

Abstract
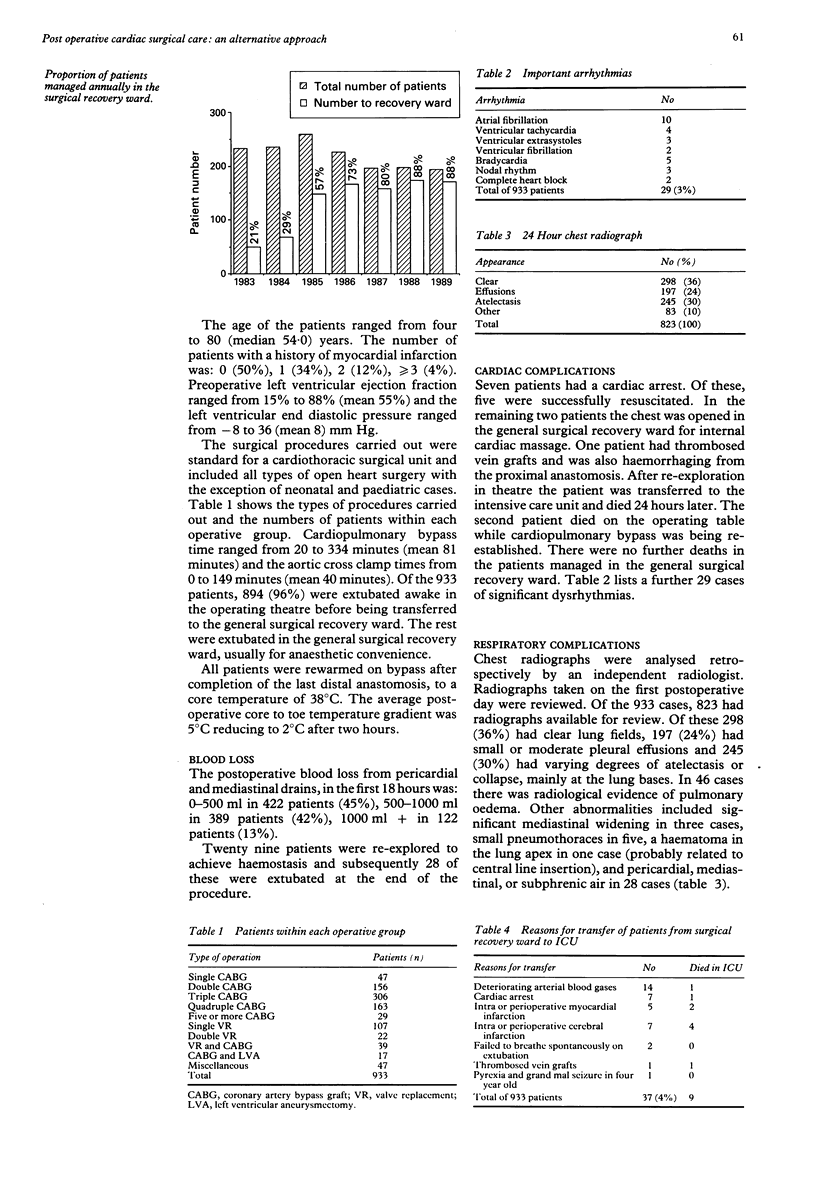
Combined appropriate anaesthetic and surgical techniques have allowed increasing numbers of patients to be successfully managed in a general surgical recovery ward after cardiac surgery rather than in an intensive care unit. From 1983 to 1989, 933 of 1542 patients undergoing open heart surgery were transferred to the general surgical recovery ward in the immediate postoperative period. Of these, 718 (77%) had undergone coronary artery bypass grafts, sometimes combined with other procedures and 168 (18%) had had cardiac valve replacements with or without other procedures. The remaining 47 (5%) had had miscellaneous cardiac operations. Significant cardiac complications occurred in 29 (3%) patients. The 24 hour chest radiograph was reported as abnormal (mainly atelectasis and effusion) in 63% of patients. Most resolved spontaneously or with physiotherapy. Twenty nine (3%) patients were re-explored to achieve haemostasis. There were no deaths in the general surgical recovery ward. Thirty seven (4%) patients had to be transferred to the intensive care unit for various reasons. The remaining 896 patients were transferred to the general ward after one night (871 patients) or two nights (25 patients) in the general surgical recovery ward. The average duration of stay in hospital for these patients was 9·3 days. Because of the overall success of such management and the low rate of complications over 80% of patients are now managed in the general surgical recovery ward after open heart surgery. The resulting savings in capital expenditure of equipment, medical, nursing, and technical personnel are substantial, and there are major implications for the planning of new cardiothoracic units.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Alfieri A., Kotler M. N. Noncardiac complications of open-heart surgery. Am Heart J. 1990 Jan;119(1):149–158. doi: 10.1016/s0002-8703(05)80095-x. [DOI] [PubMed] [Google Scholar]
- Aps C., Hutter J. A., Williams B. T. Anaesthetic management and postoperative care of cardiac surgical patients in a general recovery ward. Anaesthesia. 1986 May;41(5):533–537. doi: 10.1111/j.1365-2044.1986.tb13280.x. [DOI] [PubMed] [Google Scholar]
- Carter A. R., Sostman H. D., Curtis A. M., Swett H. A. Thoracic alterations after cardiac surgery. AJR Am J Roentgenol. 1983 Mar;140(3):475–481. doi: 10.2214/ajr.140.3.475. [DOI] [PubMed] [Google Scholar]
- Gale G. D., Teasdale S. J., Sanders D. E., Bradwell P. J., Russell A., Solaric B., York J. E. Pulmonary atelectasis and other respiratory complications after cardiopulmonary bypass and investigation of aetiological factors. Can Anaesth Soc J. 1979 Jan;26(1):15–21. doi: 10.1007/BF03039447. [DOI] [PubMed] [Google Scholar]
- Hutter J. A., Aps C., Hemsi D., Williams B. T. The management of cardiac surgical patients in a general surgical recovery ward. J Cardiovasc Surg (Torino) 1989 Mar-Apr;30(2):273–276. [PubMed] [Google Scholar]
- Kennedy J. W., Kaiser G. C., Fisher L. D., Fritz J. K., Myers W., Mudd J. G., Ryan T. J. Clinical and angiographic predictors of operative mortality from the collaborative study in coronary artery surgery (CASS). Circulation. 1981 Apr;63(4):793–802. doi: 10.1161/01.cir.63.4.793. [DOI] [PubMed] [Google Scholar]
- Koning H. M., Koning A. J., Leusink J. A. Serious acute renal failure following open heart surgery. Thorac Cardiovasc Surg. 1985 Oct;33(5):283–287. doi: 10.1055/s-2007-1014142. [DOI] [PubMed] [Google Scholar]
- Thorsen M. K., Goodman L. R. Extracardiac complications of cardiac surgery. Semin Roentgenol. 1988 Jan;23(1):32–48. doi: 10.1016/s0037-198x(88)80016-6. [DOI] [PubMed] [Google Scholar]