

ABSTRACT
Background and Aims:
Modified radical mastectomy (MRM) is associated with significant postoperative pain for which many blocks including thoracic paravertebral (TPV) block are being used. Erector spinae plane (ESP) block is a recently described technique. We planned to compare the efficacy and safety of ultrasound-guided continuous ESP and TPV blocks for postoperative analgaesia following MRM.
Methods:
Sixty-six patients belonging to American Society of Anaesthesiologists physical status I and II, aged 25–85 years, undergoing MRM were enrolled and randomly allocated into two groups. Ipsilateral block was given preoperatively at T3 or T4 level with 20 ml of 0.5% ropivacaine and 50 μg fentanyl. Infusion of 0.5% and 0.2% ropivacaine with fentanyl 2 μg/ml at a rate of 5 ml/hr was continued during intraoperative and postoperative period, respectively. Pain was assessed using visual analogue scale (VAS) till 24 hours. Block performance time, time to first rescue analgaesia, total amount of rescue analgaesic consumed, the incidence of procedure-related and postoperative complications, failure rate and patient satisfaction score were also recorded. Data collected were analysed using the Chi-square test or Student’s t-test with the help of SPSS 22.0.
Results:
Demographics, baseline vitals, VAS scores both at rest and on movement, block performance time, time to first rescue analgaesia, the total amount of rescue analgaesia and patient satisfaction score were comparable in both groups (P value > 0.05). No complications were observed in either group.
Conclusion:
In patients undergoing MRM, continuous catheter technique ESP block is as efficacious and safe as TPV block for providing prolonged postoperative analgaesia.
Keywords: Anaesthetics, analgaesics, local, mastectomy, modified radical, nerve block, opioid, pain, postoperative, visual analogue scale
INTRODUCTION
Modified radical mastectomy (MRM) is a commonly performed surgery for breast cancer, the most common malignancy occurring in Indian females.[1] Following MRM, the severity of postoperative acute pain and the perioperative anaesthesia/analgaesia techniques used have shown to affect the development of chronic pain (55% patients) and cancer recurrence with inadequate pain control as an independent predictor.[2,3] Both opioids and non-opioids analgaesics have been used for management of acute pain, but each has its inherent side effects and limitations. Regional nerve blocks during cancer surgeries have been reported to cause reduction of cancer progression by attenuating surgical stress response, improved analgaesia and reduced opioid consumption. This has prompted anaesthesiologists world over to adopt various regional anaesthesia techniques like thoracic epidural analgaesia (TEA), pectoral nerve blocks (PEC I and II), serratus anterior plane block (SAP), thoracic paravertebral block (TPVB), erector spinae plane block (ESPB) and pecto-intercostal fascial block for MRM.[4-8] TEA is considered to be the most effective, but the requirement of the unilateral block has allowed the TPVB to become popular. Recently, ESPB has been suggested as a new, less invasive alternative to both TEA and TPVB, for surgical and postoperative analgaesia in MRM.[7]
The present study prospectively compared continuous ESPB with TPVB for their safety and efficacy in providing postoperative analgaesia following MRM. We hypothesised that ESPB is not inferior to the TPVB with regard to postoperative analgaesia and safety. The primary objective was to compare postoperative analgaesia in both the groups using visual analogue scale (VAS) for 24 hours, and secondary objectives were to compare time to first rescue analgaesic, its total amount used, block performance time, the incidence of procedure-related and postoperative complications, failure rate and patient satisfaction between groups.
METHODS
The present study was conducted at a tertiary care institute in India after getting institutional ethics committee approval (vide registration number AIIMS/IEC/2018-1055 dated 08-03-2018) and clinical trial registration [Registered with Clinical trials registry- India (http://www.ctri.nic.in), Reg. No.: CTRI/2018/05/013961]. Informed and written consent was obtained from all enrolled patients for participation in the study and use of the patient data for research and educational purposes. The study was carried out in accordance with the principles of the Declaration of Helsinki, 2013. Sixty-six patients belonging to the American Society of Anaesthesiologists (ASA) physical status I and II, aged between 25 and 85 years and scheduled to undergo MRM, were enrolled. Patient’s refusal, pregnancy, repeat surgery, pre-existing infection at block site, coagulation disorder, preoperative hypotension (mean arterial BP <50 mmHg), bradycardia (heart rate <45 beats/min), dysrhythmia, psychiatric illness, pre-existing neurological deficits, morbid obesity [Body Mass Index (BMI) >40 kg/m2], decreased pulmonary reserve, cardiac disorders, renal dysfunctions, known allergy to study drugs, fungating growth, chronic pain and regular analgaesic use were exercised as exclusion criteria.
