

Abstract
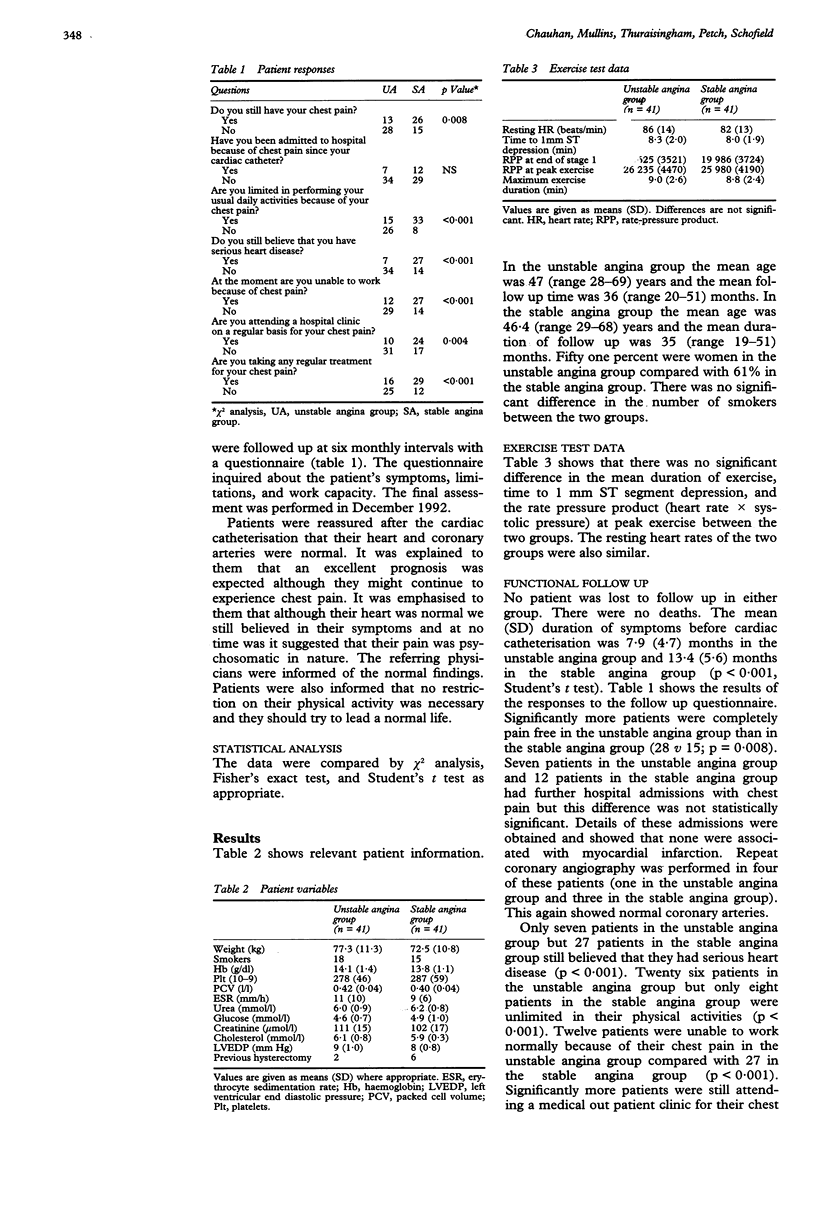
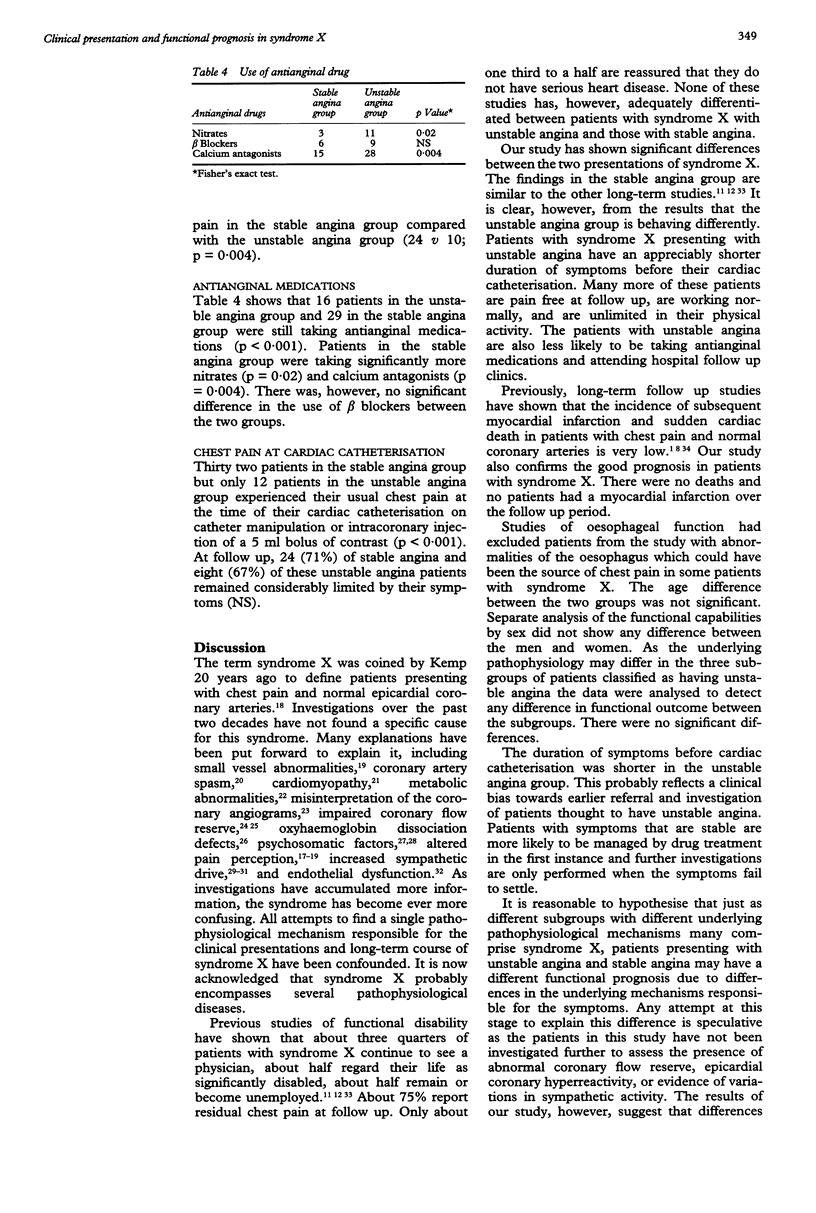
OBJECTIVES--To assess the effect of clinical presentation on functional prognosis in patients with syndrome X. DESIGN--A prospective study. Patients with syndrome X presenting with unstable angina and stable angina were followed up with a questionnaire to examine their functional state. PATIENTS--41 patients with syndrome X and unstable angina and 41 patients with syndrome X and stable angina. Syndrome X was defined as typical anginal chest pain, a positive exercise test, and normal coronary angiogram. SETTING--Regional cardiothoracic centre. RESULTS--The mean follow up time was 36 (range 20-51) months for the unstable angina group and 35 (range 19-51) months for the stable angina group. No patient was lost to follow up in either group. At follow up 28 patients in the unstable angina group were pain free compared with 15 patients in the stable angina group (p = 0.008). Seven patients in the unstable angina group had further hospital admission with chest pain after the cardiac catheterisation compared wtih 12 patients in the stable angina group (NS). Seven patients in the unstable angina group believed that they had heart disease compared with 27 in the stable angina group (p < 0.001). 26 patients in the unstable angina group but only eight patients in the stable angina group were unlimited in their physical activity (p < 0.001). 12 patients in the unstable angina group compared with 27 patients in the stable angina group were unable to work normally because of chest pain (p < 0.001). The mean (SD) duration of symptoms before cardiac catheterisation was 7.9 (4.7) months in the unstable angina group and 13.4 (5.6) months in the stable angina group (p < 0.001). 10 patients in the unstable angina group and 24 patients in the stable angina group still attended hospital outpatient clinics because of chest pain (p = 0.004). 16 patients in the unstable angina group and 29 patients in the stable angina group were still taking regular antianginal medication (p < 0.001). CONCLUSIONS--Patients with syndrome X who present with unstable angina have a significantly better functional prognosis than those presenting with symptoms of stable angina. This may reflect differences in underlying pathophysiological mechanisms.