

Abstract
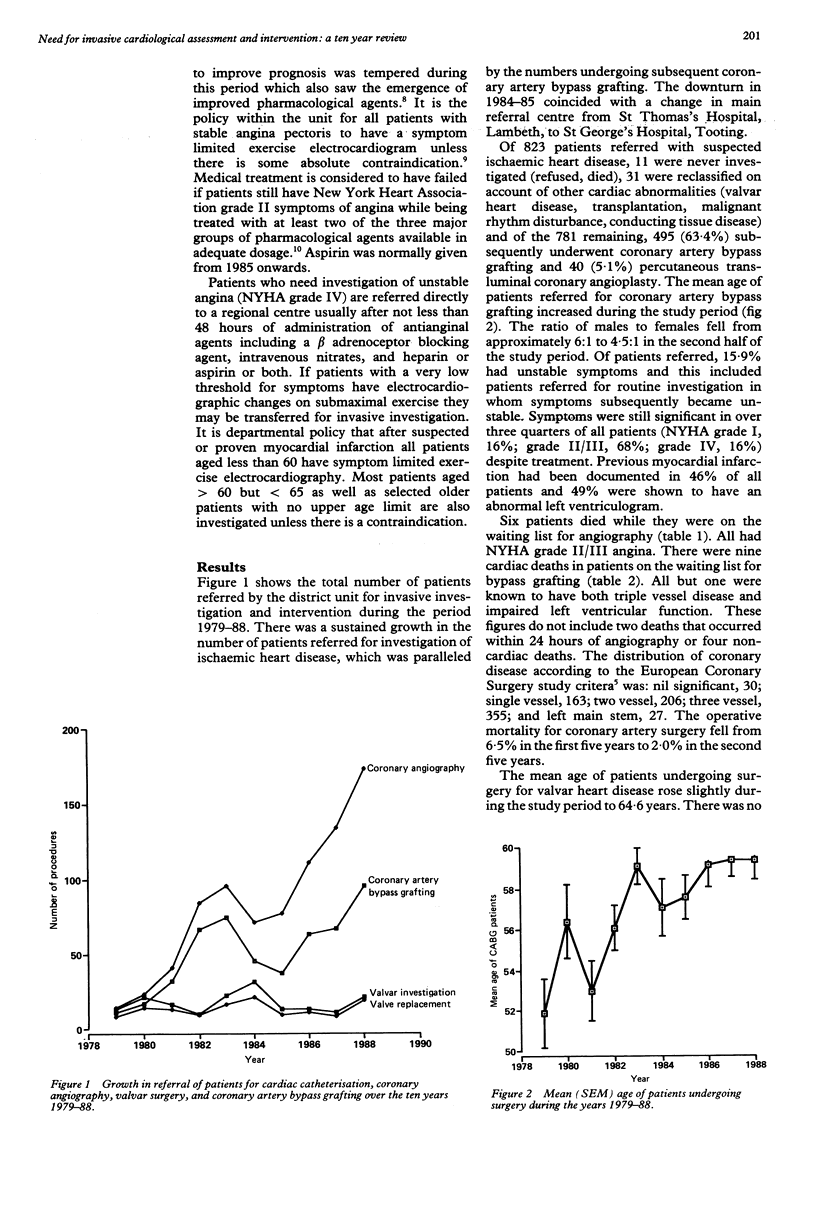
The uptake of invasive cardiological investigation and cardiopulmonary bypass procedures by the North West Surrey Health District was audited over the years 1979-88. Growth was almost continuous throughout the ten year period. The need within the district each year for coronary angiography seemed to be between 111 and 171 and for surgical revascularisation of the myocardium between 63 and 96 procedures; the first figure is the mean of the second quinquennial period (1984-88) and the second figure the total for 1988. After correction for the standardised mortality ratio and catchment area, the national requirement should lie between 690 and 1070 coronary angiograms and 390 and 600 coronary artery bypass graft operations per million population each year. There is a further national requirement for 70 valvar heart operations and 30 miscellaneous procedures per million population each year. Owing to delays in the provision of services, 20 patients died of a cardiovascular cause while they were on the waiting list for investigation or surgery. In the United Kingdom the annual target to be achieved by 1990 was 300 coronary artery bypass procedures per million population.