All patients were examined during the preoperative visit by the attending anaesthesiologist. Routine investigations were done as per requirement. Patients were made well conversant with the VAS score.
Patients were randomly allocated into two groups (group A-TPVB and group B-ESPB) using computer-generated random numbers. The group allocation numbers were concealed in sealed opaque envelopes that were opened just before the performance of the block. Blocks were administered at T3 or T4 levels on the operative side. The patient and the anaesthesiologist involved in the data collection were not aware of the group allocation, while the anaesthesiologist performing the block was not involved in the further care of the patient.
In the operating room, routine monitoring comprising continuous ECG, peripheral oxygen saturation monitor (SpO2) and non-invasive blood pressure (NIBP) were attached. Screening ultrasound (parasagittal scan) using high-frequency (8–15 MHz) linear transducer of machine (‘LOGIQ e’, GE Healthcare, Chicago, United States) was done with patient in sitting position. The structures identified were superior costotransverse ligament (SCTL) and pleura in group A and trapezius, rhomboid major and erector spinae muscles superficial to the hyperechoic transverse process shadow in group B. Under all aseptic precautions, a 22-gauge, 10-cm echogenic needle (Contiplex D, B. Braun Melsungen, Germany) was inserted using in-plane technique and 20 ml, 0.5% ropivacaine with 50 μg fentanyl was injected anterior to the SCTL ligament in group A and posterior to the transverse process in group B followed by catheter size 24-gauge (Contiplex D, B. Braun Melsungen, Germany), insertion 3–4 cm distal to the needle tip. All the blocks were performed by anaesthesiologists having minimum three years of experience in anaesthesia and nerve blocks, not involved in the preoperative or postoperative assessment of patients, anaesthesia management and data collection. The chief investigator, medical and nursing personnel and the patients were blinded.
Following the block, general anaesthesia was induced using standard technique, and airway was secured with i-gel or endotracheal tube and maintained with sevoflurane (1.5–2.5%) in oxygen and air (40:60) mixture. Throughout the intraoperative period in both groups, 0.5% ropivacaine with fentanyl 2 μg/ml at 5 ml/h was infused through catheter. At the end of the surgery, patients were extubated after satisfying the criteria and were shifted to postanaesthesia care unit (PACU) and further to ward and monitored for 24 h after surgery.
Infusion of 0.2% ropivacaine with fentanyl 2 μg/ml was started in both groups. Postoperative pain was assessed using VAS at every hour till 4h and then every 4h till 24 hours. Pain on movement was assessed by asking the patient to lift the arm till shoulder level. An immediate postoperative VAS score ≥4 was considered a block failure. However, the infusion was continued, and the data from that patient was included in the final analysis in an attempt to intention to treat analysis. Rescue analgaesia in the form of IV paracetamol (PCM) 20 mg/kg (maximum 1 gm) was given if VAS score ≥4 was recorded at rest or during movement at any point of time during the postoperative period. The patient was again evaluated after 30 min of PCM administration, and in case of no response, IV tramadol 2 mg/kg in 100 ml normal saline over 30 minutes was administered. No round-the-clock analgaesia was provided to the patient. Block performance time (time elapsed between putting the USG probe on the patient after cleaning, draping and probe preparation and real-time confirmation of the correct catheter position by injecting saline through it), time to first rescue analgaesia (time between the end of the local anaesthetic bolus injection and administration of first rescue analgaesic), the total amount of analgaesics used in 24 hours postoperatively, procedure-related complications (pneumothorax, vascular or neural injury, Horner’s syndrome, etc.), postoperative complications (hypotension, respiratory depression, postoperative nausea and vomiting (PONV), shivering, headache, dizziness, constipation, urinary retention, pruritus) and failure rate were also recorded. At 24 hours after surgery, the satisfaction of the patients was assessed using a numerical satisfaction score as 4 = excellent, 3 = good, 2 = fair and 1 = poor.
