

Abstract
Purpose
To determine the role of Doppler ultrasonography when combined with B-mode ultrasonography in diagnosing uterine intracavitary pathologies (UIPs) in perimenopausal and postmenopausal bleeding women.
Methods
This multicentre prospective observational study included 150 women aged > 40 years with abnormal uterine bleeding (AUB), who were hospitalised at Hospital X and Hospital Y between June 2016 and June 2019. All participants underwent transvaginal B-mode ultrasound and transvaginal Doppler ultrasound, and the results of sonography were compared to histopathological endpoint.
Results
The morphological features, structure, margin, border line of the endometrial-mass lesion, intracavitary uterine fluid, and Doppler signal clearly differed between benign and malignant intracavitary pathologies (p < 0.0001). However, echogenicity had a limited value in differentiating among UIPs (p = 0.1). The sensitivity and specificity of the pedicle sign in diagnosing endometrial polyps were 50.0% and 97.6%; for the circular pattern in endometrial fibroids were 46.2% and 100.0%; for the multiple vessel pattern in endometrial cancer were 64.0% and 96.0%; and for the scattered vessel pattern in endometrial hyperplasia were 43.96% and 56.43%, respectively. The additional value of Doppler ultrasound was greater than that of separate B-mode ultrasound in assessing UIPs in our study.
Conclusions
B-mode ultrasound used in combination with Doppler as a noninvasive tool was significantly valuable in the diagnostic procedures for UIPs in perimenopausal and postmenopausal bleeding women. Doppler ultrasound and B-mode transvaginal ultrasound should be used together routinely for discrimination between malignant diseases and benign endometrial changes. Further studies are needed to better understand the benefits of combining Doppler ultrasound and B-mode ultrasound in routine sonographic practice.
Keywords: Abnormal uterine bleeding, B-mode sonography, Doppler transvaginal ultrasound, Intracavitary uterine pathologies, Perimenopause, Postmenopause
Key points
| The morphological features, structure, margin, border line of the endometrial-mass lesion, uterine intracavitary fluid, and Doppler signal clearly differed between benign and malignant intracavitary pathologies; however, echogenicity did not. |
| A difference exists in the proportion of dominant vascular pattern following UIPs. |
| Adding Doppler ultrasound to B-mode ultrasound is useful in diagnosing UIPs and helps in differentiating between benign and malignant intrauterine lesions in peri-and postmenopausal women with AUB, especially in low-resource settings that lack other imaging modalities. |
Introduction
Abnormal uterine bleeding (AUB) is defined as bleeding from the uterus that differs from the normal menstrual cycle in terms of quantity, duration, regularity, and frequency, without relation to pregnancy [1]. AUB occurs in 70% of perimenopausal and postmenopausal women and dramatically affects the quality of life in women aged > 40 years old worldwide [2]. Uterine intracavitary pathologies (UIPs) are common structural causes of AUB; they include endometrial polyps (EP), endometrial hyperplasia (EH), submucosal/endometrial fibroids (EF), and endometrial cancer (EC) [3, 4]. Investigating the etiologies of AUB in the assessment of perimenopausal and postmenopausal bleeding women is a fundamental step in gynecologic practice for the management of uterine cancer [5]. Currently, we have many diagnostic methods, each with advantages and disadvantages, including non-invasive imaging modalities (sonography, computed tomography, magnetic resonance imaging) and invasive procedures (blind biopsy, hysteroscopy) [6, 7]. B-mode ultrasound is an easily accessible modality and a cost-effective tool for investigating the abnormal structure and morphological features of the uterus, especially in low-middle income countries and low-resource settings [8]. Furthermore, many studies have shown that Doppler ultrasound can be used routinely to detect vascular proliferation in gynecologic tumors [9–11]. Additionally, the dominant vascular phenotype can help diagnose UIPs. In 2015, Cogendez et al. showed the value of transvaginal Doppler ultrasound in the diagnosis of polyps by vascular pedicle and endometrial fibroid, using the circular vascular imaging as soft markers. The sensitivity and positive predictive value of these patterns were 80.0%, 100.0%, 72.0%, and 100.0%, respectively [12]. In addition, Alcazar et al. demonstrated that multiple angiogenesis signs were pivotal features of endometrial cancer, with a sensitivity of 78.8%, specificity of 100.0%, and PPV of 100.0%, meanwhile, endometrial hyperplasia was more commonly associated with a scattered vascular proliferation [13]. Therefore, we aimed to determine the value of B-mode ultrasound combined with Doppler ultrasound as a diagnostic method in perimenopausal and postmenopausal women with AUB.
Materials and methods
This multicentre prospective observational study was conducted according to the standards of the Ethics Committee of the Hue University of Medicine and Pharmacy and was approved by our Institutional Review Board (IRB), with number 1435-QD/DHYD. Written informed consent was obtained from all patients. This study was performed at Hue University Hospital and Hue Central Hospital between June 2016 and June 2019.
The inclusion criteria were as follows: all women > 40 years of age complaining of abnormal uterine bleeding, perimenopausal or postmenopausal. The patients underwent transvaginal B-mode ultrasound and Doppler ultrasound, using histopathological results for comparison.
Exclusion criteria were vaginal bleeding related to pregnancy, hormone replacement therapy, tamoxifen, or coagulation disorders; vaginal bleeding not originating from the uterine cavity; abnormalities associated with the cervix; iatrogenic bleeding; and lack of information on the study protocol.
