

Abstract
Background
Evidence suggests that changes in advanced glycation end‐products (AGEs) may influence body weight. Previous studies have focused on cooking methods as the primary way how to reduce the dietary AGEs but little is known about the effects of a change in diet composition.
Objective
The aim of this study was to assess the effects of a low‐fat plant‐based diet on dietary AGEs and test the association with body weight, body composition, and insulin sensitivity.
Methods
Participants who were overweight (n = 244) were randomly assigned to an intervention (low‐fat plant‐based) (n = 122) or control group (n = 122) for 16 weeks. Before and after the intervention period, body composition was measured by dual X‐ray absorptiometry. Insulin sensitivity was assessed with the predicted insulin sensitivity index (PREDIM). Three‐day diet records were analyzed using the Nutrition Data System for Research software and dietary AGEs were estimated, using a database. Repeated measure ANOVA was used for statistical analysis.
Results
Dietary AGEs decreased in the intervention group by 8768 ku/day on average (95% −9611 to −7925; p < 0.001), compared with the control group (−1608; 95% CI −2709 to −506; p = 0.005; treatment effect −7161 ku/day [95% CI −8540 to −5781]; Gxt, p < 0.001). Body weight decreased by 6.4 kg in the intervention group, compared with 0.5 kg in the control group (treatment effect −5.9 kg [95% CI −6.8 to −5.0]; Gxt, p < 0.001), largely due to a reduction in fat mass, notably visceral fat. PREDIM increased in the intervention group (treatment effect +0.9 [95% CI + 0.5 to +1.2]; p < 0.001). Changes in dietary AGEs correlated with changes in body weight (r = +0.41; p < 0.001), fat mass (r = +0.38; p < 0.001), visceral fat (r = +0.23; p < 0.001), and PREDIM (r = −0.28; p < 0.001), and remained significant even after adjustment for changes in energy intake (r = +0.35; p < 0.001 for body weight; r = +0.34; p < 0.001 for fat mass; r = +0.15; p = 0.03 for visceral fat; and r = −0.24; p < 0.001 for PREDIM).
Conclusions
Dietary AGEs decreased on a low‐fat plant‐based diet, and this decrease was associated with changes in body weight, body composition, and insulin sensitivity, independent of energy intake. These findings demonstrate positive effects of qualitative dietary changes on dietary AGEs and cardiometabolic outcomes.
Clinical Trial Registry Number
Keywords: advanced glycation end‐products, diet, nutrition, vegan, weight
Abbreviations
- AGEs
advanced glycation end‐products
- BMI
body mass index
- HOMA‐IR
homeostasis model assessment insulin resistance
1. INTRODUCTION
From 2000 to 2018, the prevalence of obesity among U.S. adults increased to over 42%. 1 , 2 The extra weight is frequently associated with hyperglycemia, dyslipidemia, hypertension and insulin resistance in a cluster known as the metabolic syndrome, which is associated with chronic oxidative stress and inflammation. 3 Although overnutrition is considered a major cause of obesity, not all obese individuals develop the metabolic syndrome; more research is needed to clarify the relevant pathophysiologic mechanisms. One possible mechanism in the development of the metabolic syndrome is an accelerated production of advanced glycation end products (AGEs).
AGEs are a large heterogenous group of compounds resulting from the spontaneous, non‐enzymatic reaction of the carbonyl groups of sugars with free amino groups in protein; this is the classical Maillard reaction but many other reactions, even in the absence of hyperglycemia, can lead to AGE formation. 4 AGEs are important because they cause inflammation and oxidative stress, processes that eventually lead to chronic diseases, particularly type 2 diabetes and cardiovascular disease. While AGEs are generated constantly during normal metabolism, their rate of formation is markedly enhanced during hyperglycemia and/or conditions characterized by increased oxidative stress. They may also be ingested through the diet. 5 , 6 Thermally prepared foods, particularly of animal origin, are rich in AGEs, which are perceived as flavorful, therefore enhancing palatability and consumption, promoting weight gain. Excessive intake of dietary AGEs, identified by at least one distinct marker, carboxymethyllysin, has been linked to high serum AGEs, oxidative stress and inflammation, reduced innate immune defenses, and insulin resistance in humans. 7 This has led to a postulated model in which both endogenous and exogenous AGEs contribute to oxidative stress and inflammation, which represent underlying mechanisms of chronic diseases, including metabolic syndrome and type 2 diabetes. 4 , 8 , 9
Plant‐based diets have been shown to cut the risk of developing the metabolic syndrome and type 2 diabetes by about a half. 10 , 11 Since plant foods are generally lower in dietary AGEs than animal‐derived foods, 6 it is plausible that a plant‐based diet would reduce the dietary AGEs. Two randomized interventional trials have shown that dietary AGE restriction ameliorated insulin resistance in obese people with metabolic syndrome. 7 , 12 These trials were performed in individuals who at baseline had a spontaneous high dietary AGE intake with a mixed diet, and their consumption of animal‐derived foods was significant. The dietary AGE reduction was achieved simply by changing the cooking technique of the same foods, for example, from grilling, roasting, and frying to stewing or poaching, so as to decrease the level and duration of heat application, as well as using more water in the cooking medium. However, studies exploring the effect of changing the actual food composition of the diet as it happens in the transition to a plant‐based diet on levels of dietary AGE intake are lacking.