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Alison H. W., Russell R. O., Jr, Mantle J. A., Kouchoukos N. T., Moraski R. E., Rackley C. E. Coronary anatomy and arteriography in patients with unstable angina pectoris. Am J Cardiol. 1978 Feb;41(2):204–209. doi: 10.1016/0002-9149(78)90157-1. [DOI] [PubMed] [Google Scholar]
- Bass C., Wade C. Chest pain with normal coronary arteries: a comparative study of psychiatric and social morbidity. Psychol Med. 1984 Feb;14(1):51–61. doi: 10.1017/s003329170000307x. [DOI] [PubMed] [Google Scholar]
- Bass C., Wade C., Hand D., Jackson G. Patients with angina with normal and near normal coronary arteries: clinical and psychosocial state 12 months after angiography. Br Med J (Clin Res Ed) 1983 Nov 19;287(6404):1505–1508. doi: 10.1136/bmj.287.6404.1505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boden W. E., Bough E. W., Korr K. S., Benham I., Gheorghiade M., Caputi A., Shulman R. S. Exercise-induced coronary spasm with S-T segment depression and normal coronary arteriography. Am J Cardiol. 1981 Jul;48(1):193–197. doi: 10.1016/0002-9149(81)90591-9. [DOI] [PubMed] [Google Scholar]
- Boudoulas H., Cobb T. C., Leighton R. F., Wilt S. M. Myocardial lactate production in patients with angina-like chest pain and angiographically normal coronary arteries and left ventricle. Am J Cardiol. 1974 Oct 3;34(5):501–505. doi: 10.1016/0002-9149(74)90118-0. [DOI] [PubMed] [Google Scholar]
- Bugiardini R., Borghi A., Biagetti L., Puddu P. Comparison of verapamil versus propranolol therapy in syndrome X. Am J Cardiol. 1989 Feb 1;63(5):286–290. doi: 10.1016/0002-9149(89)90332-9. [DOI] [PubMed] [Google Scholar]
- Cannon R. O., 3rd, Camici P. G., Epstein S. E. Pathophysiological dilemma of syndrome X. Circulation. 1992 Mar;85(3):883–892. doi: 10.1161/01.cir.85.3.883. [DOI] [PubMed] [Google Scholar]
- Cannon R. O., 3rd, Epstein S. E. "Microvascular angina" as a cause of chest pain with angiographically normal coronary arteries. Am J Cardiol. 1988 Jun 1;61(15):1338–1343. doi: 10.1016/0002-9149(88)91180-0. [DOI] [PubMed] [Google Scholar]
