

Abstract
Background
Parathyroid carcinoma (PC) is an uncommon cause of primary hyperparathyroidism (PHPT) and particularly rare in the mediastinum. Herein, we present a case of mediastinal PC and conduct a related literature review.
Case presentation
We described a case of a 50-year-old female patient with PHPT due to mediastinal PC. She was initially admitted to a local hospital in her hometown with hypercalcemia and high blood concentrations of PTH (parathyroid hormone). The patient underwent neck parathyroidectomy and pathological examination suggested parathyroid adenoma. Although the overproduction of serum calcium and PTH declined after the surgery, calcium and PTH increased again one month later, so the patient was transferred to our hospital. A 99mTc-sestamibi scan revealed an ectopic finding in the mediastinum, which was also indicated on the CT image. After removing the mediastinal mass, the metabolism of calcium and PTH quickly reverted to normal and the pathologic features of the mass were consistent with PC. By reviewing the related literature, we noticed that only scattered reports were published before 1982, and those were not included in the present review due to their differences with current radiological examination and treatment methods. After excluding outdated studies, we summarized and analyzed 20 reports of isolated mediastinal PC and concluded that. Parathyroidectomy remains the only curative treatment for the disease. Furthermore, the success of treatment directly depends on accurate preoperative localization.
Conclusion
With this study, we emphasize the importance of accurate preoperative diagnosis of mediastinal PC and improve clinicians’ understanding of the disease.
Keywords: Primary hyperparathyroidism, Parathyroid carcinoma, Ectopic, Mediastinum, Case report
Background
Parathyroid carcinoma (PC) is a rare endocrine disease, that accounts for 1-5% of all causes of sporadic primary hyperparathyroidism (PHPT) in North America, major western countries, and in Japan [1, 2]. Only 6–16% of parathyroid tumor can be found in ectopic locations such as the thyroid, the thymus, or behind the esophagus [3], and the condition rarely affects the mediastinum [4].
PC generally develops slowly [5], and many tumors are hormonally functional, which means they can induce excessive synthesis and secretion of parathyroid hormone (PTH) and hyper calcium, affecting multiple systems and organs. Patients may manifest a variety of symptoms, including gastrointestinal discomfort, osteoporosis, bone pain and pathologic fracture [6]. The diagnosis of mediastinal PC is typically very challenging, because of the nature of the disease (slow growth, and atypical symptoms in some patients) and ectopic locations for the parathyroid glands [7].
In this study, we reported an unusual case of PHPT caused by PC in the mediastinum and reviewed the related literature to raise awareness of disease diagnosis.
Case presentation
A 50-year-old female was initially admitted to a local hospital in her hometown with a 3-month history of nausea, emesis, asthenia and moderate backache. High levels of serum calcium (4.3 mmol/L, with the normal range at 2-2.8 mmol/L) and PTH (129.5 pmol/L, normal, 1.6–6.9 pmol/L) were detected. Although neck ultrasonography revealed an increase in the volume of the parathyroid glands, no further examinations were performed at the time to determine whether there was a possibility of ectopic lesions. A left-sided parathyroidectomy and bilateral subtotal thyroidectomy were subsequently performed and pathological examination revealed parathyroid adenoma (2 × 1.5 cm) and nodular goiter. The patient’s hypercalcemia was resolved with decreasing levels of PTH observed after the operation. However, the woman developed more sever nausea and asthenia one month later, and her levels of serum calcium and PTH increased again.
After the patient was referred to our hospital, our priority was to lower her serum calcium levels while initiating diagnostic procedures to elucidate the lesion site as soon as the hypercalcemic crisis had been diagnosed. Physical examination showed that the patient’s vital signs were normal but reveled that she had difficulties in walking. However, no lumps were identified on her neck. Laboratory assessments revealed a serum calcium level of 4.63 mmol/L (normal, 2.11–2.52 mmol/L), urinary calcium level of 15.7 mmol/24 h (normal, 2.5–7.5 mmol/24 h), serum PTH of 1562.3 pg/mL (normal, 8.5–88 pg/mL), serum BUN of 13.9 mmol/L (normal, 2.6–7.5 mmol/L), and serum creatinine of 174 umol/L (normal, 41–73 umol/L).