The effects of a plant‐based diet on weight loss, improved body composition and insulin sensitivity, were previously assessed in a 16‐week randomized trial in 244 people who were overweight. 13 This secondary analysis tested the effect of this plant‐based nutrition intervention on dietary AGE intake, and evaluated the potential role of dietary AGEs in changes in body weight, body composition, and insulin sensitivity previously observed. It was hypothesized that the dietary AGEs would decrease on a low‐fat plant‐based diet and that this reduction would be associated with the previously observed weight loss, reduction in body fat, visceral fat, and increase in insulin sensitivity.
2. METHODS
2.1. Study design and eligibility
The methods have been previously described. 13 In brief, this randomized, open parallel controlled study was conducted for four replications between February 2017 and February 2019 in Washington, D.C. Enrolled participants were men and women (n = 244), aged 25–75 years, with a body mass index between 28 and 40 kg/m2. Exclusion criteria included history of diabetes, pregnancy or lactation, recent or current smoking, alcohol or drug abuse, and current use of a vegan diet. The study protocol was reviewed and approved by the Chesapeake Institutional Review Board and all participants provided written informed consent.
2.2. Randomization and study groups
Using a computer‐generated system, participants were randomly assigned to an intervention or control group in a 1:1 ratio. The intervention group was asked to follow an ad libitum low‐fat vegan diet (∼75% of energy from carbohydrates, 15% protein, and 10% fat) consisting of fruits, vegetables, grains, and legumes (beans, peas, and lentils), while the control group was requested to make no diet changes. Energy intake was not limited for either group. Participants in the intervention group were instructed to avoid all animal products and added fats and to take a vitamin B12 supplement (500 μg/day). For both groups, no meals were provided, and alcoholic beverages (of any type) were limited to one per day for women and two per day for men. All participants were asked not to alter their exercise habits and to continue their preexisting medication regimens for the duration of the study, except as modified by their personal physicians.
2.3. Outcomes
Measurements were performed at baseline and week 16. A 3‐day dietary record (two weekdays and one weekend day) was completed by each participant at each assessment. Dietary intake data were collected and analyzed by a staff member certified in the Nutrition Data System for Research, developed by the Nutrition Coordinating Center at the University of Minnesota, Minneapolis, MN. 14
In a post‐hoc analysis of above data, AGE scores were assigned to each food item from the above database, using a published database of AGE content in about 560 food items that has been previously used in epidemiologic studies to estimate dietary AGE intake. 15 , 16 , 17 Consistent with previously published methodology, 15 , 16 , 17 each food item identified was assigned a dietary AGE value in kilounits/gram of food, which was then multiplied by the number of grams of this food consumed per day. The dietary AGE values for each and all foods consumed during the day were then added up to provide a total dietary AGE value in kilounits/day per participant. Whenever a food present in the original database was not listed in the dietary AGE database, a value was assigned based on the similarity of nutrient ingredients and cooking methods with foods listed in the dietary AGE database. This was done by a co‐author (JU) who was completely masked regarding dietary intervention assignment. In the database, carboxymethyllysin‐AGE content was estimated using ELISA based on monoclonal anti‐carboxymethyllysin antibody. 6
Physical activity was assessed by the International Physical Activity Questionnaire. 18 All laboratory assessments were measured after a 10–12 h overnight fast, with only water allowed ad libitum. Height, at baseline only, and weight were measured using a stadiometer and a calibrated scale accurate to 0.1 kg, respectively. Body composition and visceral fat volume were assessed using dual energy X ray absorptiometry (iDXA; GE Healthcare), which has been validated both against X‐ray computed tomography 19 and magnetic resonance imaging. 20 Predicted insulin sensitivity index (PREDIM) was used to assess insulin sensitivity, which has been previously validated against clamp‐derived measures of insulin sensitivity, 21 and was determined through a calculation of dynamic postprandial insulin sensitivity following a liquid breakfast (Boost Plus, Nestle, Vevey, Switzerland; 720 kcal, 34% of energy from fat, 16% protein, 50% carbohydrate).