- Cannon R. O., 3rd, Quyyumi A. A., Schenke W. H., Fananapazir L., Tucker E. E., Gaughan A. M., Gracely R. H., Cattau E. L., Jr, Epstein S. E. Abnormal cardiac sensitivity in patients with chest pain and normal coronary arteries. J Am Coll Cardiol. 1990 Nov;16(6):1359–1366. doi: 10.1016/0735-1097(90)90377-2. [DOI] [PubMed] [Google Scholar]
- Day L. J., Sowton E. Clinical features and follow-up of patients with angina and normal coronary arteries. Lancet. 1976 Aug 14;2(7981):334–337. doi: 10.1016/s0140-6736(76)92591-5. [DOI] [PubMed] [Google Scholar]
- Eliot R. S., Bratt G. The paradox of myocardial ischemia and necrosis in young women with normal coronary anteriograms. Relation to abnormal hemoglobin-oxygen dissociation. Am J Cardiol. 1969 May;23(5):633–638. doi: 10.1016/0002-9149(69)90023-x. [DOI] [PubMed] [Google Scholar]
- Galassi A. R., Kaski J. C., Crea F., Pupita G., Gavrielides S., Tousoulis D., Maseri A. Heart rate response during exercise testing and ambulatory ECG monitoring in patients with syndrome X. Am Heart J. 1991 Aug;122(2):458–463. doi: 10.1016/0002-8703(91)91000-d. [DOI] [PubMed] [Google Scholar]
- Isner J. M., Salem D. N., Banas J. S., Jr, Levine H. J. Long-term clinical course of patients with normal coronary arteriography: follow-up study of 121 patients with normal or nearly normal coronary arteriograms. Am Heart J. 1981 Oct;102(4):645–653. doi: 10.1016/0002-8703(81)90088-0. [DOI] [PubMed] [Google Scholar]
- James T. M. Angina without coronary disease (sic). Circulation. 1970 Aug;42(2):189–191. doi: 10.1161/01.cir.42.2.189. [DOI] [PubMed] [Google Scholar]
- Kemp H. G., Jr Left ventricular function in patients with the anginal syndrome and normal coronary arteriograms. Am J Cardiol. 1973 Sep 7;32(3):375–376. doi: 10.1016/s0002-9149(73)80150-x. [DOI] [PubMed] [Google Scholar]
- Kemp H. G., Jr, Vokonas P. S., Cohn P. F., Gorlin R. The anginal syndrome associated with normal coronary arteriograms. Report of a six year experience. Am J Med. 1973 Jun;54(6):735–742. doi: 10.1016/0002-9343(73)90060-0. [DOI] [PubMed] [Google Scholar]
- Kemp H. G., Jr, Vokonas P. S., Cohn P. F., Gorlin R. The anginal syndrome associated with normal coronary arteriograms. Report of a six year experience. Am J Med. 1973 Jun;54(6):735–742. doi: 10.1016/0002-9343(73)90060-0. [DOI] [PubMed] [Google Scholar]
