

Abstract
AIM
To investigate the effectiveness and safety of subconjunctival injection of conbercept in the treatment of corneal neovascularization (CNV).
METHODS
The data on 10 consecutively recruited patients with CNV who received a subconjunctival conbercept (1 mg) once, and measured the area, length, and diameter of neovascularization before and after (1d, 1, 2wk, and 1mo) treatment as well as the occurrence of systemic and ocular complications after treatment were analyzed.
RESULTS
There was a statistically significant reduction in the area of CNV one day after treatment (mean±SD: 38.46±11.36 mm2), compared with before treatment (42.46±12.80 mm2, P<0.01). There was also a statistically significant reduction in the length (3.86±1.80 mm vs 4.64±1.77 mm, P<0.01) and diameter (0.044±0.022 vs 0.060±0.026, P<0.05) of CNV, one week after treatment comparing to before treatment. The reduction in all three parameters was maximized at two weeks after treatment (area: 29.49±8.83 mm2, P<0.001; length: 3.50±1.88 mm, P<0.001; and diameter: 0.038±0.017 mm, P<0.01). No severe systemic or ocular complication was observed during the study.
CONCLUSION
During the observation period of one-month, subconjunctival injection of conbercept is an effective and safe method for the reduction of CNV. It may be effective as a preoperative drug for neovascular corneal transplantation.
Keywords: corneal neovascularization, conbercept, anti-vascular endothelial growth factor, subconjunctival injection
INTRODUCTION
Corneal neovascularization (CNV) is the in-growth of new immature vasculature from the limbus into the avascular corneal tissue, which could lead to the opacification of the transparent cornea. As a highly prevalent cause of blindness in the world, CNV affects over 1.4 million people annually, 12% of whom suffer subsequent vision loss[1]–[2]. To date, the treatment of CNV includes local use of glucocorticoids and non-steroid anti-inflammatory medications, laser photocoagulation, fine needle diathermy, photodynamic therapy, and conjunctival, limbal, and amniotic membrane transplantation, all with however suboptimal effectiveness [1],[3]. One potential explanation for the suboptimal effectiveness might be that none of these treatments targets the molecular mediators of angiogenesis.
Recently, inhibitors of vascular endothelial growth factor (VEGF), which is the most important regulatory factor for angiogenesis, have shown good clinical application prospects and been approved for the treatment of neovascular fundus abnormalities[4]. Existing pre-clinical and clinical research has shown the effectiveness of subconjunctival or corneal stromal injection of different anti-VEGF agents (e.g., bevacizumab, ranibizumab, and aflibercept) in the treatment of CNV[5]–[6]. Conbercept (KH902; Chengdu Kanghong Biotech Co., China) is a recombinant fusion protein with key domains 2, 3, and 4 from VEGF receptors 1 and 2. It has a high affinity for all VEGF isoforms as well as placental growth factors[7]. In 2013, it was approved in China for the treatment of neovascular (wet) age-related macular degeneration and choroidal neovascularization secondary to pathological myopia[7]. Whether conbercept could be used in the treatment of CNV is however largely unknown. The present study aimed therefore to understand the effectiveness and safety of conbercept via subconjunctival injection in modulating the characteristics of CNV.
SUBJECTS AND METHODS
Ethical Approval
This study was additionally approved by the biomedical research ethics committee of Beijing Huimin Hospital (No.2018.1012). All recruited patients gave their written informed consent before their inclusion as participants in this study.
Study Participants
This is a case series study, including 10 patients with CNV who were consecutively recruited during December 2018-November 2019 in Beijing Huimin Hospital, Beijing, China.
Inclusion criteria: age ≥18y, clinical diagnosis of CNV without active eye diseases, and neovascularization more than 2 mm into the corneal limbus.
Exclusion criteria: corneal trauma, infection, or ophthalmic surgery during the past month; use of contact lenses during the past month; or severe systemic diseases.
Treatment
Levofloxacin eye drops were applied four times a day for three days before the injection of conbercept. On the day of injection, we used proparacaine hydrochloride eye drops as anesthesia, iodophor solution to sterilize the skin around the eyes, and povidone-iodine solution to sterilize the conjunctival sac. We injected 0.1 mL of conbercept (10 mg/mL) into the corneoscleral limbus near the root of the new blood vessels. All injections were administered by the same ophthalmologist (Sun C).
