

Abstract
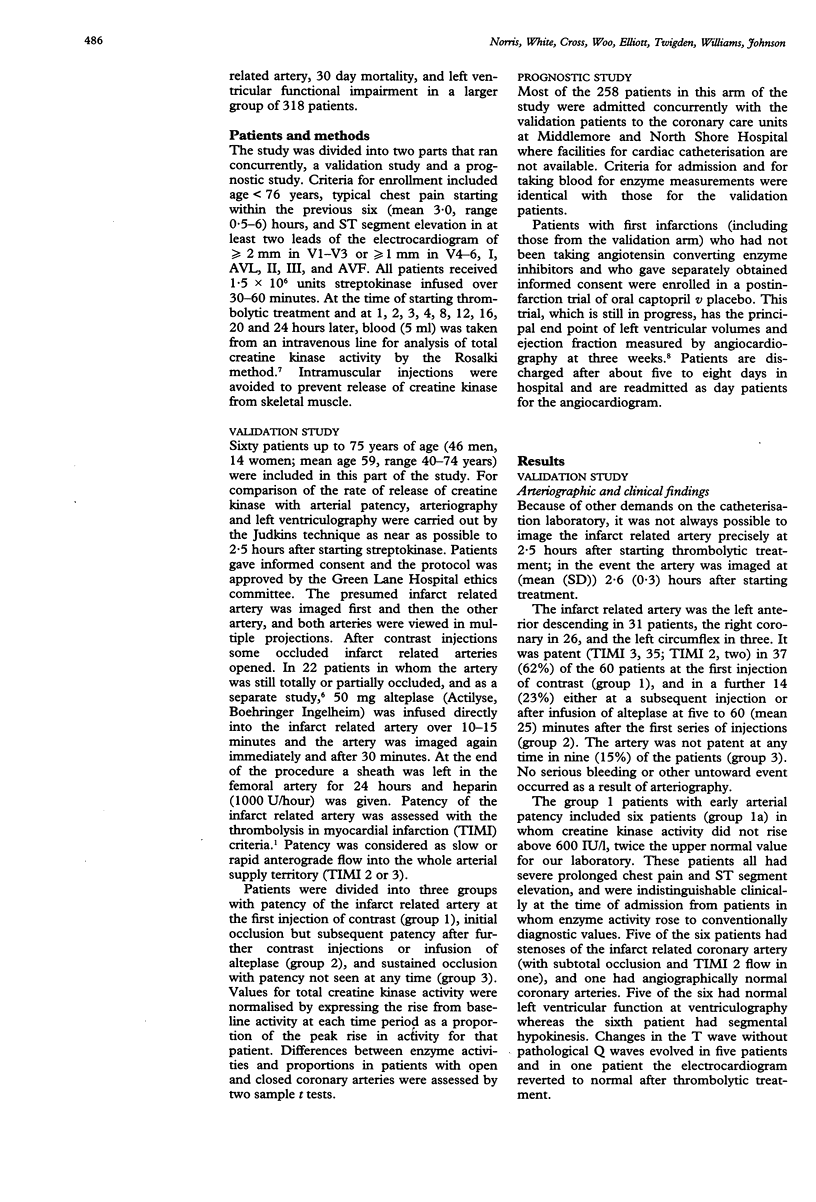
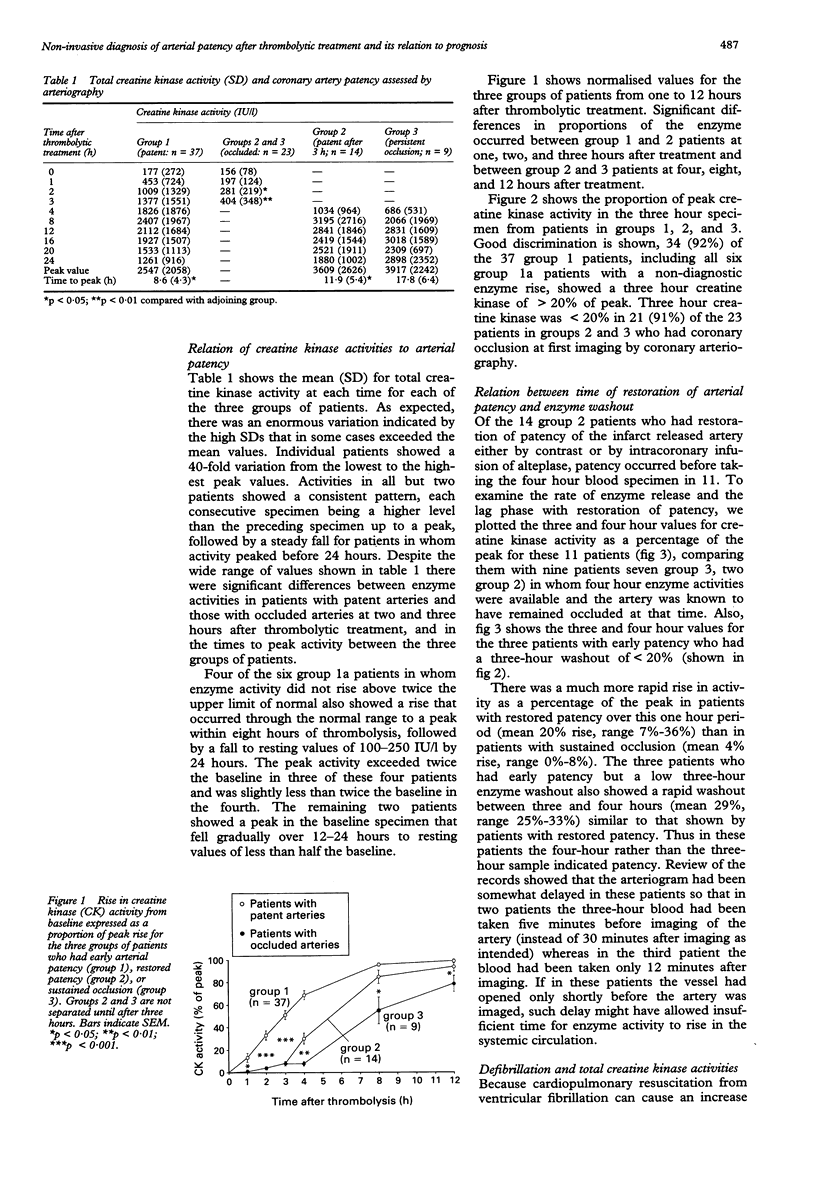
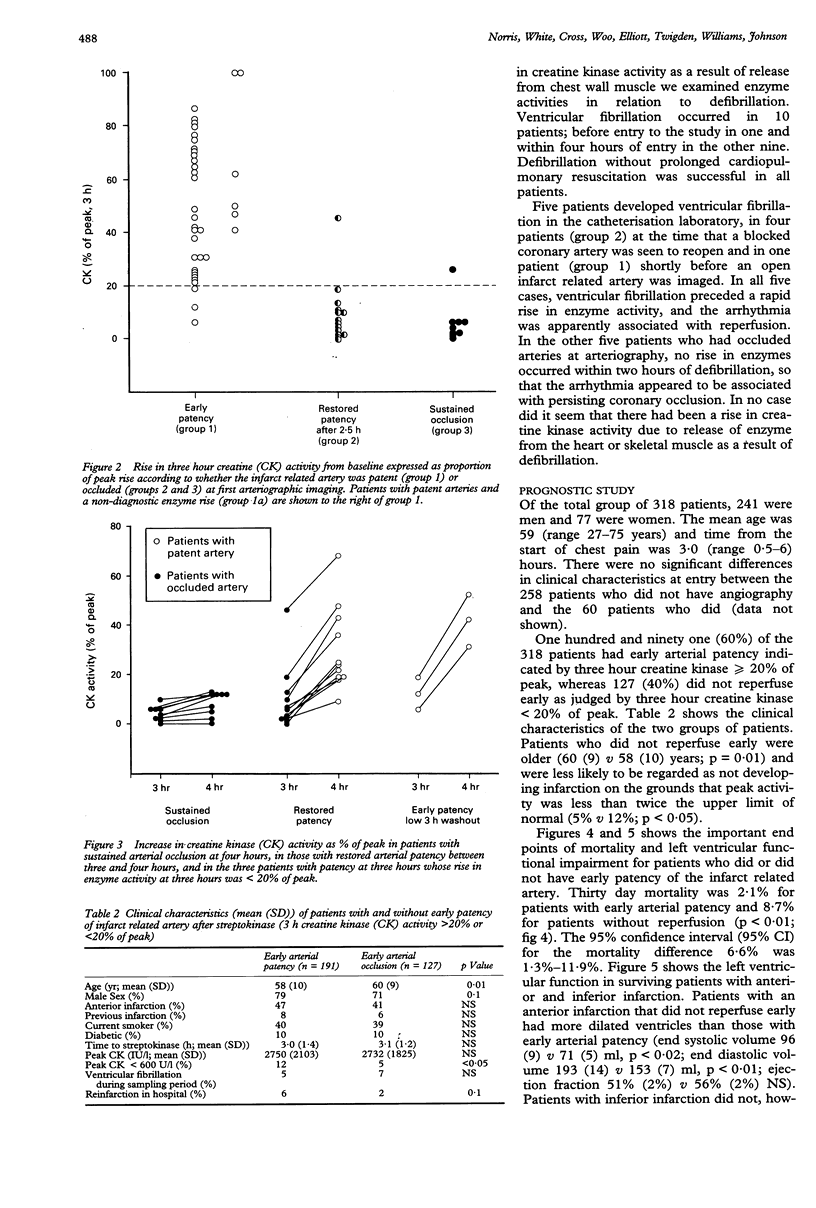
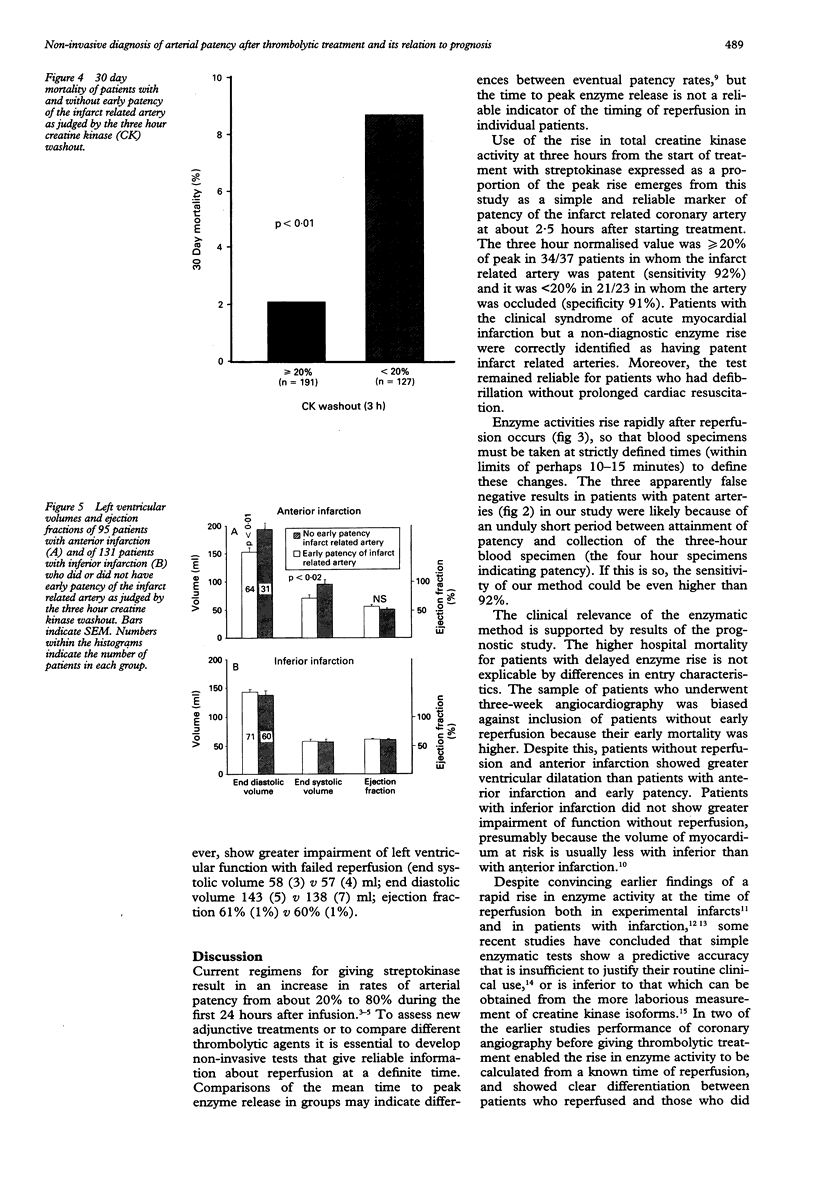
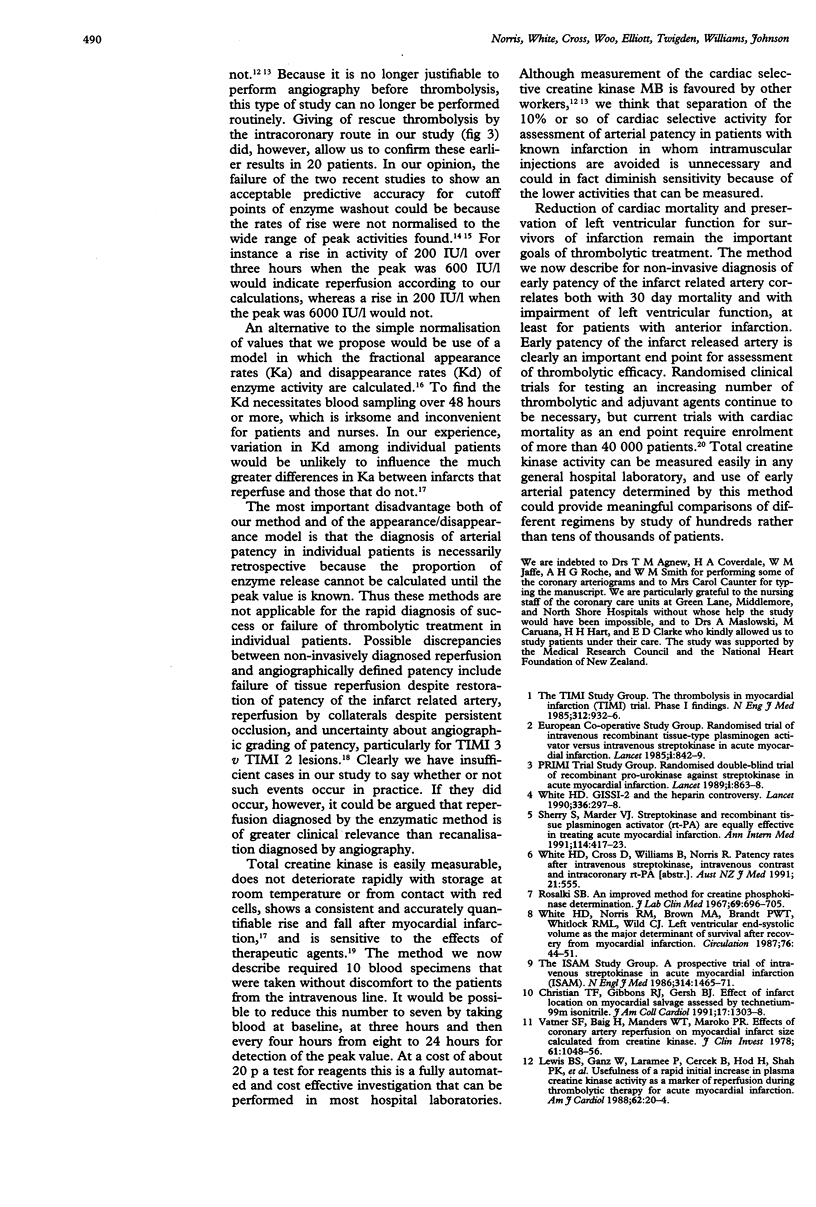
OBJECTIVE--To validate a simple noninvasive method with serial creatine kinase measurements for diagnosis of early patency of the infarct related artery after thrombolytic treatment with streptokinase. To investigate the relation between early patency of the infarct related artery and prognosis. DESIGN--Patients under 76 years of age and seen within six hours of the start of prolonged chest pain and ST segment elevation were treated with streptokinase (1.5 x 10(6) U) intravenously over 30-60 minutes. Blood for measurement of total creatine kinase activity was taken at baseline and at 1, 2, 3, 4, 8, 12, 16, 20, and 24 hours after starting treatment. The rise in enzyme activity at each time from baseline was expressed as a proportion of the total rise from baseline to peak. PATIENTS--Patients studied were in the following groups: (a) Sixty patients took part in a validation study with angiographic determination of patency of the infarct related coronary artery at 2.6 (0.3) hours (mean (SD)) after starting streptokinase. (b) A further 258 patients did not have early arteriography, but data were added to those from the 60 validation patients to find the relation between enzymatically determined early patency of the infarct related artery and 30 day mortality. (c) A further subset of 232 patients with first infarctions (including patients from groups (a) and (b) had angiocardiography at three weeks after infarction, and data were used to investigate the relation between early patency of the infarct related artery and left ventricular function. MAIN OUTCOME MEASURES--Normalised rate of rise of creatine kinase activity at three hours after starting streptokinase in relation to angiographic patency of the infarct related coronary artery at 2.5 hours; 30 day cardiac mortality; and left ventricular function at three weeks in survivors of first infarction. RESULTS--In the validation study, a rise in three hour creatine kinase activity of > 20% of peak occurred in 34/37 patients with initially patent infarct related coronary arteries (sensitivity 92%), and a rise to < 20% of peak occurred in 21/23 patients with initially occluded arteries (specificity 91%). In the prognostic study, 30 day mortality was 2.1% in the 191 patients with three hour creatine kinase > 20% of peak and 8.7% in the 127 patients with three hour creatine kinase < 20% of peak (p < 0.01). Angiocardiography in three week survivors of anterior infarction (n = 95) showed better left ventricular function when three hour creatine kinase was > or = 20% than when it was < 20% of peak (mean (SEM) end systolic volume 71 (5) v 96 (9) ml, p < 0.02; ejection fraction 56% (2%) v 51% (2%), NS). CONCLUSION--Non-invasive determination of early patency of the infarct related artery by the normalised rate of rise of creatine kinase activity at three hours seems to be reliable, and may be prognostically important and of value for use in clinical trials.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bosker H. A., van der Laarse A., Cats V. M., Bruschke A. V. Are enzymatic tests good indicators of coronary reperfusion? Br Heart J. 1992 Feb;67(2):150–154. doi: 10.1136/hrt.67.2.150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garabedian H. D., Gold H. K., Yasuda T., Johns J. A., Finkelstein D. M., Gaivin R. J., Cobbaert C., Leinbach R. C., Collen D. Detection of coronary artery reperfusion with creatine kinase-MB determinations during thrombolytic therapy: correlation with acute angiography. J Am Coll Cardiol. 