X-ray revealed a previously undetected fracture of the left superior pubic ramus, and examination of bone mineral density (BMD) using dual-energy X-ray absorptiometry revealed decreased density in the lumbar spine (T score = − 2.6). Furthermore, ultrasonography of the patient’s urinary system revealed the presence of bilateral renal calculi. Although cervical ultrasonography did not detect any abnormalities, computed tomography (CT) of the chest showed a low-density mass in the upper-middle mediastinum, approximately 6.7 cm×4.8 cm in size (Fig. 1a), importantly, 99mTc-hexakis-2-methoxyisobuthylisonitrile (99mTc-MIBI) scintigraphy showed increased uptake in a location identical to that in the CT scan image (Fig. 1b, c). To exclude the diagnosis of multiple endocrine neoplasia (MEN), pituitary magnetic resonance imaging (MRI) and abdominal CT were performed. The images of pituitary and adrenal glands were normal, but abdominal CT revealed a sign of acute pancreatitis (Fig. 2). However, serum amylase and lipase levels were normal, and no family member carried a medical history of hyperparathyroidism, pituitary tumor, thyroid medullary carcinoma, or pheochromocytoma.
Fig. 1.

CT imaging and scintigraphic analysis using technetium-99 m. a A mass is found in the mediastinum on CT imaging. b, c Parathyroid scintigraphy shows high focal radiotracer uptake at 15 and 90 min after injection of 99mTc-sestamibi
Fig. 2.
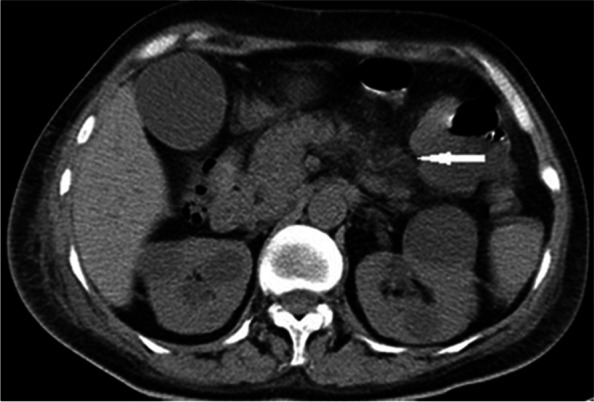
CT image of the abdomen. The CT scan image shows an enlarged pancreas with indistinct boundaries and surrounding exudates
Subsequently, the patient underwent right thoracotomy and a mass measuring 6.8 cm×4.9 cm×5.3 cm was resected. The lymph node dissection was not performed since there were no obviously swollen lymph nodes seen around the tumor. Levels of serum calcium (2.42 mmol/L) and PTH (19.2 pg/mL) returned to normal after the operation. Over subsequent days, blood calcium concentrations declined, and intravenous infusion of calcium gluconate and oral vitamin D3 was administrated to correct these abnormalities. Postoperative pathological evaluation of the resected specimen disclosed a parathyroid adenocarcinoma due to vascular invasion and Ki-67 positivity in approximately 10% of the tumor cells (Fig. 3). Other immunochemical examinations showed PAX-8 (+), PTH (+), galectin-3 (-), syn (-),CgA (+), cyclin D1(+), and CEA (−).After 20 days of hospitalization, the patient was discharged and treated with oral calcium carbonate (3 g/day) and calcitriol (0.5 ug/day). She did not exhibit any signs of recurrence during a six-month follow-up.
Fig. 3.

Histopathological and immunohistochemical findings. a Histological evaluation shows vascular invasion by parathyroid tumor cells (H&E, ×40). b Immunohistochemical findings show that approximately 10% of the tumor cells were Ki-67 positive (×100)
Literature review
We systematically searched PubMed for reports of isolated mediastinal parathyroid carcinoma in humans using the terms “parathyroid carcinoma (or cancer), mediastinal”. The cut-off time for retrieval was December 2020, and we only considered results in English language only. Furthermore, we excluded irrelevant documents (such as those on parathyroid adenoma, parathyroid hyperplasia, PC caused by secondary hyperparathyroidism) by manual screening. The first case of mediastinal parathyroid carcinoma was reported by Weissman in 1957 [8] and we identified that there were only scattered reports published before 1982, which were not included in this review due to their inherent differences with current radiological examination and treatment methods [9, 10]. Table 1 summarized 20 cases included in our final sample [11–30].
Table 1.
