

Abstract
Despite the effectiveness of currently available antihypertensive medications, there is still a need for new treatment strategies that are more effective in certain groups of hypertensive and for additional resources to combat hypertension. However, medication non‐adherence was previously recognized as a major problem in the treatment of hypertension. The mechanisms behind the positive impacts of lifestyle changes might occur in different ways. In comparison with other studies, the efficacy and effectiveness of lifestyle modifications and antihypertensive pharmaceutical treatment for the prevention and control of hypertension and concomitant cardiovascular disease have been demonstrated in randomized controlled trials. However, in this review, the attitudinal lifestyle modifications and barriers to blood pressure control were elaborated on. An effective method for reducing blood pressure (BP) and preventing cardiovascular events with antihypertensive medications has been outlined. Maintaining healthy lifestyle factors (body mass index, diet, smoking, alcohol consumption, sodium excretion, and sedentary behavior) could lower systolic blood pressure BP by 3.5 mm Hg and reduce the risk of cardiovascular disease (CVD) by about 30%, regardless of genetic susceptibility to hypertension. Conducting a lifestyle intervention using health education could improve lifestyle factors, such as reducing salt, sodium, and fat intake, changing eating habits to include more fruits and vegetables, not smoking, consuming less alcohol, exercising regularly, maintaining healthy body weight, and minimizing stressful conditions. Each behavior could affect BP by modulating visceral fat accumulation, insulin resistance, the renin‐angiotensin‐aldosterone system, vascular endothelial function, oxidative stress, inflammation, and autonomic function. Evidence of the joint effect of antihypertensive medications and lifestyle reforms suggests a pathway to reduce hypertension.
Keywords: blood pressure, cardiovascular disorders, diets control, public health
1. INTRODUCTION
Hypertension is a leading cause of premature death worldwide and a serious public health problem. According to a 2015 survey, 1.13 billion people worldwide suffer from hypertension, one in four women and one in five men. 1 Blood pressure (BP) is a measure of the force with which the heart pumps blood through the body. BP Readings are expressed as the ratio of the systolic pressure (the first number or numerator) to diastolic pressure (the second number or denominator). According to the most current version of the American Academy of Pediatrics Pediatric Clinical Practice Guidelines (CPG), adolescents over 13 years of age are considered to have hypertension if their systolic and/or diastolic blood pressure values are ≥130/80 mmHg. 2 Generally, a high BP is said at an average measurement of more than 140/90 mmHg in individuals 18 years and above. 3 , 4 Hypertension is detected on two different measurement days when the systolic blood pressure value is ≥140 mmHg and/or the diastolic blood pressure value is ≥90 mmHg. 1 , 5 Numerous factors are responsible for the rising prevalence of hypertension in both developed and developing countries. These include the aging of the population, dietary changes, physical inactivity, rising body mass index (BMI), and problematic alcohol consumption. 6 Hypertension is the main risk factor for kidney disease, 7 , 8 stroke, 9 preterm birth, 10 heart failure, 11 and cardiovascular diseases 12 , 13 and is present in 70%–80% of patients with chronic kidney disease (CKD), contributing to the progression of end‐stage renal disease. 14 The clinical application of ambulatory blood pressure monitoring (ABPM) has made it possible to identify parameters other than the 24‐h average that could be useful for improving prognostic accuracy. ABPM measures blood pressure at regular intervals and is believed to be able to reduce the “white coat hypertension effect,” in which a patient's blood pressure is elevated during the examination due to nervousness and anxiety about the clinical environment. Loss of nocturnal BP drop is also common in CKD, 15 , 16 , 17 and attenuated BP drops at night have been associated with accelerated loss of renal function. 18 , 19 It is well known that increased BP variability (BPV) is associated with worse outcomes in hypertension, and dialysis patients are subject to severe BP variability due to intravascular volume changes in the intra‐ and interdialytic phase. 20
The most important strategies for managing this disease are population‐based screening for hypertension, patient follow‐up, and community‐based primary health care systems. 21 According to Sun et al. 22 follow‐up services (FUS) are ongoing care for people diagnosed with hypertension. It includes a review of the patient's health status in terms of symptom control through physical examination, blood pressure measurement, medication instructions and health‐related behaviors, and knowledge about disease prevention. Other research confirmed the effect of FUS on the effective management of non‐communicable diseases in China 5 , 23 and Mozambique. 24 However, Tang et al. 25 stated in a research that, the effectiveness of FUS treatment in the context of blood pressure control in hypertensive patients is proven. In their study, of the total of 2321 participants with hypertension aged 35 years or older who participated in a survey, the number of proactive FUS seekers was 3.17 times higher than passive seekers (odds ratio [OR] = 3.17, 95% confidence interval [CI] = 2.56–3.93, p < .001). It was concluded that hypertensive patients who actively sought FUS were more likely to control their blood pressure better than patients who passively sought FUS. This pathway of lifestyle modification and patient attitude towards FUS are some of the measures to ensure better blood pressure control in affected individuals. These healthy lifestyle changes include eating a healthy diet (reducing salt, sodium, and fat), changing eating habits to include more fruits and vegetables, not smoking, consuming less alcohol, exercising regularly, maintaining healthy body weight, and minimizing stressful situations. Similarly, in a research conducted by Kebede et al. 26 nearly half of the study participants had a positive attitude toward healthy lifestyle change, but only about one‐third had good follow‐up practice.
One of the main challenges to the treatment of high blood pressure is poor anti‐hypertensive adherence. 27 Additionally, it undercuts efforts to enhance public health made by the healthcare system, decision‐makers, and healthcare professionals. Patient's quality of life is impacted by noncompliance, which also wastes money and erodes public trust in healthcare systems. 28 It also exacerbates the medical and psychological complications of the disease and wastes scarce medical resources. Better control of blood pressure in hypertensive patients can be achieved not only by the services but also by the proactive attitude of the patient who visits FUS. 25 In two articles, 29 , 30 it was pointed out that being male is a risk for the development of hypertension in urban dwellers. Regarding age, Christiani et al. 31 mentioned that men aged <45 years and women aged >45 years have a higher risk of hypertension. Christiani et al. 31 and Liew et al. 30 showed that certain ethnicities were associated with hypertension based on the location of their studies. The Singapore study revealed that Malays were at higher risk for hypertension, while the Sarawak study showed that Chinese and Iban were risk factors for hypertension. The study also confirmed that low levels of education and socioeconomic were associated with hypertension in the urban population. Other contributing factors included high BMI and increased waist circumference, 31 dyslipidemia, 31 , 32 and smoking. 32
Given that countries currently undergoing rapid modernization and quick lifestyle changes have a high incidence of hypertension; these populations may show epidemiological shifts in trends and risk factors for the development of hypertension. Any therapy regimen whose main objective is blood pressure lowering should include knowledge of blood pressure variability. Modifiable and non‐modifiable risk factors are the two categories into which the risk factors for developing hypertension are categorized. Lifestyle modifications such as diet, physical activity, alcohol, and cigarette use, as well as obesity or overweight, are all included as modifiable risk factors. Contrarily, the risk factors that cannot be changed include having a family history of hypertension, being over 65, and having other concomitant conditions including diabetes and chronic renal disease. 1 Hence, the simplest and most affordable strategy for managing hypertension is to concentrate on modifiable risk factors and find a rapid cure. Therefore, this comprehensive review aims to fill the knowledge gap, focusing on the underlying mechanisms for the positive associations of lifestyle reforms, pathways of attitude‐related lifestyle changes, and barriers to blood pressure control.