Study Outcomes
Visual acuity and area, length, and diameter of neovascularization at five different time points (before treatment, 1d, 1, 2wk, and 1mo after treatment), as well as systemic and ocular complications after treatment, were documented. Corneal images were taken at all five time points, using an anterior segment slit-lamp microscope at the magnification required to delineate the fine details of the vessels.
Data Analysis
We used Image pro plus 6.0 to measure the area, length, and diameter of neovascularization. Area was calculated by using the following formula: area (mm2)=CN/12×3.1416×[R2−(R−VL)2], where CN is the clock hours of neovascularization, R is the radius of the cornea, and VL is the longest vessel length, extending from the limbal vasculature[8]. In terms of length, we identified three blood vessels with the greatest length in the densest quadrant of CNV and measured the greatest distance between the starting point of each vessel at the corneal limbus and anywhere along the vessel. We then calculated the mean value of the length of these three vessels as the measured length. In terms of diameter, we measured the diameters of all new blood vessels at the corneal limbus and calculated the average value as the diameter.
Statistical Analysis
Statistical analysis was performed using SPSS 19.0. Shapiro-Wilk method was used to test the normality of data, and one-way repeated measure analysis of variance was used to compare data across the five time points. We also performed within-individual analysis to study the temporal trend of different parameters across the time points. Data are reported as mean±standard deviation (SD). A P<0.05 was considered statistically significant.
RESULTS
Clinical Characteristics
Among the 10 patients with CNV, all were male, with a mean age of 44±10.15y (Table 1).
Table 1. Clinical characteristics of the 10 patients with corneal neovascularization.
| ID | Sex/age | Right/left eye | Primary disease | CNV location | Vision acuity before treatment | Vision acuity 1mo after treatment | Complications |
| 1 | M/32 | Right | Chemical injury | Central | 3.3 | 3.6 | No |
| 2 | M/54 | Right | Herpes simplex virus keratitis | Peripheral | 4.0 | 4.0 | No |
| 3 | M/49 | Left | Chemical injury | Central+peripheral | 2.6 | 2.6 | No |
| 4 | M/28 | Left | Chemical injury | Central | 2 | 2 | No |
| 5 | M/48 | Left | Blepharokeratoconjunctivitis | Peripheral | 3.9 | 4.0 | No |
| 6 | M/61 | Right | Chemical injury | Central | 1 | 1 | No |
| 7 | M/34 | Left | Chemical injury | Central | 3.0 | 3.3 | No |
| 8 | M/38 | Right | Chemical injury | Central+peripheral | 2.3 | 2.6 | No |
| 9 | M/52 | Right | Neurotrophic keratopathy | Peripheral | 4.0 | 4.0 | No |
| 10 | M/44 | Right | Chemical injury | Central+peripheral | 2 | 2 | No |
CNV: Corneal neovascularization.
The mean±SD area of neovascularization was 42.46±12.80 mm2 before treatment, and there was a statistically significant difference between all the time points after treatment and the time point before treatment (all P<0.05, Table 2, Figure 1). There was also a clearly declining area across the four different time points after treatment (F=31.373, P<0.001).
Table 2. Area, length, and diameter of neovascularization before and after subconjunctival conbercept.
| Time point | Area (mm2) | Length (mm) | Diameter (mm) |
| Before | 42.46±12.80 | 4.64±1.77 | 0.060±0.026 |
| 1d | 38.46±11.36b | 4.27±1.89 | 0.055±0.021 |
| 1wk | 34.18±9.54b | 3.86±1.80b | 0.044±0.022a |
| 2wk | 29.49±8.83c | 3.50±1.88c | 0.038±0.017b |
| 1mo | 36.90±13.61a | 3.69±1.72b | 0.048±0.022a |
| F | 31.373 | 19.652 | 16.661 |
| P | <0.001 | <0.001 | <0.001 |
Compared with before treatment, aP<0.05, bP<0.01, cP<0.001.
Figure 1. Outcomes of corneal neovascularization (CNV) parameters at five different time points.

A: CNV area; B: CNV length; C: CNV diameter. Compared with before treatment, aP<0.05, bP<0.01, cP<0.001. The significant therapeutic response which was evidenced as early as 1d, then peaked at 2wk, and reduced at 1mo.
The mean±SD length of neovascularization was 4.64±1.77 mm before treatment and there was a statistically significant difference between the length measured at 1, 2wk, as well as 1mo after treatment and the length measured before treatment (all P<0.01; Table 2, Figure 1). There was also a declining trend of length across the four time points after treatment (F=19.652, P<0.001).