This study was non-inferiority trial. The objective was to show that the ESPB is not inferior to TPV block in terms of analgaesic efficacy. The primary endpoint was pain measured on a VAS scale. The non-inferiority limit was two. The sample size of 33 patients in each group was required with an anticipated standard deviation of 2.5; assuming a one-sided type I error of 2.5% and 90% power, and true mean difference between the treatments was zero. The non-inferiority margin of two was selected based on the critical appraisal of the published literature on TPVB.[9] The average pain score during 24-hour postoperative period was two in patients receiving TPVB. A VAS score of ≤4 was taken as adequate analgaesia. So, the non-inferiority of ESP could be established if the patient receiving ESPB would have VAS ≤4. The difference of average VAS score between TPVB and the upper limit of VAS for adequate analgaesia was taken as non-inferiority margin.
Data collected was analysed using SPSS IBM software version 22 (IBM SPSS Advanced Statistics, Chicago, IL, USA). Results of the categorical measurements were presented in numbers or ratio, and of quantitative variables were presented as median (range) or mean (SD). Chi-square test was applied for comparing qualitative data, and unpaired Student’s t-test using Bonferroni multiple comparisons’ test for comparing quantitative data. Time to first analgaesic administration was analysed by Kaplan–Meier survival analysis and log-rank test. P value < 0.025 was considered significant.
RESULTS
A total of 83 patients were assessed for eligibility, of which 66 were randomised into two groups and received the allocated intervention [Figure 1]. We performed an intention to treat analysis, i.e. the data from patients with failed block was included in the final analysis. Both groups were comparable with respect to age, ASA status, height, weight, BMI, baseline vitals (HR, MAP and SpO2), block performance time and duration of surgery [Table 1].
Figure 1.
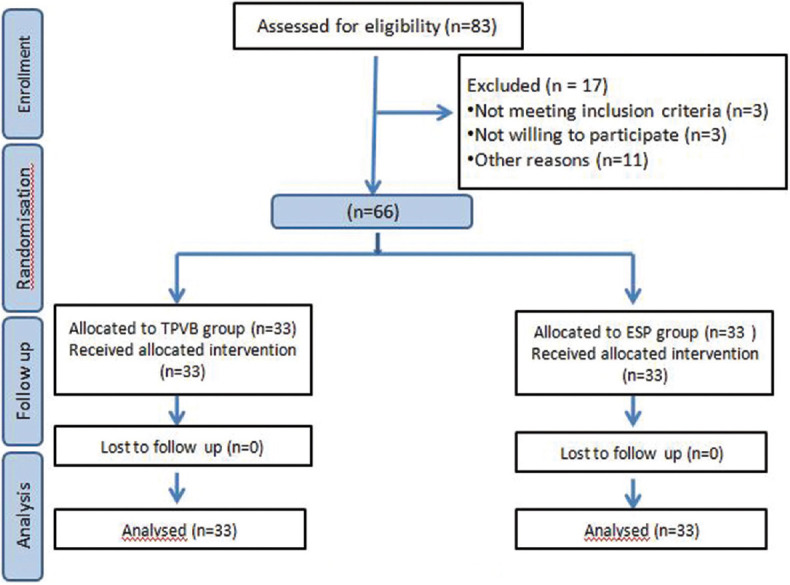
CONSORT diagram
Table 1.
Comparison of demographics, baseline vitals, block performance time and duration of surgery between groups
| Demographics | Group A (n=33) | Group B (n=33) | P |
|---|---|---|---|
| Age (years) | 50.76±10.24 | 49.09±11.90 | 0.54 |
| ASA‡ (I/II) | 25/8 | 23/10 | 0.58 |
| Height (cm) | 152.14±4.78 | 152.68±5.64 | 0.67 |
| Weight (kg) | 61.89±12.22 | 59.94±10.76 | 0.49 |
| BMI (kg/m2) | 26.19±6.58 | 25.71±4.37 | 0.73 |
| Heart rate (per minute) | 83.79±12.99 | 82.58±15.9 | 0.74 |
| Mean blood pressure (mmHg) | 102.6±8.19 | 98.32±8.53 | 0.06 |
| SpO2 (%) | 98.97±1.01 | 99.39±0.75 | 0.09 |
| Block performance time (min) | 22.36±7.01 | 19.39±5.96 | 0.054 |
| Duration of surgery (minutes) | 161.45±33.97 | 155.06±38.26 | 0.48 |
Values are presented as mean±SD. ‡Values presented as number.
