

Abstract
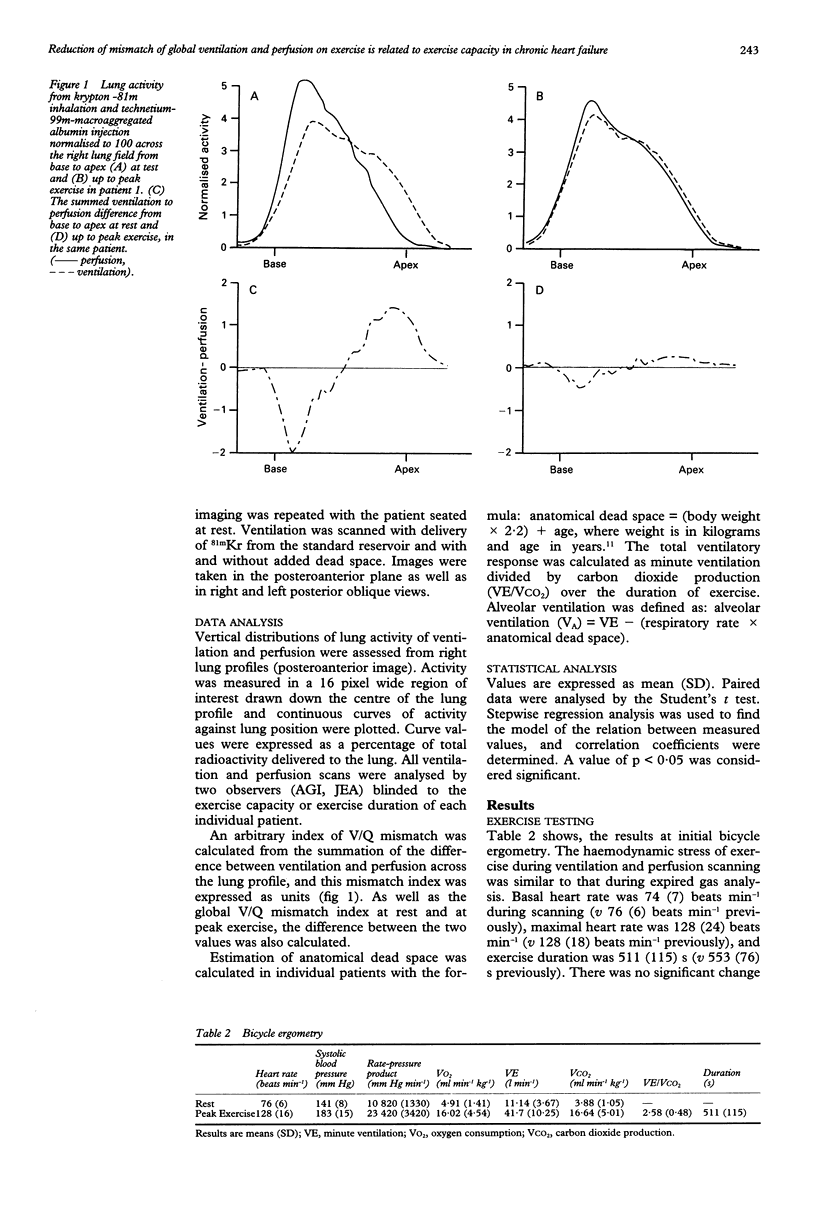
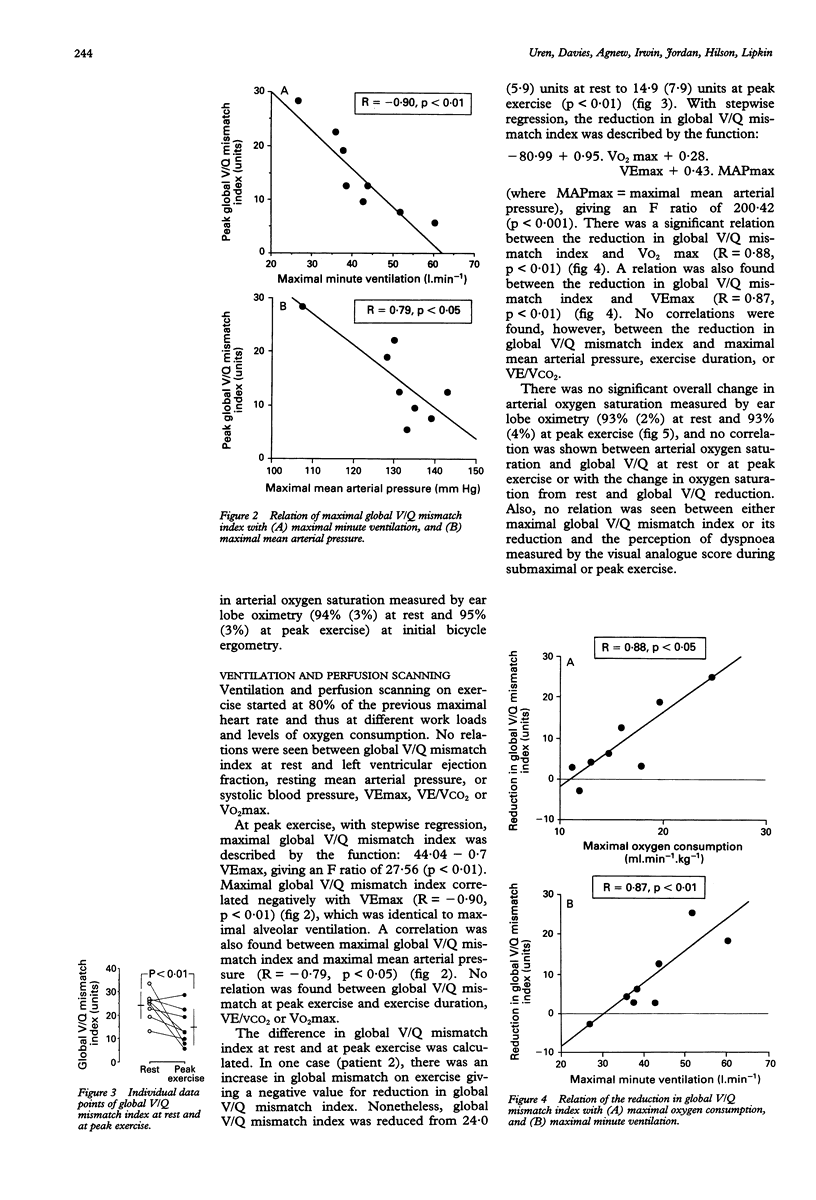
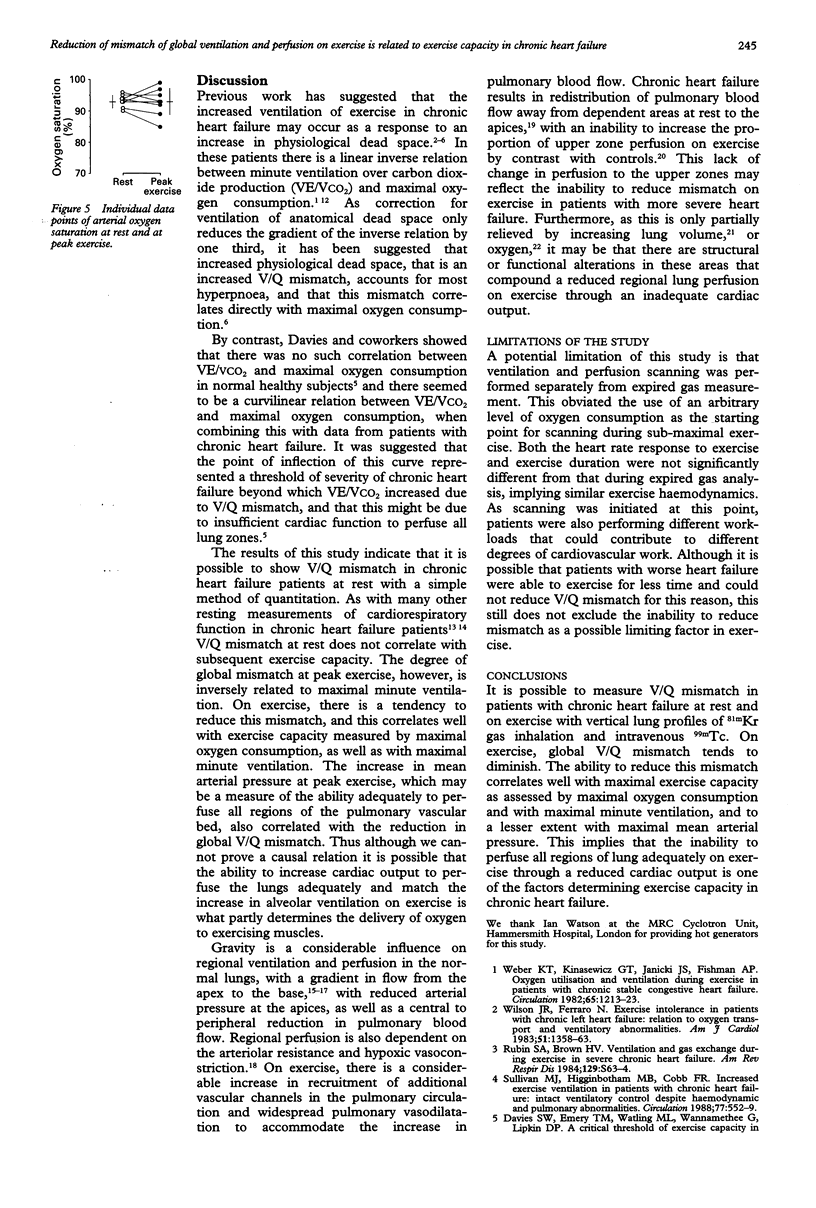
BACKGROUND--The inability to match lung perfusion to ventilation because of a reduced cardiac output on exercise contributes to reduced exercise capacity in chronic heart failure. OBJECTIVE--To quantify ventilation to perfusion matching at rest and at peak exercise in patients with chronic heart failure and relate this to haemodynamic and ventilatory variables of exercise capacity. DESIGN--Eight men in New York Heart Association class II underwent maximal bicycle ergometry with expired gas analysis. MAIN OUTCOME MEASURES--On separate days, ventilation and perfusion gamma camera imaging was performed at rest, and at 80% of previous peak exercise heart rate during bicycle ergometry. The vertical distribution of mismatch between ventilation and perfusion (V/Q) was estimated from subtracted profiles of activity (ventilation and perfusion) to derive a numerical index of global mismatch. RESULTS--Maximal mean (SD) oxygen consumption on bicycle ergometry was 16.0 (4.5) ml min-1 kg-1. There was a reduction in the global V/Q mismatch index from 23.96 (5.90) to 14.88 (7.90) units (p < 0.01) at rest and at peak exercise. Global V/Q mismatch index at peak exercise correlated negatively with maximal minute ventilation (R = -0.90, p < 0.01) and with maximal mean arterial pressure (R = -0.79, p < 0.05), although no relation was seen with maximal oxygen consumption. The reduction in global V/Q mismatch index from rest to peak exercise correlated with maximal oxygen consumption (R = 0.88, p < 0.01), and with maximal minute ventilation (R = 0.87, p < 0.01). CONCLUSIONS--During exercise in patients with