

Abstract
Purpose
Prostate cancer (PC) is the second leading cause of cancer and the fifth cause of cancer-related death. This manuscript aims to determine the incidence, mortality, and Disability Adjusted Life Years (DALYs) trends of PC in the last 30 years in Latin America and Mexico.
Methods
We performed a cross-sectional analysis of a publicly available data set. Data regarding the burden of prostate cancer in 20 Latin-American countries, and the 32 states of Mexico, were retrieved from the Global Burden of Disease Study 2019. Collected information included incidence and mortality rates (per 100,000), as well as the DALYs as absolute numbers and rates (per 100,000) and the annual rates of change in rates from 1990 to 2019.
Results
In Latin America in males aged 55 years or older, the mean incidence rate was 344 cases per 100,000. The number of deaths attributable to prostate cancer observed was 67,110 and the mean mortality rate was 210 per 100,000. The overall burden of disease was 1,120,709 DALYs and the contribution of years of life lost (YLL) was 91.7% ( = 1,027,946). Mexico presented an incidence rate (279.6) and mortality (99.1) rate (per /100 thousand). In Mexico, 13 states had a DALYs’ rate above the national mean (883 per 100,000) and the highest burden (1360 DALYs/100,000) were documented in the state of Guerrero (Southwestern Mexico).
Conclusion
Only two Latin-American countries (Brazil and Colombia) and eight states of Mexico showed a decreased trend about the rate of change of DALYs in the last 30 years.
Supplementary Information
The online version contains supplementary material available at 10.1007/s11255-023-03653-7.
Keywords: Prostate cancer, Incidence, Mortality, Mexico, Disability adjusted life years
Introduction
Worldwide and among males, prostate cancer (PC) is the second leading cause of cancer (excluding those originating from the skin) and the fifth cause of cancer-related death [1]. In 2018, estimated 1.3 million cases were diagnosed, and 359,000 deaths occurred [2].
Each country presents different rates of prevalence, incidence, and mortality, due to multiple factors that include, among others, the measurement of the prostate-specific antigen (PSA) as screening test. This latter has proved to be useful in the diagnosis of PC even in early stages.
Projections have been made to know the incidence and mortality in different countries, which allows us to estimate the burden of the disease. For example, a decrease in the incidence of 0 to 2% for the year 2030 has been predicted in USA together with an increase in the incidence of advanced metastatic disease of 1% per year in the same period [3].
The cancer-related burden of disease is growing rapidly throughout the world. This may be due to the reflection of population aging and growth, but also to changes in the prevalence and distribution of the main cancer risk factors. It has been seen that a strongly associated factor is the socioeconomic development of the country [4].
In 2020, the cancer diagnosis and treatment were negatively affected by the coronavirus disease 2019 (COVID-19) pandemic. Reduced access to care due to health care facility closures and fear of exposure to COVID-19 resulted in delays in diagnosis and treatment that could lead to short-term declines in cancer incidence. However, an increase in late-stage disease and mortality was later seen [5].
Therefore, it is relevant to know the cancer trends and thus to assess the cancer-related burden of the disease in each country. From this perspective and given that they combine morbidity and mortality data, the Disability Adjusted Life Years (DALYs) are useful tools to describe the impact of PC in different populations.
The DALYs due to PC have increased steadily from 1990 (3,694,299 DALYs) to 2017 (6,405,220 DALYs). In terms of prevalence rate, the global estimate went from 68.5 to 90.6 per 100,000 thousand during the same period [6]. Regional differences were observed. For this reason, we consider that it is important to determine the incidence, mortality, and DALY trends of PC in the last 30 years in Latin America and Mexico.
Materials and methods
We performed a cross-sectional analysis of a publicly available data set. Data regarding the burden of PC (International Statistical Classification of Diseases and Related Health Problems, 10th revision [ICD-10], C61) in 20 Latin-American countries, and the 32 states of Mexico, were retrieved from the Global Burden of Disease Study 2019 (GBD 2019) (https://vizhub.healthdata.org/gbd-results/; accessed 10 February 2023). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were used to ensure the reporting of this observational study (https://www.equator-network.org/reporting-guidelines/strobe/; accessed 10 February 2023).
Collected information included incidence and mortality rates (per 100,000), as well as the DALYs as absolute numbers and rates (per 100,000) and the annual rates of change in rates from 1990 to 2019. Inclusion criteria: all the estimates of interest were obtained for men aged 55 years or older. This cut-off was chosen given that PC are infrequent in younger males [7].
