

Abstract
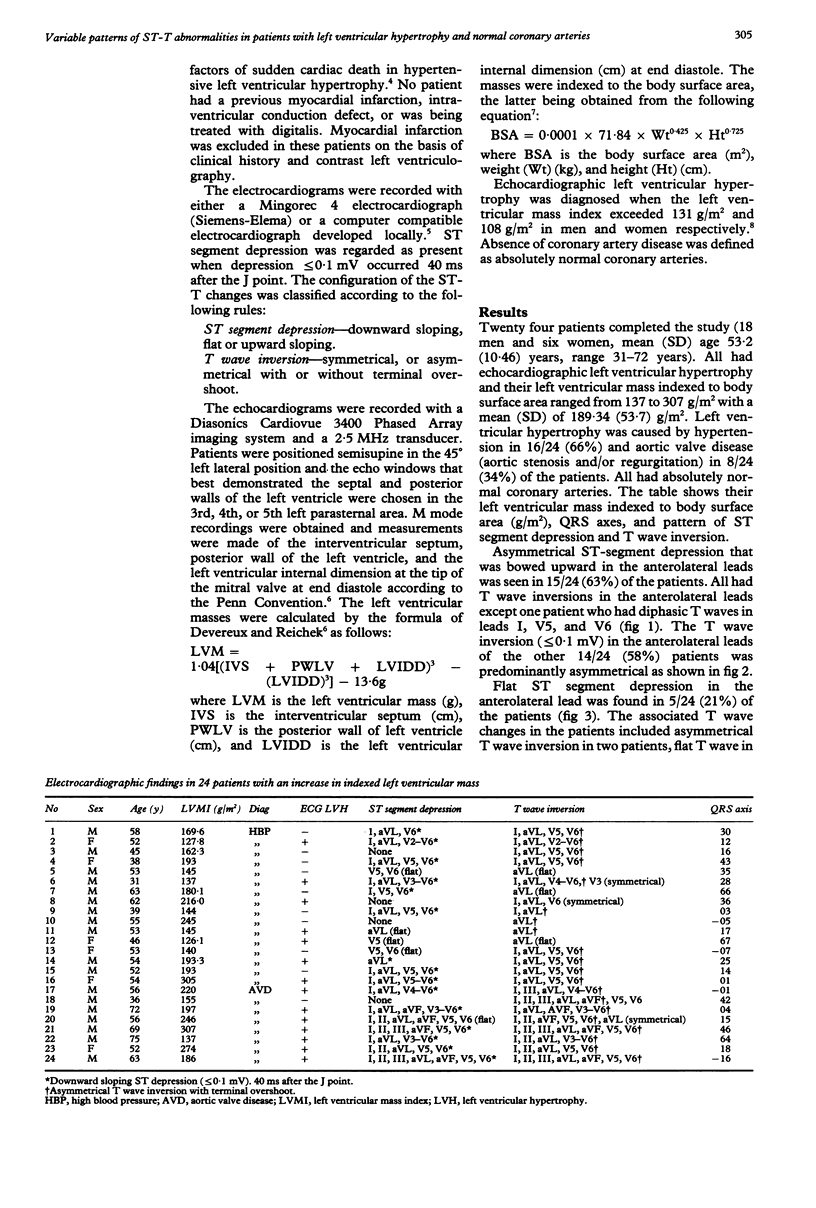
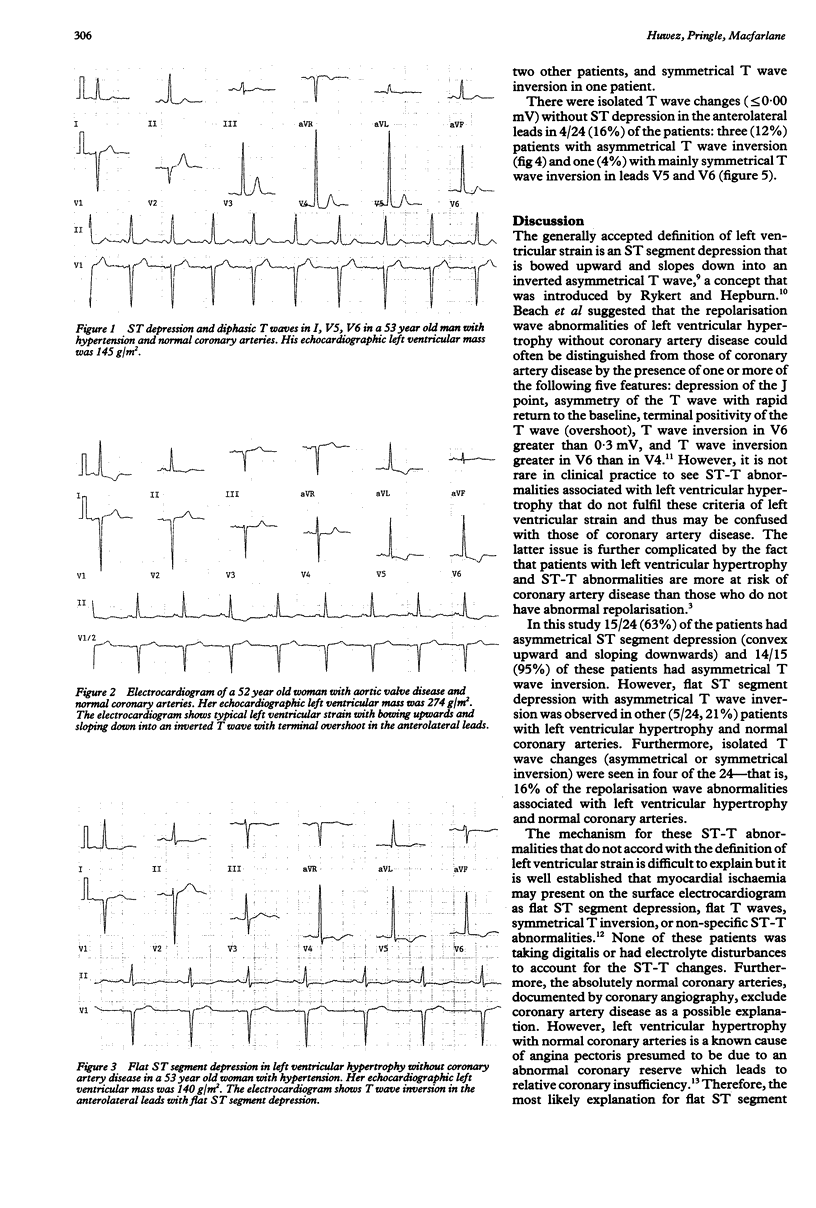
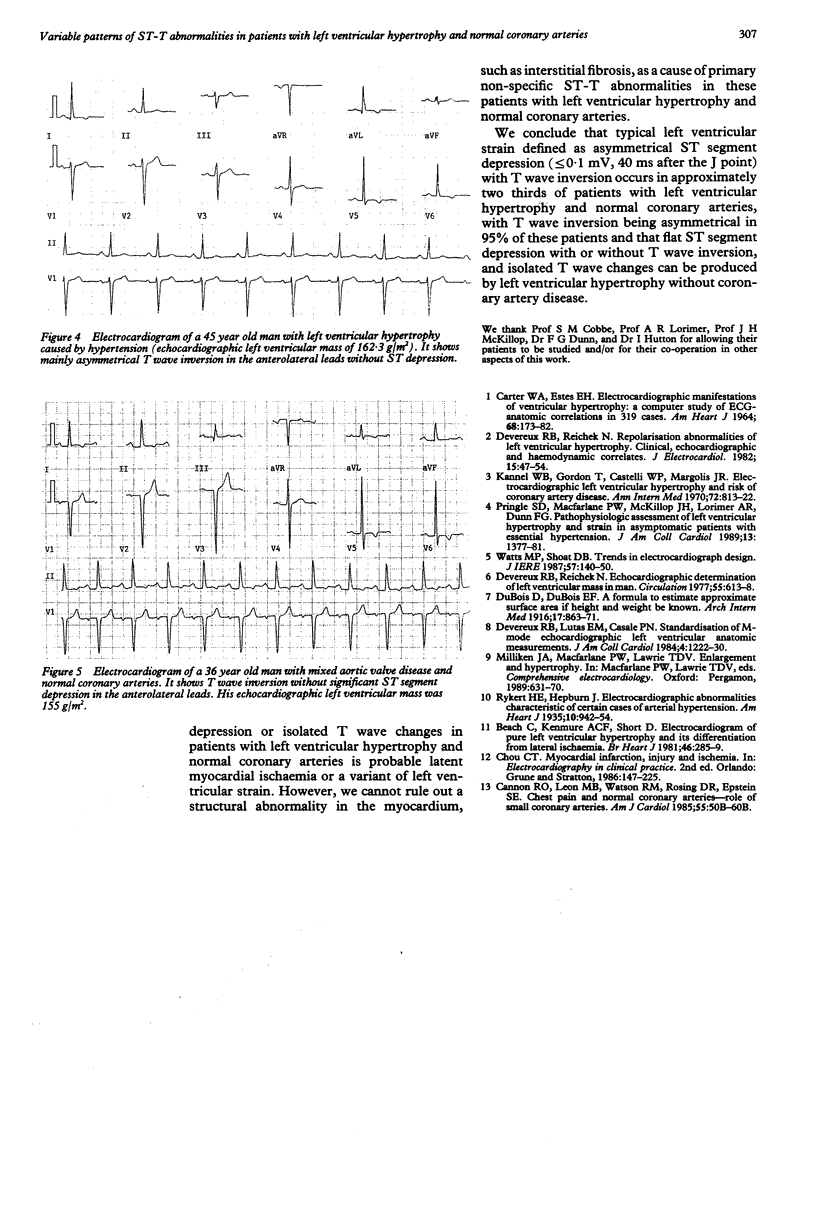
BACKGROUND--Classically, the ST-T configuration in the electrocardiogram of patients with left ventricular hypertrophy is said to have a typical pattern of ST depression together with asymmetrical T wave inversion (the so-called left ventricular strain pattern). However, many patients with left ventricular hypertrophy may also have ischaemic heart disease. To revise the electrocardiographic criteria for left ventricular hypertrophy the ST-T configuration in patients with left ventricular hypertrophy documented by echocardiography and with normal coronary arteries was assessed. METHODS--24 patients were selected for this study. All had left ventricular hypertrophy documented by echocardiography, normal coronary arteries by cardiac catheterisation, and ST and/or T wave abnormalities in the lateral leads of their electrocardiogram. There were eight patients with aortic valve disease and 16 with hypertension who had coronary angiography