

Abstract
Objective:
To examine the impacts of a Solar Market Garden 1-year solar-powered drip irrigation (SMG) programme in Kalalé district of northern Benin on mothers’ nutritional status and micronutrient levels.
Design:
Using a quasi-experimental design, sixteen villages were assigned to four groups: (i) SMG women’s groups (WG); (ii) comparison WG; (iii) SMG non-WG (NWG); and (iv) comparison NWG. Difference-in-differences (DID) estimates were used to assess impacts on mothers’ food consumption, diversity, BMI, prevalence of underweight (BMI < 18·5 kg/m2) and anaemia, and deficiencies of iron (ID) and vitamin A (VAD).
Setting:
Kalalé district, northern Benin.
Participants:
Non-pregnant mothers aged 15–49 years (n 1737).
Results:
The SMG programme significantly increased mothers’ intake of vegetables (DID = 25·31 percentage points (pp); P < 0·01), dietary diversity (DID = 0·74; P < 0·01) and marginally increased their intake of flesh foods (DID = 10·14 pp; P < 0·1). Mean BMI was significantly increased among SMG WG compared with the other three groups (DID = 0·44 kg/m2; P < 0·05). The SMG programme also significantly decreased the prevalence of anaemia (DID = 12·86 pp; P < 0·01) but no impacts were found for the prevalence of underweight, ID and VAD.
Conclusions:
Improving mothers’ dietary intake and anaemia prevalence supports the need to integrate gender-based agriculture to improve nutritional status. However, it may take more than a year, and additional nutrition and health programmes, to impact the prevalence of maternal underweight, ID and VAD.
Keywords: Women’s underweight, Women’s dietary diversity, Anaemia, Iron status, Vitamin A status, Solar-powered irrigation, Africa
Improving the health and nutritional status of mothers and providing them socio-economic resources are critically important to ensure their own well-being and may have positive impacts on their children’s health and nutritional status(1–3). According to the 2012 Benin Demographic and Health Survey (DHS), anaemia affected 41 % of women aged 15–49 years(4). In the 2006 Benin DHS, vitamin A deficiency (VAD) as measured by night blindness was reported by 12 % of women aged 15–49 years during their last pregnancy, with greater prevalence rates (14 %) in northern Benin(5). Alaofè et al.(6) found that 32 % of adolescent girls from two boarding schools in southern Benin had iron deficiency (ID). According to the 2012 Benin DHS(4), the prevalence of underweight (BMI <18·5 kg/m2) among women was 6·2 %, with the highest prevalence found among the poorest (8·3 %) and those living in the north (8·4 %). Further, the rural population in Benin was reported at 55·6 % in 2016, and rainfed cereal crops such as maize or sorghum are the main sources of food and income(7). However, these foods have limited nutritional content and relatively low market value and, as a result, have low poverty and malnutrition reduction potential via either consumption or sales(8).
Due to regional hydrology and lack of access to water, agricultural production is often interrupted during the dry season when many farmers must rely on food stocks accumulated during the rainy season and/or on food purchases(9). Evidence shows that women’s underweight status is associated with illness and inadequate diets, in part due to seasonal cereal shortages(4,10,11). Since crop production practices are strongly gender-divided across the region, with men often in charge of cereal and cash crops and women in charge of legumes and family gardens(12), irrigated horticulture targeted to mothers of young children can be one way to improve their nutritional status(13). Irrigation can have a direct impact on food availability because of increased productivity and changes in cropping patterns(14–16). Moreover, irrigation will likely increase the stability of the food supply because of improved water control, which will reduce potentially adverse impacts of too little rain on production(17). Greater availability of food can also favour greater food intake at the household level(18), but its intra-household distribution may not be equitable(19).
Despite the potential of irrigated agriculture to benefit women, supporting evidence from rigorous programme evaluations is scarce(9). To date, evaluations of these interventions have primarily assessed changes in food consumption and dietary diversity(20,21), whereas few have evaluated changes in prevalence of anaemia(20,22), or women’s nutritional status(20,23,24), or examined both(20,24). These evaluations have demonstrated positive impacts on household and women’s dietary diversity. However, only one has found a positive impact on increasing the Hb levels of women living in fruit and vegetable-producing households by 0·14–0·15 g/dl(22), and one study demonstrated a positive impact on increasing women’s BMI(24). Of the two studies that have looked at the impact of drip irrigation systems, none of them evaluated their effect on mothers’ BMI or prevalence of underweight(14,25). To our knowledge, no studies have assessed the impact of irrigated agriculture on the micronutrient status of women.