The median (IQR) (range) of VAS scores at rest and during movement was comparable between groups at all points of observation [Table 2, Figure 2]. Total six patients required rescue analgaesia in group A, out of which four patients required rescue analgaesia at 1st hour while the other two required it within first 4 hours postoperatively [Table 3]. In group B, five patients required rescue analgaesia, out of which four required at 1st hour and one patient required it within the first 4 hours postoperatively. Time to first rescue analgaesia was also compared using Kaplan–Meier analysis and log-rank test which showed no significant difference in time to first rescue analgaesia between the two groups [Chi-square 0.005 by log-rank (Mantel–Cox); P = 0.95] [Figure 3]. In group A, total rescue analgaesia consumed during the observation period was 14 gm while in group B was it 13 gm [Table 3]. Four patients in each group had VAS score ≥4 at first assessment and were considered as block failure.
Table 2.
Comparison of VAS scores at rest and movement between study groups
| Time (h) | VAS at rest | Median Diff (95% CI) | P | VAS during movement | Median Diff (95% CI) | P | ||
|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||
| Group A (n=33) | Group B (n=33) | Group A (n=33) | Group B (n=33) | |||||
| 1 | 1 (1,1) (1-4) | 1 (1,2) (1-5) | 0, -0.5-0.32 | 0.514 | 2 (1,2.75) (1-5) | 2 (1,3) (1-6) | 0, -0.8-0.4 | 0.431 |
| 2 | 1 (1,2) (1-4) | 1 (1,1) (1-3) | 0, -0.1-0.5 | 0.227 | 2 (1,3) (1-5) | 2 (1,2) (1-4) | 0, -0.4-0.7 | 0.849 |
| 3 | 1 (1,1) (1-3) | 1 (1-3) | 0, -0.16-0.4 | 0.484 | 1.5 (1,2) (1-4) | 1 (1,2) (1-4) | 0.5, -0.26-0.63 | 0.509 |
| 4 | 1 (1,1) (1-4) | 1 (1,1) (1-3) | 0, -0.17-0.41 | 0.503 | 1.5 (1,2) (1-5) | 1 (1,2) (1-5) | 0.5, -0.2-0.7 | 0.297 |
| 8 | 1 (1,1) (1-5) | 1 (1,1) (1-2) | 0, -0.22-0.29 | 0.526 | 1 (1,2) (1-5) | 1 (1,1.75) (1-3) | 0, -0.4-0.47 | 0.939 |
| 12 | 1 (1,1) (1-3) | 1 (1,1) (1-2) | 0, -0.1-0.34 | 0.586 | 1 (1,1.75) (1-4) | 1 (1,1) (1-3) | 0, -0.23-0.54 | 0.851 |
| 16 | 1 (1,1) (1-3) | 1 (1,1) (1-3) | 0, -0.21-0.39 | 0.079 | 2 (2,2) (2-4) | 2 (2,2) (2-4) | 0, -0.21-0.39 | 0.079 |
| 20 | 1 (1,1) (1-3) | 1 (1,1) (1-3) | 0, -0.21-0.39 | 0.079 | 1 (1,1) (1-4) | 1 (1,1) (1-2) | 0, -0.47-0.65 | 0.271 |
| 24 | 1 (1,1) (1-3) | 1 (1,1) (1-3) | 0, -0.21-0.39 | 0.079 | 1 (1,1.75) (1-4) | 1 (1,1) (1-2) | 0, -0.004-0.79 | 0.128 |
Values are presented as median (IQR) (range)
Figure 2.
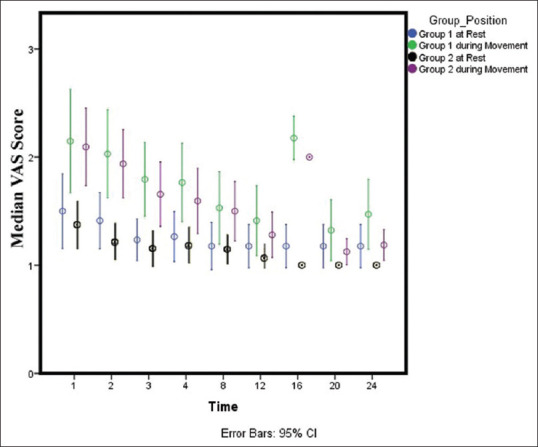
Error bars
Table 3.