as part of an investigation into the risk factors of sudden cardiac death caused by hypertensive left ventricular hypertrophy. No patient was receiving digitalis preparations or had electrolyte disturbances, and none had a previous myocardial infarction or ventricular conduction defect. RESULTS--Typical electrocardiographic evidence of left ventricular strain was found in approximately two thirds (63%) of patients and 95% of this subgroup had asymmetrical T wave inversion. Flat ST segment depression, with or without T wave inversion or isolated T wave inversion (symmetrical or asymmetrical) in the anterolateral leads, was seen in the remaining 37% of patients. CONCLUSIONS--These findings indicate that left ventricular hypertrophy without coronary artery disease can cause variable types of ST-T abnormalities in the anterolateral leads including the typical left ventricular strain pattern and non-specific ST-T changes. Non-specific abnormalities could not be distinguished from those of coronary artery disease and may adversely affect the accuracy of the electrocardiographic criteria for the diagnosis of left ventricular hypertrophy because they do not accord with the criteria for left ventricular strain.
Full text
PDF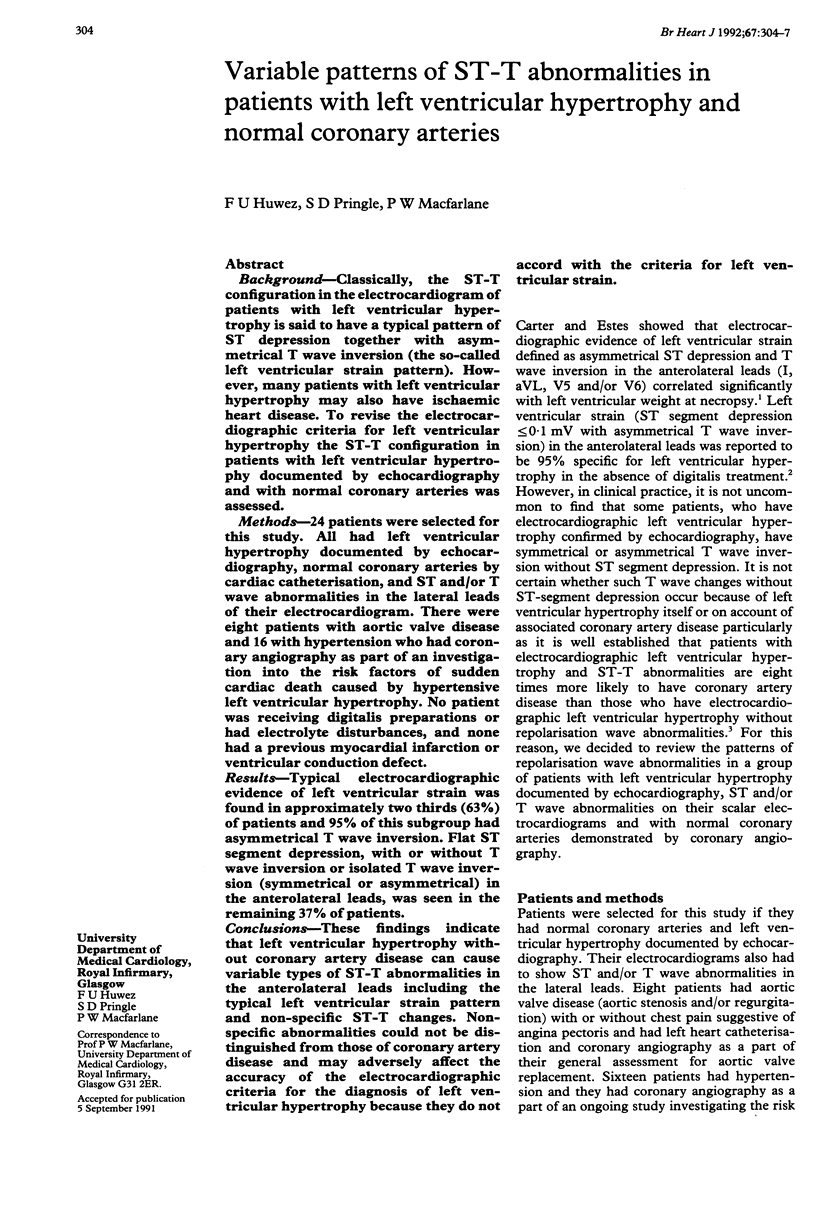
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Beach C., Kenmure A. C., Short D. Electrocardiogram of pure left ventricular hypertrophy and its differentiation from lateral ischaemia. Br Heart J. 1981 Sep;46(3):285–289. doi: 10.1136/hrt.46.3.285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- CARTER W. A., ESTES E. H., Jr ELECTROCARDIOGRAPHIC MANIFESTATIONS OF VENTRICULAR HYPERTROPHY; A COMPUTER STUDY OF ECG-ANATOMIC CORRELATIONS IN 319 CASES. Am Heart J. 1964 Aug;68:173–182. doi: 10.1016/0002-8703(64)90038-9. [DOI] [PubMed] [Google Scholar]
- Devereux R. B., Lutas E. M., Casale P. N., Kligfield P., Eisenberg R. R., Hammond I. W., Miller D. H., Reis G., Alderman M. H., Laragh J. H. Standardization of M-mode echocardiographic left ventricular anatomic measurements. J Am Coll Cardiol. 1984 Dec;4(6):1222–1230. doi: 10.1016/s0735-1097(84)80141-2. [DOI] [PubMed] [Google Scholar]
