

Abstract
Key Clinical Message
On dermoscopy, the central area was greenish‐yellow with a coarse cobblestone‐like structureless material‐filled pattern, along with a bull's‐horn‐like tip and white globules. The marginal area was skin‐colored with a dark red background and a dome‐shaped pattern. A collarette with white ring and radial streaks, and whitish globules was noted.
Abstract
In recent years, the dermoscopic findings of Warty dyskeratoma have only been reported in a few cases. A 71‐year‐old man presented with a brownish papular lesion, with a central umbilical fossa, posterior to the right auricle. Histopathologically, a keratocystic tumor with a dome‐like morphology and an epidermal invagination in its limbic part was noted. The central part surrounding the fissure was filled with horn‐like cells with cornification tendency. Corps ronds were mostly distributed in the stratum corneum and granulosa, and grains were observed in the stratum corneum as acantholytic cells within the epidermal voids (lacunae). On dermoscopy, the central area was greenish‐yellow with a coarse cobblestone‐like structureless material‐filled pattern, along with a bull's‐horn‐like tip and white globules. The marginal area was skin‐colored with a dark red background and a dome‐shaped pattern. A collarette with white ring and radial streaks, and whitish globules was noted. No prominent vascular pattern was observed.
Keywords: acantholytic dyskeratosis, dermatopathology, dermoscopy, follicular dyskeratosis, warty dyskeratoma
A cup‐shaped epidermal invagination in focal acantholytic dyskeratosis

1. INTRODUCTION
Warty dyskeratoma (WD), a benign follicular‐type tumor, was first reported by Szymanski in 1957. 1 The dermoscopic aspect of WD was described in reports between 2016 and 2020, 1 , 3 , 4 , 5 , 6 , 7 but the reports did not include sufficient detail. Here, we present a case of WD based on its dermoscopic appearance. This study aimed to examine the relationship between the dermoscopic and histopathologic findings of WD in the context of previous studies.
2. CASE PRESENTATION
A 71‐year‐old man presented with an asymptomatic 4 mm × 6 mm brownish papule in the right postauricular region (Figure 1). The patient's medical and family history were unremarkable. The patient had noticed this lesion approximately 6 months earlier. Dermoscopy (performed using DermoGenius Handlupe [LINOS] with COOLPIX 4500 [NIKON]) revealed a glossy, dome‐shaped lesion that was whitish to reddish in color. The central part was umbilicated and foveal, it was also whitish, verrucous, and filled with keratinous material. The patient's hair was in contact with the tumor margin (Figure 1). A clinical diagnosis of keratoacanthoma was made, and a simple tumor resection was performed. Pathological findings of the resected specimen showed an irregularly thickened epithelium with increased keratinocytes displaying a dilated follicular infundibular architecture (Figure 2A). A hyalinized and fibrous stroma with intrastromal clefts was noted in the mid‐portion of the lower layer. The area above the basal cell layer of the thickened epithelium was void, and the basal cells exhibited a villous distribution (Figure 2B). Round cells (corps ronds) with clear areas (clear halo) around dyskeratotic keratinocytes and nuclei were distributed in the upper stratum spinosum. Hyperkeratotic cells (grains) with elongated nuclei were distributed in the stratum granulosum and stratum corneum (Figure 2C). There was inflammatory cell infiltration, mainly comprising lymphocytes and histiocytes, surrounding the blood vessels in the upper dermis. The lesion was excised longitudinally, as judged from the obtained specimen, along the short axis. These findings led to a final diagnosis of WD. Six months postoperatively, local recurrence was not observed, and the patient has been scheduled for periodic follow‐up.
FIGURE 1.

Clinical presentation and dermoscopic findings. A brownish papule with central umbilication on the posterior portion of the right ear. Dermoscopy shows a glossy and dome‐shaped morphology that is whitish to reddish in color. The central part is foveal and umbilicated. It is filled with keratinous material, has no identifiable structure, and is whitish in color. The inner marginal area is skin‐colored with a dark red dome‐like pattern, and a collarette with white ring streaks, white radial streaks, and whitish globules. The hair is in contact with the outer tumor margin, and a punctate whitish lesion is observed. There is no specific vascular finding (inset outlined with a black box).
FIGURE 2.