2. MONITORING AND MANAGEMENT OF HYPERTENSION IN PRIMARY HEALTH CARE SYSTEMS IN DEVELOPED AND DEVELOPING COUNTRIES
Access to critical health care is more difficult to obtain in some regions and for some countries than in others due to uneven development in the economic and health systems. Although the prevalence of hypertension is higher in economically developed countries than in economically developing countries (37% and 23%, respectively, in adults), about two‐thirds of the total affected population currently lives in developing regions. 33 Overall, low‐ and middle‐income nations account for more than 80% of the disease burden associated with hypertension. 26 , 34 In high‐income countries, older age groups (60 years and older) bore most of the burden compared to low‐ and middle‐income countries, middle‐age groups (40–59 years). 35 A startling conclusion from research conducted in Brazil showed that almost one‐third of the indigenous population had high blood pressure (HBP). 36 The top five countries with the highest percentage of men with HBP are all in Central and Eastern Europe (Figure 1). 37 According to the national survey in China, which was conducted in 2010, there are an estimated 330 million persons who have hypertension. 38 , 39 In addition, the staggering direct economic expenditure on hypertension in 2002 was RMB 32 billion (US$ 51 billion), or nearly 5.6% of the country's total health expenditure in that year. 5 Urbanization and resulting lifestyle changes, such as increased consumption of salt, alcohol, and fats and decreased physical activity, have been associated with the prevalence of hypertension in developing countries. 40 , 41 , 42 , 43 Hypertension was projected to affect 13% of men and women in Ghana, 44 , 45 while the estimated national prevalence of hypertension in Ethiopia is 19.6% 26 (23.5% in urban and 14.7% in rural population) all located in Africa. According to Kebede et al. 26 HBP was virtually nonexistent in African nations throughout the first half of the 20th century. Unfortunately, the five countries with the highest proportion of women with HBP are all on the African continent, namely Niger, Chad, Mali, Burkina Faso, and Somalia. 46 However, primary health care management specifically for non‐communicable diseases (NCDs) differs among developed and developing countries. In China, the government has launched the reform of the new health care system, pledging that primary health care will include treatment for patients with chronic diseases and free follow‐up. 5 Besides, control rates are typically low in developing nations due to weak health systems. 6 An effective policy needs effective implementation and evaluation. Knowing epidemiology and natural history, which are both still poorly understood in many societies, is the first step in tackling the burden of hypertension in many developing countries, particularly in sub‐Saharan Africa. 47 To combat hypertension, salt is of utmost importance, and aside from obesity, is one of the few reversible causes of hypertension that lowers blood pressure when intake is restricted. The evidence that salt taste thresholds fall with lowering intake is still present since high‐salt foods become unpleasant to eat after 4–6 weeks of following a low‐sodium diet. 48 According to the WHO Global Burden of Disease Study, societal action to encourage a decrease in the amount of salt in processed foods could prevent more than 21 million total disabilities and adjusted life years each year globally. 49 However, to combat obesity and prevent hypertension, it is necessary to reduce calorie intake and address physical inactivity beginning at a young age. The prevalence of hypertension, abdominal obesity, hypercholesterolemia, and hypertriglyceridemia was considerably reduced by a community‐based program in Iran that was created to encourage healthy lifestyle behaviors using population and high‐risk tactics. 50 Another study conducted a treatment adherence trial in more than 500 treatment‐naive hypertensive patients in rural and urban Nigeria. 51 A simple thiazide diuretic and b‐blocker medication was provided to patients without charge, and they were monitored monthly for a period of 6 months as part of a nurse‐led treatment program with a backup clinician. At the end of the 6 months, an amazing 81% of patients were adhering to their treatment, and 66% had their hypertension under control. The positive results were attributed to good patient education, in conjunction with a simple medication regimen, and the free service given to these participants during hospital visits. As mentioned earlier, the proportion of known hypertensive individuals with controlled hypertension in developing countries continue to be low due to the low levels of awareness, control, and high cost of service provided. This may be because many developing countries governments and policymakers continue to underestimate the rising epidemic of non‐communicable diseases, especially hypertension. According to Mills et al. 52 the majority of implementation strategy trials to remove obstacles to BP control have taken place in high‐income nations (HICs). Uncertainty exists regarding whether the same tactics will be successful in Low and Middle Income Countries (LMICs). In low‐income patients in Argentina, a multifaceted intervention that included a doctor's intervention, a text‐messaging intervention, and a community health worker‐led home intervention (health coaching, home blood pressure monitoring, and BP audit and feedback) over 18 months significantly reduced systolic blood pressure by 6.6 mmHg (95% CI, 4.6–8.6; p < .001) and diastolic blood pressure by 5.4 mmHg (95% CI, 4.0–6.8 mmHg; p < .001). 53 The lack of BP knowledge in LMICs may be effectively addressed by large‐scale screening programs in communities or medical facilities. For instance, May Measurement Month (MMM) 2017 was a blood pressure screening program designed to increase awareness of hypertension throughout the world. 54 The program examined nearly 1.2 million people in 80 countries who had not had their blood pressure monitored in the previous year and discovered that 34.9% of them had hypertension, 17.3% of whom were not receiving treatment, and 46.3% of whom did not have controlled BP (systolic BP ≥140 mmH or diastolic BP ≥90 mmHg). 52 It was revealed from the study that blood pressure screening in convenience samples can be affordable and can find a lot of people who could benefit from starting or intensifying antihypertensive therapy. One must understand the initial state of the hypertension management problem in order to evaluate the reform and policy. However, the most crucial methods for preventing this disease are population‐wide screening for hypertension, patient follow‐up management with less cost for easy accessibility for all. Good follow‐up management can help evaluate some key components of the standards policy and some features of the healthcare system reform. Furthermore, based on these findings, priority strategies could be developed to reduce hypertension in specific populations. According to Zhou et al., 55 ensuring universal access to essential public health services (EPHS) is fundamental to these reforms and is in line with international efforts.
FIGURE 1.
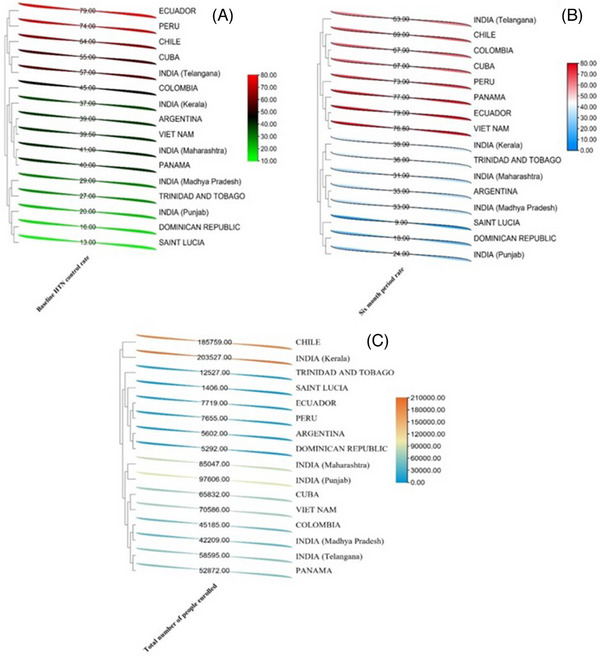
A heatmap representation that illustrate hypertension control rates from 3–6 months in some countries according to Macedo et al. 4
3. BARRIERS TO BLOOD PRESSURE CONTROL AMONG HYPERTENSIVE INDIVIDUALS
There is a noticeable gap in translating findings from clinical trials into practice for optimal control of hypertension. The three main categories of barriers to hypertension control BP are patient‐related, physician‐related, and medical environment/health system factors. Patient‐related barriers include poor medication adherence, beliefs about hypertension and its treatment, depression, health literacy, comorbidity, and patient motivation. 56 , 57 Most important is treatment adherence, as it is central to the other factors. 58 The most important physician‐related barrier is clinical inertia, which is the failure of healthcare providers to initiate or intensify drug therapy in a patient with uncontrolled hypertension and BP. The main reasons for clinical inertia are: overestimation of the level of care provided by physicians, lack of training to achieve target values BP, and physicians' use of soft reasons to avoid intensifying treatment by taking the “wait until the next visit” approach in response to patients' excuses. 58
Despite efforts to combat hypertension with medication, control rates for the condition are still poor. 59 In addition to medical treatment, appropriate lifestyle modification is a crucial and economical way to reduce hypertension. To monitor and manage hypertensive patients in the best way possible, a comprehensive intervention is needed 60 , 61 ; this is dependent on many interconnected factors relating to the patient and the healthcare provider as well as how care is provided. 62 , 63 Previous studies by Modey Amoah et al., 59 show that BP control in patients taking antihypertensive medication is related to modifiable parameters such as duration of physical activity, alcohol consumption, and diet composition.