Comparison of time to first rescue analgaesia between study groups
| Parameter | Group A | Group B | P |
|---|---|---|---|
| Number of patients requiring rescue analgaesia (%) | 6 (18) | 5 (15) | - |
| Total amount of rescue analgaesic consumed (gm) | 14 | 13 | - |
| Patient satisfaction score [median (range)] | 4 (3-4) | 4 (3-4) | 0.6580 |
Figure 3.
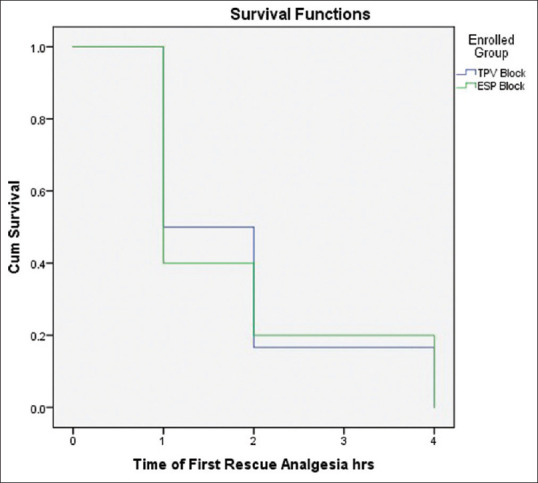
Kaplan–Meier survival analysis
Block performance time for TPV block (22.36 ± 7.01) was higher although not significant compared to ESPB (19.39 ± 5.96) (P value = 0.054). The median (range) satisfaction scores in for both group A and group B were four (3–4) (P value = 0.6580) [Table 3]. No procedure-related or postoperative complications were observed.
DISCUSSION
Our study demonstrated that continuous ESPB is not inferior to continuous TPVB for providing postoperative analgaesia assessed using VAS score in patients undergoing MRM. Also, the performance time of ESPB was comparable to TPVB, and none of the patient receiving blocks had any procedural and perioperative complications. Continuous catheter technique extended the duration of postoperative analgaesia with minimal requirement of additional analgaesics and excellent patient satisfaction.
Forty percent of patients undergoing breast surgery report moderate to severe pain in the immediate postoperative period, which is one of the factors implicated for progression to postmastectomy pain syndrome (PMPS).[10] The term PMPS is used for patients suffering from persistent pain after breast cancer treatment. There is evidence of increased risk of metastasis with postoperative pain, stress and use of morphine.[11] Therefore, regional anaesthesia techniques have found its way in this direction offering multiple benefits, e.g. decreased postoperative nausea vomiting (PONV), decreased length of PACU stay, opioid and volatile anaesthetics sparing effect (both have been found to be associated with immune-suppression and thus the risk of tumour recurrence), increased IL-10 levels (which inhibit the production of pro-inflammatory cytokines and exert antitumor and antimetastatic activity), increased natural killer (NK) cell cytotoxicity (which is critical in antitumor immune response), reduced cancer progression (by attenuation of the surgical stress response, better analgaesia and reduced opioid usage) and by the direct protective action of LA on cancer cells migration.[3,12]
Among regional techniques, TPVB has gained popularity for providing intraoperative and postoperative analgaesia in patients undergoing MRM. However, being in close proximity to the pleura and central neuraxial system and associated serious potential complications like pneumothorax, many anaesthesiologists hesitate to use it. Use of ultrasound has decreased the risk but not eliminate it. In the pursuit to find a safer alternative, interfascial blocks, viz. SAP and pectoral nerve block, came into practice. ESP is one such technique, where the needling path poses no risk to any vital structures, and the endpoint of needling is the transverse process of the vertebra making it safe and easy to perform.