Summary statistics were computed. The DALYs’ rates were used to describe and compare the burden of disease related to PC within the Latin-American countries and within the states of Mexico. The annual rates of change in DALYs’ rate, from 1990 to 2019, were also retrieved.
Cancerology State Institute ethics committee (Colima State Health Services, Mexico) approved the present study (Approval Code: CEICANCL03022023-EPNPROS-03; approval date: January 10, 2023).
Results
A total of 159,981 incident cases of prostate cancer were registered during 2019 in Latin America in males aged 55 years or older. The mean incidence rate in this age group was 344 cases per 100,000 and ranged from 208 to 631 in Honduras and Cuba, respectively. The number of deaths attributable to prostate cancer observed in the same period was 67,110 and the mean mortality rate was 210 per 100,000 males aged 55 years and older. Figure 1 shows the incidence and mortality rates for each country from the evaluated region. In Mexico and in the same age group, the documented incidence and mortality rates were 279.6 and 99.1 (per 100,000 men), respectively. Supplementary data 1 presents the precise incidence and mortality rates of PC in 2019.
Fig. 1.

Incidence and mortality rate (per 100 thousand) of prostate cancer in men aged 55 years or older in Latin-American countries, 2019
The overall burden of disease was 1,120,709 DALYs and the contribution of years of life lost (YLL) was 91.7% ( = 1,027,946). As observed in Table 1, the DALYs rates (per 100,000) were used to identify the Latin-American countries with the highest burden. The highest rates were documented in Haiti (2499), Dominican Republic (1910), and Cuba (1769). These three countries have also led the annual rate of change (1990–2019) in DALYs rate, where most of the countries (excepting Brazil, and Colombia) showed increasing trends (Fig. 2).
Table 1.
Burden of prostate cancer in Latin-American countries in men aged 55 years or older, 2019
| Rank/location | DALYs (rate/ | %YLL | ||
|---|---|---|---|---|
| 1 | Haiti | 2499 | 23,689 | 97.0 |
| 2 | Dominican Republic | 1910 | 26,974 | 94.2 |
| 3 | Cuba | 1769 | 54,121 | 89.3 |
| 4 | Venezuela | 1680 | 72,993 | 89.4 |
| 5 | Uruguay | 1654 | 12,942 | 92.9 |
| 6 | Bolivia | 1640 | 21,579 | 95.3 |
| 7 | Nicaragua | 1381 | 8276 | 90.6 |
| 8 | Argentina | 1297 | 103,018 | 93.4 |
| 9 | Chile | 1220 | 44,619 | 91.4 |
| 10 | Guatemala | 1188 | 19,006 | 94.2 |
| 11 | Costa Rica | 1170 | 9204 | 87.0 |
| 12 | Panama | 1158 | 7714 | 89.3 |
| 13 | Brazil | 1132 | 389,400 | 92.3 |
| 14 | Paraguay | 1126 | 9381 | 92.8 |
| 15 | Ecuador | 1089 | 25,560 | 93.4 |
| 16 | Honduras | 995 | 8777 | 93.8 |
| 17 | El Salvador | 979 | 8326 | 91.4 |
| 18 | Peru | 973 | 49,403 | 92.6 |
| 19 | Colombia | 897 | 72,178 | 88.8 |
| 20 | Mexico | 883 | 153,548 | 90.2 |
The rate per 100 thousand is presented
DALYs Disability Adjusted Life Years, YLL Years of Life Lost
Fig. 2.
