers CK, Kondo KK, et al. Racial and Ethnic Disparities in COVID-19-Related Infections, Hospitalizations, and Deaths : a Systematic Review. Ann Intern Med. 2021;174(3):362–373. doi: 10.7326/M20-6306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tong A, Sainsbury P, Craig J. Consolidated Criteria for Reporting Qualitative Research (COREQ): a 32-Item Checklist for Interviews and Focus Groups. Int J Qual Health Care. 2007;19(6):349–357. doi: 10.1093/intqhc/mzm042. [DOI] [PubMed] [Google Scholar]
- 11.Kuri-Cervantes L, Pampena MB, Meng W, et al. Comprehensive Mapping of Immune Perturbations Associated with Severe COVID-19. Sci Immunol. 2020;5(49). doi:10.1126/SCIIMMUNOL.ABD7114. [DOI] [PMC free article] [PubMed]
- 12.Mathew D, Giles JR, Baxter AE, et al. Deep Immune Profiling of COVID-19 Patients Reveals Distinct Immunotypes with Therapeutic Implications. Science. 2020;369(6508). doi:10.1126/SCIENCE.ABC8511. [DOI] [PMC free article] [PubMed]
- 13.Centers for Disease Control and Prevention. Underlying medical conditions associated with higher risk for severe COVID-19: Information for healthcare professionals. Accessed https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/underlyingconditions.html. Accessed 30 Nov 1999. [PubMed]
- 14.Bradley EH, Curry LA, Devers KJ. Qualitative Data Analysis for Health Services Research: Developing Taxonomy, Themes, and Theory. Health Serv Res. 2007;42(4):1758–1772. doi: 10.1111/j.1475-6773.2006.00684.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Falvey JR, Cohen AB, O’Leary JR, Leo-Summers L, Murphy TE, Ferrante LE. Association of Social Isolation With Disability Burden and 1-Year Mortality Among Older Adults With Critical Illness. JAMA Intern Med. 2021;181(11):1433–1439. doi: 10.1001/JAMAINTERNMED.2021.5022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Marshall JC, Murthy S, Diaz J, et al. A Minimal Common Outcome Measure Set for COVID-19 Clinical Research. Lancet Infect Dis. 2020;20(8):e192–e197. doi: 10.1016/S1473-3099(20)30483-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kind AJH, Buckingham WR. Making Neighborhood-Disadvantage Metrics Accessible — the Neighborhood Atlas. N Engl J Med. 2018;378(26):2456. doi: 10.1056/NEJMP1802313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.University of Wisconsin School of Medicine and Public Health. 2020 Area Deprivation Index v3.2. Downloaded from https://www.neighborhoodatlas.medicine.wisc.edu/. Accessed Dec 16, 2022.
- 19.Charmaz K. Constructing Grounded Theory: a Practical Guide through Qualitative Analysis. London: Sage; 2006.
- 20.Leech NL, Onwuegbuzie AJ. Beyond Constant Comparison Qualitative Data Analysis: Using NVivo. Sch Psychol Q. 2011;26(1):70–84. doi: 10.1037/a0022711. [DOI] [Google Scholar]
- 21.Centers for Disease Control and Prevention. Long COVID or Post-COVID Conditions. https://www.covid.gov/longcovid/definitions. Accessed 28 March 2023.
- 22.Kirksey L, Tucker DL, Taylor E, White Solaru KT, Modlin CS. Pandemic Superimposed on Epidemic: COVID-19 Disparities in Black Americans. J Natl Med Assoc. 2021;113(1):39. doi: 10.1016/J.JNMA.2020.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Borowsky SJ, Lv Rubenstein, Meredith LS, Camp P, Jackson-Triche M, Wells KB. Who Is at Risk of Nondetection of Mental Health Problems in Primary Care? J Gen Intern Med. 2000;15(6):381. doi: 10.1046/J.1525-1497.2000.12088.X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hauschildt KE, Seigworth C, Kamphuis LA, et al. Financial Toxicity After Acute Respiratory Distress Syndrome: a National Qualitative Cohort Study. Crit Care Med. 2020;48(8):1103–1110. doi: 10.1097/CCM.0000000000004378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Maani N, Galea S. The Role of Physicians in Addressing Social Determinants of Health. JAMA. 2020;323(16):1551–1552. doi: 10.1001/JAMA.2020.1637. [DOI] [PubMed] [Google Scholar]
- 26.Brochier A, Messmer E, Garg A. Physicians and Social Determinants of Health. JAMA. 2020;324(12):1214–1215. doi: 10.1001/JAMA.2020.12106. [DOI] [PubMed] [Google Scholar]
- 27.Shah N. Physicians’ Role in Protecting Patients’ Financial Well-being. Virtual Mentor. 2013;15(2):162–166. doi: 10.1001/VIRTUALMENTOR.2013.15.2.MSOC1-1302. [DOI] [PubMed] [Google Scholar]
- 28.Santhosh L, Block B, Kim SY, et al. Rapid Design and Implementation of Post-COVID-19 Clinics. Chest. 2021;160(2):671. doi: 10.1016/J.CHEST.2021.03.044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hoffman C, Paradise J. Health Insurance and Access to Health Care in the United States. Ann N Y Acad Sci. 2008;1136:149–160. doi: 10.1196/ANNALS.1425.007. [DOI] [PubMed] [Google Scholar]
- 30.McWilliams JM, Meara E, Zaslavsky AM, Ayanian JZ. Health of Previously Uninsured Adults After Acquiring Medicare Coverage. JAMA. 2007;298(24):2886–2894. doi: 10.1001/JAMA.298.24.2886. [DOI] [PubMed] [Google Scholar]
- 31.Wilson E, Chen AH, Grumbach K, Wang F, Fernandez A. Effects of Limited English Proficiency and Physician Language on Health Care Comprehension. J Gen Intern Med. 2005;20(9):800–806. doi: 10.1111/J.1525-1497.2005.0174.X. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.