A total of 150 women were recruited for this study. All patients were evaluated based on medical history, general examination, gynecologic examination, cervical cytology (Pap smear) and laboratory investigations (complete blood count, liver function tests, kidney function tests, and coagulation profile). Transvaginal sonography was performed on all patients using a 5–7.5 MHz endovaginal transducer of a sonographic machine (Samsung WS80A, HS70A). One of four sonographers, each with more than 5 years of experience, was randomly assigned to each patient.
All patients underwent interventional procedures, such as endometrial biopsy, hysteroscopy, myomectomy, or hysterectomy. These indications were determined according to the hospital’s medical protocol (Fig. 1).
Fig. 1.

Study flowchart
Features of intracavitary abnormalities on morphological ultrasound
Intracavitary fluid, structure, echogenicity, border, and endometrial–myometrial boundary of the endometrium/lesion were classified according to the International Endometrial Tumor Analysis (IETA) System, evaluated using B-mode ultrasound (Fig. 2). While evaluating, each practioner first determined the location of the uterus and allowed it to occupy 2/3 of the screen for the clearest image [14–16].
Fig. 2.

Morphologic evaluation of uterine intracavitary pathologies by International Endometrial Tumor Analysis (IETA)
Determination of predominant angiostenosis pattern
According to color/power Doppler flow mapping, four different vascular patterns were defined, as described in Fig. 3:
Scattered vessel pattern: disseminated vascular in the endometrium. This pattern was considered characteristic of endometrial hyperplasia [13].
Multiple vascular pattern: multiple vessels present at the endometrium and at the myometrial–endometrial interface. This pattern was considered characteristic of endometrial cancer, since angiogenesis proliferation occurs in endometrial cancer within tumor tissue and the surrounding area.
Pedicle vascular pattern: a single vessel penetrates the endometrium from the myometrium. This pattern was considered characteristic of endometrial polyps, since the vessel is thought to correspond to a vascularised polyp’s pedicle.
Circular vascular pattern (rim-likely form, circle-shaped form, or ring-shaped): increased vascularity in the peripheral surrounding of the tumor. This pattern was considered characteristic of uterine fibroids.
Fig. 3.

Pattern of angiogenesis vessels in the present study
All morphological and structural features of endometrium, lesion mass, and intracavitary uterine abnormalities were evaluated on B-mode ultrasound following IETA standards [17].
Phenotypes of vascular angiogenesis such as pedicle vessel, scattered vessel, multiple-vessel, circular vascular pattern, and lacking vascular pattern were determined by sonographers with more than 5 years of experience.
Endometrial hyperplasia, endometrial polyp, endometrial fibroid, and endometrial cancer were identified via histopathological results.
Each was coded in categorical variables.
Statistical analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS), version 20.0. Data collected were presented as number (n), percentage (%), and comparison between categorical variable groups using Chi-squared test. p-value < 0.05 was considered statistically significant. Cohen’s kappa coefficient (k) was used to measure interrater reliability for result of B-mode ultrasound, Doppler ultrasound, and histopathological endpoint. Test’s value was identified following Se(%), Sp(%), PPV(%), NPV(%), AC(%), LR ( +), and LR( −).
Results
Regarding the structure of the endometrium/lesion mass, almost all endometrial fibroid and malignant lesions showed heterogeneous-mixed echogenicity, while other benign pathologies were predominantly homogenous. Most lesions had hyperechogenic echogenicity; however, the hypoechoic form was predominant (7/13 cases) with endometrial fibroids. In the present study, 20/25 (80%) cases of endometrial cancer were characterised by irregularly unidentified borders; on the other hand, 97.8% of endometrial hyperplasia cases were clearly distinguished from the endometrial–myometrial boundary, and 100% of endometrial polyp and submucosal fibroid cases were clearly observed (p < 0.0001). The endometrial–myometrial boundary in endometrial cancer was unidentified in 5/6 (83.3%) cases and identified in 1/6 (16.7%) cases.
In the benign group, the endometrial–myometrial junction was regular in almost all (94.4%) cases; irregular junctions only accounted for 5.6% of cases. In contrast, 24 out of 25 (96%) cases were irregular (p < 0.0001) in the malignant group. In intracavitary lesions, fluid was absent in almost all (88%) benign lesions, while in endometrial cancer cases, intracavitary fluid was present in 56% of cases. In our study, 14/25 (56%) endometrial cancer cases were hypoechogenic and mixed-echogenic in intracavitary fluid; in contrast, fluid was present in only 11.8% of benign cases (p < 0.0001). Additionally, 9/91 cases of endometrial hyperplasia, 3/16 cases of polyps, 2/13 cases of endometrial fibroids, and 1/5 other cases had intracavitary fluid; the majority, however, showed no fluid and were hypoechogenic (Table 1).
Table 1.