Literature review of published mediastinal parathyroid carcinoma cases
| Case | Age/sex | presenting symptoms | Calcium (mmol/L) |
PTH (pg/ml) |
size of tumor (cm) |
radiological studies | surgical approach/ operation num |
References |
|---|---|---|---|---|---|---|---|---|
| 1 | 34/F | kidney stones, osteitis fibrosa cystica, recurrent acute pancreatitis | 4.7 | 3304 | 6 × 3.5 × 3 | US,CT,MIBI | transcervical surgery and median sternotomy/3 | Jiajue R et al [11] |
| 2 | 53/F | backache, multiple fractures, nausea, vomiting, fatigue, and unexplained myocardial ischemia-like symptoms. | 3.7 | >1900 | 4 × 3 × 2.5 | US, MRI,MIBI | sternotomy/1 | Xin Y et al [12] |
| 3 | 53/M | fatigue, polyuria, night sweats and renal stones | 3.4 | 2630 | 5 × 3 × 3 | US,CT,MIBI | transthorascopic surgery/1 | Cao C et al [13] |
| 4 | 72/M | severe epigastric pain | 3.5 | 168 | 2 × 1.5 × 1 | US, MRI,MIBI | lower cervical collar incision/1 | Tseng CW et al [14] |
| 5 | 54/M | fatigue, ostealgia and myalgia | 6.2 | / | 4 cm in diameter | / | NA | Peshev ZV et al [15] |
| 6 | 28/M | nausea, ostealgia, fatigue, edema | 5.83 | 2307 | 3.7 × 3.2 × 4.3 | CT, MIBI | thoracotomy/1 | Meng Z et al [16] |
| 7 | 23/M | recurrent fractures and osteoporosis | 3.58 | >2306 | 3.6 × 2.5 | US, CT,MIBI | median sternotomy/1 | Yong T et al [17] |
| 8 | 61/M | kidney stones | 1.9 | 1220 | 0.85 × 0.5 × 0.38 | CT, MIBI | neck collar incision/1 | Iwata T et al [18] |
| 9 | 10/boy | / | >3.75 | >3000 | 2 × 2 × 2.5 | US, MIBI | exploration of the neck/1 | Righi A et al [19] |
| 10 | 66/F | bone and joint pain | 2.83 | 124 | 3 cm in diameter | US,CT,MIBI | median sternotomy/1 | Damadi A et al [20] |
| 11 | 84/F | Progressive dyspnea, severe osteoporosis with hip and vertebral fractures | 2.8 | 230 | / | CT,MR angiography | NA | Vazquez FJ et al [21] |
| 12 | 55/M | fatigue, weight loss, mild lumbar pain, severe uremia | 2.49 | 2807 | 2.7 cm in diameter | CT, MIBI | no detailed information/2 | Tkaczyk M et al [22] |
| 13 | 27/M | skeletal symptoms | 2.96 | 1412 | / | CT, MIBI | exploration of the neck and median sternotomy/3 | Srouji IA et al [23] |
| 14 | 33/M | fatigue, decreased motivaton | 3.35 | 722 | 3 × 2 × 1 | CT, MIBI | exploration of the neck /1 | Chandran M et al [24] |
| 15 | 43/M | thirst, polyuria | 3.53 | / | MIBI | no detailed information/2 | Yamashita K et al. [25] | |
| 16 | 44/M | hematuria, flank pain | 4.14 | 964.81 | 5 × 5 × 2.5 | US, MIBI | exploration of the neck and median sternotomy/2 | Delaney SE et al [26] |
| 17 | 62/F | recurrent renal colic, thirst, vague abdominal pain, hoarseness | 3.62 | 275 | 3 cm in diameter | CT | exploration of the neck and median sternotomy/2 | Kelly MD et al [27] |
| 18 | 47/M | shortness of breath, hoarseness, dysphagia | 4.38 | 6500 | / | CT | exploration of the neck and median sternotomy/1 | Putnam JB et al [28] |
| 19 | 57/F | marked osteopenia, fatigue | 4.06 | >3000 | 5 cm in diameter | CT | exploration of the neck and sternotomy/2 | Kastan DJ et al [29] |
| 20 | 51/M | hoarseness, productive cough, dyspnea on exertion | / | / | a large mass (no exact value) | chest x-ray | no detailed information/1 | Murphy MN et al [30] |
Discussion and conclusions
In the majority of patients, PHPT is caused by benign adenomas that are located close to the thyroid gland [31]. Approximately 6-30% of patients with PHPT have ectopic parathyroid glands [32], but when it comes to parathyroid cancer, a slow-growing malignancy, accounts for less than 1% of the causes of hyperparathyroidism [33]. Ectopic parathyroid glands are found in some anatomic locations of the body, such as the mediastinum, and intrathymic and retro/paraesophageal sites [34], which can be explained by their embryologic origin [34, 35]. The parathyroid glands originate from the endodermal tissue and develop in association with the thymus from the third pharyngeal pouch, and may then migrate into the mediastinum [36]. Cases of mediastinal PCs are rare, which makes them difficult to diagnose. They are usually sporadic, while the familial form is observed in approximately 5% of cases. Among the reports we accessed for our literature review, only one reported a case of familial form in an individual diagnosed with FIHP (familial isolated hyperparathyroidism) [25].