Comorbidity has been noted as a potential barrier to the proper use of antihypertensive medications. Adherence to antihypertensive has been reported to decrease when comorbidity is present. 64 In other words, the presence of multiple diseases is considered an obstacle to good adherence and promotes poor adherence. For example, adherence was reported to be 80% in 72.3% of individuals with hypertension (HTN) alone, which was better compared with hypothyroidism comorbidity (68.4%) or gout comorbidity (36.8%), 65 as measured by the ratio of medication possession to a daily supply of the dispensed medication at 1‐year follow‐up. Comorbidities are generally considered barriers to patients with hypertension and are taken into account when assessing patient adherence. 64 In addition to physical illness, psychiatric conditions such as depressive symptoms have also been reported to interfere with adherence to antihypertensive medication and lead to poor BP control. 66
Adherence to antihypertensive medication is a key component in the control of blood pressure levels. 64 Adherence is a multifactorial phenomenon that can be influenced by several factors. These factors can be divided into five different dimensions: social and economic factors, treatment‐related factors, disease‐related factors, patient‐related factors, and healthcare system factors. Poor adherence to antihypertensive medications leads to the development of hypertensive complications and increases the risk of cardiovascular events, which in turn affects clinical outcomes. 65 Demographic factors such as age, ethnicity, gender, education, and marital status affect adherence to antihypertensive medication and are sometimes barriers to blood pressure control BP. 67
4. THE ROLE OF LIFESTYLE ATTITUDES IN BLOOD PRESSURE CONTROL IN HYPERTENSIVE PATIENTS
Lifestyle changes, formerly referred to as non‐pharmacologic therapy, play a critical role in both hypertensive and non‐hypertensive patients. Lifestyle changes can be used in hypertensive patients as an initial treatment before starting pharmacologic therapy and as an adjunct to drug treatment in those already receiving it. These treatments can support medication withdrawal and reduction in hypertensive patients with medication‐controlled blood pressure if highly motivated patients successfully implement and maintain lifestyle changes. Lifestyle changes in nonhypertensive patients may prevent hypertension and, more broadly, lower BP, which in turn minimizes the risk of BP‐related clinical outcomes in entire populations. Indeed, even a seemingly tiny reduction in blood pressure could have a significant beneficial effect on cardiovascular events if extended to the entire population. The key to assisting hypertension individuals in acquiring good lifestyle behaviors is lifestyle adjustment. 68 Effective treatment and control techniques require a detailed understanding of the consequences of smoking, drinking alcohol, and consuming unlimited salt.
4.1. Lowering the intake of salt (sodium chloride)
Lowering the intake of salt is a peculiar lifestyle change to the reduction of cardiovascular diseases. Numerous public health and scientific organizations have urged significant dietary salt reduction due to systematic reviews indicating the harmful health impacts of excessive salt consumption, particularly increased BP. Results from clinical trials, epidemiological studies, food and animal studies all serve as evidence. Recent research has shown that consuming less sodium (Na) can prevent hypertension (TOHP2, phase 2 of the Trials of Hypertension Prevention), 69 can facilitate hypertension control in older‐aged persons on medication (TONE, Trials of Non‐Pharmacologic Interventions in the Elderly) 70 and can help those who are overweight to potentially prevent cardiovascular problems. 71 , 72 According to Appel, 73 TOPH2 documented that sodium reduction, or combined with weight loss has a 20% reduction in the prevalence of hypertension. However, in the TONE, lowering salt intake effectively decreased blood pressure and the need for antihypertensive medication in elderly people, whether or not they lose weight. It was reported that in both studies, total sodium intake was reduced to about 100 mmol/d by the dietary measures. The latter corresponds to the current recommendations to keep salt consumption to 6 g/d, or 100 mmol of sodium (2400 mg) each day. 74 The Dietary Approaches to Stop Hypertension (DASH)‐Sodium feeding trial, found that a reduced sodium consumption, around 60 mmol/d, further lowers blood pressure in a large population of both hypertensive and nonhypertensive people. 75 The DASH sodium study examined how three stages of sodium reduction in two different diets affected BP. The three sodium levels were “higher” (target of approximately 143 mmol/d, reflecting the average intake in the United States), “medium” (target of 106 mmol/d, reflecting the maximum of recent U.S. guidelines), and “lower” (target of 65 mmol/d, representing a level that could lead to further blood pressure reduction). In a typical U.S. diet, lowering sodium intake from the higher to the middle level resulted in a 2.1 mmHg reduction in systolic blood pressure, and lowering sodium intake from the middle to the lower level resulted in a 4.6 mmHg reduction. On the DASH diet, the corresponding changes in systolic blood pressure were BP ‐1.3 and ‐1.7 mmHg, respectively (Figure 2). 73 Compared with the control diet with higher sodium content, the sodium‐reduced DASH diet lowered systolic blood pressure BP by 7.1 mmHg in nonhypertensive subjects and by 11.5 mmHg in hypertensive. Results for diastolic BP were similar. The results of the DASH‐sodium study support current population‐based recommendations to reduce salt intake. Currently, condiments are the primary sources of salt, but processed foods are anticipated to contribute significantly more in the future. Added salt continues to be the leading source of sodium intake, followed by sodium from processed foods. Similar circumstances exist in South Korea, where dietary salt is primarily obtained from added condiments. 76 According to Du et al. 77 the prevalence of hypertension in Chinese adults, particularly untreated hypertension is high due to salt intake. Sodium intake showed a strong dose‐response relationship with the occurrence of hypertension for the third to fifth quintiles when sodium and potassium intake were measured. It was also found that the highest sodium intake is in central China, which is due to the use of large amounts of salt and soy sauce in the preparation of dishes, especially Huaiyang and Lu cuisine. However, the North has seen a faster decline in added salt consumption than the South. The Chinese government, under the leadership of the Chinese Nutrition Society and the National Institute of Nutrition and Food Safety, has initiated nationwide salt reduction campaigns and studies that include more localized measures. 77 To reduce salt consumption, consumers should select low‐salt foods, limit the amount of salt added to foods, and/or use salt substitutes such as potassium (K). According to Zhou et al. 78 blood pressure can be raised by sodium, while potassium can minimize blood pressure. A report on rural families in China with prevalence of hypertension received normal and salt substitute treatment. 78 As salt intake, 100% sodium chloride was given to the group with the usual salt, and salt substitution consisted of 65% sodium chloride, 25% potassium chloride, and 10% magnesium sulfate. The results showed that the participants who received salt substitution had lower systolic and diastolic blood pressure than the participants in the normal salt group. It was postulated that salt substitution may be a valuable tool for both hypertensive and prehypertensive individuals. Because routine salt substitution by industries, households, or individuals is simple, feasible, and without complications. Figure 3 depicts the classification of hypertension and proposed K+ and Na+ intake that can reduce blood pressure as adapted from Ojangba et al. 79 Despite their best efforts, many still find it challenging to cut down on their salt intake due to the excessive amounts of salt that food manufacturers add to foods during processing. High sodium intake, low potassium intake, and high Na/K ratio all have significant effects on the occurrence of hypertension (Figure 3). Therefore, any effective plan to reduce salt consumption must include efforts by food manufacturers, who should reduce the amount of salt added during preparation, and strict government regulations to ensure compliance.
FIGURE 2.
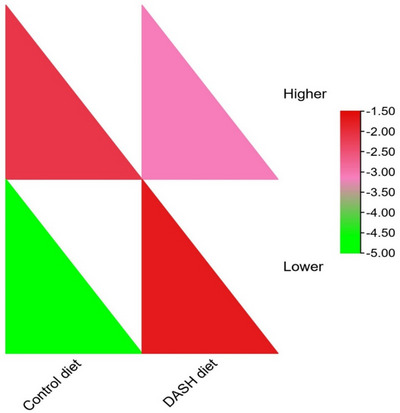
Heatmap of reduced sodium intake using the Dietary Approaches to Stop Hypertension (DASH) diet versus a regular American diet with values adapted from Appel. 73
FIGURE 3.
