

Abstract
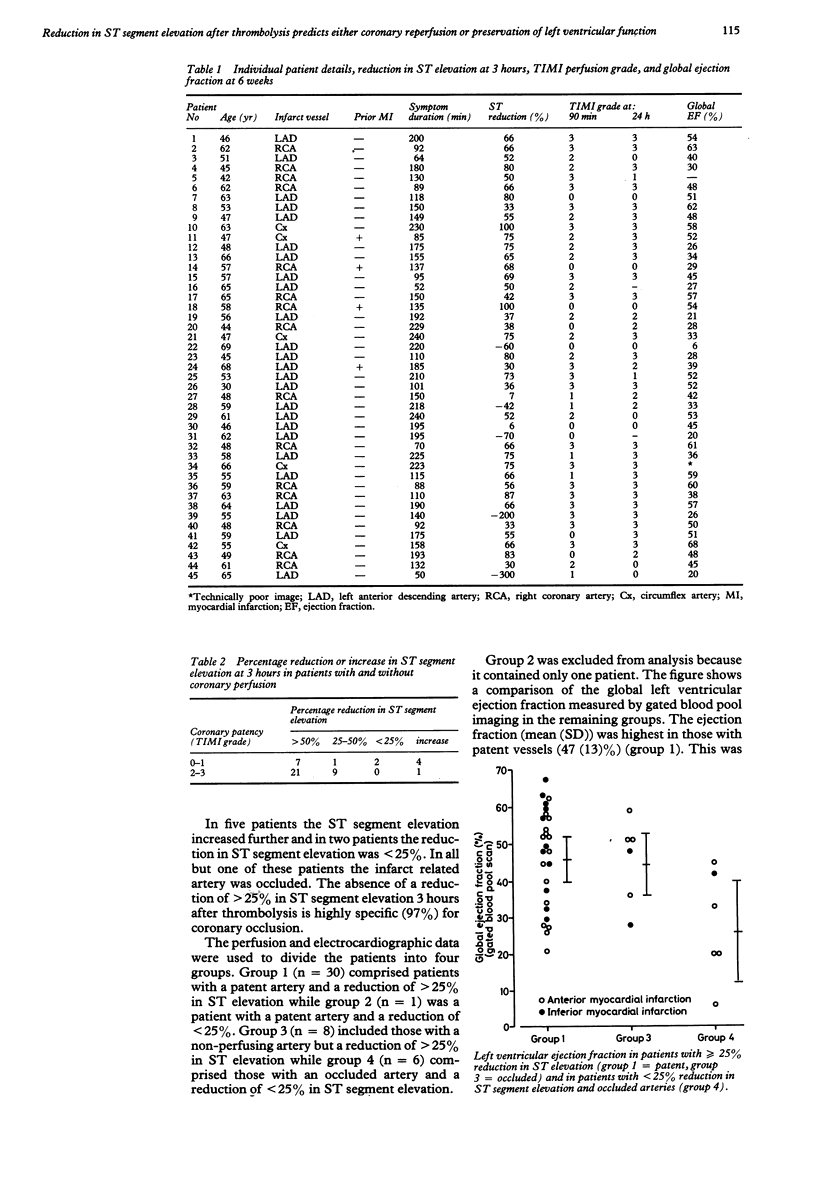
The usefulness of a reduction in ST segment elevation to predict coronary reperfusion in myocardial infarction remains uncertain. ST segment changes and angiographic findings were compared in 45 patients soon after thrombolysis. The percentage ST segment change 3 hours after treatment (in the lead showing the greatest initial ST elevation) was compared with the TIMI perfusion grade (thrombolysis in myocardial infarction trial) obtained between 90 minutes and 3 hours after treatment. Global ejection fraction and regional wall motion were assessed by cineventriculography (11 (5) days (mean (SD))) and by gated blood pool imaging (44 (11) days). Prediction of coronary patency by a reduction of greater than 25% in ST segment elevation 3 hours after thrombolytic treatment had a sensitivity of 97% but a specificity of only 43%. Where the ST segment elevation was reduced by greater than 25% the global ejection fraction was well maintained whether or not the infarct vessel was patent. In patients with a reduction of less than 25% in ST elevation, the ejection fraction was significantly lower and regional wall motion abnormality more severe. Reduction in ST elevation of greater than 25% within 3 hours of thrombolysis indicates either a patent infarct artery or preservation of left ventricular function. When the ST segment elevation does not fall by greater than 25% persistent coronary occlusion is likely (predictive accuracy 86%) and is associated with a lower ejection fraction. These patients may benefit from further treatment or additional interventions.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Been M., Muir A. L., de Bono D. P. Left ventricular function after anisoylated plasminogen streptokinase activator complex. Drugs. 1987;33 (Suppl 3):191–197. doi: 10.2165/00003495-198700333-00034. [DOI] [PubMed] [Google Scholar]
- Been M., de Bono D. P., Muir A. L., Boulton F. E., Hillis W. S., Hornung R. Coronary thrombolysis with intravenous anisoylated plasminogen-streptokinase complex BRL 26921. Br Heart J. 1985 Mar;53(3):253–259. doi: 10.1136/hrt.53.3.253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chesebro J. H., Knatterud G., Roberts R., Borer J., Cohen L. S., Dalen J., Dodge H. T., Francis C. K., Hillis D., Ludbrook P. Thrombolysis in Myocardial Infarction (TIMI) Trial, Phase I: A comparison between intravenous tissue plasminogen activator and intravenous streptokinase. Clinical findings through hospital discharge. Circulation. 1987 Jul;76(1):142–154. doi: 10.1161/01.cir.76.1.142. [DOI] [PubMed] [Google Scholar]
- Hirai T., Fujita M., Nakajima H., Asanoi H., Yamanishi K., Ohno A., Sasayama S. Importance of collateral circulation for prevention of left ventricular aneurysm formation in acute myocardial infarction. Circulation. 1989 Apr;79(4):791–796. doi: 10.1161/01.cir.79.4.791. [DOI] [PubMed] [Google Scholar]