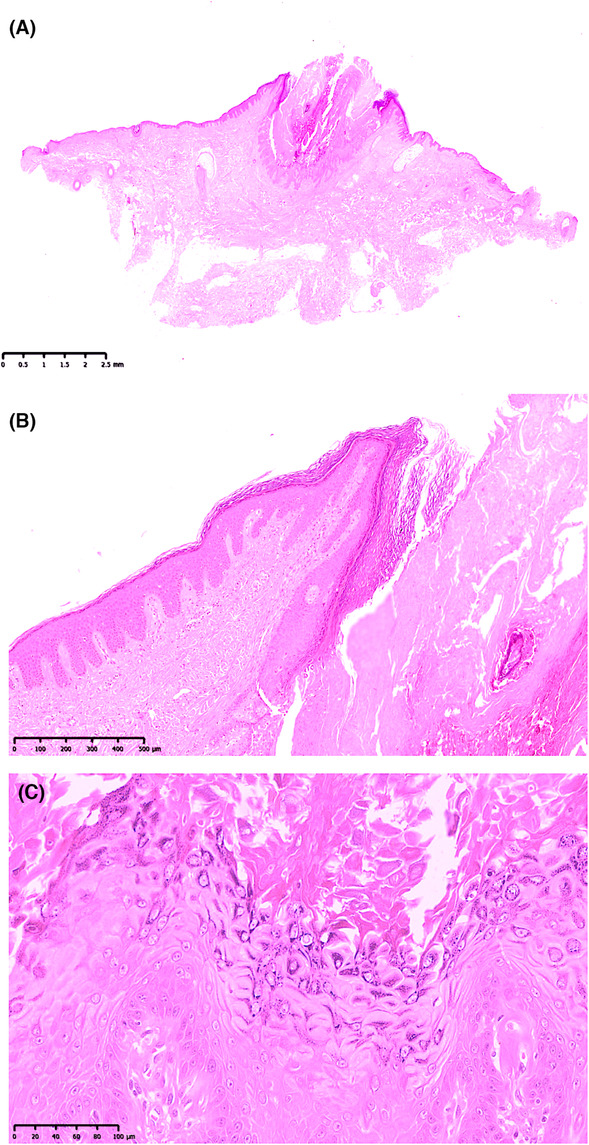
Histopathological findings. Hematoxylin–eosin (H&E) stain. (A) Complete image of the resected specimen. The epidermis is irregularly thickened, forming a dilated follicular, infundibular structure (H&E stain. Original magnification, ×8; scale bar, 2.5 mm). (B) Epidermal invagination can be seen. The stratum corneum is thickened in a complex fashion. A clear layer with strongly positive eosin staining is observed, and thickening of the granular layer is also observed. Ill‐defined structures that were weakly positive for eosin can be seen in the interdigitation. Inflammatory cell infiltration, mainly by lymphocytes and histiocytes, is observable in the vascular circumference in the upper layer of the corium (H&E stain. Original magnification, ×50; scale bar, 500 μm). (C) There are voids above the basal cell layer of the thickened epithelium, and the basal cells exhibit a villous distribution. Round cells (corps ronds) with clear areas (clear halo) around dyskeratotic keratinocytes and nuclei are distributed in the upper stratum spinosum. Hyperkeratotic cells (grains) with elongated nuclei are distributed in the stratum granulosum and stratum corneum (H&E stain. Original magnification, ×200; scale bar, 100 μm).
3. DISCUSSION/CONCLUSION
In 1972, Ackerman 8 suggested that WD should be included within the spectrum of dermatoses with focal acantholytic dyskeratosis (FAD). He proposed that the term WD should be restricted to lesions clinically presenting as a single nodule. He classified solitary FAD into three forms as follows: clinically nonapparent type (histologically incidental lesions), papular type (focal acantholytic dyskeratoma), and nodular type (WD). In 2002, Kaddu et al. 9 described three architectural patterns of cutaneous WD: cup‐shaped (63%), cystic (13%), and nodular (4%). According to these two classifications, the present case was the nodular type and showed cup‐shaped architecture. The dermoscopic findings of WD have been reported in six papers since the first report by Lencastre et al. 2 in 2016 and the most recent by Ingordo et al. 7 in 2020. Eight lesions were reported, six of which belonged to the same classification as the WD in the current patient. The dermoscopic appearance of WD reported in these six articles is described in the Appendix. 7 The dermoscopic features of WD in previous reports were nonspecific to the diagnosis of WD. In the current case, dermoscopy (Figure 1) showed that the central part of the lesion was filled with circular keratinous structureless material with a clear boundary. The surface was rough and irregular, and the color was whitish to light green. The lesion was well circumscribed and showed epidermal invagination with a structureless dome shape. The surface was shiny and smooth, and the color was pale white to reddish. In the collarette part of the image, a circular whitish ring corresponding to the epidermal invagination can be seen. From there, a whitish line is also observed toward the outer edge. Moreover, small scattered whitish areas can be seen in the dome‐like structure. Scattered hair and pigmentation were observed in the lateral margin. No prominent vascular pattern was detected. In summary (Figure 1), the central area showed a greenish‐yellow, unstructured, material‐filled pattern with a bull's‐horn‐like tip, and white pebbles (corresponding to keratotic cells with continuous acantholytic keratinocytes, corps ronds, and grains including whitish, homogenous zones demonstrating yellow clods interspersed hair‐like follicles). Second, the marginal area was skin‐colored with a dark red dome‐like pattern, a collarette with white ring streaks, white radial streaks, and whitish globules (corresponding to an epidermal invagination with intraepithelial intercellular cleft formation, dyskeratotic cells, hyperkeratosis, hypergranulosis, and acanthosis). Third, there was no prominent vascular pattern.