Morphological and structural features of uterine intracavitary pathologies
| Features | Characteristic | Benign pathologies n (%) | Malignant pathology n (%) | p test value* | ||||
|---|---|---|---|---|---|---|---|---|
| EH | EP | EF | Others | Total | EC | |||
| Endometrial/lesion structure | Uniform | 65 (71.4) | 11 (68.8) | 0 (0.0) | 3 (60.0) | 78 (62.4) | 3 (12.0) | < 0.0001 |
| Non-uniform | 26 (28.6) | 5 (31.3) | 13 (100.0) | 2 (40.0) | 47 (37.6) | 22 (88.0) | ||
| Endometrial/lesion echogenicity | Hyperechogenic | 85 (93.4) | 14 (87.5) | 7 (53.8) | 5 (83.3) | 111 (88.8) | 19 (76.0) | 0.1 |
| Hypoechogenic | 4 (4.4) | 2 (12.5) | 6 (46.2) | 1 (16.7) | 12 (9.6) | 6 (24.0) | ||
| Homoechogenic | 2 (2.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (1.6) | 0 (0.0) | ||
| Endometrial–myometrium junction | Identified | 89 (97.8) | 16 (100.0) | 13 (100.0) | 4 (80.0) | 122 (97.6) | 5 (20.0) | < 0.0001 |
| Unidentified | 2 (2.2) | 0 (0.0) | 0 (0.0) | 1 (20.0) | 3 (2.4) | 20 (80.0) | ||
| Endometrial/lesion bordeline | Regular | 85 (93.4) | 16 (100.0) | 13 (100.0) | 4 (80.0) | 118 (94.4) | 1 (4.0) | < 0.0001 |
| Irregular | 6 (6.6) | 0 (0.0) | 0 (0.0) | 1 (20.0) | 7 (5.6) | 24 (96.0) | ||
| Intracavitary fluid | Absent | 82 (90.1) | 13 (81.3) | 11 (84.6) | 4 (80.0) | 110 (88.0) | 11 (44.0) | < 0.0001 |
| Hypoechogenic | 8 (8.8) | 2 (12.5) | 2 (15.4) | 0 (0.0) | 12 (9.6) | 7 (28.0) | ||
| Heterogeneous | 1 (1.1) | 1 (6.3) | 0 (0.0) | 1 (20.0) | 3 (2.4) | 7 (28.0) | ||
EC endometrial cancer; EH endometrial hyperplasia; EP endometrial polyps; EF endometrial fibroid
*p value from χ2 test (Chi-squared test)
In the malignant group, detectable Doppler signals were present in 24/25 (99%) cases; in the benign group, they appeared in only 72/125 (57.6%) cases. In the benign group, only 48.4% of cases of endometrial hyperplasia were detected with Doppler signal, but 75.0% of polyps and 100% of endometrial fibroids had Doppler signals (Table 2, Fig. 4).
Table 2.
Distribution of dominant vascular pattern following uterine intracavitary pathologies
| Pathology | ||||||
|---|---|---|---|---|---|---|
| Vascular pattern | EC | EP | EF | EH | Other | Total |
| n (%) | n (%) | n (%) | n (%) | n (%) | ||
| Lacking vascular presence | 1 (4.0) | 4 (25.0) | 0 (0.0) | 47 (51.6) | 2 (40.0) | 54 |
| Scattered vessel | 8 (32.0) | 3 (18.8) | 4 (30.8) | 40 (44.0) | 3 (60.0) | 58 |
| Circular vessel | 0 (0.0) | 0 (0.0) | 6 (46.2) | 0 (0.0) | 0 (0.0) | 6 |
| Multiple vessel | 16 (64.0) | 1 (6.2) | 2 (15.4) | 2 (2.2) | 0 (0.0) | 21 |
| Pedicle vessel | 0 (0.0) | 8 (50.0) | 1 (7.7) | 2 (2.2) | 0 (0.0) | 11 |
| Total | 25 (100.0) | 16 (100.0) | 13 (100.0) | 91 (100.0) | 5 (100.0) | 150 |
EC endometrial cancer; EH endometrial hyperplasia; EP endometrial polyps; EF endometrial fibroid
Fig. 4.
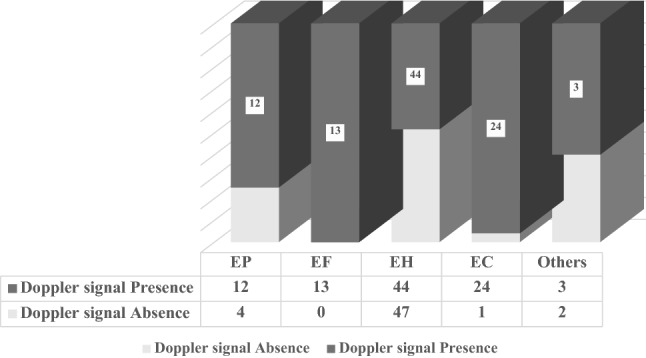
Frequency of Doppler signal following uterine intracavitary pathologies
In the endometrial cancer group, the multiple vascular pattern accounted for 64.0% of cases. In cases of polyps, pedicle vascularity accounted for 50%. In the endometrial fibroid group, the circular vascular pattern accounted for 46.2% of cases. Vascular proliferation was absent in almost all endometrial hyperplasia cases; nevertheless, if there was a Doppler signal, it was a scattered vessel pattern (44%). In general, most of the dominant vascular phenotypes had low sensitivity for diagnosing intracavitary pathologies (< 80%) but showed high specificity (> 80%). The scattered vessel pattern could be observed in many different pathologies. The circular vascular pattern was a specific feature of endometrial fibroids and did not appear in other pathologies (Sp, 100% and PPV, 100%) (Table 3).
Table 3.