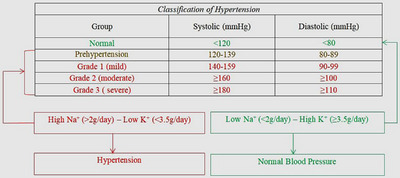
The classification of hypertension and proposed K+ and Na+ intake that can reduce blood pressure.
4.2. Increasing physical activity
Increased levels of physical activity may lower BP, independent of concurrent weight changes (Figure 4). However, not all hypertensive patients are suitable for moderate‐to‐vigorous intensity physical activity. Optimal physical activity from a health promotion and disease prevention perspective may include both substantial periods of low‐intensity physical activity to reduce sedentary time and moderate vigorous physical activity to improve aerobic capacity. 80 Evidence indicates that recurrent, relatively brief bouts of low‐intensity physical activity, for example, 6 min/h, can have substantial health benefits, including blood pressure reduction. In addition, the active living index, work index, and home/life index can be of significant benefit in reducing incident hypertension. 81 In a recent study, compared with 7 h of sitting, 3 min of low‐intensity physical activity every 30 min, that is, 6 min/h or 10% of the time, for example, walking at a pace of ≈2 miles per hour, significantly lowered systolic and diastolic blood pressure, as well as plasma noradrenaline. 81 On the other hand, the components of physical activity, exercise, and physical fitness are commonly recommended as important lifestyle modifications that may aid in the prevention of hypertension. Hypertensive and non‐hypertensive patients who met recommended levels of moderate–vigorous physical activity by self‐report are mostly younger, healthier, and more likely to be men. Thus, effective approaches to improving moderate vigorous physical activity among patients, especially women and middle‐aged and older individuals, are important in realizing more of the health benefits of moderate vigorous physical activity, including a reduction in incident hypertension. Aerobic exercise (a form of exercise that involves the use of large muscle groups to perform repetitive activities that result in increases in heart rate and energy expenditure [e.g. walking; cycling]), resistance training (a form of exercise designed to improve muscular strength and/or endurance wherein physical effort is performed against an opposing force that elicits resistance to induce muscular contraction, typically at a high intensity of effort for a short duration of time [e.g. weight lifting]), cardiorespiratory fitness (the ability of the circulatory and respiratory systems to supply oxygen during sustained physical activity), muscular strength (the amount of external force that a skeletal muscle can exert), and muscular endurance (the ability of muscle groups to exert external force for many repetitions or successive exertions) are effective approaches of moderate vigorous physical activity to reduce hypertension. 82 , 83
FIGURE 4.
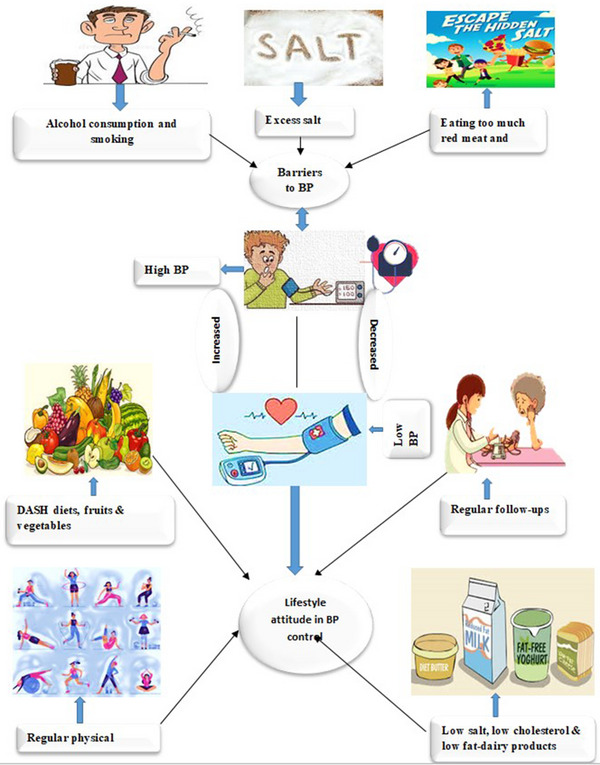
A models of lifestyle attitudes in hypertension control.
Blood pressure control among diagnosed individuals was found to be aided by weekly exercise, which included activity lasting up to an hour or longer. 59 Individuals assigned to an aerobic exercise intervention showed a 4 mmHg net drop in systolic blood pressure, according to a meta‐analysis of 27 randomized trials. 84 Interestingly, the extent of BP fluctuations was not related to the amount of physical activity. Increased physical activity should lower blood pressure and also have a direct beneficial effect on blood pressure by supporting early weight loss and promoting maintenance of weight loss once achieved. 73 Furthermore, results from other studies indicated that exercising frequently is a powerful indicator of hypertension control. 26 , 85 , 86 The WHO has recommended that persons up to the age of 64 should engage in 75 min of intense aerobic activity per week, or a total of 150 min of moderate aerobic activity, for better health outcomes. 87 Moreover, work‐related physical activity, often low‐intensity and moderate vigorous physical activity, has fallen >100 calories/day from the 1960s to the early 2000s and may account for the majority of weight gain in the US population over the past 5 decades. 88
4.3. Limiting alcohol consumption and avoidance of smoking
Excessive alcohol consumption and smoking are associated with increased BP (Figure 4). Smoking causes an acute increase in blood pressure (BP) and heart rate and has been associated with malignant hypertension. Nicotine acts as an adrenergic agonist and mediates the local and systemic release of catecholamines and possibly the release of vasopressin. The addictive effects of smoking are only partially known, but the hemodynamic effects of tobacco smoking may likely contribute to habituation. 89 It has long been known that blood pressure and heart rate increase with smoking. These effects are specifically associated with nicotine, while the other constituents, of whom more than a thousand have been isolated, appear to be of lesser importance. 89 The increase in blood pressure is due to both an increase in cardiac output and total peripheral vascular resistance. The increase in blood pressure occurs immediately and before any increase in circulating catecholamines. 90 In hypertensive patients, the antihypertensive effect of beta‐blockers may be partially reversed by smoking, whereas alpha‐receptor blockers appear to maintain the antihypertensive effect in smokers. It is paradoxical that although smoking acutely increases blood pressure, larger epidemiological studies have found a somewhat lower blood pressure level in smokers than in nonsmokers.