The mean±SD diameter of neovascularization was 0.060±0.026 mm before treatment and there was a statistically significant difference between the diameter measured at 1wk, 2wk, as well as 1mo after treatment and the diameter measured before treatment (all P<0.05; Table 2, Figure 1). There was also a declining trend of diameter across the four time points after treatment (F=16.661, P<0.001).
The slit-lamp photographs of patient 3 were shown in Figure 2.
Figure 2. The effect of subconjunctival conbercept in patient 3, a 49-year-old man with chemical injury in the left eye complicated by corneal scarring, and neovascularization.
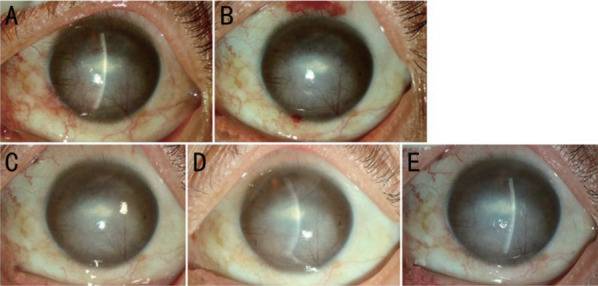
A: Baseline picture shows two main vessel branches emerging from the 12-o'clock and 5-o'clock position at the limbus and passing into the depressed scar in the corneal mid-periphery where it branched several times into smaller-caliber vessels. B, C, D, E: 1d, 1, 2wk, and 1mo after subconjunctival conbercept.
DISCUSSION
The formation of CNV is a complex process, involving vascular endothelial cells, keratinocytes, and inflammatory cells[9]. Neovascular patterns can be separated into three groups, namely deep neovascularization overlying Descemet's membrane (herpetic and luetic interstitial keratitis), stromal neovascularization (as a result of stromal keratitis), and vascular pannus (ocular surface disorders)[10]. Multiple factors might contribute to the development of CNV. For instance, VEGF is the most important pro-angiogenic factor[2] and demonstrates a significantly increased concentration in the vascularized cornea[9]. On the other hand, VEGF antagonists have been shown to reduce CNV in animal models[10], whereas anti-VEGF drugs have been shown to improve the survival rate of transplanted corneal grafts by restoring the “immune privilege” of the cornea[11]. Subconjunctival bevacizumab, ranibizumab, and aflibercept crossed the blood and seemed to be effective in inhibiting CNV without causing epitheliopathy in an experimental rat model compared to the controls. No significant results were noted between these three anti-VEGF molecules, however, multiple-dose bevacizumab treatment seems to be more effective[11]–[12].
Several anti-VEGF agents are currently used in clinical off-label for the treatment of CNV, and most of them appear to be a safe, effective, and practical method[5],[13]–[16]. In the first report of human use of topical bevacizumab for CNV, two patients showed significant reductions in superficial and deep stromal neovascularization without impairment in the corneal endothelium[17]. Others have also shown that perilimbal and intrastromal injection of bevacizumab before penetrating keratoplasty can improve surgical outcomes of high-risk patients[18]. Ranibizumab, another monoclonal antibody against VEGF-A, has also been used to reduce CNV in both animal models and clinical studies[19]–[20]. Aflibercept (VEGF TrapR1R2) has strong anti-VEGF activity and is a soluble fusion protein with binding domains for both VEGF receptors 1 and 2. Subconjunctival injection of aflibercept can reduce donor vascularization and improve graft survival in a high-risk graft murine model[21]. However, Sella et al[22] showed that a single subconjunctival aflibercept injection was ineffective to regress formed CNV.
So far, the only topical antiangiogenic agent tested in phase II and III trials is aganirsen. Administration of topical aganirsen eye drops (86 µg/d per eye) in patients with keratitis related progressive CNV has been shown to lead to significant amelioration of CNV and reduced need for corneal transplantation[23]. Although these agents are effective in the treatment of actively growing vessels, they have limited efficacy in well-established CNV[24].
Conbercept can both bind to placental growth factor and all isoforms of VEGF-A and VEGF-B[25]. As it has multiple targets, strong affinity, and a long half-life cycle, conbercept has proved to be effective and safe in the treatment of diabetic macular edema[26]. In cases of refractory macular edema secondary to central retinal vein occlusion (CRVO), after switching from bevacizumab/ranibizumab, conbercept can improve macular thickness and extend interval of injection[27]. Du et al[28] confirmed that conbercept, especially early administration, can effectively inhibit CNV in rabbits, intrastromal administrations has the better effect than subconjunctival injection.