- Lantinga L. J., Sprafkin R. P., McCroskery J. H., Baker M. T., Warner R. A., Hill N. E. One-year psychosocial follow-up of patients with chest pain and angiographically normal coronary arteries. Am J Cardiol. 1988 Aug 1;62(4):209–213. doi: 10.1016/0002-9149(88)90213-5. [DOI] [PubMed] [Google Scholar]
- Lavey E. B., Winkle R. A. Continuing disability of patients with chest pain and normal coronary arteriograms. J Chronic Dis. 1979;32(3):191–196. doi: 10.1016/0021-9681(79)90064-x. [DOI] [PubMed] [Google Scholar]
- Maseri A., Crea F., Kaski J. C., Crake T. Mechanisms of angina pectoris in syndrome X. J Am Coll Cardiol. 1991 Feb;17(2):499–506. doi: 10.1016/s0735-1097(10)80122-6. [DOI] [PubMed] [Google Scholar]
- Maseri A. Pathogenetic classifications of unstable angina as a guideline to individual patient management and prognosis. Am J Med. 1986 Apr 30;80(4C):48–55. doi: 10.1016/0002-9343(86)90452-3. [DOI] [PubMed] [Google Scholar]
- Mosseri M., Yarom R., Gotsman M. S., Hasin Y. Histologic evidence for small-vessel coronary artery disease in patients with angina pectoris and patent large coronary arteries. Circulation. 1986 Nov;74(5):964–972. doi: 10.1161/01.cir.74.5.964. [DOI] [PubMed] [Google Scholar]
- Ockene I. S., Shay M. J., Alpert J. S., Weiner B. H., Dalen J. E. Unexplained chest pain in patients with normal coronary arteriograms: a follow-up study of functional status. N Engl J Med. 1980 Nov 27;303(22):1249–1252. doi: 10.1056/NEJM198011273032201. [DOI] [PubMed] [Google Scholar]
- Opherk D., Zebe H., Weihe E., Mall G., Dürr C., Gravert B., Mehmel H. C., Schwarz F., Kübler W. Reduced coronary dilatory capacity and ultrastructural changes of the myocardium in patients with angina pectoris but normal coronary arteriograms. Circulation. 1981 Apr;63(4):817–825. doi: 10.1161/01.cir.63.4.817. [DOI] [PubMed] [Google Scholar]
- Papanicolaou M. N., Califf R. M., Hlatky M. A., McKinnis R. A., Harrell F. E., Jr, Mark D. B., McCants B., Rosati R. A., Lee K. L., Pryor D. B. Prognostic implications of angiographically normal and insignificantly narrowed coronary arteries. Am J Cardiol. 1986 Dec 1;58(13):1181–1187. doi: 10.1016/0002-9149(86)90378-4. [DOI] [PubMed] [Google Scholar]
