

Abstract
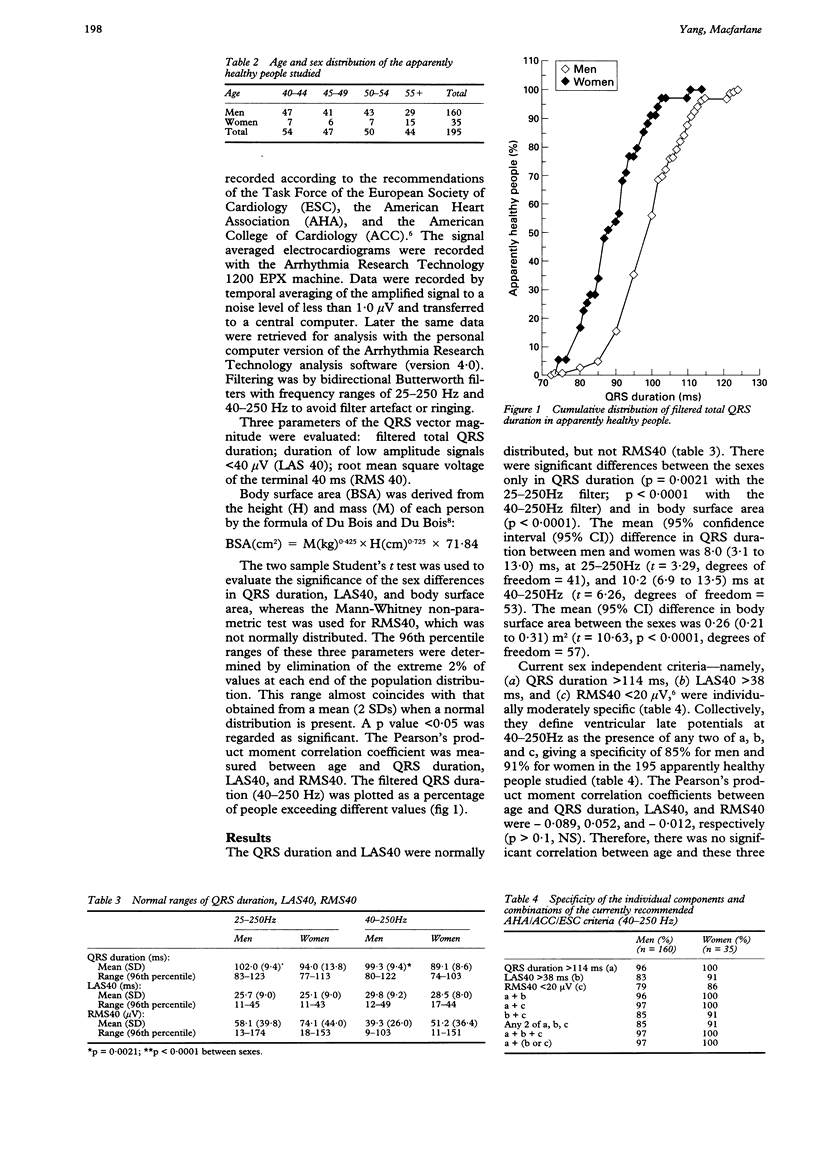
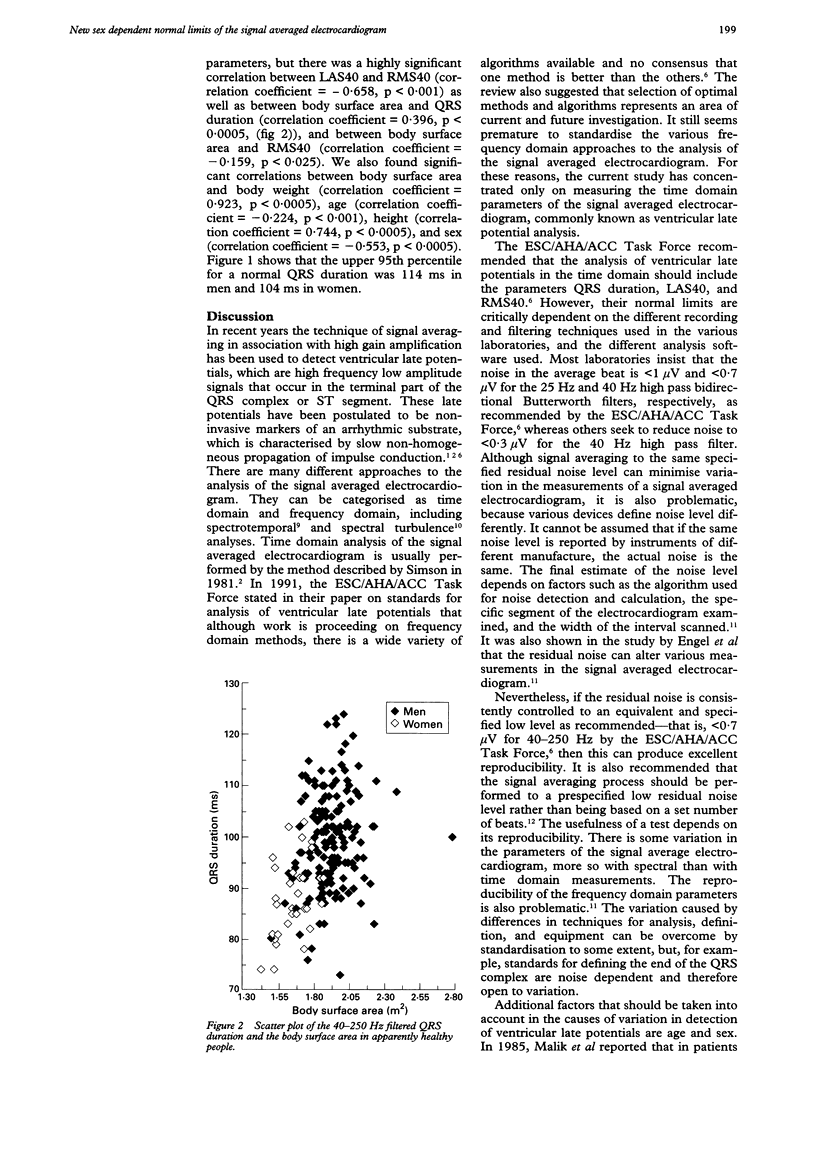
BACKGROUND--An earlier study of 1555 normal 12 lead electrocardiograms has shown that the mean QRS duration in men is 8 ms longer than in women. OBJECTIVE--To establish the sex related normal limits of the signal averaged electrocardiogram. PEOPLE--195 people (160 men and 35 women aged 40 to 69) with normal clinical history, physical examination, 12 lead electrocardiogram, and echocardiogram were recruited for this study. METHODS--Signal averaged electrocardiograms were recorded by the Arrhythmia Research Technology 1200 EPX machine and analysed twice with bidirectional Butterworth filters with frequency ranges of 25-250 Hz and 40-250 Hz. Three time domain parameters of the QRS vector magnitude, namely filtered total QRS duration, duration of low amplitude signals under 40 microV (LAS40), and root mean square voltage of the last 40 ms (RMS40), were evaluated. RESULTS--There were significant differences between the two sexes in QRS duration (mean (95% confidence interval (95% CI) (8.0 (3.1 to 13.0) ms, t = 3.29, degrees of freedom = 41, p = 0.0021 with the 25-250Hz filter; mean (95% CI) 10.2 (6.9 to 13.5) ms, t = 6.26, degrees of freedom = 53, p < 0.0001 with the 40-250Hz filter)) and in body surface area (mean (95% CI) 0.26 (0.21 to 0.31) m2, t = 10.63, degrees of freedom = 57). There was no significant correlation between age and QRS duration, LAS40, or RMS40, but there was a highly significant correlation between body surface area and QRS duration (correlation coefficient = 0.396, p < 0.0005) and RMS40 (correlation coefficient = -0.159, p < 0.025). Current sex independent criteria defining ventricular late potentials as the presence of any two of QRS duration > 114 ms, LAS40 > 38 