Diagnostic value of dominant vascular pattern
| Vascular pattern | Se (%) | Sp (%) | PPV (%) | NPV (%) | AC (%) | LR + | LR − |
|---|---|---|---|---|---|---|---|
| Scattered vessel | 43.96 | 56.43 | 68.97 | 30.51 | 54.0 | 1.00 | 0.99 |
| Circular vessel | 46.2 | 100.0 | 100.0 | 95.14 | 95.33 | - | 0.54 |
| Multiple vessel | 64.0 | 96.0 | 76.19 | 93.02 | 90.67 | 16.0 | 0.38 |
| Pedicle vessel | 50.0 | 97.76 | 72.73 | 94.24 | 92.67 | 22.32 | 0.51 |
Se sensitivity; Sp specificity; PPV positive predicting value; NPV negative predicting value; AC accurate; LR ( +) positive likelihood ratio; LR − negative likelihood ratio
The present study included 133 cases examined with transvaginal B-mode ultrasound. Sonography detected only 5/23 cases of endometrial cancer. In contrast, B-mode ultrasound was accurate in 63/79 cases of endometrial hyperplasia, 8/12 cases of endometrial fibroids, and 8/14 cases of endometrial polyps. Doppler ultrasound accurately identified 21/25 of cases with histopathological endpoints in endometrial cancer. Similarly, 76/91 of endometrial hyperplasia cases were diagnosed by ultrasound, compatible with histopathological results; polyps were diagnosed by ultrasound in 13/16 cases, and endometrial fibroids were diagnosed by ultrasound in 12/13 cases (Table 4).
Table 4.
Diagnostic value of ultrasound in accordance with histopathological result
| Ultrasound | Pathologies | ||||||
|---|---|---|---|---|---|---|---|
| EC | EP | EF | EH | Otherb | Total | ||
| n (%) | n (%) | n (%) | n (%) | n (%) | N | ||
| Doppler | EC | 21 (84.0) | 0 (0.0) | 0 (0.0) | 1 (1.1) | 1 (20.0) | 23 |
| EP | 0 (0.0) | 12 (75.0) | 1 (7.7) | 6 (6.6) | 0 (0.0) | 19 | |
| EF | 1 (4.0) | 1 (6.2) | 12 (92.3) | 1 (1.1) | 0 (0.0) | 15 | |
| EH | 2 (8.0) | 2 (12.6) | 0 (0.0) | 76 (83.6) | 4 (80.0) | 84 | |
| Othersa | 1 (4.0) | 1 (6.2) | 0 (0.0) | 7 (7.7) | 0 (0.0) | 9 | |
| Total | 25 (100.0) | 16 (100.0) | 13 (100.0) | 91 (100.0) | 5 (100.0) | 150 | |
| B-mode | EC | 5 (21.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (20.0) | 6 |
| EP | 0 (0.0) | 8 (57.1) | 2 (16.7) | 5 (6.3) | 0 (0.0) | 15 | |
| EF | 1 (4.3) | 1 (7.1) | 8 (66.6) | 0 (0.0) | 0 (0.0) | 10 | |
| EH | 9 (39.2) | 3 (21.5) | 0 (0.0) | 63 (79.8) | 3 (60.0) | 78 | |
| Otherc | 8 (34.8) | 2 (14.3) | 2 (16.7) | 11 (13.9) | 1 (20.0) | 24 | |
| Total | 23 (100.0) | 14 (100.0) | 12 (100.0) | 79 (100.0) | 6 (100.0) | 133** | |
EC endometrial cancer; EH endometrial hyperplasia; EP endometrial polyps; EF endometrial fibroid
**133/150 cases had separately B-mode sonographic result, 17 missing cases due to lacking conclusion of sonographer
aUnidentified lesion, retained fluid
bNormal endometrium
cNormal sonographic image or unidentified uterine intracaviatary lesion
B-mode ultrasound and Doppler ultrasound had similar sensitivity in diagnosing endometrial hyperplasia (79.8% vs. 83.5%). However, we found a significant difference between B-mode ultrasound and Doppler ultrasound in the diagnosis of malignant lesions (21.7% vs. 84.0%). Based on the Kappa Index, Doppler ultrasound was more compatible with histopathological diagnosis than B-mode ultrasonography (Table 5).
Table 5.
Comparison between the conclusion of B-mode ultrasound and Doppler ultrasound with histopathological result
| Ultrasound | UIPs | Se (%) | PPV (%) | Kappa Index |
|---|---|---|---|---|
| B-mode | EC | 21.7 | 83.3 |
k = 0.452 (p < 0.0001) |
| EP | 57.1 | 53.3 | ||
| EF | 66.6 | 80.0 | ||
| EH | 79.8 | 80.8 | ||
| Doppler | EC | 84.0 | 91.3 |
k = 0.683 (p < 0.0001) |
| EP | 75.0 | 63.2 | ||
| EF | 92.3 | 80.0 | ||
| EH | 83.5 | 90.5 |
Se sensitivity; PPV positive predicting value; EC endometrial cancer; EH endometrial hyperplasia; EP endometrial polyps; EF endometrial fibroid; UIPs uterine intracavitary pathologies
Discussion
Morphological features of uterine intracavitary pathologies on B-mode ultrasound
Table 1 shows the heterogeneous echogenic structure was markedly predominant (88% of cases) in the endometrial lesions in the malignant group, compared to 37.6% of cases in the benign group. Meanwhile, more than half of benign cases were homogeneous (p < 0.0001). The echogenic structures of 100% of cases were heterogeneous in the malignant group, and 51% were homogenous in the benign group, which was in line with Ashour et al. (2017)’s study [18]. In a study by Madkour et al. (2017), 90% of the malignant group had mixed echogenicity, whereas 92% of the benign group had homogeneous echogenicity [19].