The present study used conbercept in patients with CNV and showed that the area of CNV reduced significantly already one day after treatment whereas the length and diameter of CNV reduced significantly one week after treatment. As the reduction in all three parameters peaked at two weeks after treatment, it might be beneficial to administer new injections to maintain or enhance effectiveness. For instance, although there were still significant reductions in all three indicators at one month after treatment, compared to the pre-treatment period, the magnitude of reductions diminished compared to two weeks after treatment. The observation time of this study was only 1mo, and it is speculated that with the extension of time (such as 3mo), the CNV may recur, suggesting the potential need of repeated treatments[15]. Alternatively, for patients with stable CNV, transplantation of corneal graft might be considered at this time point, with the aim to achieve the best treatment effect for reducing neovascularization.
Although all patients in the present study demonstrated a reduction in CNV after treatment, the reduction varied in magnitude and none of the patients had a complete resolution. There are multiple potential explanations for the partial effectiveness. First, the dosage administered in the present treatment is not sufficient to completely antagonize the corneal VEGF burden. Second, we only injected conbercept once and this might have led to a low cumulative concentration of the medication. Third, cytokines other than VEGF, such as transforming growth factor-α, transforming growth factor-β1, and fibroblast growth factor, can also induce CNV[29] and are not targeted by conbercept. Because neovascularization likely involves multiple processes, targeting VEGF alone might prevent the pro-angiogenic cascade but not others. Finally, conbercept works mostly on newly formed blood vessels, whereas our case series included patients with CNV due to different reasons and patients with both newly formed and long-standing neovascularization. As a result, some of the patients included in this study had more severe CNV with more mature vessels. As discussed above, the limited number of treatments might have also affected the treatment effectiveness.
Previous evidence suggests that VEGF inhibitors can influence corneal healing by interfering with macrophage infiltration[30]. Soleimani et al[31] reported two cases with Descemet membrane detachment after intrastromal bevacizumab injection in patients with previous lamellar keratoplasty. The hemorrhagic Descemet membrane detachment was not resolved, the donor had to exchange with a new one because of staining in one of the patients. We should emphasize that the complications were not related to bevacizumab, instead the injection method was involved in these situations. In this study, we injected conbercept in the corneoscleral limbus near the root of the CNV to avoid damaging the corneal tissue. The subconjunctival injection may be a safer method, and the medication can however diffuse in a short distance through the conjunctival tissue to the central blood vessels. There was no thinning of the corneal epithelium or stroma, injury in corneal epithelium, conjunctivitis, keratitis, endophthalmitis, cataract, or other complications, demonstrating the safety of subconjunctival conbercept.
In conclusion, subconjunctival conbercept may be an effective and safe option for the treatment of CNV, significantly reducing the area, length, and diameter of CNV without severe complications. Conbercept may also be considered an adjunct to other medical or surgical treatments of CNV. The use of conbercept for CNV is however still off-label. Further studies with a larger number of patients and longer follow-up are needed to validate our findings and to optimize the treatment regimen (e.g., number and timing of injections as well as injections versus other routes of administration). Comparison studies with other anti-VEGF agents are also helpful.
Acknowledgments
Foundation: Supported by the National Natural Science Foundation of China (No.81970764); the Youth Beijing Scholar (No.2020-022).
Conflicts of Interest: Sun C, None; Ruan F, None; Li S, None; Zhang JQ, None; Jie Y, None.