In a prospective cross‐sectional study by Kebede et al. 26 nearly 84% of 100 men with hypertension were aware of how smoking affects hypertension. This corresponds to Primatesta et al. 91 who reported that more men than women were heavy smokers. This is due to the connection between smoking and chronically enhanced atherogenesis in large capacitance vessels, which results in isolated systolic hypertension. 92 , 93 Men of normal weight did not show any correlation between smoking and SBP, whereas men who were overweight or obese exhibited a substantial rise in SBP among both heavy and moderate smokers, women, did not exhibit these variations. 91
Current studies have shown that e‐cigarettes also have a blood pressure‐raising effect. 94 In one report, people who used e‐cigarettes and people who smoked combustible cigarettes had greater increases in blood pressure, heart rate, and blood vessel constriction, immediately after vaping or smoking, compared to people who did not use any nicotine. E‐cigarettes are electronic devices that heat a liquid and produce an aerosol, or mix of small particles in the air. Using an e‐cigarette is sometimes called “vaping.” 94 The liquid used in e‐cigarettes often contains nicotine and flavorings. Users inhale e‐cigarette aerosol into their lungs. Flavorings such as diacetyl, a chemical linked to serious lung disease. 95 JUUL is a brand of e‐cigarette that is shaped like a USB flash drive. Like other e‐cigarettes, JUUL is a battery‐powered device that heats a nicotine‐containing liquid to produce an aerosol that is inhaled. 96 All JUUL e‐cigarettes have a high level of nicotine. According to the manufacturer, a single JUUL pod contains as much nicotine as a pack of 20 regular cigarettes. 97 Through authority granted by the Family Smoking Prevention and Tobacco Control Act (FSPTCA), FDA has authority to develop regulations that address the manufacturing, marketing, and sale of e‐cigarettes. It is recommended to set a good example by being tobacco‐free and ensure that kids are not exposed to secondhand emissions from any tobacco products, including e‐cigarettes which can cause hypertension. Setting up an appointment with kids' health care providers so that they can hear from a medical professional about the health risks of tobacco products, including e‐cigarettes to decrease early‐stage hypertension caused by vaping. Moreover, teachers and school administrator enforcement of tobacco‐free school grounds policies and tobacco prevention curricula could help to reduce vaping as a result of e‐cigarettes and reduce hypertension among students. 95 The changes in BP related to smoking that were observed by Primatesta et al. 91 varied with age and across men and women and were as well partially explained by variations in the confounding effects of BMI and alcohol consumption. However, people with elevated BP must be encouraged to avoid smoking because smoking and high blood pressure have been proven to have a synergistic negative impact on the risk of coronary heart disease. 98 , 99
Alcoholic beverages are very popular. Light‐to‐moderate alcohol consumption is typically safe, but excessive alcohol consumption can increase the risk of several metabolic conditions, including high blood pressure. 100 Consuming alcohol affects the renin‐angiotensin‐aldosterone system (RAAS). The RAAS is controlled by the kidneys, and its function is to regulate blood pressure through three hormones: renin, angiotensin, and aldosterone. Alcohol increases blood levels of the hormone renin, which causes the blood vessels to constrict. 100 This means that they get smaller in diameter. Renin also decreases how much fluid the body eliminates as urine. Recent data suggest that moderate and heavy drinking contributes to high blood pressure in men and women. To prevent various health complications, including high blood pressure, limiting alcohol consumption is recommended. Reducing alcohol consumption has also been shown in studies to lower blood pressure in normotensive and hypertensive men who are heavy drinkers. However, in the prevention and treatment of hypertension study, moderate‐to‐heavy drinkers' blood pressure decreased by a modest, insignificant amount, when alcohol consumption was reduced. 101 Consumption of alcohol is closely related to smoking 102 and appears to have an impact on the smoking‐BP association. Overall, there is support for keeping alcohol consumption for men to no more than two drinks per day and for women to no more than one drink per day.
4.4. Diet pattern
Low BP has been linked to specific food patterns. For instance, vegetarian diets have been associated with lower blood pressure in observational studies and two clinical trials. The macronutrients (particularly the type and amount of fat), micronutrients (potassium, magnesium, and calcium), and fiber have received the majority of attention. 73 The DASH diet, which is the most beneficial diet, emphasizes fruits, vegetables, low‐fat dairy products, whole grains, poultry, fish, and nuts while limiting red meat, fat, sweets, and beverages with added sugar (Figure 4). Calcium, magnesium, and potassium are abundant in these diets. These diets lowered systolic and diastolic blood pressure by 3.5 and 2.1 mmHg, respectively, in nonhypertensive people. 73 Therefore, it is recommended to limit sodium intake to a maximum of 2300 mg per day. 103 Reduce total fat to 27% of daily calories and saturated fat to no more than 6%. 104 Systolic blood pressure appears to be particularly favorably affected by low‐fat dairy products. Consumption of fresh fruits and vegetables in moderate amounts is recommended because the effects of excessive fructose intake on serum glucose and uric acid levels are not beneficial to health. 105 Limiting protein intake to no more than 18% of daily calories is beneficial to the body. 106 The best sources of protein include fish, skinless poultry, and soy products. The DASH diet also sets a daily cholesterol goal of 150 mg and a carbohydrate goal of no more than 55% of daily calories. 106 A daily intake of 30 grams (g) of fiber could also be beneficial. 107 The results of the study by Modey Amoah et al. 59 show that when evaluating the components of a person's diet, patients with poor blood pressure control reported diets that were primarily made up of meat, fat, and starch because these food items have been recognized as being unhelpful for lowering blood pressure. 6 , 85 Other factors might also influence BP control. A diet rich in monounsaturated fatty acids has been shown to lower blood pressure by 8 and 6 mmHg, respectively, in earlier research. 108 Also, two meta‐analyses indicated that high dosages of omega‐3 PUFA, typically 3 g or more of fish oil per day, reduce blood pressure. 109 In addition, strong evidence from epidemiological research suggests that consuming more protein can reduce BP. 110 , 111 Finally, a variety of dietary components affect blood pressure. Even while each element usually has a small impact, the overall impact might be significant. From the standpoint of public health, even a slight decrease in blood pressure should have a significant, positive impact on the occurrence of hypertension and its repercussions. In light of the epidemic of BP‐related diseases and the scientifically demonstrated effects of lifestyle modifications on BP, the current challenge for healthcare professionals, researchers, public officials, and patients is to develop and implement effective clinical and public health strategies that achieve and maintain healthy lifestyle modification. The various parameters that aid in the management of HTN are shown in Figure 4.
5. CONCLUSION
The occurrence and burden of hypertension have reached unprecedented levels in low‐ and middle‐income countries, while the problem has either stabilized or declined in high‐income countries. Our findings indicated that interventions that encourage lifestyle change and non‐pharmacological therapy compliance are essential for managing and preventing hypertension and its related consequences. The interventions complement one another, with double benefits by improving blood pressure control which is positively related to making hypertensive patients proactive in seeking follow‐up care, limiting excess salt intake, making use of fruits and vegetables, regular exercise, moderate alcohol consumption, avoiding smoking, and managing stress as lifestyle reform practices to control high BP. By following these routes, people can adopt healthy lifestyle behaviors that improve their fitness, health, and productivity while using fewer antihypertensive drugs.
AUTHOR CONTRIBUTIONS
Dr. Dong Wenyong proposed the structure and conceptulized lifestyles of the review. Ojangba Theodora and Boamah Solomon conceived and wrote the manuscript, Miao Yudong revised and supervised the write‐up, Agboyibor Clement, Guo Xinghong, Feng Yifei and Jingjing Yuan edited the write‐up. All authors have read and agreed to the published version of the manuscript.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest
PATIENT CONSENT STATEMENT
There is no human subject in this article and consent statement is not applicable
ACKNOWLEDGMENTS
The authors would like to thank the entire team that participated in the success of the study. The study was funded by National Social Science Fund of China, Study on Transaction Cost measurement and Solutions of Integrated Delivery System (21BGL222), Henan Provincial Joint Project for Medical Science and Technology Innovation, Self‐management intervention mode of elderly hypertensive patients in rural areas based on “Internet +”, Grant number, LHGJ20220017 and Henan Provincial Philosophy and Social Science Innovation Talent Support Plan.
Ojangba T, Boamah S, Miao Y, et al. Comprehensive effects of lifestyle reform, adherence, and related factors on hypertension control: A review. J Clin Hypertens. 2023;25:509–520. 10.1111/jch.14653
DATA AVAILABILITY STATEMENT
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, to any qualified researcher.