The clinical manifestations of parathyroid carcinoma are majorly caused by the effects of excessive secretion of PTH from the tumor rather than by the infiltration of the tumor into other organs [16]. Thus, signs and symptoms of hypercalcemia are often reported, which include renal stone formation, and gastric /duodenal ulceration commonly accompanied by digestive discomfort, fatigue, weight loss, backache, osteoporosis, and fracture [6], as we noticed in our patient. High levels of serum calcium and parathyroid hormone are the most recognizable and characteristic abnormalities of the biochemical features of PCs. Compared with patients with adenomatous PHPT, patients with parathyroid carcinoma usually exhibit much higher serum calcium levels, which may then lead to hypercalcemic crisis [37, 38]. The proportion of cases with a serum calcium level greater than 3.5 mmol/L was as high as 60% (12/20) in our reviewed cases (Table 1). However, cases of non-secretory parathyroid cancer in the mediastinum also have to be considered [30] and that is why a diagnosis of PC cannot rely solely on the clinical manifestations and related biochemical abnormalities, and shall also involve the results of pathological examination after performing the resection of the gland.
Currently, surgical interventions is the best treatment for PHPT caused by mediastinal parathyroid carcinoma and the success of the procedure largely depend on the precise localization of the parathyroid tumor. Therefore, accurate preoperative diagnosis of ectopic lesions is critical part of the recovery process. Localization examinations include ultrasonography, CT, MRI and parathyroid scintigraphy with 99mTc-MIBI, the latter being the most effective method, especially with ectopic parathyroid lesions [39]. The sensitivity rate of 99mTc-MIBI is 68-86% and its specificity rate reaches as high as 98.3% in localization of parathyroid adenomas [40, 41]. False positives may appear in thymomas, which are usually rich in mitochondria that absorb the tracer well [42], whereas negative results are more common in multiple adenomas or hyperplasia [43]. Our literature review revealed that 14 patients were performed with 99mTc-MIBI, and the results were all positive. However, the effectiveness of this technique depends on the size of the gland. It is worth mentioning that four-dimensional CT and 3T MRI can be favorable supplemental techniques to improve this process [40, 44].
Our patient demonstrated relevant clinical manifestations, and the markedly elevated PTH levels and hypercalcemia led to the preoperative suspicion of PC. Unfortunately, the local surgeons did not properly investigate the location of the tumor and then directly removed the parathyroid gland in the neck. At our department, a mass in the mediastinum identified with CT scan showed an elevated uptake rate of 99mTc-MIBI, which eventually confirmed the diagnosis of parathyroid carcinoma. If hyperparathyroidism is diagnosed, clinicians should consider the existence of ectopic glands and improve relevant examinations to avoid unnecessary harm to the patient.
The most effective therapy is undoubtedly complete surgical resection, which is recommended for all symptomatic patients and most asymptomatic patients [6, 40, 42], and a variety of surgical approaches to remove tumors have already been explored. Traditionally, median sternotomy or thoracotomy involving an open operation was used for patients with deep mediastinal parathyroid lesions. Recently, thoracoscopic surgery was considered a safe and feasible method for the resection of mediastinal parathyroid tumor [39], and a cervical approach may be appropriate for the excision of lesions located in the aortic arch or upper region [39]. Our patient underwent a traditional thoracotomy because the tumor was large and compressed the surrounding blood vessel (the superior vena cava). Intriguingly, we uncovered in our literature review of mediastinal parathyroid carcinoma that among patients with distinct records of surgical procedures, 10 out of 15 cases had undergone open chest surgery (including sternotomy or thoracotomy), which might be related to large tumor size. Furthermore, ectopic mediastinal PC is considered an important indicator associated with surgical recidivism. In the reports we analyzed, 38.9% of diagnosed cases with surgical records underwent two or more operations (Table 1). The treatments of metastatic and non-resectable PC are still limited and therapeutic methods such as chemotherapy, radiotherapy, and radiofrequency ablation of metastasis were associated with positive outcomes in several case reports [45]. When the cancer is widely metastasized and there is no opportunity for surgery, controlling hypercalcemia remains the primary treatment for patients [46].