1988 Apr;11(4):729–734. doi: 10.1016/0735-1097(88)90204-5. [DOI] [PubMed] [Google Scholar]
- Karagounis L., Sorensen S. G., Menlove R. L., Moreno F., Anderson J. L. Does thrombolysis in myocardial infarction (TIMI) perfusion grade 2 represent a mostly patent artery or a mostly occluded artery? Enzymatic and electrocardiographic evidence from the TEAM-2 study. Second Multicenter Thrombolysis Trial of Eminase in Acute Myocardial Infarction. J Am Coll Cardiol. 1992 Jan;19(1):1–10. doi: 10.1016/0735-1097(92)90043-m. [DOI] [PubMed] [Google Scholar]
- Karagounis L., Sorensen S. G., Menlove R. L., Moreno F., Anderson J. L. Does thrombolysis in myocardial infarction (TIMI) perfusion grade 2 represent a mostly patent artery or a mostly occluded artery? Enzymatic and electrocardiographic evidence from the TEAM-2 study. Second Multicenter Thrombolysis Trial of Eminase in Acute Myocardial Infarction. J Am Coll Cardiol. 1992 Jan;19(1):1–10. doi: 10.1016/0735-1097(92)90043-m. [DOI] [PubMed] [Google Scholar]
- Lewis B. S., Ganz W., Laramee P., Cercek B., Hod H., Shah P. K., Lew A. S. Usefulness of a rapid initial increase in plasma creatine kinase activity as a marker of reperfusion during thrombolytic therapy for acute myocardial infarction. Am J Cardiol. 1988 Jul 1;62(1):20–24. doi: 10.1016/0002-9149(88)91358-6. [DOI] [PubMed] [Google Scholar]
- Norris R. M., Whitlock R. M., Barratt-Boyes C., Small C. W. Clinical measurement of myocardial infarct size. Modification of a method for the estimation of total creatine phosphokinase release after myocardial infarction. Circulation. 1975 Apr;51(4):614–620. doi: 10.1161/01.cir.51.4.614. [DOI] [PubMed] [Google Scholar]
- Peter T., Norris R. M., Clarke E. D., Heng M. K., Singh B. N., Williams B., Howell D. R., Ambler P. K. Reduction of enzyme levels by propranolol after acute myocardial infarction. Circulation. 1978 Jun;57(6):1091–1095. doi: 10.1161/01.cir.57.6.1091. [DOI] [PubMed] [Google Scholar]
- Rosalki S. B. An improved procedure for serum creatine phosphokinase determination. J Lab Clin Med. 1967 Apr;69(4):696–705. [PubMed] [Google Scholar]