In a series of 46 cases of WD, 9 the histopathological features of cup‐shaped lesions consisted of relatively large, well‐circumscribed epidermal invaginations lined, mainly at the periphery and the base, by a proliferation of epithelial cells extending into the papillary dermis. The invagination was partially covered by a parakeratotic plug and often surrounded by an epidermal collarette and a hyperplastic epidermis with hypergranulosis and papillomatous features reminiscent of verruca vulgaris. All the lesions revealed foci of acantholysis with dyskeratosis. 9 The pathological findings in the current case were almost consistent with the findings of the above report (Figure 2A–C). In addition, a study of another 43 WD cases conducted in 2007 commonly revealed a cupuliform structure (77%) on histological examination, with numerous contiguous invaginated foci in 43% of the cases. 10
This case seems to be the most characteristic, single‐type, cup‐shaped WD to date. Histopathologically, it showed features of a cup‐shaped WD. Considering the relationship between dermoscopic and pathological findings, the current report describes the specific dermoscopic features of WD. Although only one case was reported, this paper is an essential addition to previous dermoscopy reports of WD. Future reports of the dermoscopic appearance of WD should specify the type and architecture of the WD. After describing the clinical presentation, a dermatoscopy evaluation should be performed, and histological assessment should follow to resolve the clinical dilemma.
AUTHOR CONTRIBUTIONS
Tomoaki Takada: Conceptualization; data curation; formal analysis; funding acquisition; investigation; methodology; project administration; resources; software; supervision; validation; visualization; writing – original draft; writing – review and editing.
FUNDING INFORMATION
This research received no external funding.
CONFLICT OF INTEREST STATEMENT
The author has no conflicts of interest to declare.
INSTITUTIONAL REVIEW BOARD STATEMENT
All the procedures adopted in this study were in accordance with the ethical standards of the World Medical Association Declaration of Helsinki. Ethical approval was not required for this study in accordance with local and national guidelines.
CONSENT
Written informed consent was obtained from the patient for the publication of this case report and accompanying images.
ACKNOWLEDGMENTS
I am grateful to the patients for providing consent for the use of their samples in this study. Moreover, we would like to thank the Wiley Editing Service for the English language editing.
Takada T. Warty dyskeratoma: The relationship between its dermoscopic and histopathological findings. Clin Case Rep. 2023;11:e7495. doi: 10.1002/ccr3.7495
DATA AVAILABILITY STATEMENT
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
REFERENCES
- 1. Szymanski FJ. Warty dyskeratoma: a benign cutaneous tumor resembling Darier’ disease microscopically. AMA Arch Derm. 1957;75:567‐572. [DOI] [PubMed] [Google Scholar]
- 2. Lencastre A, Campos S, Cbete J. Warty dyskeratoma. J Am Acad Dermatol. 2016; 75:e97‐e98. [DOI] [PubMed] [Google Scholar]
- 3. Salerni G, Alonso C, Calligaris M, Gorosito M, Fernandez‐Bussy R. Dermoscopy of multiple warty dyskeratoma. Dermatol Pract Concept. 2017; 7;47‐49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Nakagawa T, Umekage K, Komatsu S, et al. Case of warty dyskeratoma with unique dermoscopic features. J Dermatol. 2018;45:e74‐e75. [DOI] [PubMed] [Google Scholar]
- 5. Isaka Y, Matsuda H, Ogita A, Saeki H, Tanaka M, Ansai SI. Case of warty dyskeratoma on the anterior chest: the relationship between its dermoscopic and histopathological findings. J Dermatol. 2018;45:e171‐e172. [DOI] [PubMed] [Google Scholar]
- 6. Di Brizzi EV, Russo T, Piccolo V, et al. Warty dyskeratoma: clinical and dermoscopic features. Int J Dermatol. 2019;58:e229‐e231. [DOI] [PubMed] [Google Scholar]
- 7. Ingordo V, Ferrara G, Ingordo I, Argenziano G. A case of post‐inflammatory warty dyskeratoma of the chest: other dermoscopic features. Dermatol Reports. 2020;12:8791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Ackerman AB. Focal acantholytic dyskeratosis. Arch Dermatol. 1972;106:702‐706. [PubMed] [Google Scholar]
- 9. Kaddu S, Dong H, Mayer G, Kerl H, Cerroni L. Warty dyskeratoma—“follicular dyskeratoma”: analysis of clinicopathologic features of a distinctive follicular adnexal neoplasm. J Am Acad Dermatol. 2002;47:423‐428. [DOI] [PubMed] [Google Scholar]
- 10. Diallo M, Cribier B, Scrivener Y. Warty dyskeratoma: infundibular histogenesis. Anatomoclinical study of 43 cases. Ann Dermatol Venereol. 2007;134:633‐636. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.