Ultimately, the effective diagnosis of PC requires pathological examination for further confirmation, which often poses diagnostic challenges [47]. The main difficulty in histological examinations is to distinguish PC from atypical adenomas, in the latter tumors share some histological features with PC, e.g., diffuse growth pattern, fibrous septa, and high mitotic activity [45]. The unequivocal histological criteria for PC, however, should be restricted to those tumors that invade adjacent tissues, blood vessels, and perineural spaces or to those tumors that produce distant metastases [48]. In addition, immunohistochemical staining for parafibromin can help avoid diagnostic errors. The negative staining of parafibromin and overexpression of Ki-67(> 5%) are highly relevant to PC [28, 33]. In the case of our patient, her diagnosis was confirmed due to the vascular invasion and high levels of immunohistochemical Ki-67(10%).
It is equally important to acknowledge the limitations of our study. Firstly, we were unable to adequately obtain the medical records from the patient’s initial visit to her local hospital. Secondly, the patient’s diagnosis of osteoporosis was only based on the T-score of the lumbar spine, we should improve it by giving patients multi-site DXA scan (lumbar spine, femoral neck, forearm and total hip) to assess their BMD more completely. Thirdly, parafibromin immunohistochemical staining is important in the diagnosis of PC, the lack of which in our case might make the diagnosis less persuasive. Nevertheless, we consider our diagnosis is unequivocal based on the combined evidence (vascular invasion and overexpression of Ki-67). Regarding our literature review, we may still have missed a small number of cases even after conducting a careful manual screening.
Our study highlights the necessity of accurate diagnosis in the management of PC in the mediastinum by reporting an unusual case and conducting a corresponding literature review. In challenging cases like ours, ectopic parathyroid lesions (including mediastinal tumor) must be considered to avoid the need of reoperation and accompanying related risks to patients.
Acknowledgements
Not applicable.
Abbreviations
- PTCA
Parathyroid carcinoma
- PHPT
Primary hyperparathyroidism
- PTH
Parathyroid hormone
- MEN
Multiple endocrine neoplasia
- FIHP
Familial isolated hyperparathyroidism
- 99mTc-MIBI
99mTc-hexakis2-methoxyisobuthylisonitrile
Authors’ contributions
YB conceived, designed, and wrote the review. Gj K performed the operation for the patient. Xy W provided pathological analysis. JL revised the review. YH and YW contributed to collect the data. All authors read and approved the final manuscript.
Funding
Not applicable.
Availability of data and materials
All the data supporting our findings are contained within the manuscript.
Declarations
Ethics approval and consent to participate
All procedures performed in studies involving human participant were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the Medical Ethics Committees of Renmin Hospital of Wuhan University.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Competing interests
Yan Bao, Ganjun Kang, Xiaoyan Wu, Jing Li, Yan Huang and Ye Wang declare that they have no conflict of interest.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Cetani F, Pardi E, Marcocci C. Update on parathyroid carcinoma. J Endocrinol Invest. 2016;39(6):595–606. doi: 10.1007/s40618-016-0447-3. [DOI] [PubMed] [Google Scholar]
- 2.Harari A, Waring A, Fernandez-Ranvier G, Hwang J, Suh I, Mitmaker E, et al. Parathyroid carcinoma: a 43-year outcome and survival analysis. J Clin Endocrinol Metab. 2011;96(12):3679–86. doi: 10.1210/jc.2011-1571. [DOI] [PubMed] [Google Scholar]