We found that the predominant echogenicity in the endometrial cancer group was hyperechogenic (76%), compared to the hypoechogenic form (24%), supporting Razik et al.’s findings [20]. In the benign group, 88.8% cases were hyperechoic, 9.6% cases were hypoechoic, and 1.6% cases were homogenous with uterine myometrial echogenicity. Similarly, Talaat et al. (2009) found the echogenic level of polyps was mostly hyperechogenicity, accounting for 91.2% (31/45) of cases, with three cases of hypoechogenicity (8.8%)) [21]. In Cil et al.’s (2010) study, in cases of polyps, hyperechogenicity accounted for 96.9% (31/32), while hypoechogenicity only accounted for 3.1% (1/10) [22]. In our study, these features were 87.5% and 12.5%, respectively; none of the cases were homoechogenic. By contrast, in submucosal fibroid cases, echogenicity accounted for only 5.9% (1/17), hypoechogenicity accounted for 47.1% (8/17), and homoechogenicity accounted for 47.1% (8/17) (p < 0.001). In Cil et al.’s (2010) study, hyperechogenicity accounted for 53.8% of cases, and hypoechogenicity was detected in 46.2% of cases [22]. Cogendez et al. found that, in the pathology of submucosal fibroids, echogenicity accounted for 11.1% (2/18) of cases, homoechogenicity accounted for 50% (9/18) of cases, and hypoechogenicity was found in 38.9% (7/18) of cases [12]. Thus, the level of echogenicity is not an important feature to distinguish between benign and malignant pathologies; it is only useful for discrimination among benign pathologies [23].
Our findings regarding the endometrial–myometrial junction showed that almost all malignant lesions were irregular, with unclear, discontinuous boundaries, whereas benign lesions had regular margins with clearly observable boundaries. In contrast, endometrial hyperplasia was characterised by sharply clear borderlines, present in 32/32 (100%) cases, similar to Razik et al.’s (2012) findings [20]. Ashour et al. (2017) found that regular borderlines accounted for 93.7% of benign cases, while irregular borderlines accounted for 6.3%. Endometrial margins had regular characteristics in 25% of malignant cases and irregular characteristics in 75% [18]. This can be explained by the invasive tendency of malignant lesions; the endometrial–myometrial boundary may disappear, resulting in an irregular endometrial border.
In the present study, hypoechogenous and mixed echogenous fluid were present in almost all malignant cases, unlike the benign group. Similarly, in a study by Talaat et al., there were 3/45 cases of polyps with intracavitary fluid [21]. Razik et al. found that 83.3% of endometrial cancer cases had uterine intracavitary fluid, and 100% of other diseases showed no fluid on ultrasound (p < 0.001) [20]. Thus, the presence of uterine intracavitary fluid in perimenopausal and postmenopausal women with AUB is possible in benign disease, but it is an alert sign for endometrial cancer, especially in postmenopausal bleeding women [10, 23]. In benign pathology, the presence of fluid can help in the differential diagnosis of endometrial polyp from fibroid [24].
Presence of Doppler signal in uterine intracavitary pathologies
Figure 4 shows that most malignant cases had a Doppler signal (96.0%), whereas a Doppler signal was detected in only 58.4% of the benign group. This characteristic is in accordance with the vascular proliferation of malignant diseases. In a study by Alcazar et al., signs of vascular proliferation were found in 32/33 cases of endometrial cancer, and only one case had no Doppler signal [13]. Recently, in a study by Li et al. (2019), 66.7% of endometrial cancer cases had Doppler signals, while only 11.1% of benign cases did. Therefore, the presence of Doppler signal in endometrial lesions is strongly related to the risk of malignancy (odds ratio (OR), 16.0; 95% CI: 1.3–192.8) [25, 26]. Nevertheless, we found that in the benign group, the Doppler signal was present in of 12/16 (75%) cases of polyps and 13/13 (100%) cases of endometrial fibroids.
Distribution characteristics and diagnostic values of dominant vascular phenotypes
Value diagnosis of multiple vascular pattern
In the present study, the predominant pattern in endometrial cancer was multiple vessel, in 16/25 (64%) of cases; a scattered vessel pattern accounted for 32% cases. This aligns with the results of El Kady in Egypt [27]. In a study by Madkour et al. (2017), signs of multiple angiogenesis were found in 7/10 cancer cases; in the remaining cases, one showed disseminated vascular proliferation and two lacked Doppler signals [19]. In our study, the LR index ( +) was 16, showing that signs of multiple vascularity were valuable for diagnosing endometrial cancer (Table 3).
Valuable diagnosis of pedicle vascular pattern
Table 2 shows that, in the polyp group, the predominant pattern was vascular pedicle in 8/16 (50%) of cases, followed by scattered vessels in 3/16 (18.8%) of cases and multiple vessels in 1/16 (5.9%). In a study by Amreen et al. (2018), the vascular pedicle sign was found in 13/16 (76.5%) of cases; moreover, the polyp size was related to the vascular pedicle sign. The more common the vascular pedicle sign, the larger the polyp; the average size of polyps in the study was 17.77 mm (p = 0.044) [28]. This assessment differs from that of Medina et al. (2002), who found no association between polyp size and vascular pedicle sign [29]. In our study, the LR index ( +) of 22.32 showed the value of the vascular pedicle sign in diagnosing polyps (Table 3).
