

Abstract
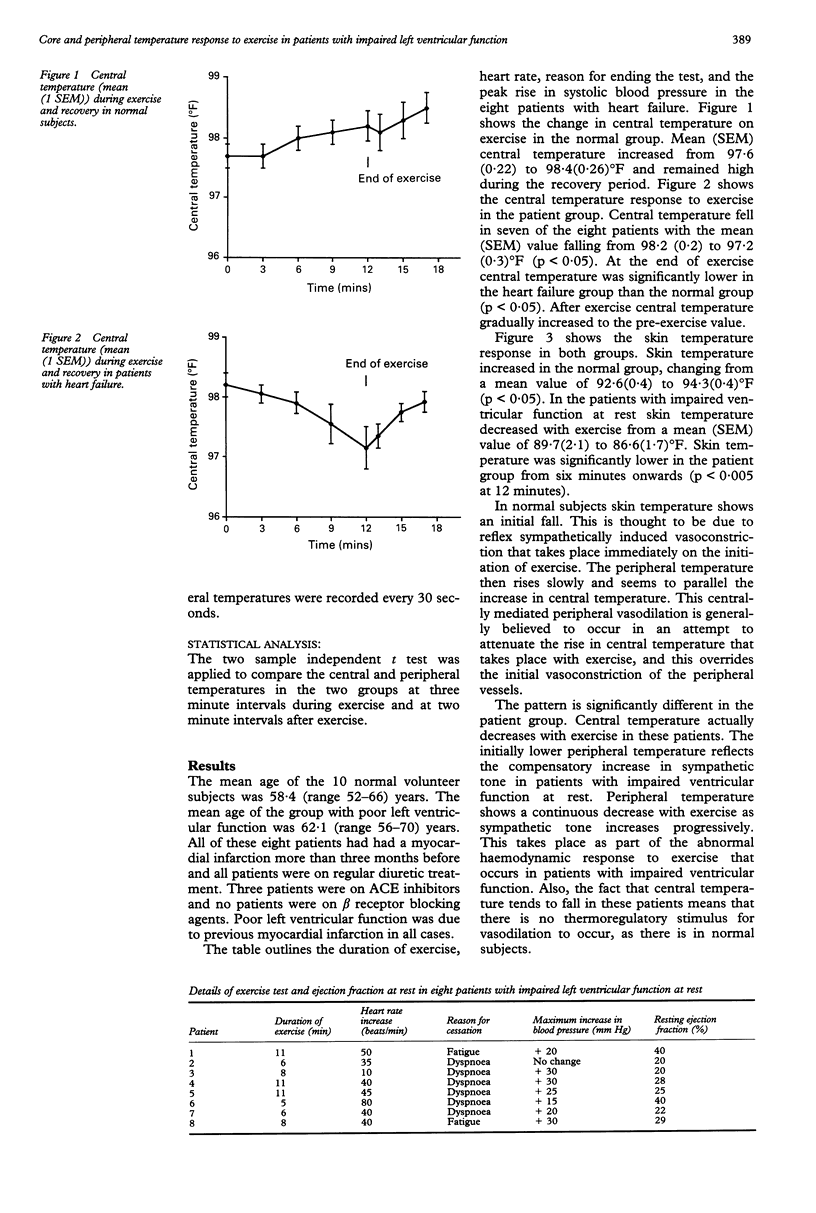
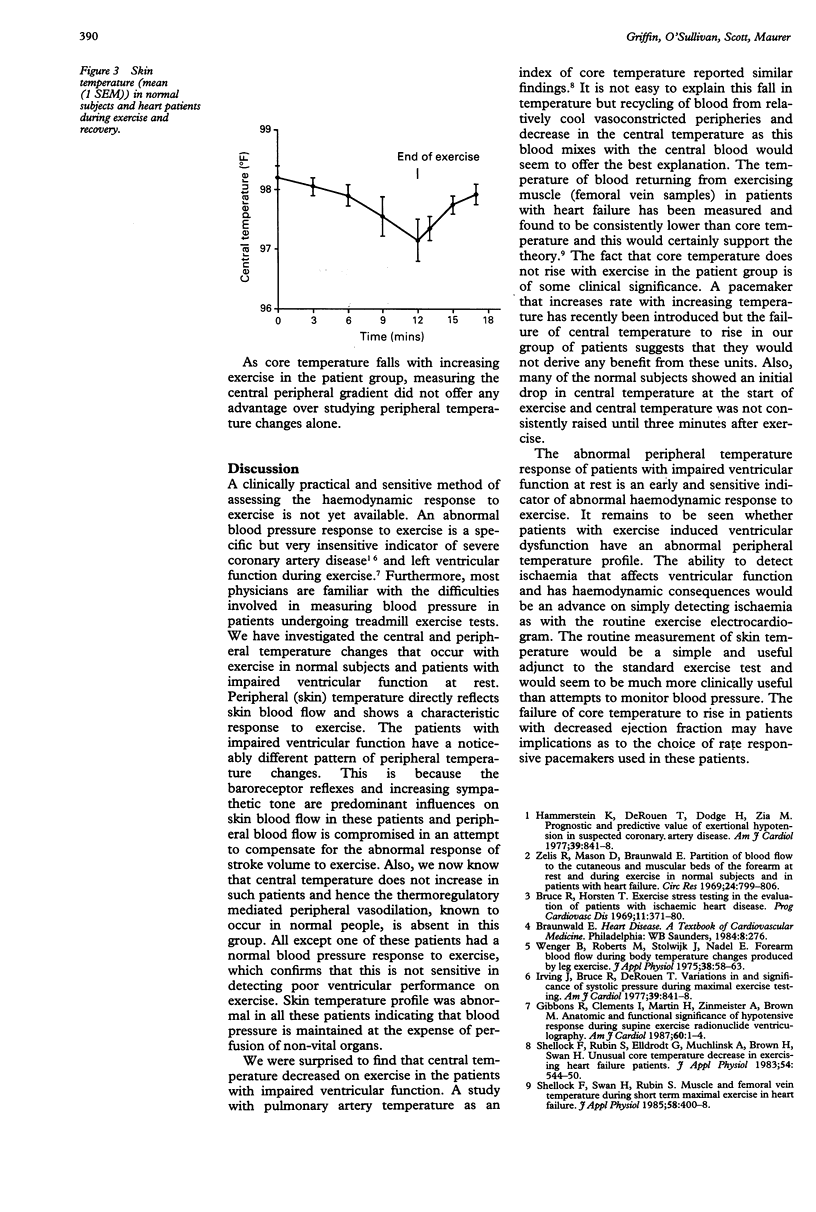
OBJECTIVE--Exercise induced hypotension is a specific but insensitive indicator of severe coronary artery disease. Skin blood flow is subject to control by baroreceptor mediated reflexes as well as thermoregulatory reflexes. Monitoring skin temperature or the skin to central temperature gradient may be a more sensitive indicator of impaired cardiac output response to exercise than hypotension. DESIGN AND PARTICIPANTS--Central and skin temperature changes associated with exercise were studied in 10 normal volunteers and eight patients with impaired resting ventricular function due to ischaemic heart disease. Patients exercised according to a modified Bruce protocol. The two sample independent t test was applied to compare the central and peripheral temperatures in the two groups at three minute intervals during exercise and at two minute intervals after exercise. RESULTS--A significant decrease was found in mean (1 SEM) central temperature on exercise in our patient group (98.2(0.2) degrees F to 97.2(0.3) degrees F), compared with the normal increase in central temperature (97.7(0.2) degrees F to 98.3(0.3) degrees F). Mean (1 SEM) skin temperature changes reflected the expected skin blood flow changes with exercise in normal subjects. In the patient group skin temperature declined during exercise (89.7(2.1) degrees F to 86.6(1.7) degrees F) and was significantly lower than normal from six minutes onwards. CONCLUSIONS--The abnormal peripheral temperature changes of patients with impaired resting ventricular function is an early and sensitive indicator of an abnormal haemodynamic response to exercise. It is possible that skin temperature measurement during exercise could help detect exercise induced ventricular dysfunction due to ischaemia or impaired cardiac output due to valvar heart disease.