2.4. Statistical analysis
For baseline characteristics, all enrolled participants were included; between‐group t‐tests were performed for continuous variables and X 2 or Fisher's exact test for categorical variables. A repeated measure ANOVA model was used with between‐subject and within‐subject factors and interactions. Factors group, subject, and time were included in the model. Interaction between group and time (Gxt) was calculated for each variable. Data from only those with measurements at both timepoints were included in the ANOVA model. Within each group, paired comparison t‐tests were calculated to test whether the changes from baseline to 16 weeks were statistically significant. Pearson correlations were calculated to test the association between changes in dietary AGEs and changes in body weight, fat mass, visceral fat, and insulin sensitivity in both study groups combined, first unadjusted and then and then Pearson partial correlations controlling for the effect of energy intake. All results are presented as means with 95% confidence intervals (CI).
3. RESULTS
3.1. Participant characteristics
Of 3115 people screened by telephone, 244 met participation criteria and provided informed consent. Using a computer‐generated system, they were randomly assigned (in a 1:1 ratio) to the intervention (n = 122) or control (n = 122) groups. The baseline characteristics of the study population has been reported earlier. 13 Mostly for reasons unrelated to the study, 21 participants dropped out (5 from the intervention and 16 from the control group), leaving 223 (91.0%) study completers, who were included in the repeated measure ANOVA model.
3.2. Body weight, body composition, and insulin sensitivity
As described previously, 13 mean body weight decreased by 6.4 kg in the intervention group from 93.6 to 87.2 kg, which represents a 7% reduction in body weight, compared with a nonsignificant weight loss of 0.5 kg in the control group (treatment effect −5.9 kg [95% CI −6.7 to −5.0]; p < 0.001). This was largely due to a reduction in body fat (treatment effect −4.1 kg [95% CI −4.7 to −3.5] kg; p < 0.001) and visceral fat volume (treatment effect −209 cm3 [95% CI −304 to −114]; p < 0.001). Insulin sensitivity, measured by PREDIM, increased significantly in the intervention group (treatment effect +0.9 mg/min/kg [95% CI, +0.5 to +1.2]; p < 0.001). Physical activity decreased slightly in both groups, with no difference between the groups. Self‐reported energy intake was reduced in both groups (from 1834 to 1344 kcal/day in the intervention and from 1793 to 1657 kcal/day in the control group), more so in the intervention group (treatment effect −355 kcal/day [95% CI, −519 to −19; p < 0.001).
3.3. Dietary AGEs
Dietary AGEs decreased in the vegan group by 79%, that is, by 8768 ku/day on average (95% −9611 to −7925; p < 0.001), compared with the control group (decrease by 15%, i.e., by 1608 ku/day; 95% CI −2709 to −506; p = 0.005; treatment effect −7161 ku/day [95% CI −8540 to −5781]; Gxt, p < 0.001; Figure 1). About 55% of the reduction of the dietary AGEs in the intervention group was due to the reduction of meat intake, 26% thanks to decreased dairy intake, and 15% was attributable to the decreased use of added fats. Most of the dietary AGEs from meat were due to white meat consumption (59%), followed by processed meat (27%). The dietary AGEs in all major food groups are shown in Table 1.
FIGURE 1.
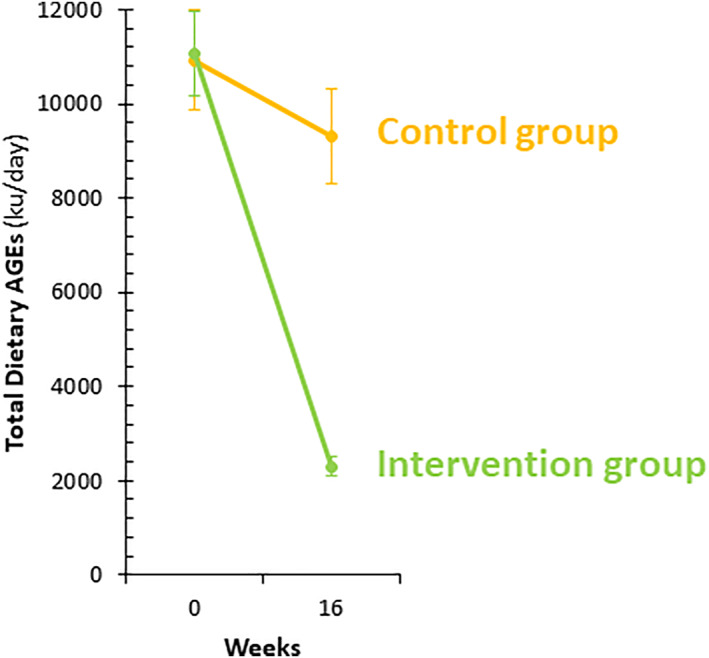
Change in total dietary advanced glycation end‐products (AGEs) in the intervention (green symbols and line) and the control group (orange symbols and line) from week 0 to week 16. The data are shown as means with 95% confidence intervals (CI).
TABLE 1.