As a way to improve food and nutrition security, in 2007, the Solar Electric Light Fund began a pilot test of commercial-scale, solar-powered drip irrigation systems in the Kalalé district of northern Benin(26). The Solar Market Garden (SMG) combines solar (photovoltaic) water pumping and low-pressure drip irrigation, allowing farmers in remote, dry regions to grow high-value and nutritious crops year-round(27). The SMG is a direct-coupled system (no batteries); it is simple and safe to install and operate. The pilot SMG systems were installed in conjunction with local women’s agricultural groups engaged in horticulture. Over the first two years of operation, these gardens were found to have a significant impact on the food security and economic well-being of the farmers and their households(26,28). However, there was no evidence base on their impact on women’s dietary diversity, anthropometrics or clinical indicators. In addition, although drip irrigation is the most rapidly expanding type of irrigation in sub-Saharan Africa, the impact of this technology has been limited by reliable access to water and lack of agronomic and marketing support(29–31). Therefore, the SMG systems – by combining the efficiency of drip irrigation with the reliability of a solar-powered water pump – are an innovative technology whose health and nutrition impacts needed to be assessed. In the present study, we determined the impact of expanding SMG systems on three important sets of outcomes for mothers: dietary diversity; prevalence of underweight; and anaemia and micronutrient deficiencies including VAD and ID.
Participants and methods
Project context and research design
The SMG implemented in the district of Kalalé in northern Benin was designed to expand agricultural production for local women’s farming groups (WG) engaged in hand-watered horticulture. By providing a reliable labour-saving energy access to pump irrigation water, the SMG had the potential to improve mothers’ dietary diversity and nutritional status through two primary programme impact pathways: (i) increased production to increase income; and (ii) increased production to increase consumption of these foods. The participation in SMG was expected to increase the ability of beneficiary mothers to contribute to their own well-being and the well-being of their children and other household members.
Before the baseline evaluation, villages in the district of Kalalé were identified for possible inclusion in the SMG; participating villages needed to have potential water sources (as determined by geophysical survey to map groundwater) to support production during the dry season. Sixteen eligible villages were identified, and they were matched and assigned to one of two groups (Fig. 1): (i) SMG villages, where SMG were installed in