- 3.Rawat N, Khetan N, Williams DW, Baxter JN. Parathyroid carcinoma. Br J Surg. 2005;92(11):1345–53. doi: 10.1002/bjs.5182. [DOI] [PubMed] [Google Scholar]
- 4.Do Cao C, Aubert S, Trinel C, Odou MF, Bayaram M, Patey M. Parathyroid carcinoma: diagnostic criteria, classification, evaluation. Ann Endocrinol (Paris) 2015;76(2):165–8. doi: 10.1016/j.ando.2015.03.016. [DOI] [PubMed] [Google Scholar]
- 5.Fang SH, Lal G. Parathyroid cancer. Endocr Pract. 2011;17(Suppl 1):36–43. doi: 10.4158/EP10310.RA. [DOI] [PubMed] [Google Scholar]
- 6.Walker MD, Silverberg SJ. Primary hyperparathyroidism. Nat Rev Endocrinol. 2018;14(2):115–25. doi: 10.1038/nrendo.2017.104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kebebew E, Arici C, Duh QY, Clark OH. Localization and reoperation results for persistent and recurrent parathyroid carcinoma. Arch Surg. 2001;136(8):878–85. doi: 10.1001/archsurg.136.8.878. [DOI] [PubMed] [Google Scholar]
- 8.Weissman I, Worden JP, Christie JM. Mediastinal parathyroid carcinoma with metastases; report of a case and review of the literature. Radiology. 1957;68(3):352–7. doi: 10.1148/68.3.352. [DOI] [PubMed] [Google Scholar]
- 9.Scholz DA, Purnell DC, Woolner LB, Clagett OT. Mediastinal hyperfunctioning parathyroid tumors: review of 14 cases. Ann Surg. 1973;178(2):173–8. doi: 10.1097/00000658-197308000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Krudy AG, Doppman JL, Marx SJ, Brennan MF, Spiegel A, Aurback GD. Radiographic findings in recurrent parathyroid carcinoma. Radiology. 1982;142(3):625–9. doi: 10.1148/radiology.142.3.7063676. [DOI] [PubMed] [Google Scholar]
- 11.Jiajue R, Song A, Wang O, Li W. Persistent Hypercalcemia Crisis and recurrent Acute Pancreatitis due to multiple ectopic parathyroid carcinomas: Case Report and Literature Review of Mediastinal Parathyroid Carcinoma. Front Endocrinol (Lausanne) 2020;11:647. doi: 10.3389/fendo.2020.00647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Xin Y, Zhao T, Wei B, Gu H, Jin M, Shen H, et al. Intrapericardial parathyroid carcinoma: a case report. Endocrine. 2020;69(2):456–60. doi: 10.1007/s12020-020-02283-8. [DOI] [PubMed] [Google Scholar]
- 13.Cao C, Dou C, Chen F, Wang Y, Zhang X, Lai H. An unusual mediastinal parathyroid carcinoma coproducing PTH and PTHrP: a case report. Oncol Lett. 2016;11(6):4113–6. doi: 10.3892/ol.2016.4548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Tseng CW, Lin SZ, Sun CH, Chen CC, Yang AH, Chang FY, et al. Ectopic mediastinal parathyroid carcinoma presenting as acute pancreatitis. J Chin Med Assoc. 2013;76(2):108–11. doi: 10.1016/j.jcma.2011.10.015. [DOI] [PubMed] [Google Scholar]
- 15.Peshev ZV, Borisov BB, Genova SN, Danev VH. Parathyroid carcinoma of the mediastinum. Folia Med (Plovdiv) 2012;54(4):80–3. doi: 10.2478/v10153-012-0010-8. [DOI] [PubMed] [Google Scholar]
- 16.Meng Z, Li D, Zhang Y, Zhang P, Tan J. Ectopic parathyroid carcinoma presenting with hypercalcemic crisis, ectopic uptake in bone scan and obstruction of superior vena cava. Clin Nucl Med. 2011;36(6):487–90. doi: 10.1097/RLU.0b013e31820ae007. [DOI] [PubMed] [Google Scholar]
- 17.Yong TY, Li JY. Mediastinal parathyroid carcinoma presenting with severe skeletal manifestations. J Bone Miner Metab. 2010;28(5):591–4. doi: 10.1007/s00774-010-0173-4. [DOI] [PubMed] [Google Scholar]
- 18.Iwata T, Inoue K, Morita R, Mizuguchi S, Tsukioka T, Onoda N, et al. Functional large parathyroid carcinoma extending into the superior mediastinum. Ann Thorac Cardiovasc Surg. 2008;14(2):112–5. [PubMed] [Google Scholar]