Full text
PDF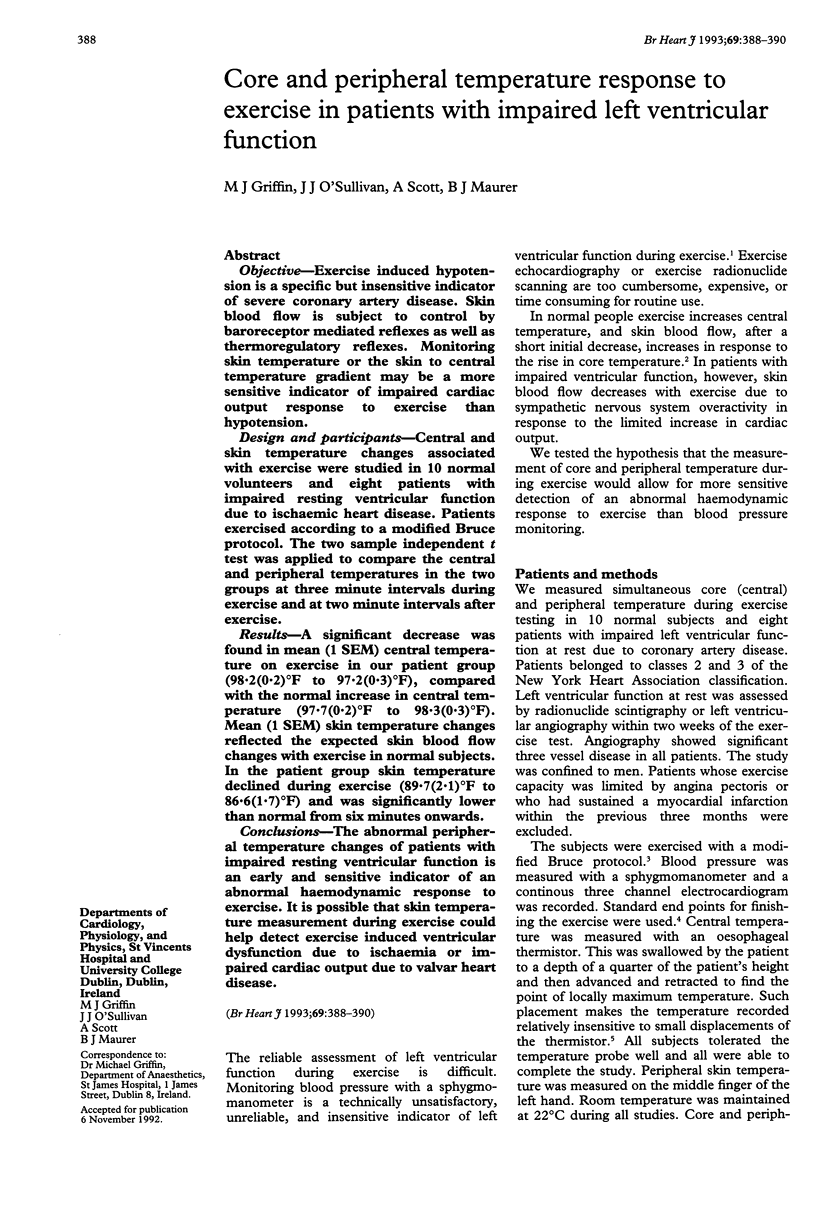
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Irving J. B., Bruce R. A., DeRouen T. A. Variations in and significance of systolic pressure during maximal exercise (treadmill) testing. Am J Cardiol. 1977 May 26;39(6):841–848. doi: 10.1016/s0002-9149(77)80037-4. [DOI] [PubMed] [Google Scholar]
- Shellock F. G., Swan H. J., Rubin S. A. Muscle and femoral vein temperatures during short-term maximal exercise in heart failure. J Appl Physiol (1985) 1985 Feb;58(2):400–408. doi: 10.1152/jappl.1985.58.2.400. [DOI] [PubMed] [Google Scholar]
- Wenger C. B., Roberts M. F., Stolwijk J. A., Nadel E. R. Forearm blood flow during body temperature transients produced by leg exercise. J Appl Physiol. 1975 Jan;38(1):58–63. doi: 10.1152/jappl.1975.38.1.58. [DOI] [PubMed] [Google Scholar]
- Wenger C. B., Roberts M. F., Stolwijk J. A., Nadel E. R. Forearm blood flow during body temperature transients produced by leg exercise. J Appl Physiol. 1975 Jan;38(1):58–63. doi: 10.1152/jappl.1975.38.1.58. [DOI] [PubMed] [Google Scholar]
- Zelis R., Mason D. T., Braunwald E. Partition of blood flow to the cutaneous and muscular beds of the forearm at rest and during leg exercise in normal subjects and in patients with heart failure. Circ Res. 1969 Jun;24(6):799–806. doi: 10.1161/01.res.24.6.799. [DOI] [PubMed] [Google Scholar]