chronic heart failure, there is a reduction in the global V/Q mismatch index. A lower global V/Q mismatch index at peak exercise is associated with higher maximal ventilation. The reduction in global V/Q mismatch index on exercise correlates well with maximal exercise capacity. This may imply that the inability to perfuse adequately all regions of lung on exercise and match this to ventilation is a factor determining exercise capacity in chronic heart failure.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Amis T. C., Jones H. A., Hughes J. M. Effect of posture on inter-regional distribution of pulmonary perfusion and VA/Q ratios in man. Respir Physiol. 1984 May;56(2):169–182. doi: 10.1016/0034-5687(84)90101-4. [DOI] [PubMed] [Google Scholar]
- Amis T. C., Jones H. A., Hughes J. M. Effect of posture on inter-regional distribution of pulmonary ventilation in man. Respir Physiol. 1984 May;56(2):145–167. doi: 10.1016/0034-5687(84)90100-2. [DOI] [PubMed] [Google Scholar]
- Buller N. P., Poole-Wilson P. A. Mechanism of the increased ventilatory response to exercise in patients with chronic heart failure. Br Heart J. 1990 May;63(5):281–283. doi: 10.1136/hrt.63.5.281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DAWSON A., KANEKO K., MCGREGOR M. REGIONAL LUNG FUNCTION IN PATIENTS WITH MITRAL STENOSIS STUDIED WITH XENON-133 DURING AIR AND OXYGEN BREATHING. J Clin Invest. 1965 Jun;44:999–1008. doi: 10.1172/JCI105217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davies N. J., Denison D. M. The measurement of metabolic gas exchange and minute volume by mass spectrometry alone. Respir Physiol. 1979 Feb;36(2):261–267. doi: 10.1016/0034-5687(79)90029-x. [DOI] [PubMed] [Google Scholar]