REFERENCES
- 1.Feizi S, Azari AA, Safapour S. Therapeutic approaches for corneal neovascularization. Eye Vis. 2017;4(1):1–10. doi: 10.1186/s40662-017-0094-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shirzaei Sani E, Kheirkhah A, Rana D, Sun ZM, Foulsham W, Sheikhi A, Khademhosseini A, Dana R, Annabi N. Sutureless repair of corneal injuries using naturally derived bioadhesive hydrogels. Sci Adv. 2019;5(3):eaav1281. doi: 10.1126/sciadv.aav1281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Yin QC, Han HJ, Shi KX, Zhou JY, Zheng SF, Yao K, Shentu XC. Targeted dexamethasone nano-prodrug for corneal neovascularization management. Biomed J. 2023:S2319-S4170(23)00029-X. doi: 10.1016/j.bj.2023.03.005. [DOI] [PubMed] [Google Scholar]
- 4.Tolentino M. Systemic and ocular safety of intravitreal anti-VEGF therapies for ocular neovascular disease. Surv Ophthalmol. 2011;56(2):95–113. doi: 10.1016/j.survophthal.2010.08.006. [DOI] [PubMed] [Google Scholar]
- 5.Yeung SN, Lichtinger A, Kim P, Amiran MD, Slomovic AR. Combined use of subconjunctival and intracorneal bevacizumab injection for corneal neovascularization. Cornea. 2011;30(10):1110–1114. doi: 10.1097/ICO.0b013e31821379aa. [DOI] [PubMed] [Google Scholar]
- 6.Gore A, Horwitz V, Cohen M, Gutman H, Cohen L, Gez R, Kadar T, Dachir S. Successful single treatment with ziv-aflibercept for existing corneal neovascularization following ocular chemical insult in the rabbit model. Exp Eye Res. 2018;171:183–191. doi: 10.1016/j.exer.2018.03.010. [DOI] [PubMed] [Google Scholar]
- 7.Zhang JX, Liang Y, Xie J, Li D, Hu Q, Li XS, Zheng WY, He R. Conbercept for patients with age-related macular degeneration: a systematic review. BMC Ophthalmol. 2018;18(1):142. doi: 10.1186/s12886-018-0807-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lu Y, Tai PWL, Ai JZ, Gessler DJ, Su Q, Yao XY, Zheng Q, Zamore PD, Xu X, Gao GP. Transcriptome profiling of neovascularized corneas reveals miR-204 as a multi-target biotherapy deliverable by rAAVs. Mol Ther Nucleic Acids. 2018;10:349–360. doi: 10.1016/j.omtn.2017.12.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Andrés G, Leali D, Mitola S, Coltrini D, Camozzi M, Corsini M, Belleri M, Hirsch E, Schwendener RA, Christofori G, Alcamì A, Presta M. A pro-inflammatory signature mediates FGF2-induced angiogenesis. J Cellular Molecular Medi. 2009;13(8b):2083–2108. doi: 10.1111/j.1582-4934.2008.00415.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ellenberg D, Azar DT, Hallak JA, Tobaigy F, Han KY, Jain S, Zhou ZJ, Chang JH. Novel aspects of corneal angiogenic and lymphangiogenic privilege. Prog Retin Eye Res. 2010;29(3):208–248. doi: 10.1016/j.preteyeres.2010.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Eski MT, Teberik K, Oltulu P, Ankaralı H, Kaya M, Alpay M. The effects of subconjunctival bevacizumab, ranibizumab, and aflibercept on corneal neovascularization. Hum Exp Toxicol. 2022;41:9603271221084674. doi: 10.1177/09603271221084674. [DOI] [PubMed] [Google Scholar]
- 12.Ulas B, Altan-Yaycioglu R, Bal N. Comparison of the inhibitory effect of different doses of subconjunctival bevacizumab application in an experimental model of corneal neovascularization. Int J Ophthalmol. 2018;11(7):1090–1095. doi: 10.18240/ijo.2018.07.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.DeStafeno JJ. Topical bevacizumab therapy for corneal neovascularization. Arch Ophthalmol. 2007;125(6):834. doi: 10.1001/archopht.125.6.834. [DOI] [PubMed] [Google Scholar]
- 14.Cheng SF, Dastjerdi MH, Ferrari G, Okanobo A, Bower KS, Ryan DS, Amparo F, Stevenson W, Hamrah P, Nallasamy N, Dana R. Short-term topical bevacizumab in the treatment of stable corneal neovascularization. Am J Ophthalmol. 2012;154(6):940–948.e1. doi: 10.1016/j.ajo.2012.06.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chu HS, Chen TC, Hu FR, Chen WL. Recurrence of corneal neovascularization associated with lipid deposition after subconjunctival injection of bevacizumab. Cornea. 2013;32(11):1446–1453. doi: 10.1097/ICO.0b013e31825ec407. [DOI] [PubMed] [Google Scholar]