conjunction with pre-existing local women’s agricultural groups engaged in horticulture (eight intervention villages), each SMG is used jointly by thirty to thirty-five women in an agricultural group, each of whom farms her own 120 m2 plot; or (ii) comparison villages that did not utilize the SMG, based on similarity along several variables, including pre-existing local WG, location along the same roads, administrative status and size (eight matched-pair comparison villages). This sample size was based on available funds with the expectation that it would be able to show differences in agricultural production and changes in food security when scaled up from the original pilot study. The sample size was not based on changes in nutritional status.
Fig. 1.
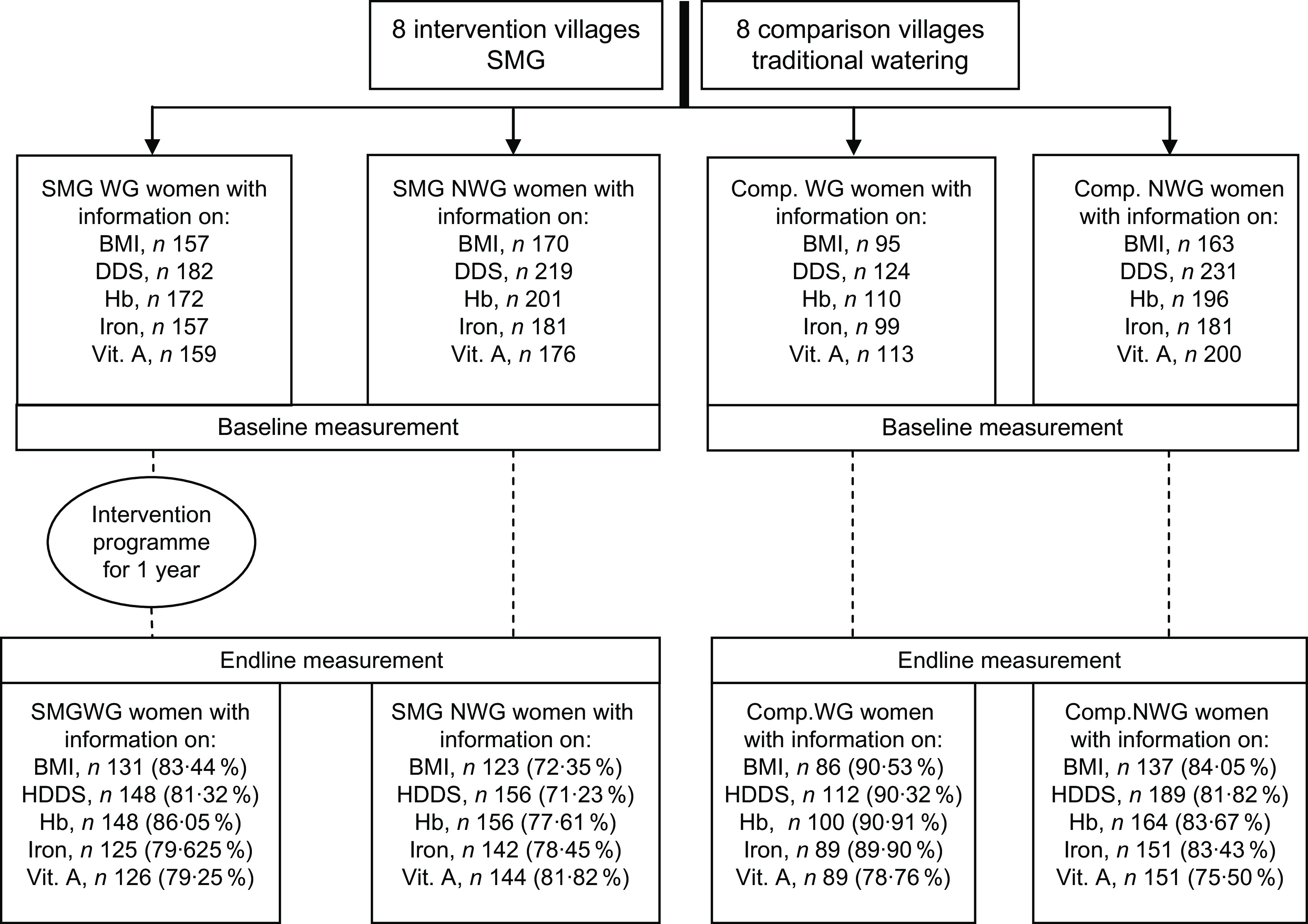
Flowchart showing the number of women aged 15–49 years with information on BMI, dietary diversity, Hb, iron and vitamin A status at baseline (January–March 2014) and after the 1-year intervention (February–March 2015) in Kalalé district, northern Benin (SMG, Solar Market Garden; WG, women’s group; NWG, non-women’s group; Comp., comparison; HDDS, Household Dietary Diversity Score; vit. A, vitamin A)
In each village, all households represented in women’s groups (WG) were surveyed along with a maximum of thirty non-women’s group (NWG) households from the same village. In each investigated household, only one mother or caregiver of childbearing age (15–49 years) who had a child aged 6–59 months at the time of the baseline survey (January–March 2014) was invited to participate in the impact evaluation. Delegates/leaders of the selected villages were contacted to obtain a complete listing of all NWG households with a target mother–child. From that list, a single household was selected as a starting point, using a random number between one and the required number of households in the village. If there was more than one woman/child in the house, only one mother–child pair was selected. The evaluation used a longitudinal design and followed the same households, mothers and children over time. An endline survey was conducted 1 year after programme implementation between February and March 2015. In total, 770 households were surveyed at baseline. There was some attrition from baseline to follow-up (4·3 %) that was spread across villages, with no structural differences in terms of who was most likely to drop out(32).
Data collection
Household surveys were used to collect data at baseline and endline on sociodemographic characteristics, health status and dietary intake, while anthropometric measurements and blood samples were taken from the selected mother–child pairs to assess anaemia, iron and vitamin A status by health workers at health centres or schools (when health centres were not available).