Changes in dietary advanced glycation end‐products (AGEs) from specific food groups at baseline and at week 16 in the control and the intervention group
| Control group | Intervention group | |||||
|---|---|---|---|---|---|---|
| AGEs from specific food groups (ku/day) | Baseline | Week 16 | Baseline | Week 16 | Treatment effect | p‐value |
| Total AGEs | 10,922 (9855–11,989) | 9315 (8312‐10,317)** | 11,067 (10,184–11,950) | 2299 (2093–2505)*** | −7161 (−8540 to −5781) | <0.001 |
| Fruit | 144.3 (80.3–208.3) | 29.3 (21.7–36.9)*** | 128.0 (79.2–176.7) | 41.0 (35.6–46.5)*** | +28.0 (−50.3 to +106.4) | 0.48 |
| Vegetables | 100.2 (80.6–119.8) | 105.4 (83.3–127.6) | 181.3 (93.2–159.6) | 107.9 (91.1–124.8) | −23.8 (−64.4 to +16.8) | 0.25 |
| Legumes | 73.9 (53.5–94.2) | 63.0 (44.9–81.2) | 70.2 (52.1–88.2) | 195.1 (156.6–233.6)*** | +135.8 (+91.8 to +179.8) | <0.001 |
| Grains total | 859.5 (711.0–1008) | 663.8 (532.1–795.4)* | 894.3 (762.7–1026) | 640.5 (550.4–730.6)** | −58.1 (−292.8 to +176.7) | 0.63 |
| Whole grains | 241.2 (195.3–287.2) | 170.7 (129.6–211.8)* | 216.9 (176.2–257.6) | 257.1 (220.5–293.7) | +110.7 (+32.7 to +188.7) | 0.006 |
| Some whole grains | 82.4 (41.9–122.8) | 63.8 (33.2–94.4) | 100.7 (53.7–147.8) | 76.5 (39.9–113.0) | −5.8 (−79.4 to +67.9) | 0.88 |
| Refined grains | 535.9 (390.9–680.9) | 429.2 (309.7–548.8) | 576.6 (464.4–688.9) | 306.9 (238.9–375.0)*** | −163.0 (−378.4 to +52.4) | 0.14 |
| Total meat | 3983 (3447–4519) | 3852 (3233–4471) | 4131 (3568‐4695) | 42.2 (1.4–83.0)*** | −3958 (−4800 to −3117) | <0.001 |
| Red meat | 596.4 (379.5–813.3) | 527.8 (335.3–720.4) | 481.8 (310.3–653.3) | 0.0 (0.0–0.0)*** | −413.2 (−723.1 to +103.3) | 0.009 |
| White meat | 2547 (2094–2999) | 2159 (1682–2637) | 2734 (2246‐3223) | 19.2 (0.0–48.7)*** | −2, 328 (−3057 to −1598) | <0.001 |
| Processed meat | 722.1 (551.4–892.8) | 1039 (764.5–1314)* | 783.5 (622.5–944.5) | 25.2 (0.0–54.7)*** | −1075 (−1407 to −743.7) | <0.001 |
| Fried meat | 132.4 (18.8–246.1) | 141.4 (25.6–257.2) | 152.3 (32.3–272.2) | 0.0 (0.0–0.0)* | −161.2 (−331.1 to +8.6) | 0.06 |
| Meat alternatives | 154.5 (69.3–239.7) | 148.9 (61.3–236.4) | 140.2 (75.8–204.6) | 506.8 (394.3–619.3)*** | +372.2 (+216.4 to +528.1) | <0.001 |
| Eggs total | 527.1 (351.1–703.2) | 23.6 (17.7–29.5)*** | 562.2 (416.5–708.0) | 0.1 (0.0–0.3)*** | −58.6 (−283.3 to +166.1) | 0.61 |
| Boiled | 6.9 (3.4–10.4) | 7.8 (3.3–12.3) | 4.1 (1.2–7.1) | 0.1 (0.0–0.2)** | −5.0 (−9.3 to −0.7) | 0.02 |
| Baked | 0.9 (0.0–1.9) | 1.3 (0.0–2.7) | 2.8 (1.1–4.5) | 0.1 (0.0–0.1)** | −3.1 (−5.4 to −0.7) | 0.01 |
| Fried | 519.3 (342.6–696.0) | 14.5 (10.0–19.0)*** | 555.3 (409.2–701.4) | 0.0 (0.0–0.0)*** | −50.5 (−275.6 to +174.5) | 0.66 |
| Nuts and seeds total | 1224 (886.3–1563) | 995.5 (771.3–1220) | 1092 (782.9–1401) | 319.5 (232.6–406.4)*** | −543.5 (−1035 to −52.1) | 0.03 |
| Raw | 105.9 (42.3–169.6) | 96.1 (17.9–174.4) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | +9.8 (−50.0 to +69.6) | 0.75 |
| Roasted | 723.3 (456.3–990.3) | 637.0 (439.1–834.9) | 883.6 (588.0–1179) | 171.4 (97.8–245.0)*** | −625.9 (−1053 to −199.0) | 0.004 |
| Nut butter raw | 27.4 (0.0–74.6) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | +27.4 (−16.3 to +71.2) | 0.22 |
| Nut butter roasted | 367.8 (163.2–572.4) | 262.4 (168.2–356.6) | 208.4 (137.9–278.8) | 148.1 (104.0–192.3) | +45.2 (−174.1 to +264.4) | 0.69 |
| Dairy total | 2410 (1917–2904) | 1926 (1409–2443) | 2386 (1959–2814) | 32.4 (8.4–56.3)*** | −1870 (−2607 to −1133) | <0.001 |
| Full‐fat | 2097 (1638–2557) | 1630 (1130–2129) | 1917 (1514–2320) | 32.0 (8.0–56.0)*** | −1418 (−2122 to −713.6) | <0.001 |