- Pasternac A., Bourassa M. G. Pathogenesis of chest pain in patients with cardiomyopathies and normal coronary arteries. Int J Cardiol. 1983 Jun;3(3):273–280. doi: 10.1016/0167-5273(83)90168-7. [DOI] [PubMed] [Google Scholar]
- Pasternak R. C., Thibault G. E., Savoia M., DeSanctis R. W., Hutter A. M., Jr Chest pain with angiographically insignificant coronary arterial obstruction. Clinical presentation and long-term follow-up. Am J Med. 1980 Jun;68(6):813–817. doi: 10.1016/0002-9343(80)90199-0. [DOI] [PubMed] [Google Scholar]
- Plotnick G. D., Greene H. L., Carliner N. H., Becker L. C., Fisher M. L. Clinical indicators of left main coronary artery disease in unstable angina. Ann Intern Med. 1979 Aug;91(2):149–153. doi: 10.7326/0003-4819-91-2-149. [DOI] [PubMed] [Google Scholar]
- Proudfit W. L., Shirey E. K., Sones F. M., Jr Selective cine coronary arteriography. Correlation with clinical findings in 1,000 patients. Circulation. 1966 Jun;33(6):901–910. doi: 10.1161/01.cir.33.6.901. [DOI] [PubMed] [Google Scholar]
- Quyyumi A. A., Cannon R. O., 3rd, Panza J. A., Diodati J. G., Epstein S. E. Endothelial dysfunction in patients with chest pain and normal coronary arteries. Circulation. 1992 Dec;86(6):1864–1871. doi: 10.1161/01.cir.86.6.1864. [DOI] [PubMed] [Google Scholar]
- Romeo F., Gaspardone A., Ciavolella M., Gioffrè P., Reale A. Verapamil versus acebutolol for syndrome X. Am J Cardiol. 1988 Aug 1;62(4):312–313. doi: 10.1016/0002-9149(88)90232-9. [DOI] [PubMed] [Google Scholar]
- Selzer A. Cardiac ischemic pain in patients with normal coronary arteriograms. Am J Med. 1977 Nov;63(5):661–665. doi: 10.1016/0002-9343(77)90149-8. [DOI] [PubMed] [Google Scholar]
- Shapiro L. M., Crake T., Poole-Wilson P. A. Is altered cardiac sensation responsible for chest pain in patients with normal coronary arteries? Clinical observation during cardiac catheterisation. Br Med J (Clin Res Ed) 1988 Jan 16;296(6616):170–171. doi: 10.1136/bmj.296.6616.170-a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Turiel M., Galassi A. R., Glazier J. J., Kaski J. C., Maseri A. Pain threshold and tolerance in women with syndrome X and women with stable angina pectoris. Am J Cardiol. 1987 Sep 1;60(7):503–507. doi: 10.1016/0002-9149(87)90294-3. [DOI] [PubMed] [Google Scholar]