

Key Clinical Message
Although one of the most important differential diagnoses of cardiac masses in cancer patients is metastasis from the underlying tumor, it may also be caused by benign etiologies. In this article, we describe cardiac calcified amorphous tumor, which is one of the benign causes of cardiac masses, in a patient with colon cancer.
Keywords: calcified amorphous tumor, cardiac mass, colon cancer
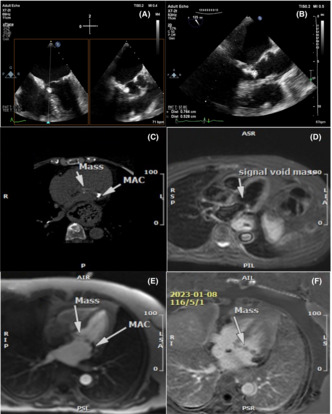
Multimodality imaging using transesophageal echocardiography (TEE), cardiac computed tomography (CT), and cardiac magnetic resonance imaging (CMR). TEE demonstrating a pedunculated mobile calcified mass (0.7 × 0.5 cm) attached to posterior of mitral valve (MV) annulus (A and B). Cardiac CT demonstrating mitral annular calcification (MAC) and calcified mass attached to MV annulus (C). CMR demonstrating the mass with low signal intensity on T2‐weighted images (D), with no perfusion in the first pass perfusion sequences (E) and no enhancement in the late‐enhancement sequences (F).
1. CASE PRESENTATION
A 80‐year‐old woman with a history of colon cancer who was treated by chemotherapy agents (Cyclophosphamide, Vincristine, Doxorubicin) until last year was admitted due to incidental mitral valve (MV) mass found on transthoracic echocardiography (TTE). The patient did not complain of fever, dyspnea, syncope, or chest pain.
On admission, vital signs were stable. Clinical examination revealed regular cardiac rhythm and no cardiac murmur. Pulmonary auscultation was normal. The peripheral pulses were normal, and there were no skin lesions.
Twelve‐lead electrocardiogram showed sinus rhythm and low QRS voltage in limb leads. Basic hematological and biochemical tests were unremarkable. Blood culture was also negative.
Transesophageal echocardiography (TEE) was performed and revealed mild left ventricle systolic dysfunction (left ventricle ejection fraction: 50%–55%), thick and calcified MV with severe anterior and posterior mitral annular calcification (MAC), mild to moderate mitral regurgitation and pedunculated mobile mass (0.7 × 0.5 cm) attached to posterior of MV annulus in favor of metastatic tumor from the colon, calcified amorphous tumor (CAT), clot, vegetation, or primary cardiac tumors (Figure 1A,B). CAT was confirmed by cardiac magnetic resonance imaging (CMR) and cardiac computed tomography (CT):
An irregular pedunculated semi‐motion calcified mass attached to MV annulus (0.7 × 0.5 cm) was seen.
In the T2‐weighted short‐tau inversion recovery (T2w‐STIR) sequences, the mass is low signal intensity.
In the T1‐weighted sequences with fat suppression images, the mass is low signal intensity.
In the first pass perfusion sequences, the mass has no perfusion.
In the early‐enhancement sequences, the mass has no enchantment.
In the late‐enhancement sequences, the mass has no enhancement (Figure 1C,D).
FIGURE 1.