- Devereux R. B., Reichek N. Echocardiographic determination of left ventricular mass in man. Anatomic validation of the method. Circulation. 1977 Apr;55(4):613–618. doi: 10.1161/01.cir.55.4.613. [DOI] [PubMed] [Google Scholar]
- Devereux R. B., Reichek N. Repolarization abnormalities of left ventricular hypertrophy. Clinical, echocardiographic and hemodynamic correlates. J Electrocardiol. 1982 Jan;15(1):47–53. doi: 10.1016/s0022-0736(82)80044-7. [DOI] [PubMed] [Google Scholar]
- Kannel W. B., Gordon T., Castelli W. P., Margolis J. R. Electrocardiographic left ventricular hypertrophy and risk of coronary heart disease. The Framingham study. Ann Intern Med. 1970 Jun;72(6):813–822. doi: 10.7326/0003-4819-72-6-813. [DOI] [PubMed] [Google Scholar]
- Pringle S. D., Macfarlane P. W., McKillop J. H., Lorimer A. R., Dunn F. G. Pathophysiologic assessment of left ventricular hypertrophy and strain in asymptomatic patients with essential hypertension. J Am Coll Cardiol. 1989 May;13(6):1377–1381. doi: 10.1016/0735-1097(89)90314-8. [DOI] [PubMed] [Google Scholar]