Results of our study are consistent with the similar studies done by El Ghamry et al.[13] and Gürkan Y et al.,[14] and they found no difference in total analgaesic consumption, time to first rescue analgaesia, pain scores and incidence of complication (pneumothorax, nausea and vomiting) between groups. They used a single injection of LA solution without catheter placement. In both studies, patients required additional analgaesics (morphine) in the postoperative period. There was a vast difference in the mean morphine consumption [27.3 ± 2.9 mg in TPV block and 26.7 ± 2.1 mg in ESPB][5.64 ± 4.15 mg in the PVB group and 5.6 ± 3.43 mg in the ESP group] between both studies.[13,14] In our study, catheter placement provided prolonged analgaesia and significantly reduced the requirement of additional analgaesics as only six (18%) patients in TPVB group and five (15%) patient in ESPB group required additional analgaesia, and the total consumption was 14 gm and 13 gm PCM, respectively, while none of the patients required tramadol. Recently, few case reports have highlighted the role of continuous ESPB for postoperative analgaesia in patients undergoing MRM and found that it provided excellent analgaesia without the need of additional analgaesic.[15,16] To the best of our knowledge, there has been no RCT in MRM patients where the continuous catheter technique was used to compare TPVB and ESPB performed under USG guidance, thereby totally eliminating the use of opioids for postoperative analgaesia.
In our study, failed block was defined as a recording of VAS ≥ four in the immediate postoperative period, and four (12%) patients in each group had failed block. Moustafa et al.[17] observed a significantly higher success rate for ESPB (100%) compared to TPVB (77.8%) (P = 0.002) when performed by novice anaesthesiologists. We observed that the mean block performance time for TPVB (22.36 ± 7.01) was higher although not significant compared to ESPB (19.39 ± 5.96) P value = 0.054). However, Moustafa et al.[17] observed a significantly lower time to perform the ESPB (4.39 ± 1.2 min) compared to TPVB (8.18 ± 2.42 min) (P value < 0.0001). The additional time taken in our study could be due to the different definition of performance time as well as time taken to thread the catheter.
There are a few limitations of our study. First, the onset of blocks could not be assessed prior to skin incision due to high OR turnover and non-availability of separate block room. In the absence of data for block onset, the success or failure of block could only be assessed after the surgery, and a VAS score of ≥4 in immediate postoperative period is not a standardised method. Even though categorised as block failures, the continued infusion and relief of pain with PCM indicate that the block had some analgaesic effect if not complete. Second, although the use of opioid (fentanyl) as an adjuvant during the bolus drug administration as well as during continuous infusion (intraoperative and postoperative) is not contraindicated, the practice is not backed up by supporting literature. Moreover, a few studies have demonstrated prolonged postoperative analgaesia when fentanyl has been combined with local anaesthetic and epinephrine in TPVB.[18] Third, we could not compare intraoperative analgaesic requirement between the groups. We used standard anaesthesia technique in both groups, and all patients received 2 μg/kg IV fentanyl at induction, continuous infusion of local anaesthetic through the block catheter and 1 gm IV PCM 30 min before the completion of surgery. Fourth, although the sample size was calculated beforehand, we believe that further studies with larger sample size are required to reciprocate the finding of our study.
CONCLUSION
Continuous ESPB is not inferior to TPV block in providing postoperative analgaesia measured in terms of VAS scores in patients who underwent MRM. The continuous catheter technique provided prolonged pain relief observed over 24 hours without the need of postoperative opioid and comparable patient satisfaction.