- Fazio F., Jones T. Assessment of regional ventilation by continuous inhalation of radioactive krypton-81m. Br Med J. 1975 Sep 20;3(5985):673–676. doi: 10.1136/bmj.3.5985.673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fink L. I., Wilson J. R., Ferraro N. Exercise ventilation and pulmonary artery wedge pressure in chronic stable congestive heart failure. Am J Cardiol. 1986 Feb 1;57(4):249–253. doi: 10.1016/0002-9149(86)90900-8. [DOI] [PubMed] [Google Scholar]
- Friedman W. F., Braunwald E. Alterations in regional pulmonary blood flow in mitral valve disease studied by radioisotope scanning. A simple nontraumatic technique for estimation of left atrial pressure. Circulation. 1966 Sep;34(3):363–376. doi: 10.1161/01.cir.34.3.363. [DOI] [PubMed] [Google Scholar]
- Harf A., Pratt T., Hughes J. M. Regional distribution of VA/Q in man at rest and with exercise measured with krypton-81m. J Appl Physiol Respir Environ Exerc Physiol. 1978 Jan;44(1):115–123. doi: 10.1152/jappl.1978.44.1.115. [DOI] [PubMed] [Google Scholar]
- Higginbotham M. B., Morris K. G., Conn E. H., Coleman R. E., Cobb F. R. Determinants of variable exercise performance among patients with severe left ventricular dysfunction. Am J Cardiol. 1983 Jan 1;51(1):52–60. doi: 10.1016/s0002-9149(83)80010-1. [DOI] [PubMed] [Google Scholar]
- Hughes J. M., Glazier J. B., Rosenzweig D. Y., West J. B. Factors determining the distribution of pulmonary blood flow in patients with raised pulmonary venous pressure. Clin Sci. 1969 Dec;37(3):847–858. [PubMed] [Google Scholar]
- Mohsenifar Z., Amin D. K., Shah P. K. Regional distribution of lung perfusion and ventilation in patients with chronic congestive heart failure and its relationship to cardiopulmonary hemodynamics. Am Heart J. 1989 Apr;117(4):887–891. doi: 10.1016/0002-8703(89)90628-5. [DOI] [PubMed] [Google Scholar]