- Schofer J., Ress-Grigolo G., Voigt K. D., Mathey D. G. Early detection of coronary artery patency after thrombolysis by determination of the MM creatine kinase isoforms in patients with acute myocardial infarction. PRIMI Study Group. Am Heart J. 1992 Apr;123(4 Pt 1):846–853. doi: 10.1016/0002-8703(92)90686-p. [DOI] [PubMed] [Google Scholar]
- Sherry S., Marder V. J. Streptokinase and recombinant tissue plasminogen activator (rt-PA) are equally effective in treating acute myocardial infarction. Ann Intern Med. 1991 Mar 1;114(5):417–423. doi: 10.7326/0003-4819-114-5-417. [DOI] [PubMed] [Google Scholar]
- Vatner S. F., Baig H., Manders W. T., Maroko P. R. Effects of coronary artery reperfusion on myocardial infarct size calculated from creatine kinase. J Clin Invest. 1978 Apr;61(4):1048–1056. doi: 10.1172/JCI109004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- White H. D. GISSI-2 and the heparin controversy. Lancet. 1990 Aug 4;336(8710):297–298. doi: 10.1016/0140-6736(90)91818-u. [DOI] [PubMed] [Google Scholar]
- White H. D., Norris R. M., Brown M. A., Brandt P. W., Whitlock R. M., Wild C. J. Left ventricular end-systolic volume as the major determinant of survival after recovery from myocardial infarction. Circulation. 1987 Jul;76(1):44–51. doi: 10.1161/01.cir.76.1.44. [DOI] [PubMed] [Google Scholar]