Financial support and sponsorship
This work was supported by the Department of Anaesthesiology and Critical Care, All India Institute of Medical Sciences, Jodhpur, INDIA.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.ICMR-NCDIR National Cancer Registry Programme estimates 12% increase in cancer cases in the country by 2025, Press Release, ICMR Department of Health Research. https://main.icmr.nic.in/sites/default/files/press_realease_files/ICMR_Press_Release_NCRP_18082020.pdf. [Google Scholar]
- 2.Belfer I, Schreiber KL, Shaffer JR, Shnol H, Blaney K, Morando A, et al. Persistent postmastectomy pain in breast cancer survivors:Analysis of clinical, demographic, and psychosocial factors. J Pain. 2013;14:1185–95. doi: 10.1016/j.jpain.2013.05.002. [DOI] [PubMed] [Google Scholar]
- 3.Heaney A, Buggy DJ. Can anaesthetic and analgesic techniques affect cancer recurrence or metastasis? Br J Anaesth. 2012;109:i17–28. doi: 10.1093/bja/aes421. [DOI] [PubMed] [Google Scholar]
- 4.Sekandarzad MW, van Zundert AA, Lirk PB, Doornebal CW, Hollmann MW. Perioperative anesthesia care and tumor progression. Anesth Analg. 2017;124:1697–708. doi: 10.1213/ANE.0000000000001652. [DOI] [PubMed] [Google Scholar]
- 5.Blanco R, Fajardo M, Maldonado TP. Ultrasound description of Pecs II (modified Pecs I):A novel approach to breast surgery. Rev Esp Anestesiol Reanim. 2012;59:470–5. doi: 10.1016/j.redar.2012.07.003. [DOI] [PubMed] [Google Scholar]
- 6.Blanco R, Parras T, McDonnell JG, Prats-Galino A. Serratus plane block:A novel ultrasound-guided thoracic wall nerve block. Anaesthesia. 2013;68:1107–13. doi: 10.1111/anae.12344. [DOI] [PubMed] [Google Scholar]
- 7.Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block:A novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41:621–7. doi: 10.1097/AAP.0000000000000451. [DOI] [PubMed] [Google Scholar]
- 8.Hong B, Yoon SH, Youn AM, Kim BJ, Song S, Yoon Y. Thoracic interfascial nerve block for breast surgery in a pregnant woman:A case report. Korean J Anesthesiol. 2017;70:209. doi: 10.4097/kjae.2017.70.2.209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Schnabel A, Reichl SU, Kranke P, Pogatzki-Zahn EM, Zahn PK. Efficacy and safety of paravertebral blocks in breast surgery:A meta-analysis of randomized controlled trials. Br J Anaesth. 2010;105:842–52. doi: 10.1093/bja/aeq265. [DOI] [PubMed] [Google Scholar]
- 10.Andersen KG, Duriaud HM, Jensen HE, Kroman N, Kehlet H. Predictive factors for the development of persistent pain after breast cancer surgery. Pain. 2015;156:2413–22. doi: 10.1097/j.pain.0000000000000298. [DOI] [PubMed] [Google Scholar]
- 11.Andersen KG, Kehlet H. Persistent pain after breast cancer treatment:A critical review of risk factors and strategies for prevention. J Pain. 2011;12:725–46. doi: 10.1016/j.jpain.2010.12.005. [DOI] [PubMed] [Google Scholar]
- 12.Brack A, Rittner HL, Stein C. Immunosuppressive effects of opioids—clinical relevance. J Neuroimmune Pharmacol. 2011;6:490–502. doi: 10.1007/s11481-011-9290-7. [DOI] [PubMed] [Google Scholar]
- 13.El Ghamry MR, Amer AF. Role of erector spinae plane block versus paravertebral block in pain control after modified radical mastectomy. A prospective randomised trial. Indian J Anaesth. 2019;63:1008–14. doi: 10.4103/ija.IJA_310_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gürkan Y, Aksu C, Kuş A, Yörükoğlu UH. Erector spinae plane block and thoracic paravertebral block for breast surgery compared to IV-morphine:A randomized controlled trial. J Clin Anesth. 2020;59:84–8. doi: 10.1016/j.jclinane.2019.06.036. [DOI] [PubMed] [Google Scholar]
- 15.Kumar R, Syal R, Kamal M, Sharma RS. Continuous erector spinae plane block in a patient with multiple comorbidities undergoing modified radical mastectomy. Indian J Pain. 2019;33:106. [Google Scholar]
- 16.Thota RS, Mukherjee D. Continuous erector spinae plane block as an anesthetic technique for breast cancer surgery. J Anaesthesiol Clin Pharmacol. 2019;35:420–1. doi: 10.4103/joacp.JOACP_192_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Moustafa MA, Alabd AS, Ahmed AM, Deghidy EA. Erector spinae versus paravertebral plane blocks in modified radical mastectomy:Randomised comparative study of the technique success rate among novice anaesthesiologists. Indian J Anaesth. 2020;64:49. doi: 10.4103/ija.IJA_536_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bhuvaneswari V, Wig J, Mathew PJ, Singh G. Post-operative pain and analgesic requirements after paravertebral block for mastectomy:A randomized controlled trial of different concentrations of bupivacaine and fentanyl. Indian J Anaesth. 2012;56:34. doi: 10.4103/0019-5049.93341. [DOI] [PMC free article] [PubMed] [Google Scholar]