

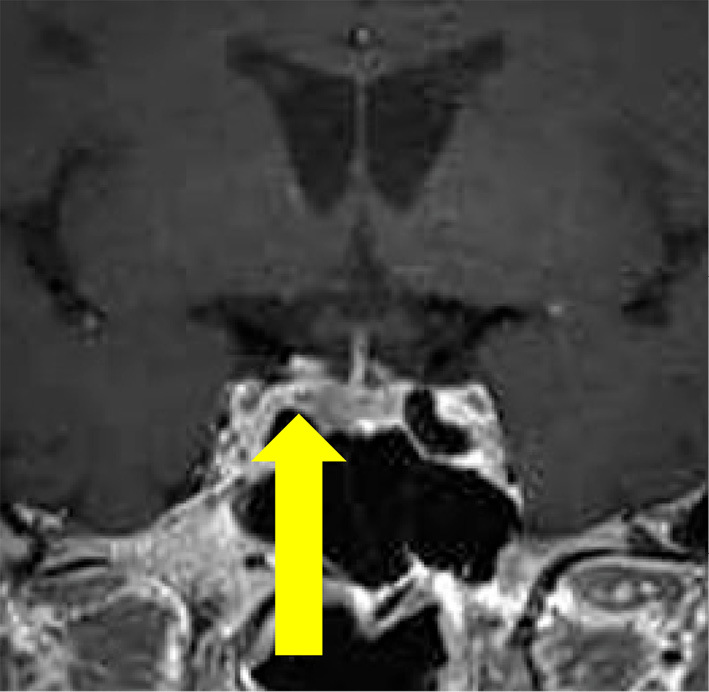
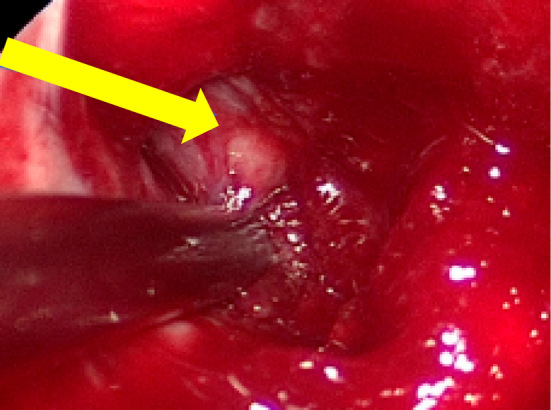
A 34-year-old man presented with hypokalemia (minimum, 2.3 mEq/L) for 3 months after remission of gastroenteritis. He has been treated for hypertension with amlodipine at 10 mg/day and irbesartan at 100 mg/day for 8 years. He had central obesity and red abdominal striae. Elevated levels of plasma adrenocorticotropic hormone (ACTH) at 68.9 pg/mL (reference range: 7.2-63.3), serum cortisol at 25.2 μg/dL (7.1-19.6), and 24-h urine cortisol at 164.4 μg/day (11.2-80.3) were observed. Diurnal variation of cortisol was lost. A normal response was obtained in the corticotropin releasing hormone stimulation test. Low-dose (0.5 mg) dexamethasone did not suppress the cortisol level, but high-dose (8 mg) dexamethasone did suppress it. Pituitary magnetic resonance imaging showed a poorly enhanced lesion (2×2 mm) adjacent to the pituitary gland (Picture 1, arrow). The inferior petrosal sinus sampling test showed the right predominance of ACTH secretion. The tumor was located within the right cavernous sinus and separated from the normal pituitary gland by the cavernous sinus medial wall (Picture 2, arrow). After the removal of the tumor, the hypokalemia improved. A histopathological examination revealed the pseudorosette arrangement of basophilic cells (Picture 3A Hematoxylin and Eosin staining), positive immunoreactivity for ACTH (Picture 3B), and a Ki-67 index of 1% (Picture 3C), consistent with ectopic ACTH-secreting pituitary neuroendocrine tumor (EA-PitNET). EA-PitNET is an extremely rare entity that is often overlooked (1,2). In cases of persistent hypokalemia and the absence of an obvious tumor in the sella turcica, EA-PitNET should be considered.
Picture 1.
Picture 2.
Picture 3.

The authors state that they have no Conflict of Interest (COI).
Acknowledgement
We are indebted to Dr. Shozo Yamada (Moriyama Neurological Center Hospital) for performing the neurosurgery operation, Dr. Naoko Inoshita (Moriyama Neurological Center Hospital) for performing the pathological examination, and Dr. Ichiro Fujisawa (Kishiwada City Hospital) for performing the radiologic examination.
References
- 1.Lacroix A, Feelders RA, Stratakis CA, et al. Cushing's syndrome. Lancet 386: 913-927, 2015. [DOI] [PubMed] [Google Scholar]
- 2.Koizumi M, Usui T, Yamada S, et al. Successful treatment of Cushing's disease caused by ectopic intracavernous microadenoma. Pituitary 14: 295-298, 2011. [DOI] [PubMed] [Google Scholar]