- 16.Stevenson W, Cheng SF, Dastjerdi MH, Ferrari G, Dana R. Corneal neovascularization and the utility of topical VEGF inhibition: ranibizumab (lucentis) vs bevacizumab (avastin) Ocular Surf. 2012;10(2):67–83. doi: 10.1016/j.jtos.2012.01.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lichtinger A, Yeung SN, Kim P, Amiran MD, Elbaz U, Slomovic AR. Corneal endothelial safety following subconjunctival and intrastromal injection of bevacizumab for corneal neovascularization. Int Ophthalmol. 2014;34(3):597–601. doi: 10.1007/s10792-013-9807-6. [DOI] [PubMed] [Google Scholar]
- 18.Vassileva PI, Hergeldzhieva TG. Avastin use in high risk corneal transplantation. Graefes Arch Clin Exp Ophthalmol. 2009;247(12):1701–1706. doi: 10.1007/s00417-009-1170-y. [DOI] [PubMed] [Google Scholar]
- 19.Liarakos VS, Papaconstantinou D, Vergados I, Douvali M, Theodossiadis PG. The effect of subconjunctival ranibizumab on corneal and anterior segment neovascularization: study on an animal model. Eur J Ophthalmol. 2014;24(3):299–308. doi: 10.5301/ejo.5000391. [DOI] [PubMed] [Google Scholar]
- 20.Ferrari G, Dastjerdi MH, Okanobo A, Cheng SF, Amparo F, Nallasamy N, Dana R. Topical ranibizumab as a treatment of corneal neovascularization. Cornea. 2013;32(7):992–997. doi: 10.1097/ICO.0b013e3182775f8d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Dohlman TH, Omoto M, Hua J, Stevenson W, Lee SM, Chauhan SK, Dana R. VEGF-trap aflibercept significantly improves long-term graft survival in high-risk corneal transplantation. Transplantation. 2015;99(4):678–686. doi: 10.1097/TP.0000000000000512. [DOI] [PubMed] [Google Scholar]
- 22.Sella R, Ben Ishai M, Livny E, Nahum Y, Bahar I. Subconjunctival aflibercept for the treatment of formed corneal neovascularization. Eye Contact Lens. 2020;47(4):180–184. doi: 10.1097/ICL.0000000000000709. [DOI] [PubMed] [Google Scholar]
- 23.Cursiefen C, Viaud E, Bock F, et al. Aganirsen antisense oligonucleotide eye drops inhibit keratitis-induced corneal neovascularization and reduce need for transplantation. Ophthalmology. 2014;121(9):1683–1692. doi: 10.1016/j.ophtha.2014.03.038. [DOI] [PubMed] [Google Scholar]
- 24.Chang JH, Garg NK, Lunde E, Han KY, Jain S, Azar DT. Corneal neovascularization: an anti-VEGF therapy review. Surv Ophthalmol. 2012;57(5):415–429. doi: 10.1016/j.survophthal.2012.01.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sun XD, Lu XM. Profile of conbercept in the treatment of neovascular age-related macular degeneration. Drug Des Dev Ther. 2015:2311. doi: 10.2147/DDDT.S67536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Liu K, Wang HY, He W, et al. Intravitreal conbercept for diabetic macular oedema: 2-year results from a randomised controlled trial and open-label extension study. Br J Ophthalmol. 2022;106(10):1436–1443. doi: 10.1136/bjophthalmol-2020-318690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zhao T, Zhang HS, Chen Y, Wang ZJ. Efficacy of conbercept after switching from bevacizumab/ranibizumab in eyes of macular edema secondary to central retinal vein occlusion. Int J Ophthalmol. 2022;15(4):609–614. doi: 10.18240/ijo.2022.04.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Du LQ, Sun JZ, Liu J, Xu N, Liu M, Wu XY. Effect of conbercept on corneal neovascularization in a rabbit model. Semin Ophthalmol. 2023:1–9. doi: 10.1080/08820538.2023.2201652. [DOI] [PubMed] [Google Scholar]
- 29.Chang JH, Gabison EE, Kato T, Azar DT. Corneal neovascularization. Curr Opin Ophthalmol. 2001;12(4):242–249. doi: 10.1097/00055735-200108000-00002. [DOI] [PubMed] [Google Scholar]
- 30.Kim SW, Ha BJ, Kim EK, Tchah H, Kim TI. The effect of topical bevacizumab on corneal neovascularization. Ophthalmology. 2008;115(6):e33–e38. doi: 10.1016/j.ophtha.2008.02.013. [DOI] [PubMed] [Google Scholar]
- 31.Soleimani M, Shahbazi A, Mohammadi N, Tabatabaei SA. Complications of intrastromal bevacizumab injection in lamellar keratoplasty. Int J Ophthalmol. 2020;13(2):356–358. doi: 10.18240/ijo.2020.02.22. [DOI] [PMC free article] [PubMed] [Google Scholar]