Valuable diagnosis of circular vascular pattern
In our study, the predominant vascular pattern of endometrial fibroids was rim-likely vascularity, found in 6/13 (46.2%) cases, followed by scattered vessel in 4/13 (30.8%) cases, multiple vessel in 2/13 (15.4%) cases (15.4%), and pedicle vessel pattern in 1/13 (7.7%) cases. According to Cogendez et al., in patients with endometrial fibroids, 72.2% had signs of circular vascularity, 27.8% had multiple angiogenesis, and none had single vascular pattern [12]. Thus, in endometrial fibroids, the circular flow may be present or absent; however, if the circular vascular pattern is present, its diagnostic value for the endometrial fibroids is 100%, making it an extremely specified phenotype for endometrial fibroids (Table 3).
Valuable diagnosis of scattered vascular pattern
In the endometrial hyperplasia group in our study, 47/91 (51.6%) cases were diagnosed without vascular proliferation, 40/91 (44%) cases with scattered vascular proliferation, 2/91 cases with multiple vessel patterns, and 2/91 cases with pedicle vessel pattern. In Cogendez et al., signs of scattered vascular proliferation were found in 72.7% of cases of endometrial hyperplasia; however, they were also observed in 66.7% cases of endometrial atrophy [12]. Consequently, signs of scattered vascular pattern were not specific to endometrial hyperplasia, and this pattern can be present in other UIPs. The diagnostic value of scattered vascular sign in endometrial hyperplasia was low, with a sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of 43.96%, 56.43, 68.97%, 30.51%, and 54.0% respectively; the positive likelihood index LR ( +) was 1.0 (Table 3).
Value of B-mode ultrasound compared to Doppler ultrasound
Our study found that Doppler ultrasound is more accurate than B-mode ultrasound for the diagnosis of UIPs. Doppler signal detection was sensitive for intracavitary lesion masses with specific vascular patterns. Commonly, malignant pathologies were present with multiple vascular proliferation (Table 5). In 2019, Liu et al. also reported the value of Doppler ultrasound in the detection of endometrial malignant disease [30]. Additionally, Cil et al. showed that power Doppler blood flow mapping is a valuable tool in the diagnosis of focal endometrial pathology and is helpful in distinguishing submucosal fibroids and endometrial polyps [22].
Strengths and limitations of the study
The research was conducted at two tertiary healthcare centres, and the ultrasonographic technique was performed by sonographers with more than 5 years of experience; therefore, the sonographic results are accurately reliable. Moreover, this study was based on interventional procedures (endometrial biopsy, hysteroscopy, hysterectomy), and the sonographic results were compared to histopathologic endpoints, providing valuable analysis. Nevertheless, as this study was conducted at two centres with two different sonographic machines and the results were collected by four sonographers, we could not avoid study bias. The sample size was limited, and more data are required to support our conclusions.
Future implications
In addition to described sonographic features in this study, Nguyen P.N. et al. recently demonstrated the value of the spectral Doppler indices of uterine artery resistance index (RI) and pulsatility index (PI) in differentiating malignant and benign pathologies [31]. Further research is needed to use ultrasound (including B-mode, Doppler, and three-dimension) and clinical risk factors to develop a model to calculate the percentage of detection of malignant endometrial diseases in peri- and postmenopausal bleeding women in the future [7, 30, 32–35].
Conclusion
Morphological features, structural features, borders, endometrial–myometrial junctions, fluid, and Doppler signals were clearly different among uterine pathologies and between benign and malignant groups, while the level of echogenicity was less useful. Using Doppler ultrasound, we found differences in the proportions of dominant vessel patterns among patients with UIPs. Combining Doppler ultrasound and B-mode transvaginal ultrasound can help differentiate among UIPs. Further studies are needed to better understand the benefits of adding Doppler ultrasound to B-mode ultrasound in routine sonographic practice.
Acknowledgments
We thank the patients, who agreed to allow us to participate in our research and to publish their clinical data. The authors are also grateful to all teachers and colleagues working at the Department of Gynecology, the Department of Image Diagnostic, and the Department of Histopathology at Hue Central Hospital and at Hue University Hospital. We are thankful directly to PhD. M.D Van Duc Vo, Ph.D. M.D Thao Nguyen Nguyen Tran, M.D. Ngoc Ty Nguyen Thi., M.D. Diem Thu Nguyen Thi, M.D. Phuong Minh Nguyen Thi, M.D. Thanh Thuy Tran Thi. All of them attributed to provide us the pictures, take care for patient and shared their precious experiences related to manage this clinical course with us.
Abbreviations
- AUB
Abnormal uterine bleeding
- EC
Endometrial cancer
- EH
Endometrial hyperplasia
- EP
Endometrial polyps
- EF
Endometrial fibroid
- TV-CDU
Transvaginal color Doppler ultrasound
- UIPs
Uterine intracavitary pathologies
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declarations
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by Ethical Committee of the Hue University of Medicine and Pharmacy with IRB approval number 1435/QD-DHYD.