REFERENCES
- 1. Mohammed Nawi A, Mohammad Z, Jetly K, et al. The prevalence and risk factors of hypertension among the urban population in southeast Asian countries: a systematic review and meta‐analysis. Int J Hypertens. 2021;2021:1‐14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Flynn JT, Kaelber DC, Baker‐Smith CM, et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics. 2017; 140(3):e20171904. [DOI] [PubMed] [Google Scholar]
- 3. Asemu MM, Yalew AW, Kabeta ND, Mekonnen D. Prevalence and risk factors of hypertension among adults: a community based study in Addis Ababa, Ethiopia. PLoS One. 2021;16(4):e0248934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Macedo ME, Lima MJ, Silva AO, Alcantara P, et al. Prevalence, awareness, treatment and control of hypertension in Portugal: the PAP study. J Hypertens. 2005;23(9):1661‐1666 [DOI] [PubMed] [Google Scholar]
- 5. Feng YJ, Wang HC, Li YC, Zhao WH. Hypertension screening and follow‐up management by primary health care system among Chinese population aged 35 years and above. Biomed Environ Sci. 2015;28(5):330‐340. [DOI] [PubMed] [Google Scholar]
- 6. Petersen L, Schnohr P, Sørensen T. Longitudinal study of the long‐term relation between physical activity and obesity in adults. Int J Obes. 2004;28(1):105‐112. [DOI] [PubMed] [Google Scholar]
- 7. Rossignol P, Massy ZA, Azizi M, et al. The double challenge of resistant hypertension and chronic kidney disease. Lancet. 2015;386(10003):1588‐1598. [DOI] [PubMed] [Google Scholar]
- 8. Lu C, Zhao H, Xu G, et al. Prevalence and risk factors associated with chronic kidney disease in a Uygur adult population from Urumqi. J Huazhong Univ Sci Technol. 2010;30(5):604‐610. [DOI] [PubMed] [Google Scholar]
- 9. Collaboration BPLTT . Effects of blood pressure lowering on cardiovascular risk according to baseline body‐mass index: a meta‐analysis of randomised trials. Lancet. 2015;385(9971):867‐874. [DOI] [PubMed] [Google Scholar]
- 10. Yang Y, He Y, Li Q, et al. Preconception blood pressure and risk of preterm birth: a large historical cohort study in a Chinese rural population. Fertil Steril. 2015;104(1):124‐130. [DOI] [PubMed] [Google Scholar]
- 11. Roy SS, Foraker RE, Girton RA, Mansfield AJ. Posttraumatic stress disorder and incident heart failure among a community‐based sample of US veterans. Am J Public Health. 2015;105(4):757‐763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Schnohr P, Jensen J, Scharling H, Nordestgaard B. Coronary heart disease risk factors ranked by importance for the individual and community. A 21 year follow‐up of 12000 men and women from The Copenhagen City Heart Study. Eur Heart J. 2002;23(8):620‐626. [DOI] [PubMed] [Google Scholar]
- 13. Brownstein JN, Bone LR, Dennison CR, Hill MN, Kim MT, Levine DM. Community health workers as interventionists in the prevention and control of heart disease and stroke. Am J Prev Med. 2005;29(5):128‐133. [DOI] [PubMed] [Google Scholar]
- 14. Manios E, Tsagalis G, Tsivgoulis G, et al. Time rate of blood pressure variation is associated with impaired renal function in hypertensive patients. Am J Hypertens. 2009;27(11):2244‐2248. [DOI] [PubMed] [Google Scholar]
- 15. Farmer C, Goldsmith D, Cox J, Dallyn P, Kingswood J, Sharpstone P. An investigation of the effect of advancing uraemia, renal replacement therapy and renal transplantation on blood pressure diurnal variability. Nephrol Dial Transplant.1997;12(11):2301‐2307. [DOI] [PubMed] [Google Scholar]
- 16. Li Kam Wa T, Macnicol A, Watson M. Ambulatory blood pressure in hypertensive patients with autosomal dominant polycystic kidney disease. Nephrol Dial Transplant. 1997;12(10):2075‐2080. [DOI] [PubMed] [Google Scholar]
- 17. Jensen L, Pedersen E. Nocturnal blood pressure and relation to vasoactive hormones and renal function in hypertension and chronic renal failure. Blood Press. 1997;6(6):332‐342. [DOI] [PubMed] [Google Scholar]
- 18. Agarwal R, Andersen M. Prognostic importance of ambulatory blood pressure recordings in patients with chronic kidney disease. Kidney Int. 2006;69(7):1175‐1180. [DOI] [PubMed] [Google Scholar]
- 19. Davidson MB, Hix JK, Vidt DG, Brotman DJ. Association of impaired diurnal blood pressure variation with a subsequent decline in glomerular filtration rate. Arch Intern Med. 2006;166(8):846‐852. [DOI] [PubMed] [Google Scholar]
- 20. Thompson A, Pickering T. The role of ambulatory blood pressure monitoring in chronic and end‐stage renal disease. Kidney Int. 2006;70(6):1000‐1007. [DOI] [PubMed] [Google Scholar]
- 21. Saha S, Hoerger TJ, Pignone MP, et al. The art and science of incorporating cost effectiveness into evidence‐based recommendations for clinical preventive services. Am J Prev Med. 2001;20(3):36‐43. [DOI] [PubMed] [Google Scholar]
- 22. Sun X, Feng Z, Zhang P, Shen X, Wei L, Tian M. Association between time of pay‐for‐performance for patients and community health services use by chronic patients. PLoS One. 2014;9(2):e89793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Niu H, Tian M, Ma A, Wang C, Zhang L. Differences and determinants in access to essential public health services in China: a case study with hypertension people and under‐sixes as target population. Chin Med J. 2014;127(09):1626‐1632. [PubMed] [Google Scholar]
- 24. Silva‐Matos C, Beran D. Non‐communicable diseases in Mozambique: risk factors, burden, response and outcomes to date. Glob. Health. 2012;8(1):1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Tang S, Bishwajit G, Ji L, et al. Improving the blood pressure control with the proactive attitude of hypertensive patients seeking follow‐up services: evidence from China. Med. 2016;95(14):e3233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Kebede T, Taddese Z, Girma A. Knowledge, attitude and practices of lifestyle modification and associated factors among hypertensive patients on‐treatment follow up at Yekatit 12 General Hospital in the largest city of East Africa: a prospective cross‐sectional study. PLoS One. 2022;17(1):e0262780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Ong KL, Cheung BM, Man YB, Lau CP, Lam KS. Prevalence, awareness, treatment, and control of hypertension among United States adults 1999–2004. Hypertension. 2007;49(1):69‐75. [DOI] [PubMed] [Google Scholar]
- 28. Balkrishnan R. The importance of medication adherence in improving chronic‐disease related outcomes: what we know and what we need to further know. Med Care. 2005; 43(6):517‐520. [DOI] [PubMed] [Google Scholar]
- 29. Bjertness MB, Htet AS, Meyer HE, et al. Prevalence and determinants of hypertension in Myanmar‐a nationwide cross‐sectional study. BMC Public Health. 2016;16:590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Liew SJ, Lee JT, Tan CS, Koh CHG, Van Dam R, Müller‐Riemenschneider F. Sociodemographic factors in relation to hypertension prevalence, awareness, treatment and control in a multi‐ethnic Asian population: a cross‐sectional study. BMJ Open. 2019;9(5):e025869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Christiani Y, Byles JE, Tavener M, Dugdale P. Gender inequalities in noncommunicable disease risk factors among Indonesian urban population. Asia Pac J Public Health. 2016;28(2):134‐145. [DOI] [PubMed] [Google Scholar]
- 32. Sison O, Castillo‐Carandang N, Ladia MA, et al. Prevalence of metabolic syndrome and cardiovascular risk factors among community health workers in selected villages in the Philippines. J ASEAN Fed Endocr Soc. 2019;34(2):171‐179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Kearney PM, Whelton M, Reynolds K, et al. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365(9455):217‐223. [DOI] [PubMed] [Google Scholar]
- 34. Lawes CM, Vander Hoorn S, Rodgers A. Global burden of blood‐pressure‐related disease, 2001. Lancet. 2008;371(9623):1513‐1518. [DOI] [PubMed] [Google Scholar]