| Low‐fat | 310.6 (200.1–421.1) | 279.7 (193.0–366.3) | 445.0 (313.9–576.2) | 0.0 (0.0–0.1)*** | −414.1 (−599.4 to −228.7) | <0.001 |
| No‐fat | 1.7 (0.9–2.5) | 15.9 (0.0–37.6) | 23.4 (0.0–48.9) | 0.0 (0.0–0.0) | −37.6 (−70.8 to −4.3) | 0.03 |
| Nondairy alternatives | 4.5 (1.1–8.0) | 8.7 (1.4–15.9) | 5.9 (1.6–10.2) | 13.2 (9.0–17.4)* | +3.2 (−4.5 to +10.8) | 0.41 |
| Added fats | 1295 (1014‐1577) | 1384 (1024–1744) | 1332 (1091–1572) | 351.9 (271.4–432.4)*** | −1068 (−1500 to −636.4) | <0.001 |
| Animal fats | 636.7 (378.3–895.2) | 695.4 (344.7–1046) | 561.2 (363.9–758.5) | 29.3 (0.6–58.0)*** | −590.5 (−970.7 to −210.3) | 0.003 |
| Plant oils | 658.6 (556.8–760.4) | 688.5 (593.0–784.0) | 770.4 (670.2–870.5) | 322.6 (260.2–384.9)*** | −477.7 (−651.0 to −304.4) | <0.001 |
| Added sugar | 116.8 (67.2–166.5) | 79.8 (25.4–134.3) | 168.6 (82.5–254.7) | 18.5 (10.7–26.3)*** | −113.1 (−208.5 to −17.7) | 0.02 |
| Sweetened beverages | 12.0 (8.4–15.5) | 8.7 (6.0–11.4)* | 10.1 (6.4–13.8) | 4.8 (3.0–6.5)** | −2.0 (−6.7 to +2.7) | 0.40 |
| Alcohol | 8.7 (5.4–12.1) | 5.9 (3.5–8.4) | 8.1 (4.5–11.7) | 4.1 (2.4–5.9)* | −1.1 (−5.6 to +3.3) | 0.61 |
Note: The results are presented as mean daily intakes with 95% confidence intervals.
Changes in dietary AGEs correlated with changes in body weight (r = +0.41; p < 0.001), fat mass (r = +0.38; p < 0.001), visceral fat (r = +0.23; p < 0.001), and PREDIM (r = −0.28; p < 0.001), and remained significant after adjustment for changes in energy intake (r = +0.35; p < 0.001 for body weight; r = +0.34; p < 0.001 for fat mass; r = +0.15; p = 0.03 for visceral fat; and r = −0.24; p < 0.001 for PREDIM).
4. DISCUSSION
This 16‐week randomized clinical trial found that the dietary AGEs decreased on a low‐fat plant‐based diet and that this reduction was associated with weight loss, reduction in body fat, and increase in insulin sensitivity in people who were overweight, even after adjustment for changes in energy intake.
Several studies have shown that a diet low in dietary AGEs is associated with reduced circulating AGE markers, weight loss, improved body composition, and other cardiometabolic outcomes. 12 , 15 , 16 , 22 A 2016 randomized clinical trial in 138 adults who were overweight with the metabolic syndrome found that a reduction in dietary AGEs by modifying the cooking methods, using boiling, stewing or steaming instead of frying, baking or grilling, keeping the diet composition otherwise constant, ameliorated insulin resistance in these individuals. 7 While that study changed cooking methods while encouraging participants to use the same foods as before, the current study achieved the reduction of AGEs by changing the diet composition so as to avoid the richest sources of dietary AGEs, that is, meat and high‐fat foods. 6 Both approaches reduced dietary AGEs, but the low‐fat plant‐based diet was more effective (the modified cooking methods reduced the dietary AGEs by 65% from about 15,000 to about 5200 ku/day, and the low‐fat vegan diet by 79%, from about 11,100 down to about 2300 ku/day), and both approaches also improved insulin sensitivity in individuals who were overweight. In addition, the low‐fat plant‐based diet resulted in weight loss and improved body composition (i.e., reduced fat mass and volume of visceral fat). In practice, the two approaches could be combined. However, changing dietary composition has practical advantages since plant‐based options are readily available at many restaurants and grocery stores, while it is more challenging to find establishments preparing foods without frying, baking, or grilling.