Informed consent
Written informed consent was obtained from the patients for recruitment in study.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Phuc Nhon Nguyen, Email: docternhon@gmail.com.
Van Tuan Nguyen, Email: tuancdythue@yahoo.com.
References
- 1.Vitale SG, Watrowski R, Barra F, et al. Abnormal uterine bleeding in perimenopausal women: the role of hysteroscopy and its impact on quality of life and sexuality. Diagnostics (Basel) 2022;12(5):1176. doi: 10.3390/diagnostics12051176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Feliciano EE, Santos AM, Agunod CD, Boshra AY, Suliman S, Malabanan MC. Perimenopausal women distressing from abnormal uterine bleeding: a Philippine quality of life assessment-based correlational study. Ann Med Health Sci Res. 2020;10:838–845. [Google Scholar]
- 3.Committee on Practice Bulletins—Gynecology (2021) Practice bulletin no. 128: diagnosis of abnormal uterine bleeding in reproductive-aged women. Obstet Gynecol 120(1):197–206. 10.1097/AOG.0b013e318262e320 [DOI] [PubMed]
- 4.Practice bulletin no. 136 (2013) Management of abnormal uterine bleeding associated with ovulatory dysfunction. Obstet Gynecol 122(1) [DOI] [PubMed]
- 5.Boeckstaens S, Dewalheyns S, Heremans R, et al. Signs and symptoms associated with uterine cancer in pre- and postmenopausal women. Heliyon. 2020;6(11):e05372. doi: 10.1016/j.heliyon.2020.e05372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yao Y, Lv W, Xie X, Cheng X. The value of hysteroscopy and transvaginal ultrasonography in the diagnosis of endometrial hyperplasia: a systematic review and meta-analysis. Transl Cancer Res. 2019;8(4):1179–1187. doi: 10.21037/tcr.2019.06.33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jones ER, O’Flynn H, Njoku K, Crosbie EJ. Detecting endometrial cancer. Obstet Gynaecol. 2021;23(2):103–112. doi: 10.1111/tog.12722. [DOI] [Google Scholar]
- 8.Abdalla S, Abou-Taleb H, Badary DM, Ali WA. Multiparametric transvaginal ultrasound in the diagnosis of endometrial cancer in post-menopausal bleeding: diagnostic performance of a transvaginal algorithm and reproducibility amongst less experienced observers. Br J Radiol. 2021;94(1119):20201195. doi: 10.1259/bjr.20201195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Goyal M, Agarwal VK. Diagnostic Accuracy of B-mode USG and doppler scan for ovarian lesions. J Clin Diagn Res. 2016;10(9):TC01–TC04. doi: 10.7860/JCDR/2016/20619.8446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Epstein E, Valentin L. Gray-scale ultrasound morphology in the presence or absence of intrauterine fluid and vascularity as assessed by color Doppler for discrimination between benign and malignant endometrium in women with postmenopausal bleeding. Ultrasound Obstet Gynecol. 2006;28(1):89–95. doi: 10.1002/uog.2782. [DOI] [PubMed] [Google Scholar]
- 11.El-Sharkawy M, El-Mazny A, Ramadan W, Hatem D, Abdel-Hafiz A, Hammam M, et al. Three-dimensional ultrasonography and power Doppler for discrimination between benign and malignant endometrium in premenopausal women with abnormal uterine bleeding. BMC Womens Health. 2016;16:18. doi: 10.1186/s12905-016-0297-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cogendez E, Eken MK, Bakal N, et al. The role of transvaginal power Doppler ultrasound in the differential diagnosis of benign intrauterine focal lesions. J Med Ultrasonics. 2015;42:533–540. doi: 10.1007/s10396-015-0628-2. [DOI] [PubMed] [Google Scholar]
- 13.Alcazar JL, Castillo G, Minguez JA, Galan MJ. Endometrial blood flow mapping using transvaginal power Doppler sonography in women with postmenopausal bleeding and thickened endometrium. Ultrasound Obstet Gynecol. 2003;21:583–588. doi: 10.1002/uog.143. [DOI] [PubMed] [Google Scholar]
- 14.Van Den Bosch T, Verbakel JY, Valentin L, et al. Typical ultrasound features of various endometrial pathologies described using international endometrial tumor analysis (IETA) terminology in women with abnormal uterine bleeding. Ultrasound Obstet Gynecol. 2021;57(1):164–172. doi: 10.1002/uog.22109. [DOI] [PubMed] [Google Scholar]
- 15.Sladkevicius P, Installé A, Van Den Bosch T, et al. International endometrial tumor analysis (IETA) terminology in women with postmenopausal bleeding and sonographic endometrial thickness ≥ 4.5 mm: agreement and reliability study. Ultrasound Obstet Gynecol. 2018;51(2):259–268. doi: 10.1002/uog.18813. [DOI] [PubMed] [Google Scholar]
- 16.Furau AM, Toma MM, Ionescu C, et al. The correlation of the IETA ultrasound score with the histopathology results for women with abnormal bleeding in western Romania. Diagnostics (Basel) 2021;11(8):1342. doi: 10.3390/diagnostics11081342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Leone FP, Timmerman D, Bourne T, Valentin L, Epstein E, Goldstein SR, Marret H, Parsons AK, Gull B, Istre O, Sepulveda W, Ferrazzi E, Van den Bosch T. Terms, definitions and measurements to describe the sonographic features of the endometrium and intrauterine lesions: a consensus opinion from the International Endometrial Tumor Analysis (IETA) group. Ultrasound Obstet Gynecol. 2010;35(1):103–112. doi: 10.1002/uog.7487. [DOI] [PubMed] [Google Scholar]