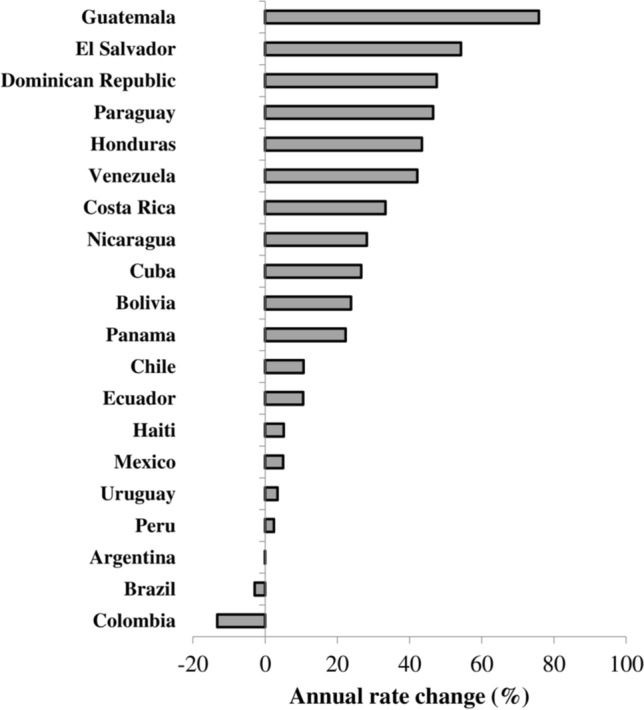
Annual rate of change in the disability-adjusted life years (DALYs) rate (per 100 thousand) due to prostate cancer in men aged 55 years or older, 1990–2019
In Mexico, a total 25,516 cases of PC were documented during 2019 in males ≥ 55 years old. The overall number of deaths was 9081. Figure 3 shows the state-stratified incidence and mortality rates (per 100,000) in the same age group. The incidence rates ranged from 468.3 (Sinaloa) to 195.4 (Oaxaca). The second and third highest rates were observed in Nayarit (399.5) and Guerrero (380.0), respectively. As also observed in Fig. 3, the mortality rates were nearly homogeneous in the 32 states and the national mean was 100.5 per 100,000 men aged 55 years and older.
Fig. 3.

Incidence and mortality rate (per 100 thousand) of prostate cancer in men aged 55 years or older in the states (n = 32) of Mexico, 2019
Also, in Mexican territory (Table 2), a total of 13 states had a DALYs’ rate above the national mean (883 per 100,000) and the highest burden (1360 DALYs per 100,000) were documented in the state of Guerrero, located in Southwestern Mexico. It was followed by the states of Nayarit (1170) and Sinaloa (1136), located in West-central and Northwestern Mexico, respectively.
Table 2.
Burden of prostate cancer in the states of Mexico in men aged 55 years or older, 2019
| Rank/Location | DALYs (rate/ | %YLL | ||
|---|---|---|---|---|
| 1 | Guerrero | 1360 | 6503 | 91.7 |
| 2 | Nayarit | 1170 | 2277 | 90.0 |
| 3 | Sinaloa | 1136 | 5446 | 87.5 |
| 4 | Chihuahua | 1103 | 5113 | 90.8 |
| 5 | Colima | 1087 | 1153 | 90.1 |
| 6 | Baja California Sur | 1055 | 964 | 88.2 |
| 7 | Sonora | 1014 | 4287 | 89.4 |
| 8 | Jalisco | 1012 | 11,402 | 90.1 |
| 9 | Tamaulipas | 958 | 4707 | 88.2 |
| 10 | Zacatecas | 956 | 2397 | 91.1 |
| 11 | Baja California | 926 | 4133 | 88.5 |
| 12 | Michoacán de Ocampo | 919 | 6772 | 90.7 |
| 13 | Mexico City | 900 | 13,724 | 89.6 |
| 14 | Coahuila | 877 | 3717 | 90.0 |
| 15 | Chiapas | 874 | 5928 | 92.8 |
| 16 | Nuevo León | 873 | 6354 | 87.8 |
| 17 | Veracruz | 872 | 11,744 | 90.7 |
| 18 | Guanajuato | 868 | 6902 | 90.3 |
| 19 | Tabasco | 868 | 2821 | 90.7 |
| 20 | Aguascalientes | 855 | 1422 | 90.0 |
| 21 | Durango | 833 | 2190 | 90.5 |
| 22 | San Luis Potosí | 829 | 3644 | 91.1 |
| 23 | Morelos | 807 | 2472 | 90.6 |
| 24 | Querétaro | 777 | 1994 | 90.3 |
| 25 | Estado de México | 751 | 15,824 | 90.1 |
| 26 | Hidalgo | 749 | 3390 | 90.3 |
| 27 | Yucatán | 739 | 2463 | 90.7 |
| 28 | Campeche | 732 | 953 | 90.6 |
| 29 | Quintana Roo | 726 | 1102 | 90.1 |
| 30 | Puebla | 715 | 5970 | 91.9 |
| 31 | Oaxaca | 696 | 4646 | 92.4 |
| 32 | Tlaxcala | 657 | 1134 | 90.9 |
The rate per 100 thousand is presented
DALYs Disability Adjusted Life Years, YLL Years of Life Lost
Regarding the trends in the burden of prostate cancer in the Mexican territory (Fig. 4), 23 out of 32 states showed increasing trends. This scenario was particularly concerning in Zacatecas, Guerrero, and Nayarit, where the DALYs’ rate has increased in about 26% and 25% per year from 1990 to 2019 and both of them already have the two highest rates.