Full text
PDF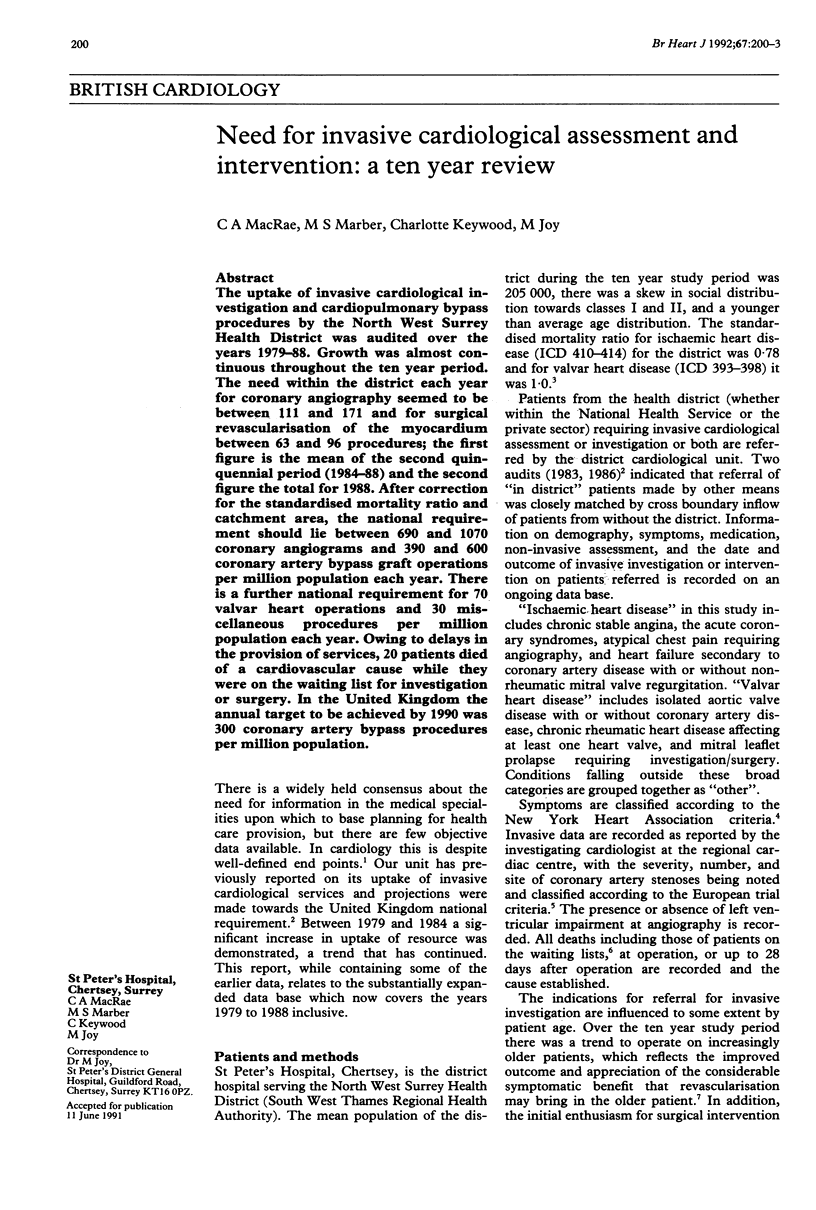

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bonow R. O., Kent K. M., Rosing D. R., Lan K. K., Lakatos E., Borer J. S., Bacharach S. L., Green M. V., Epstein S. E. Exercise-induced ischemia in mildly symptomatic patients with coronary-artery disease and preserved left ventricular function. Identification of subgroups at risk of death during medical therapy. N Engl J Med. 1984 Nov 22;311(21):1339–1345. doi: 10.1056/NEJM198411223112103. [DOI] [PubMed] [Google Scholar]
- Cripps T., Dennis M. S., Joy M. The need for invasive cardiological assessment and operation: viewpoint of a district general hospital. Br Heart J. 1986 May;55(5):488–493. doi: 10.1136/hrt.55.5.488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldschlager N., Selzer A., Cohn K. Treadmill stress tests as indicators of presence and severity of coronary artery disease. Ann Intern Med. 1976 Sep;85(3):277–286. doi: 10.7326/0003-4819-85-3-277. [DOI] [PubMed] [Google Scholar]
- Klein R. On the Oregon trail: rationing health care. BMJ. 1991 Jan 5;302(6767):1–2. doi: 10.1136/bmj.302.6767.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loop F. D., Lytle B. W., Cosgrove D. M., Goormastic M., Taylor P. C., Golding L. A., Stewart R. W., Gill C. C. Coronary artery bypass graft surgery in the elderly. Indications and outcome. Cleve Clin J Med. 1988 Jan-Feb;55(1):23–34. doi: 10.3949/ccjm.55.1.23. [DOI] [PubMed] [Google Scholar]
- Rutherford J. D., Braunwald E. Selection of patients for the surgical treatment of coronary artery disease. Q J Med. 1988 May;67(253):369–385. [PubMed] [Google Scholar]
- Tolins M., Weir E. K., Chesler E., Pierpont G. L. "Maximal" drug therapy is not necessarily optimal in chronic angina pectoris. J Am Coll Cardiol. 1984 Apr;3(4):1051–1057. doi: 10.1016/s0735-1097(84)80366-6. [DOI] [PubMed] [Google Scholar]
- Varnauskas E. Twelve-year follow-up of survival in the randomized European Coronary Surgery Study. N Engl J Med. 1988 Aug 11;319(6):332–337. doi: 10.1056/NEJM198808113190603. [DOI] [PubMed] [Google Scholar]