- 18.Ashour ASA, Fawzy T, Faisal M. The relationship between transvaginal ultrasound endometrial thickness and body mass index and endometrial pathology in women with postmenopausal bleeding. Med J Cairo Univ. 2017;85(5):2017–2023. [Google Scholar]
- 19.Madkour NM (2017) An ultrasound risk-scoring model for prediction of endometrial cancer in post-menopausal women (using IETA terminology). Middle East Fertil Soc J 1–5
- 20.Razik MA, Walid A, Maksoud MA. Transvaginal and color doppler ultrasound assessment of endometrial pathology in patients with postmenopausal bleeding. Egypt Soc Gynaecol Obstet. 2012;38(2):709–714. [Google Scholar]
- 21.Talaat S, Mostafa N, Alrauof MA. Diagnostic value of ultrasound and colour Doppler in endometrial and cervical polyps. Med J Cairo Univ. 2009;77(1):397–403. [Google Scholar]
- 22.Cil AP, Tulunay G, Kose MF, Haberal A. Power Doppler properties of endometrial polyps and submucosal fibroids: a preliminary observational study in women with known intracavitary lesions. Ultrasound Obstet Gynecol. 2010;35(2):233–237. doi: 10.1002/uog.7470. [DOI] [PubMed] [Google Scholar]
- 23.Badawy AM, Abu-Elata M. Can colour Doppler ultrasonography predict the prognosis of endometrial hyperplasia? J Obstet Gynaecol. 2003;23(3):282–284. doi: 10.1080/01443610310000100105. [DOI] [PubMed] [Google Scholar]
- 24.Azmy OM. Haitham B (2014) Ultrasound imaging of endometrial cancer, gynecologic neoplasia. In: Rizk BRMB, Puscheck EE, editors. Ultrasonography in gynecology. Cambridge: Cambridge University Press; 2014. pp. 224–232. [Google Scholar]
- 25.AbdelMaboud NM, Elsaid HH. Role of transvaginal ultrasonography and colour Doppler in the evaluation of postmenopausal bleeding. Egypt J Radiol Nucl Med. 2015;46(1):235–243. doi: 10.1016/j.ejrnm.2014.11.014. [DOI] [Google Scholar]
- 26.Li Z, Li L. Risk of malignancies among asymptomatic postmenopausal women with thickened endometrium: a cohort study. Medicine. 2019;98(6):e14464. doi: 10.1097/MD.0000000000014464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.El Kady SR, Abd El Fatah AT, Mohamed IH, Salem SM. Correlation between endometrial histopathology in postmenopausal uterine bleeding and transvaginal colour doppler. AIMJ. 2020;1(12):249–52. [Google Scholar]
- 28.Amreena S, Singha M, Choh NA, Saldanhab C, Gojwaria TA. Doppler evaluation of endometrial polyps. Egypt J Radiol Nucl Med. 2018;49:850–853. doi: 10.1016/j.ejrnm.2018.03.005. [DOI] [Google Scholar]
- 29.Perez-Medina T, Bajo J, Huertas MA, Rubio A. Predicting atypia inside endometrial polyps. J Ultrasound Med. 2002;21(2):125–128. doi: 10.7863/jum.2002.21.2.125. [DOI] [PubMed] [Google Scholar]
- 30.Liu MJ, Liu ZF, Yin WH, Chen XR, Gao LY, Sun HJ. Application of transvaginal three-dimensional power Doppler ultrasound in benign and malignant endometrial diseases. Medicine (Baltimore) 2019;98(46):e17965. doi: 10.1097/MD.0000000000017965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Nguyen PN, Nguyen VT (2022) Value of endometrial thickness and Doppler parameters of uterine artery in predicting endometrial cancer in postmenopausal women with abnormal uterine bleeding: a cross-sectional study in Vietnam [published online ahead of print, 2022 Apr 29]. Obstet Gynecol Sci 10.5468/ogs.22053 [DOI] [PMC free article] [PubMed]
- 32.Grigore M, Popovici R, Himiniuc LM, et al. The added value of three-dimensional ultrasonography in uterine pathology. Exp Ther Med. 2021;22(5):1261. doi: 10.3892/etm.2021.10696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hanafi S, Abou-Gabal A, Akl S, El Baset HA. Value of three dimensional power Doppler ultrasound in prediction of endometrial carcinoma in patients with postmenopausal bleeding. J Turk Ger Gynecol Assoc. 2014;15(2):78–81. doi: 10.5152/jtgga.2014.07355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Wynants L, Verbakel JYJ, Valentin L, De Cock B, Pascual MA, Leone FPG, et al. The risk of endometrial malignancy and other endometrial pathology in women with abnormal uterine bleeding: an ultrasound-based model development study by the IETA group. Gynecol Obstet Invest. 2022;87(1):54–61. doi: 10.1159/000522524. [DOI] [PubMed] [Google Scholar]
- 35.Madkour NM. An ultrasound risk-scoring model for prediction of endometrial cancer in post-menopausal women (using IETA terminology) Middle East Fertil Soc J. 2017;22(3):201–205. doi: 10.1016/j.mefs.2017.01.009. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.