- 19.Righi A, Dimosthenous K, Mize J. Mediastinal parathyroid carcinoma with tumor implants in a child: a unique occurrence. Int J Surg Pathol. 2008;16(4):458–60. doi: 10.1177/1066896908315821. [DOI] [PubMed] [Google Scholar]
- 20.Damadi A, Harkema J, Kareti R, Saxe A. Use of pre-operative Tc99m-Sestamibi scintigraphy and intraoperative parathyroid hormone monitoring to eliminate neck exploration in mediastinal parathyroid adenocarcinoma. J Surg Educ. 2007;64(2):108–12. doi: 10.1016/j.jsurg.2006.10.005. [DOI] [PubMed] [Google Scholar]
- 21.Vazquez FJ, Aparicio LS, Gallo CG, Diehl M. Parathyroid carcinoma presenting as a giant mediastinal retrotracheal functioning cyst. Singap Med J. 2007;48(11):e304–7. [PubMed] [Google Scholar]
- 22.Tkaczyk M, Czupryniak A, Nowicki M. Ectopic mediastinal parathyroid carcinoma as a cause of dialysis-dependent renal failure. Hemodial Int. 2007;11(4):398–402. doi: 10.1111/j.1542-4758.2007.00207.x. [DOI] [PubMed] [Google Scholar]
- 23.Srouji IA, Resouly A, Cree IA. Case of thymic parathyroid carcinoma in a haemodialysis patient: application of tumour chemosensitivity testing. J Laryngol Otol. 2004;118(2):162–4. doi: 10.1258/002221504772784685. [DOI] [PubMed] [Google Scholar]
- 24.Chandran M, Deftos LJ, Stuenkel CA, Haghighi P, Orloff LA. Thymic parathyroid carcinoma and postoperative hungry bone syndrome. Endocr Pract. 2003;9(2):152–6. doi: 10.4158/EP.9.2.152. [DOI] [PubMed] [Google Scholar]
- 25.Yamashita K, Suzuki S, Yumita W, Ikeo Y, Uehara Y, Minemura K, et al. A case of familial isolated hyperparathyroidism with ectopic parathyroid cancer. Endocr J. 2001;48(4):453–8. doi: 10.1507/endocrj.48.453. [DOI] [PubMed] [Google Scholar]
- 26.Delaney SE, Wermers RA, Thompson GB, Hodgson SF, Dinneen SF. Mediastinal parathyroid carcinoma. Endocr Pract. 1999;5(3):133–6. doi: 10.4158/EP.5.3.133. [DOI] [PubMed] [Google Scholar]
- 27.Kelly MD, Sheridan BF, Farnsworth AE, Palfreeman S. Parathyroid carcinoma in a mediastinal sixth parathyroid gland. Aust N Z J Surg. 1994;64(6):446–9. doi: 10.1111/j.1445-2197.1994.tb02251.x. [DOI] [PubMed] [Google Scholar]
- 28.Putnam JB, Schantz SP, Pugh WC, Hickey RC, Samaan NA, Garza R, et al. Extended en bloc resection of a primary mediastinal parathyroid carcinoma. Ann Thorac Surg. 1990;50(1):138–40. doi: 10.1016/0003-4975(90)90109-J. [DOI] [PubMed] [Google Scholar]
- 29.Kastan DJ, Kottamasu SR, Frame B, Greenwald KA. Carcinoma in a mediastinal fifth parathyroid gland. JAMA. 1987;257(9):1218–9. doi: 10.1001/jama.1987.03390090090030. [DOI] [PubMed] [Google Scholar]
- 30.Murphy MN, Glennon PG, Diocee MS, Wick MR, Cavers DJ. Nonsecretory parathyroid carcinoma of the mediastinum. Light microscopic, immunocytochemical, and ultrastructural features of a case, and review of the literature. Cancer. 1986;58(11):2468–76. doi: 10.1002/1097-0142(19861201)58:11<2468::AID-CNCR2820581120>3.0.CO;2-M. [DOI] [PubMed] [Google Scholar]
- 31.Ruda JM, Hollenbeak CS, Stack BC. A systematic review of the diagnosis and treatment of primary hyperparathyroidism from 1995 to 2003. Otolaryngol Head Neck Surg. 2005;132(3):359–72. doi: 10.1016/j.otohns.2004.10.005. [DOI] [PubMed] [Google Scholar]
- 32.Moran CA, Suster S. Primary parathyroid tumors of the mediastinum: a clinicopathologic and immunohistochemical study of 17 cases. Am J Clin Pathol. 2005;124(5):749–54. doi: 10.1309/WJELN05L9A069DU0. [DOI] [PubMed] [Google Scholar]
- 33.Kulkarni PS, Parikh PM. The carcinoma of parathyroid gland. Indian J Cancer. 2004;41(2):51–9. doi: 10.4103/0019-509X.12346. [DOI] [PubMed] [Google Scholar]