ms, RMS40 < 20 microV, give a specificity of 85% for men and 91% for women in this normal population. RECOMMENDATIONS--Ventricular late potentials should be regarded as present when (a) QRS duration exceeds 114 ms in men or 104 ms in women and (b) either LAS40 > 38 ms or RMS40 < 20 microV. This gives a specificity of 97% in men and 100% in women in the population studied.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Breithardt G., Cain M. E., el-Sherif N., Flowers N., Hombach V., Janse M., Simson M. B., Steinbeck G. Standards for analysis of ventricular late potentials using high resolution or signal-averaged electrocardiography. A statement by a Task Force Committee between the European Society of Cardiology, the American Heart Association and the American College of Cardiology. Eur Heart J. 1991 Apr;12(4):473–480. doi: 10.1093/oxfordjournals.eurheartj.a059926. [DOI] [PubMed] [Google Scholar]
- Coto H., Maldonado C., Palakurthy P., Flowers N. C. Late potentials in normal subjects and in patients with ventricular tachycardia unrelated to myocardial infarction. Am J Cardiol. 1985 Feb 1;55(4):384–390. doi: 10.1016/0002-9149(85)90381-9. [DOI] [PubMed] [Google Scholar]
- Cripps T. R., Counihan P. J., Frenneaux M. P., Ward D. E., Camm A. J., McKenna W. J. Signal-averaged electrocardiography in hypertrophic cardiomyopathy. J Am Coll Cardiol. 1990 Apr;15(5):956–961. doi: 10.1016/0735-1097(90)90223-c. [DOI] [PubMed] [Google Scholar]
- Engel T. R., Pierce D. L., Murphy S. P. Variation in late potentials and the reproducibility of their measurement. Prog Cardiovasc Dis. 1993 Jan-Feb;35(4):247–262. doi: 10.1016/0033-0620(93)90006-y. [DOI] [PubMed] [Google Scholar]
- Jarrett J. R., Flowers N. C. Signal-averaged electrocardiography: history, techniques, and clinical applications. Clin Cardiol. 1991 Dec;14(12):984–994. doi: 10.1002/clc.4960141209. [DOI] [PubMed] [Google Scholar]