The present study showed that about 55% of the reduction of the dietary AGEs in the intervention group was attributable to the reduction in meat intake, 26% to decreased dairy intake, and 15% to decreased consumption of added fats. This is in accordance with the previous findings that meat and high‐fat foods contribute significantly to dietary AGEs, especially when prepared using dry heat (frying or baking). 6 Surprisingly, the reduction in white meat consumption made the biggest difference in dietary AGEs coming from meat (59%), followed by processed meat (27%). The reason lies mainly in the quantity of ingested white meat. The Dietary Guidelines for Americans (2020–2025) state that a healthy dietary pattern can include lean meats and poultry, but should involve “relatively lower consumption of red and processed meats”. 23 This recommendation is likely further re‐enforcing the upward trend in white meat consumption in the U.S., 24 despite the fact that observational studies have found an increased risk of incident cardiovascular disease both for red and white meat, 25 which is also supported by the findings from a randomized clinical trial that found similar effects of white and red meat on blood lipids and lipoproteins, 17 suggesting no benefit for choosing white over red meat for reducing cardiovascular risk.
Since AGEs are a modifiable risk factor for insulin resistance, metabolic syndrome, type 2 diabetes, and cardiovascular disease 26 and reducing dietary AGEs is effective in reducing the circulating levels of AGEs and improving markers of cardiometabolic health, 27 it is important to identify effective strategies that will help achieve these improvements, both in the prevention and treatment of chronic diseases. This study suggests that a low‐fat plant‐based diet is an effective strategy for reducing dietary AGEs, with associated cardiometabolic benefits for individuals who were overweight.
The potential mechanisms for the beneficial effects of a diet low in dietary AGEs include the less expressed direct metabolic effects of AGEs, but also the interplay with satiety hormones and inflammatory markers. In a meta‐analysis and systematic review of 13 articles, the comparative effects of diets low and high in dietary AGEs on obesity and satiety hormones were elucidated. Diets low in dietary AGEs were associated with a significant weight loss, a decrease in circulating levels of leptin, and an increase in adiponectin, 28 which would further support weight loss and long‐term weight management. Another meta‐analysis found that diets low in AGEs significantly decreased inflammatory markers, such as TNF‐α and 8‐isoprostnes in healthy individuals. 29
The strengths of the current study include a randomized, parallel design. The participants started the study concomitantly, accounting for seasonal effects. The duration of the study was reasonable to allow adaptation to the diet. The assessment of dietary AGEs is novel in a clinical trial using a plant‐based diet. In addition to tracking body weight, body composition and insulin sensitivity were measured, giving a broader picture of cardiometabolic health. A low attrition rate suggests that the plant‐based diet was sustainable, confirming the results of a prior long‐term study. 30
The study also has important limitations. The dietary AGEs were calculated based on self‐reported dietary intake records, which have well‐known limitations. 31 However, it is encouraging that the reported dietary changes correspond with weight loss, improved body composition, and increased insulin sensitivity. The dietary AGE database used to estimate dietary AGE intake includes about 560 food items and therefore some items consumed in the current cohort were not listed in it; in such cases a dietary AGE value was assigned based on the similarity of nutrient ingredients and methods of cooking with foods listed in the dietary AGE database. Moreover, dietary AGEs in the database used for this study were based on ELISA measurements, which have been criticized for being less precise than methods using mass spectrometry. 32 While the randomized trial was rigorously carried out, the detailed food group AGEs analysis is hypothesis‐generating, and no formal correction for the multiple food groups assessed was performed. Nevertheless, the high statistical magnitude (p < 0.001) of reported treatment effects and associations suggests that our findings are unlikely to be due to chance.
5. CONCLUSION
In conclusion, the dietary AGEs decreased after 16 weeks of a low‐fat plant‐based diet, and this reduction was associated with weight loss, reduced body fat, and increased insulin sensitivity in people who were overweight, even after adjustment for changes in energy intake. These findings support prior observations of the favorable effects of low‐AGE diets on weight, adiposity, and insulin resistance, and extend them to show that such effects can be achieved with qualitative dietary changes alone. Further research to confirm the outcomes of the study is warranted.
AUTHOR CONTRIBUTIONS
Hana Kahleova and Neal D. Barnard designed and executed the study; Tatiana Znayenko‐Miller and Jaime Uribarri prepared the data for analysis; Richard Holubkov performed the statistical analysis. All authors had full access to the data, contributed to the manuscript, and approved its final version.
CONFLICT OF INTEREST
Hana Kahleova, Tatiana Znayenko‐Miller, and Richard Holubkov received compensation from the Physicians Committee for Responsible Medicine for their work on this study. Jaime Uribarri does not report any conflict of interest. Neal D. Barnard is an Adjunct Professor of Medicine at the George Washington University School of Medicine. He serves without compensation as president of the Physicians Committee for Responsible Medicine and Barnard Medical Center in Washington, DC, nonprofit organizations providing educational, research, and medical services related to nutrition. He writes books and articles and gives lectures related to nutrition and health and has received royalties and honoraria from these sources.