- 34.Okuda I, Nakajima Y, Miura D, Maruno H, Kohno T, Hirata K. Diagnostic localization of ectopic parathyroid lesions: developmental consideration. Jpn J Radiol. 2010;28(10):707–13. doi: 10.1007/s11604-010-0492-3. [DOI] [PubMed] [Google Scholar]
- 35.Phitayakorn R, McHenry CR. Incidence and location of ectopic abnormal parathyroid glands. Am J Surg. 2006;191(3):418–23. doi: 10.1016/j.amjsurg.2005.10.049. [DOI] [PubMed] [Google Scholar]
- 36.Taterra D, Wong LM, Vikse J, Sanna B, Pękala P, Walocha J, et al. The prevalence and anatomy of parathyroid glands: a meta-analysis with implications for parathyroid surgery. Langenbecks Arch Surg. 2019;404(1):63–70. doi: 10.1007/s00423-019-01751-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ahmad S, Kuraganti G, Steenkamp D. Hypercalcemic crisis: a clinical review. Am J Med. 2015;128(3):239–45. doi: 10.1016/j.amjmed.2014.09.030. [DOI] [PubMed] [Google Scholar]
- 38.Duan K, Mete Ö. Parathyroid carcinoma: diagnosis and clinical implications. Turk Patoloji Derg. 2015;31(Suppl 1):80–97. doi: 10.5146/tjpath.2015.01316. [DOI] [PubMed] [Google Scholar]
- 39.Bearelly S, Prendes BL, Wang SJ, Glastonbury C, Orloff LA. Transoral robotic-assisted surgical excision of a retropharyngeal parathyroid adenoma: a case report. Head Neck. 2015;37(11):E150–2. doi: 10.1002/hed.24010. [DOI] [PubMed] [Google Scholar]
- 40.Argirò R, Diacinti D, Sacconi B, Iannarelli A, Diacinti D, Cipriani C, et al. Diagnostic accuracy of 3T magnetic resonance imaging in the preoperative localisation of parathyroid adenomas: comparison with ultrasound and 99mTc-sestamibi scans. Eur Radiol. 2018;28(11):4900–8. doi: 10.1007/s00330-018-5437-8. [DOI] [PubMed] [Google Scholar]
- 41.Koljević Marković A, Janković MM, Marković I, Pupić G, Džodić R, Delaloye AB. Parathyroid dual tracer subtraction scintigraphy: small regions method for quantitative assessment of parathyroid adenoma uptake. Ann Nucl Med. 2014;28(8):736–45. doi: 10.1007/s12149-014-0867-0. [DOI] [PubMed] [Google Scholar]
- 42.Iihara M, Suzuki R, Kawamata A, Horiuchi K, Okamoto T. Thoracoscopic removal of mediastinal parathyroid lesions: selection of surgical approach and pitfalls of preoperative and intraoperative localization. World J Surg. 2012;36(6):1327–34. doi: 10.1007/s00268-011-1404-0. [DOI] [PubMed] [Google Scholar]
- 43.Hu J, Ngiam KY, Parameswaran R. Mediastinal parathyroid adenomas and their surgical implications. Ann R Coll Surg Engl. 2015;97(4):259–61. doi: 10.1308/003588415X14181254789088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Elhelf I, Kademian JC, Moritani T, Capizzano AE, Policeni B, Maley J. Ectopic mediastinal parathyroid adenoma localized with four-dimensional CT: a case report. Radiol Case Rep. 2017;12(2):247–50. doi: 10.1016/j.radcr.2017.01.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Betea D, Potorac I, Beckers A. Parathyroid carcinoma: Challenges in diagnosis and treatment. Ann Endocrinol (Paris) 2015;76(2):169–77. doi: 10.1016/j.ando.2015.03.003. [DOI] [PubMed] [Google Scholar]
- 46.Cetani F, Pardi E, Marcocci C. Parathyroid carcinoma. Front Horm Res. 2019;51:63–76. doi: 10.1159/000491039. [DOI] [PubMed] [Google Scholar]
- 47.Delellis RA. Challenging lesions in the differential diagnosis of endocrine tumors: parathyroid carcinoma. Endocr Pathol. 2008;19(4):221–5. doi: 10.1007/s12022-008-9050-2. [DOI] [PubMed] [Google Scholar]
- 48.Schulte KM, Talat N. Diagnosis and management of parathyroid cancer. Nat Rev Endocrinol. 2012;8(10):612–22. doi: 10.1038/nrendo.2012.102. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All the data supporting our findings are contained within the manuscript.