- 35. Mills KT, Bundy JD, Kelly TN, et al. Global disparities of hypertension prevalence and control: a systematic analysis of population‐based studies from 90 countries. Circulation. 2016;134(6):441‐450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Altonen BL, Arreglado TM, Leroux O, Murray‐Ramcharan M, Engdahl R. Characteristics, comorbidities and survival analysis of young adults hospitalized with COVID‐19 in New York City. PLoS One. 2020;15(12):e0243343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Zhou B, Bentham J, Di Cesare M, et al. Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population‐based measurement studies with 19· 1 million participants. Lancet. 2017;389(10064):37‐55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Wang Y‐J, Li Z‐X, Gu H‐Q, et al. China stroke statistics 2019: a report from the National center for healthcare quality management in neurological diseases, China national clinical research center for neurological diseases, the Chinese stroke association, National center for chronic and non‐communicable disease control and prevention, Chinese center for disease control and prevention and Institute for global neuroscience and stroke collaborations. Stroke Vasc Neurol. 2020;5(3):211‐239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Li Y, Wang L, Jiang Y, Li X, Zhang M, Hu N. Prevalence of hypertension among Chinese adults in 2010. Chin J Prev Vet Med. 2012;46(5):409‐413. [PubMed] [Google Scholar]
- 40. Mittal BV, Singh AK. Hypertension in the developing world: challenges and opportunities. Am J Kidney Dis. 2010;55(3):590‐598. [DOI] [PubMed] [Google Scholar]
- 41. Ibrahim MM, Damasceno A. Hypertension in developing countries. Lancet. 2012;380(9841):611‐619. [DOI] [PubMed] [Google Scholar]
- 42. Hendriks ME, Wit FW, Roos MT, et al. Hypertension in sub‐Saharan Africa: cross‐sectional surveys in four rural and urban communities. PLoS One. 2012;7(3):e32638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Agyei‐Mensah S, de‐Graft Aikins A. Epidemiological transition and the double burden of disease in Accra, Ghana. J Urban Health. 2010;87(5):879‐897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Bosu WK, Bosu DK. Prevalence, awareness and control of hypertension in Ghana: a systematic review and meta‐analysis. PLoS One. 2021;16(3):e0248137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Sanuade OA, Boatemaa S, Kushitor MK. Hypertension prevalence, awareness, treatment and control in Ghanaian population: evidence from the Ghana demographic and health survey. PLoS One. 2018;13(11):e0205985. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Van de Vijver S, Akinyi H, Oti S, et al. Status report on hypertension in Africa‐consultative review for the 6th session of the African Union conference of ministers of health on NCD's. Pan Afr Med J. 2014;16(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Tibazarwa KB, Damasceno AA. Hypertension in developing countries. Can J Cardiol. 2014;30(5):527‐533. [DOI] [PubMed] [Google Scholar]
- 48. Ma Y, He FJ, MacGregor GA. High salt intake: independent risk factor for obesity? Hypertension. 2015;66(4):843‐849 [DOI] [PubMed] [Google Scholar]
- 49. Murray CJ, Lauer JA, Hutubessy RC, et al. Effectiveness and costs of interventions to lower systolic blood pressure and cholesterol: a global and regional analysis on reduction of cardiovascular‐disease risk. Lancet. 2003;361(9359):717‐725. [DOI] [PubMed] [Google Scholar]
- 50. Sarrafzadegan N, Kelishadi R, Sadri G, et al. Outcomes of a comprehensive healthy lifestyle program on cardiometabolic risk factors in a developing country: the Isfahan Healthy Heart Program. Arch Iran Med. 2013;16(1):4. [PubMed] [Google Scholar]
- 51. Adeyemo A, Tayo BO, Luke A, Ogedegbe O, Durazo‐Arvizu R, Cooper RS. The Nigerian antihypertensive adherence trial: a community‐based randomized trial. J Hypertens. 2013;31(1):201‐207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16(4):223‐237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. He J, Irazola V, Mills KT, et al. Effect of a community health worker–led multicomponent intervention on blood pressure control in low‐income patients in Argentina: a randomized clinical trial. Jama. 2017;318(11):1016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Beaney T, Schutte AE, Tomaszewski M, et al. May Measurement Month 2017: an analysis of blood pressure screening results worldwide. Lancet Glob Health. 2018;6(7):e736‐e743. [DOI] [PubMed] [Google Scholar]
- 55. Zhou D, Feng Z, He S, et al. Equity of the essential public health service in rural china: evidence from a nationwide survey of hypertensive patients. Pak J Med Sci. 2013;29(4):1012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Ogedegbe G. Barriers to optimal hypertension control. J Clin Hypertens. 2008;10(8):644‐646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Wofford MR, Minor DS. Hypertension: issues in control and resistance. Curr Hypertens Rep. 2009;11(5):323‐328. [DOI] [PubMed] [Google Scholar]
- 58. Aggarwal R, Chiu N, Wadhera RK, et al. Racial/ethnic disparities in hypertension prevalence, awareness, treatment, and control in the United States, 2013 to 2018. Hypertension. 2021;78(6):1719‐1726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Modey Amoah E, Esinam Okai D, Manu A, Laar A, Akamah J, Torpey K. The role of lifestyle factors in controlling blood pressure among hypertensive patients in two health facilities in urban Ghana: a cross‐sectional study. Int J Hypertens. 2020;2020:1‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Campbell M, Fitzpatrick R, Haines A, et al. Framework for design and evaluation of complex interventions to improve health. BMJ. 2000;321(7262):694‐696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. WISoHW Group. 2003 World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. J Hypertens. 2003;21(11):1983‐1992. [DOI] [PubMed] [Google Scholar]
- 62. Committee G . 2003 European Society of Hypertension–European Society of Cardiology guidelines for the management of arterial hypertension. J Hypertens. 2003;21(6):1011‐1053. [DOI] [PubMed] [Google Scholar]
- 63. Ho PM, Rumsfeld JS. Beyond inpatient and outpatient care: alternative model for hypertension management. BMC Public Health. 2006;6:257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Saadat Z, Nikdoust F, Aerab‐Sheibani H, et al. Adherence to antihypertensives in patients with comorbid condition. Nephrourol Mon. 2015;7(4). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Mitchell AJ, Malone D, Doebbeling CC. Quality of medical care for people with and without comorbid mental illness and substance misuse: systematic review of comparative studies. Br J Psychiatry. 2009;194(6):491‐499. [DOI] [PubMed] [Google Scholar]
- 66. Ross S, Walker A, MacLeod MJ. Patient compliance in hypertension: role of illness perceptions and treatment beliefs. J Hum Hypertens. 2004;18(9):607‐613. [DOI] [PubMed] [Google Scholar]
- 67. Krousel‐Wood MA, Muntner P, Islam T, Morisky DE, Webber LS. Barriers to and determinants of medication adherence in hypertension management: perspective of the cohort study of medication adherence among older adults. Med Clin North Am. 2009;93(3):753‐769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. Mahmood S, Shah KU, Khan TM, et al. Non‐pharmacological management of hypertension: in the light of current research. Ir J Med Sci. 2019;188(2):437‐452. [DOI] [PubMed] [Google Scholar]
- 69. Group ToHPCR . Effects of weight loss and sodium reduction intervention on blood pressure and hypertension incidence in over‐weight people with high normal blood pressure: the Trials of Hypertension Prevention, Phase II. Arch Intern Med. 1997;157(6):657. [PubMed] [Google Scholar]
- 70. Whelton PK, Appel LJ, Espeland MA, et al. Sodium reduction and weight loss in the treatment of hypertension in older persons: a randomized controlled trial of nonpharmacologic interventions in the elderly (TONE). Jama. 1998;279(11):839. [DOI] [PubMed] [Google Scholar]
- 71. Mills KT, Chen J, Yang W, et al. Sodium excretion and the risk of cardiovascular disease in patients with chronic kidney disease. Jama. 2016;315(20):2200‐2210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Tuomilehto J, Jousilahti P, Rastenyte D, et al. Urinary sodium excretion and cardiovascular mortality in Finland: a prospective study. Lancet. 2001;357(9259):848‐851. [DOI] [PubMed] [Google Scholar]