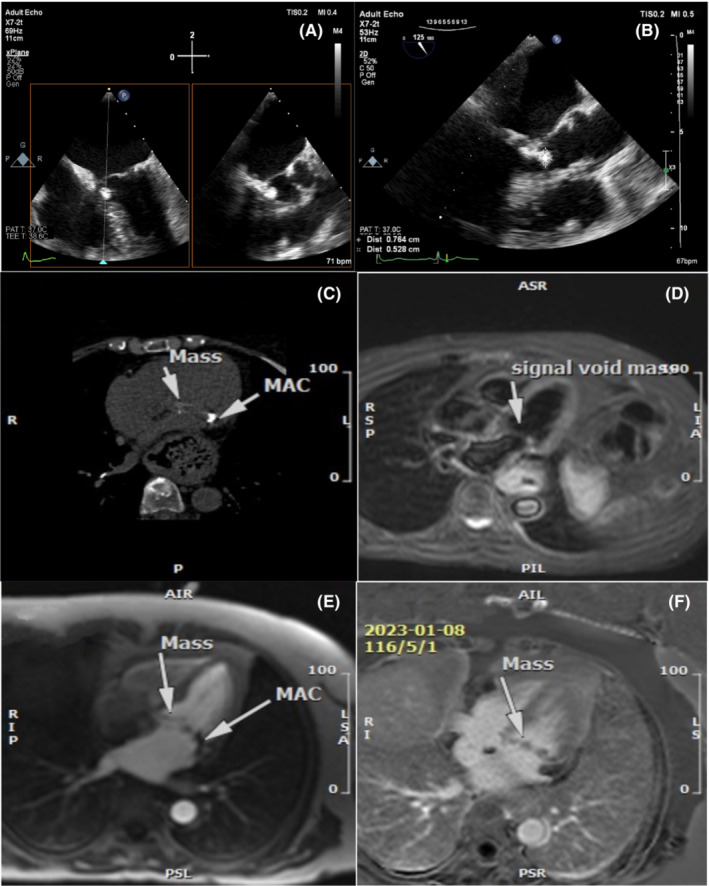
Multimodality imaging using transesophageal echocardiography (TEE), cardiac computed tomography (CT), and cardiac magnetic resonance imaging (CMR). TEE demonstrating a pedunculated mobile calcified mass (0.7 × 0.5 cm) attached to posterior of mitral valve (MV) annulus (A and B). Cardiac CT demonstrating mitral annular calcification (MAC) and calcified mass attached to MV annulus (C). CMR demonstrating the mass with low signal intensity on T2‐weighted images (D), with no perfusion in the first pass perfusion sequences (E) and no enhancement in the late‐enhancement sequences (F).
Due to the old age of the patient and history of colon cancer, he was not a suitable candidate for surgery and the decision was made to follow‐up the patient with imaging.
2. DISCUSSION
CAT is a rare non‐neoplastic intracardiac mass, which is composed of calcium deposition and amorphous fibrinous material. It was first described in 1997 by Reynolds. CAT can be asymptomatic or symptomatic.
In symptomatic cases, symptoms are related to embolization or occlusion. The most common symptoms were dyspnea, embolic event, syncope, and chest pain. 1
A definitive diagnosis of cardiac CAT is based on histologic examination that also rules out infective vegetation, myxoma and papillary fibroelastoma. It is difficult to differentiate a mobile cardiac tumor by echocardiography. In histopathological examination, CAT composed of nodular calcium deposits surrounded by an amorphous hyalinized material. 1
CMR can also be helpful in diagnosing this lesion. CAT show low signal intensity on T1 and T2‐weighted images with no contrast enhancement on CMR. 2 Given that these cardiac tumors can be a source of embolism, surgical resection should probably be considered. 1
AUTHOR CONTRIBUTIONS
Azin Alizadehasl: Conceptualization; data curation; supervision; writing – review and editing. Mohammadreza Iranian: Conceptualization; data curation; supervision; writing – original draft; writing – review and editing. Kiara Rezaei‐Kalantari: Data curation; writing – review and editing. Farzaneh Sepehr: Data curation; writing – original draft; writing – review and editing. Somaye Mohebi: Data curation; writing – review and editing. Mahsa Mohammadi: Data curation; writing – review and editing.
FUNDING INFORMATION
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
CONFLICT OF INTEREST STATEMENT
The authors declare that they have no conflict of interest.
CONSENT TO PARTICIPATE
Written informed consent was obtained from the patient to publish this report in accordance with the patient consent policy of the Clinical Case Reports journal.
Alizadehasl A, Iranian M, Rezaei‐Kalantari K, Sepehr F, Mohebi S, Mohammadi M. Cardiac calcified amorphous tumor in a patient with colon cancer. Clin Case Rep. 2023;11:e7491. doi: 10.1002/ccr3.7491
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- 1. de Hemptinne Q, de Cannière D, Vandenbossche JL, Unger P. Cardiac calcified amorphous tumor: a systematic review of the literature. Int J Cardiol Heart Vasc. 2015;7:1‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Yılmaz R, Demir AA, Önür İ, Yılbazbayhan D, Dursun M. Cardiac calcified amorphous tumors: CT and MRI findings. Diagn Interv Radiol. 2016;22(6):519‐524. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.