- Kelen G. J., Henkin R., Starr A. M., Caref E. B., Bloomfield D., el-Sherif N. Spectral turbulence analysis of the signal-averaged electrocardiogram and its predictive accuracy for inducible sustained monomorphic ventricular tachycardia. Am J Cardiol. 1991 May 1;67(11):965–975. doi: 10.1016/0002-9149(91)90169-l. [DOI] [PubMed] [Google Scholar]
- Kitzman D. W., Scholz D. G., Hagen P. T., Ilstrup D. M., Edwards W. D. Age-related changes in normal human hearts during the first 10 decades of life. Part II (Maturity): A quantitative anatomic study of 765 specimens from subjects 20 to 99 years old. Mayo Clin Proc. 1988 Feb;63(2):137–146. doi: 10.1016/s0025-6196(12)64946-5. [DOI] [PubMed] [Google Scholar]
- Lander P., Albert D. E., Berbari E. J. Spectrotemporal analysis of ventricular late potentials. J Electrocardiol. 1990 Apr;23(2):95–108. doi: 10.1016/0022-0736(90)90131-k. [DOI] [PubMed] [Google Scholar]
- Malik M., Odemuyiwa O., Poloniecki J., Kulakowski P., Farrell T., Staunton A., Camm A. J. Age-related normal values of signal-averaged electrocardiographic variables after acute myocardial infarction. Am J Cardiol. 1991 Aug 15;68(5):440–445. doi: 10.1016/0002-9149(91)90775-g. [DOI] [PubMed] [Google Scholar]
- Simson M. B. Use of signals in the terminal QRS complex to identify patients with ventricular tachycardia after myocardial infarction. Circulation. 1981 Aug;64(2):235–242. doi: 10.1161/01.cir.64.2.235. [DOI] [PubMed] [Google Scholar]
- Steinberg J. S., Bigger J. T., Jr Importance of the endpoint of noise reduction in analysis of the signal-averaged electrocardiogram. Am J Cardiol. 1989 Mar 1;63(9):556–560. doi: 10.1016/0002-9149(89)90898-9. [DOI] [PubMed] [Google Scholar]