- Rubin S. A., Brown H. V. Ventilation and gas exchange during exercise in severe chronic heart failure. Am Rev Respir Dis. 1984 Feb;129(2 Pt 2):S63–S64. doi: 10.1164/arrd.1984.129.2P2.S63. [DOI] [PubMed] [Google Scholar]
- Sullivan M. J., Higginbotham M. B., Cobb F. R. Increased exercise ventilation in patients with chronic heart failure: intact ventilatory control despite hemodynamic and pulmonary abnormalities. Circulation. 1988 Mar;77(3):552–559. doi: 10.1161/01.cir.77.3.552. [DOI] [PubMed] [Google Scholar]
- Sullivan M. J., Knight J. D., Higginbotham M. B., Cobb F. R. Relation between central and peripheral hemodynamics during exercise in patients with chronic heart failure. Muscle blood flow is reduced with maintenance of arterial perfusion pressure. Circulation. 1989 Oct;80(4):769–781. doi: 10.1161/01.cir.80.4.769. [DOI] [PubMed] [Google Scholar]
- Weber K. T., Kinasewitz G. T., Janicki J. S., Fishman A. P. Oxygen utilization and ventilation during exercise in patients with chronic cardiac failure. Circulation. 1982 Jun;65(6):1213–1223. doi: 10.1161/01.cir.65.6.1213. [DOI] [PubMed] [Google Scholar]
- Williams S. A., Boolell M., MacGregor G. A., Smaje L. H., Wasserman S. M., Tooke J. E. Capillary hypertension and abnormal pressure dynamics in patients with essential hypertension. Clin Sci (Lond) 1990 Jul;79(1):5–8. doi: 10.1042/cs0790005. [DOI] [PubMed] [Google Scholar]
- Wilson J. R., Ferraro N. Exercise intolerance in patients with chronic left heart failure: relation to oxygen transport and ventilatory abnormalities. Am J Cardiol. 1983 May 1;51(8):1358–1363. doi: 10.1016/0002-9149(83)90312-0. [DOI] [PubMed] [Google Scholar]