ACKNOWLEDGMENTS
This work was funded by the Physicians Committee for Responsible Medicine.
Kahleova H, Znayenko‐Miller T, Uribarri J, Holubkov R, Barnard ND. Dietary advanced glycation products and their associations with insulin sensitivity and body weight: a 16‐week randomized clinical trial. Obes Sci Pract. 2023;9(3):235‐242. 10.1002/osp4.646
REFERENCES
- 1. Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of obesity and severe obesity among adults: United States, 2017‐2018. NCHS Data Brief. 2020(360):1‐8. [PubMed] [Google Scholar]
- 2. Malik VS, Willet WC, Hu FB. Nearly a decade on—trends, risk factors and policy implications in global obesity. Nat Rev Endocrinol. 2020;16(11):615‐616. 10.1038/s41574-020-00411-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Pillon NJ, Loos RJF, Marshall SM, Zierath JR. Metabolic consequences of obesity and type 2 diabetes: balancing genes and environment for personalized care. Cell. 2021;184(6):1530‐1544. 10.1016/j.cell.2021.02.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Uribarri J, del Castillo MD, de la Maza MP, et al. Dietary advanced glycation end products and their role in health and disease. Adv Nutr. 2015;6(4):461‐473. 10.3945/an.115.008433 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Uribarri J, Cai W, Sandu O, Peppa M, Goldberg T, Vlassara H. Diet‐derived advanced glycation end products are major contributors to the body’s AGE pool and induce inflammation in healthy subjects. Ann N Y Acad Sci. 2005;1043(1):461‐466. 10.1196/annals.1333.052 [DOI] [PubMed] [Google Scholar]
- 6. Uribarri J, Woodruff S, Goodman S, et al. Advanced glycation end products in foods and a practical guide to their reduction in the diet. J Am Diet Assoc. 2010;110(6):911‐916. 10.1016/j.jada.2010.03.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Vlassara H, Cai W, Tripp E, et al. Oral AGE restriction ameliorates insulin resistance in obese individuals with the metabolic syndrome: a randomised controlled trial. Diabetologia. 2016;59(10):2181‐2192. 10.1007/s00125-016-4053-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Meerwaldt R, Links T, Zeebregts C, Tio R, Hillebrands J‐L, Smit A. The clinical relevance of assessing advanced glycation endproducts accumulation in diabetes. Cardiovasc Diabetol. 2008;7(1):29. 10.1186/1475-2840-7-29 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Indyk D, Bronowicka‐Szydełko A, Gamian A, Kuzan A. Advanced glycation end products and their receptors in serum of patients with type 2 diabetes. Sci Rep. 2021;11(1):13264. 10.1038/s41598-021-92630-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Rizzo NS, Sabaté J, Jaceldo‐Siegl K, Fraser GE. Vegetarian dietary patterns are associated with a lower risk of metabolic syndrome: the adventist health study 2. Diabetes Care. 2011;34(5):1225‐1227. 10.2337/dc10-1221 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Tonstad S, Butler T, Yan R, Fraser GE. Type of vegetarian diet, body weight, and prevalence of type 2 diabetes. Diabetes Care. 2009;32(5):791‐796. 10.2337/dc08-1886 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. de Courten B, de Courten MP, Soldatos G, et al. Diet low in advanced glycation end products increases insulin sensitivity in healthy overweight individuals: a double‐blind, randomized, crossover trial. Am J Clin Nutr. 2016;103(6):1426‐1433. 10.3945/ajcn.115.125427 [DOI] [PubMed] [Google Scholar]
- 13. Kahleova H, Petersen KF, Shulman GI, et al. Effect of a low‐fat vegan diet on body weight, insulin sensitivity, postprandial metabolism, and intramyocellular and hepatocellular lipid levels in overweight Adults: a randomized clinical trial. JAMA Netw Open. 2020;3(11):e2025454. 10.1001/jamanetworkopen.2020.25454 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Schakel SF, Sievert YA, Buzzard IM. Sources of data for developing and maintaining a nutrient database. J Am Diet Assoc. 1988;88(10):1268‐1271. 10.1016/s0002-8223(21)07997-9 [DOI] [PubMed] [Google Scholar]
- 15. Mark AB, Poulsen MW, Andersen S, et al. Consumption of a diet low in advanced glycation end products for 4 weeks improves insulin sensitivity in overweight women. Diabetes Care. 2014;37(1):88‐95. 10.2337/dc13-0842 [DOI] [PubMed] [Google Scholar]
- 16. Macías‐Cervantes MH, Rodríguez‐Soto JMD, Uribarri J, Díaz‐Cisneros FJ, Cai W, Garay‐Sevilla ME. Effect of an advanced glycation end product‐restricted diet and exercise on metabolic parameters in adult overweight men. Nutrition. 2015;31(3):446‐451. 10.1016/j.nut.2014.10.004 [DOI] [PubMed] [Google Scholar]