- 73. Appel LJ. Lifestyle modification as a means to prevent and treat high blood pressure. J Am Soc Nephrol. 2003;14(suppl2):S99‐S102. [DOI] [PubMed] [Google Scholar]
- 74. Papakonstantinou E, Oikonomou C, Nychas G, Dimitriadis GD. Effects of diet, lifestyle, chrononutrition and alternative dietary interventions on postprandial glycemia and insulin resistance. Nutrients. 2022;14(4):823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Sacks FM, Svetkey LP, Vollmer WM, et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. N Engl J Med. 2001;344(1):3‐10. [DOI] [PubMed] [Google Scholar]
- 76. Lee H‐S, Duffey KJ, Popkin BM. Sodium and potassium intake patterns and trends in South Korea. J Hum Hypertens. 2013;27(5):298‐303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Du S, Neiman A, Batis C, et al. Understanding the patterns and trends of sodium intake, potassium intake, and sodium to potassium ratio and their effect on hypertension in China. Am J Clin Nutr. 2014;99(2):334‐343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Zhou B, Wang H, Wang W, Wu X, Fu L, Shi J. Long‐term effects of salt substitution on blood pressure in a rural north Chinese population. J Hum Hypertens. 2013;27(7):427‐433. [DOI] [PubMed] [Google Scholar]
- 79. Ojangba T, Zhang L, Wang Z. Compilation of supporting data on reducing salt (NaCl) for healthier meat and meat products. Int J Res. 2021;3(11):57‐69. [Google Scholar]
- 80. Parry S, Chow M, Batchelor F, Fary RE. Physical activity and sedentary behaviour in a residential aged care facility. Australas J Ageing. 2019;38(1):E12‐E18. [DOI] [PubMed] [Google Scholar]
- 81. Diaz KM, Booth JN III, Seals SR, et al. Physical activity and incident hypertension in African Americans: the Jackson Heart Study. Hypertension. 2017;69(3):421‐427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Knuttgen HG. Strength training and aerobic exercise: comparison and contrast. J Strength Cond Res. 2007;21(3):973‐978. [DOI] [PubMed] [Google Scholar]
- 83. Diaz KM, Shimbo D. Physical activity and the prevention of hypertension. Curr Hypertens Rep. 2013;15(6):659‐668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Whelton SP, Chin A, Xin X, He J. Effect of aerobic exercise on blood pressure: a meta‐analysis of randomized, controlled trials. Ann Intern Med. 2002;136(7):493‐503. [DOI] [PubMed] [Google Scholar]
- 85. Menanga A, Edie S, Nkoke C, et al. Factors associated with blood pressure control amongst adults with hypertension in Yaounde, Cameroon: a cross‐sectional study. Cardiovasc Diagn Ther. 2016;6(5):439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Acheampong K, Nyamari JM, Ganu D, et al. Predictors of hypertension among adult female population in Kpone‐Katamanso District, Ghana. Int J Hypertens. 2019;2019:1‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. Du Y, Liu B, Sun Y, Snetselaar LG, Wallace RB, Bao W. Trends in adherence to the physical activity guidelines for Americans for aerobic activity and time spent on sedentary behavior among US adults, 2007 to 2016. Jama. 2019;2(7):e197597‐e197597 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Egan BM. Physical activity and hypertension. Hypertens. 2017;69(3):404‐406. [DOI] [PubMed] [Google Scholar]
- 89. Benowitz NL, Gourlay SG. Cardiovascular toxicity of nicotine: implications for nicotine replacement therapy. J Am Coll Cardiol. 1997;29(7):1422‐1431. [DOI] [PubMed] [Google Scholar]
- 90. Robertson D, Frölich JC, Carr RK, et al. Effects of caffeine on plasma renin activity, catecholamines and blood pressure. Engl J Med. 1978;298(4):181‐186. [DOI] [PubMed] [Google Scholar]
- 91. Primatesta P, Falaschetti E, Gupta S, Marmot MG, Poulter NR. Association between smoking and blood pressure: evidence from the health survey for England. Hypertension. 2001;37(2):187‐193. [DOI] [PubMed] [Google Scholar]
- 92. O'Rourke M. Arterial stiffness, systolic blood pressure, and logical treatment of arterial hypertension. Hypertension. 1990;15(4):339‐347. [DOI] [PubMed] [Google Scholar]
- 93. Fogari R, Zoppi A, Lusardi P, Marasi G, Villa G, Vanasia A. Cigarette smoking and blood pressure in a worker population: a cross‐sectional study. J Cardiovasc Risk. 1996;3(1):55‐59. [PubMed] [Google Scholar]
- 94. Lowe FJ, Luettich K, Talikka M, et al. Development of an adverse outcome pathway for the onset of hypertension by oxidative stress‐mediated perturbation of endothelial nitric oxide bioavailability. Appl Vitro Toxicol. 2017;3(1):131‐148. [Google Scholar]
- 95. Habel LA, Cooper WO, Sox CM, et al. ADHD medications and risk of serious cardiovascular events in young and middle‐aged adults. Jama. 2011;306(24):2673‐2683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96. Roditis ML, Halpern‐Felsher B. Adolescents' perceptions of risks and benefits of conventional cigarettes, e‐cigarettes, and marijuana: a qualitative analysis. J Adolesc Health. 2015;57(2):179‐185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97. Jackler RK, Ramamurthi D. Nicotine arms race: JUUL and the high‐nicotine product market. Tob. Control. 2019;28(6):623‐628. [DOI] [PubMed] [Google Scholar]
- 98. Ebrahimi M, Heidari‐Bakavoli AR, Mazidi M, et al. Prevalence of hypertension, pre‐hypertension and undetected hypertension in Mashhad, Iran. Med J Nut Metab. 2017;9(3):213‐223. [Google Scholar]
- 99. Kannel WB. Hypertension as a risk factor for cardiac events‐epidemiologic results of long‐term studies. J Cardiovasc Pharmacol. 1993;21:S27‐37. [DOI] [PubMed] [Google Scholar]
- 100. Åberg F, Puukka P, Salomaa V, et al. Risks of light and moderate alcohol use in fatty liver disease: follow‐up of population cohorts. Hepatology. 2020;71(3):835‐848. [DOI] [PubMed] [Google Scholar]
- 101. Cushman WC, Cutler JA, Hanna E, et al. Prevention and Treatment of Hypertension Study (PATHS): effects of an alcohol treatment program on blood pressure. Arch Intern Med. 1998;158(11):1197‐1207. [DOI] [PubMed] [Google Scholar]
- 102. Maasland DH, van den Brandt PA, Kremer B, Goldbohm RA, Schouten LJ. Alcohol consumption, cigarette smoking and the risk of subtypes of head‐neck cancer: results from the Netherlands cohort study. BMC Cancer. 2014;14:187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103. Grotto D, Zied E. The standard American diet and its relationship to the health status of Americans. Nutr Clin Pract. 2010;25(6):603‐612. [DOI] [PubMed] [Google Scholar]
- 104. Volk BM, Kunces LJ, Freidenreich DJ, et al. Effects of step‐wise increases in dietary carbohydrate on circulating saturated fatty acids and palmitoleic acid in adults with metabolic syndrome. PLoS One. 2014;9(11):e113605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105. Stricker S, Rudloff S, Geier A, Steveling A, Roeb E, Zimmer K‐P. Fructose consumption—free sugars and their health effects. Dtsch Arztebl Int. 2021;118(5):71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106. Krauss RM, Eckel RH, Howard B, et al. AHA dietary guidelines: revision 2000: a statement for healthcare professionals from the nutrition committee of the American Heart Association. Circulation. 2000;102(18):2284‐2299. [DOI] [PubMed] [Google Scholar]
- 107. Chawla R, Patil G. Soluble dietary fiber. Compr Rev Food Sci Food Saf. 2010;9(2):178‐196. [Google Scholar]
- 108. Ferrara LA, Raimondi AS, d'Episcopo L, Guida L, Russo AD, Marotta T. Olive oil and reduced need for antihypertensive medications. Arch Intern Med. 2000;160(6):837‐842. [DOI] [PubMed] [Google Scholar]
- 109. Appel LJ, Miller ER, Seidler AJ, Whelton PK. Does supplementation of diet with'fish oil'reduce blood pressure?: a meta‐analysis of controlled clinical trials. Arch Intern Med. 1993;153(12):1429‐1438. [PubMed] [Google Scholar]
- 110. He J, Whelton PK. Effect of dietary fiber and protein intake on blood pressure: a review of epidemiologic evidence. Clin Hypertens. 1999;21(5‐6):785‐796. [DOI] [PubMed] [Google Scholar]
- 111. Wang Y, WS Y Jr, Yu D, Champagne C, Appel L, Lin P. The relationship between dietary protein intake and blood pressure: results from the PREMIER study. J Hum Hypertens. 2008;22(11):745‐754. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, to any qualified researcher.