- Hogg K. J., Hornung R. S., Howie C. A., Hockings N., Dunn F. G., Hillis W. S. Electrocardiographic prediction of coronary artery patency after thrombolytic treatment in acute myocardial infarction: use of the ST segment as a non-invasive marker. Br Heart J. 1988 Oct;60(4):275–280. doi: 10.1136/hrt.60.4.275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kennedy J. W., Martin G. V., Davis K. B., Maynard C., Stadius M., Sheehan F. H., Ritchie J. L. The Western Washington Intravenous Streptokinase in Acute Myocardial Infarction Randomized Trial. Circulation. 1988 Feb;77(2):345–352. doi: 10.1161/01.cir.77.2.345. [DOI] [PubMed] [Google Scholar]
- Krucoff M. W., Green C. E., Satler L. F., Miller F. C., Pallas R. S., Kent K. M., Del Negro A. A., Pearle D. L., Fletcher R. D., Rackley C. E. Noninvasive detection of coronary artery patency using continuous ST-segment monitoring. Am J Cardiol. 1986 Apr 15;57(11):916–922. doi: 10.1016/0002-9149(86)90730-7. [DOI] [PubMed] [Google Scholar]
- Lee G., Amsterdam E. A., Low R., Joye J. A., Kimchi A., DeMaria A. N., Mason D. T. Efficacy of percutaneous transluminal coronary recanalization utilizing streptokinase thrombolysis in patients with acute myocardial infarction. Am Heart J. 1981 Dec;102(6 Pt 2):1159–1167. doi: 10.1016/0002-8703(81)90647-5. [DOI] [PubMed] [Google Scholar]
- Richardson S. G., Morton P., Murtagh J. G., Scott M. E., O'Keeffe D. B. Relation of coronary arterial patency and left ventricular function to electrocardiographic changes after streptokinase treatment during acute myocardial infarction. Am J Cardiol. 1988 May 1;61(13):961–965. doi: 10.1016/0002-9149(88)90106-3. [DOI] [PubMed] [Google Scholar]
- Rutsch W., Schartl M., Mathey D., Kuck K., Merx W., Dörr R., Rentrop P., Blanke H. Percutaneous transluminal coronary recanalization: procedure, results, and acute complications. Am Heart J. 1981 Dec;102(6 Pt 2):1178–1181. doi: 10.1016/0002-8703(81)90649-9. [DOI] [PubMed] [Google Scholar]
- White H. D., Norris R. M., Brown M. A., Takayama M., Maslowski A., Bass N. M., Ormiston J. A., Whitlock T. Effect of intravenous streptokinase on left ventricular function and early survival after acute myocardial infarction. N Engl J Med. 1987 Oct 1;317(14):850–855. doi: 10.1056/NEJM198710013171402. [DOI] [PubMed] [Google Scholar]
- von Essen R., Schmidt W., Uebis R., Edelmann B., Effert S., Silny J., Rau G. Myocardial infarction and thrombolysis. Electrocardiographic short term and long term results using precordial mapping. Br Heart J. 1985 Jul;54(1):6–10. doi: 10.1136/hrt.54.1.6. [DOI] [PMC free article] [PubMed] [Google Scholar]