- 17. Bergeron N, Chiu S, Williams PT, M King S, Krauss RM. Effects of red meat, white meat, and nonmeat protein sources on atherogenic lipoprotein measures in the context of low compared with high saturated fat intake: a randomized controlled trial. Am J Clin Nutr. 2019;110(1):24‐33. 10.1093/ajcn/nqz035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Hagströmer M, Oja P, Sjöström M. The International Physical Activity Questionnaire (IPAQ): a study of concurrent and construct validity. Publ Health Nutr. 2006;9(6):755‐762. 10.1079/phn2005898 [DOI] [PubMed] [Google Scholar]
- 19. Kaul S, Rothney MP, Peters DM, et al. Dual‐energy X‐ray absorptiometry for quantification of visceral fat. Obesity. 2012;20(6):1313‐1318. 10.1038/oby.2011.393 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Neeland IJ, Grundy SM, Li X, Adams‐Huet B, Vega GL. Comparison of visceral fat mass measurement by dual‐X‐ray absorptiometry and magnetic resonance imaging in a multiethnic cohort: the Dallas Heart Study. Nutr Diabetes. 2016;6(7):e221. 10.1038/nutd.2016.28 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Tura A, Chemello G, Szendroedi J, et al. Prediction of clamp‐derived insulin sensitivity from the oral glucose insulin sensitivity index. Diabetologia. 2018;61(5):1135‐1141. 10.1007/s00125-018-4568-4 [DOI] [PubMed] [Google Scholar]
- 22. Baye E, de Courten MP, Walker K, et al. Effect of dietary advanced glycation end products on inflammation and cardiovascular risks in healthy overweight adults: a randomised crossover trial. Sci Rep. 2017;7(1):4123. 10.1038/s41598-017-04214-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Dietary Guidelines for Americans, 2020‐2025 . 9th ed. 2020. DietaryGuidelines.gov: 164.
- 24. Daniel CR, Cross AJ, Koebnick C, Sinha R. Trends in meat consumption in the United States. Publ Health Nutr. 2011;14(4):575‐583. 10.1017/s1368980010002077 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Zhong VW, Van Horn L, Greenland P, et al. Associations of processed meat, unprocessed red meat, poultry, or fish intake with incident cardiovascular disease and all‐cause mortality. JAMA Intern Med. 2020;180(4):503‐512. 10.1001/jamainternmed.2019.6969 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Uribarri J, Cai W, Woodward M, et al. Elevated serum advanced glycation endproducts in obese indicate risk for the metabolic syndrome: a link between healthy and unhealthy obesity? J Clin Endocrinol Metab. 2015;100(5):1957‐1966. 10.1210/jc.2014-3925 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Baye E, Kiriakova V, Uribarri J, Moran LJ, de Courten B. Consumption of diets with low advanced glycation end products improves cardiometabolic parameters: meta‐analysis of randomised controlled trials. Sci Rep. 2017;7(1):2266. 10.1038/s41598-017-02268-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Sohouli MH, Sharifi‐Zahabi E, Lari A, Fatahi S, Shidfar F. The impact of low advanced glycation end products diet on obesity and related hormones: a systematic review and meta‐analysis. Sci Rep. 2020;10(1):22194. 10.1038/s41598-020-79216-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Kellow NJ, Savige GS. Dietary advanced glycation end‐product restriction for the attenuation of insulin resistance, oxidative stress and endothelial dysfunction: a systematic review. Eur J Clin Nutr. 2013;67(3):239‐248. 10.1038/ejcn.2012.220 [DOI] [PubMed] [Google Scholar]
- 30. Barnard ND, Gloede L, Cohen J, et al. A low‐fat vegan diet elicits greater macronutrient changes, but is comparable in adherence and acceptability, compared with a more conventional diabetes diet among individuals with type 2 diabetes. J Acad Nutr Diet. 2009;109(2):263‐272. 10.1016/j.jada.2008.10.049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Yuan C, Spiegelman D, Rimm EB, et al. Relative validity of nutrient intakes assessed by Questionnaire, 24 hour recalls, and diet records as compared with urinary recovery and plasma concentration biomarkers: findings for women. Am J Epidemiol. 2018;187(5):1051‐1063. 10.1093/aje/kwx328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Scheijen JLJM, Clevers E, Engelen L, et al. Analysis of advanced glycation endproducts in selected food items by ultra‐performance liquid chromatography tandem mass spectrometry: presentation of a dietary AGE database. Food Chem. 2016;190:1145‐1150. 10.1016/j.foodchem.2015.06.049 [DOI] [PubMed] [Google Scholar]