Fig. 4.

Annual rate of change in the disability-adjusted life years (DALYs) rate (per 100 thousand) due to prostate cancer in the states of Mexico in men aged 55 years or older, 1990–2019
Discussion
We characterized the burden of PC in 20 Latin-American countries and the 32 states of Mexico in 2019. We found that YLL contributes to nearly 92% of the regional disease burden (1,120,709 DALYs).
According to our results, the incidence and mortality of these neoplasms in the region were 344 and 210 cases per 100,000 men, respectively. These estimates were upper than those documented in Mexico (incidence, 279.6 per 100,000; mortality, 99.1 per 100,000).
The PC rates observed in Brazil and Mexico, the Latin-American countries with the highest populations, were lower than the regional mean. These heterogeneous patterns may be related, among others, to ethnic differences, biological factors, and socioeconomic status [8]. Accesses to healthcare systems, health promotion activities, and systematic PC screening also have a particular impact in each country of the region.
Published data suggest a decreasing trend in PC incidence rates and, according to projections, these trends would continue until 2030 at an average of − 2% [9, 10]. Over the last 30 years, DALYs increased in Africa, South-East Asia, and Eastern Mediterranean Region, and they decreased in the Americas, Europe, and Western Pacific Region [11]. However, there is no precise knowledge about the rate of change of DALYs in Latin America or within Mexico. In our analysis, only two Latin-American countries (Brazil and Colombia) and eight states of Mexico (Fig. 3) showed a decreased trend.
We also documented a decreasing burden of PC in three states of Mexico (Mexico City, Baja California, and Coahuila) as previously evidenced in the region [12]. Factors determining this scenario are beyond our analysis, but the per capita income in these states is higher than the national mean. This latter may have, at least partially, an effect on the observed trend.
The reduction in PC burden does not necessarily reflex improved primary prevention. It seems more plausible that this decreasing trend may be secondary to opportune diagnosis and treatment alternatives. As manifested by Steel BC and cols, to ensure that all PC patients receive accurate medical attention, health services must optimize the usage of data and resources [13].
A limitation of the present study is that epidemiological estimates related to PC in Latin-American countries from the GBD 2019 Study and GLOBOCAN show some differences [14–16] due to heterogeneous methodologies. Mexico lacks a population-based cancer registry [17]. Therefore, the estimations presented by the GBD for our country are projections based on mortality trends. However, the death registration system in Mexico has shown a good performance [18].
In conclusion, only two Latin-American countries (Brazil and Colombia) and eight states of Mexico showed a decreased trend about the rate of change of DALYs in the last 30 years (1990–2019). It is necessary to establish and/or execute public policies aimed at reducing the incidence, mortality, and DALYs for PC in most Latin-American countries and in most regions of Mexico.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 Supplementary material: Burden of prostate cancer in men aged 55 and older in 20 Latin-American countries and the 32 states of Mexico, 2019. (DOCX 20 KB)
Author contributions
JGE and IDE had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: JGE, EMZ, and IDE. Acquisition of data: JDE and MOM. Analysis and interpretation of data: LDLZ and JCCP. Drafting of the manuscript: JGE, EMZ, and IDE. Critical revision of the manuscript for important intellectual content: MOM, HRGZ, LDLZ, and LCCP. Statistical analysis: EMZ and MOM. Administrative, technical, or material support: JDE. Supervision: JGE and IDE.
Funding
This research received no external funding.
Data availability
We performed a cross-sectional analysis of a publicly available data set: Global Burden of Disease Study 2019 (GBD 2019) (https://vizhub.healthdata.org/gbd-results/; accessed 10 February 2023).
Declarations
Conflict of interest
The authors declare no conflict of interest.
Ethical approval
The study was conducted following the Declaration of Helsinki, and the Cancerology State Institute ethics committee (Colima State Health Services, Mexico) approved the present study (Approval Code: CEICANCL03022023-EPNPROS-03; approval date: January 10, 2023).
Consent for publication
Not applicable.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J Clin. 2021;71:209–249. doi: 10.3322/caac.21660. [DOI] [PubMed] [Google Scholar]
- 2.Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. doi: 10.3322/caac.21492. [DOI] [PubMed] [Google Scholar]
- 3.Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74:2913–2921. doi: 10.1158/0008-5472.CAN-14-0155. [DOI] [PubMed] [Google Scholar]
- 4.Omran AR. The epidemiologic transition. A theory of the epidemiology of population change. Milbank Mem Fund Q. 1971;49:509–538. doi: 10.2307/3349375. [DOI] [PubMed] [Google Scholar]
- 5.Yabroff KR, Wu XC, Negoita S, et al. Association of the COVID-19 pandemic with patterns of statewide cancer services. J Natl Cancer Inst. 2022;114:907–909. doi: 10.1093/jnci/djab122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Launer BM, Lloyd GL. Sociodemographic index and global trends in prostate cancer: 1990–2017. Prostate. 2021;81:825–831. doi: 10.1002/pros.24178. [DOI] [PubMed] [Google Scholar]
- 7.Zi H, He SH, Leng XY, et al. Global, regional, and national burden of kidney, bladder, and prostate cancers and their attributable risk factors, 1990–2019. Mil Med Res. 2021;8:60. doi: 10.1186/s40779-021-00354-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Badal S, Aiken W, Morrison B, et al. Disparities in prostate cancer incidence and mortality rates: solvable or not? Prostate. 2020;80:3–16. doi: 10.1002/pros.23923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74:2913–2921. doi: 10.1158/0008-5472.CAN-14-0155. [DOI] [PubMed] [Google Scholar]
- 10.Weir HK, Thompson TD, Soman A, Moller B, Leadbetter S. The past, present, and future of cancer incidence in the United States: 1975 through 2020. Cancer. 2020;121:1827–1837. doi: 10.1002/cncr.29258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mouchati C, Abdallah N, Jani C, et al. Trends in disease burden from prostate cancer amongst different regions of the world and extensively the European Union 15+ countries, from 1990 to 2019: estimates from the global burden of disease study. J Clin Oncol. 2022;40:187. doi: 10.1200/JCO.2022.40.6_suppl.187. [DOI] [Google Scholar]
- 12.Zhai Z, Zheng Y, Li N, et al. Incidence and disease burden of prostate cancer from 1990 to 2017: results from the global burden of disease study 2017. Cancer. 2020;126:1969–1978. doi: 10.1002/cncr.32733. [DOI] [PubMed] [Google Scholar]
- 13.Steele CB, Li J, Huang B, Weir HK. Prostate cancer survival in the United States by race and stage (2001–2009): findings from the CONCORD-2 study. Cancer. 2017;123(Suppl 24):5160–5177. doi: 10.1002/cncr.31026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fitzmaurice C, Global Burden of Disease Cancer Collaboration Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 2006 to 2016: a systematic analysis for the Global Burden of Disease study. J Clin Oncol. 2018;36:1568–1568. doi: 10.1200/JCO.2018.36.15_suppl.1568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. doi: 10.3322/caac.21660. [DOI] [PubMed] [Google Scholar]
- 16.World Health Organization (2023) International agency for research on cancer. Cancer Today. https://gco.iarc.fr/today/home. Accessed 26 Jan 2023
- 17.Mohar-Betancourt A, Reynoso-Noverón N, Armas-Texta D, Gutiérrez-Delgado C, Torres-Domínguez JA. Cancer trends in Mexico: essential data for the creation and follow-up of public policies. J Glob Oncol. 2017;3:740–748. doi: 10.1200/JGO.2016.007476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hernandez B, Rodriguez Angulo E, Johnson LM, et al. Assessment of the quality of the vital registration system for under-5 mortality in Yucatan. Mexico Popul Health Metr. 2022;20:7. doi: 10.1186/s12963-022-00284-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary file1 Supplementary material: Burden of prostate cancer in men aged 55 and older in 20 Latin-American countries and the 32 states of Mexico, 2019. (DOCX 20 KB)
Data Availability Statement
We performed a cross-sectional analysis of a publicly available data set: Global Burden of Disease Study 2019 (GBD 2019) (https://vizhub.healthdata.org/gbd-results/; accessed 10 February 2023).