A structured questionnaire was administered to the mother and was composed of sociodemographic information (mother’s age, education and occupation, household size, ethnicity, health and sanitation, electricity connection, food insecurity, health-care insecurity and socio-economic status (SES)) and mother’s current pregnancy status. Specifically, the self-reported food insecurity score was collected using the following question: ‘Is it currently difficult for the household to buy or obtain enough food per day?’ Frequency response categories were: ‘it is never a problem’ (0); ‘this is sometimes a problem’ (1); and ‘it is usually a problem’ (2). These categories were recoded as: ‘yes, food insecurity’ (1 and 2); and ‘no food insecurity’ (0). The self-reported health-care insecurity was based on the question: ‘Currently, is it difficult for your household to buy medication or take someone to a clinic in case of illness?’ Frequency response categories were: ‘it is never a problem’ (0); ‘this is sometimes a problem’ (1); and ‘it is usually a problem’ (2). The SES index was constructed using principal component analysis, and included house and land ownership, housing quality (e.g. house construction materials), access to services (water, electricity and gas) and household assets (various durable goods, agricultural machinery, animals and livestock)(33,34). Factor scores derived from the first factor were then used to characterize the SES of each household. Households were categorized into SES quartiles based on their individual SES index score.
A qualitative recall of all foods consumed during the previous 24 h period was performed with the women responsible for the preparation of foods in the household, selected based on our criteria of inclusion in this survey, for household and women’s consumption, respectively. The dietary recalls were conducted with the following information reported: participant identification; recall day; food consumption time (e.g. breakfast, lunch, dinner or snack); and location of food consumed (e.g. in the home, outside). Based on the Household Dietary Diversity Score (HDDS) for measurement of household food access of the FAO and Food and Nutrition Technical Assistance Project, the dietary data collected were computed into twelve food groups for households: (i) cereals; (ii) white tubers and roots; (iii) vegetables; (iv) fruits; (v) meats; (vi) eggs; (vii) fish and other seafood; (viii) legumes, nuts and seeds; (ix) milk and milk products; (x) oils and fats; (xi) sweets; and (xii) spices, condiments and beverages(35). For women, the Women’s Dietary Diversity Score (WDDS-10) was defined as the number of food groups consumed based on 24 h recall, namely: (i) starchy staples; (ii) beans and peas; (iii) nuts and seeds; (iv) dairy; (v) flesh foods; (vi) eggs; (vii) vitamin A-rich dark green leafy vegetables; (viii) other vitamin A-rich vegetables and fruits; (ix) other vegetables; and (x) other fruits(36). Dichotomous variables were constructed to capture household and women’s consumption of each of individual food groups. The dietary diversity score was calculated by summing the number of unique food groups consumed.
For anthropometric measures, selected mothers were weighed without shoes or sandals and wearing light clothes using a balance with a precision of 0·1 kg (Body Composition Monitor Scale Seca 750). Height was measured using a device with a precision of 0·1 cm (Shorr Board®). BMI was calculated. Women were classified using BMI cut-off points endorsed by the WHO as underweight (BMI < 18·5 kg/m2), normal (BMI = 18·5– 24·9 kg/m2), overweight (BMI ≥ 25·0 kg/m2) or obese (BMI ≥ 30·0 kg/m2)(37).
Venous blood (2 ml) was drawn into a sterile tube (no anticoagulant). Hb was measured immediately using the Hemocue 201® device. Five free-falling drops of blood were collected on a pre-coded special chromatography filter paper (Whatman) and dried in the shade. The dried blood spots were protected from light and stored in a plastic bag with desiccant, and the packaged dried blood spots were preserved in a refrigerator (2–8°C). Then, the packaged dried blood spots were inserted into a rip-resistant envelope and sent to Craft Technologies, Inc. (Wilson, NC, USA), where retinol levels of the dried blood spots were estimated by the HPLC method(38,39). The remainder of the blood sample was stored in a cool box and transported at a temperature of 4–8°C. Within 24 h of sample collection, serum was obtained by centrifugation at 3000 g for 10 min, then aliquoted into 0·2 ml pre-labelled PCR tubes (Sarstedt) and kept frozen at −20°C before being sent (within 3 weeks) on dry ice to VitMin Lab (Willstaett, Germany) for analysis of ferritin (SF), soluble transferrin receptor, body Fe stores, retinol-binding protein, C-reactive protein (CRP) and α1-acid glycoprotein (AGP) concentrations using a sensible sandwich ELISA technique.
Anaemia was defined according to WHO standards as Hb below 12 mg/dl for non-pregnant women(40). Subclinical inflammation was defined as CRP > 5 mg/l and/or AGP > 1 g/l. Four groups were defined based on CRP and AGP levels: (i) reference (normal CRP and AGP); (ii) incubation (raised CRP and normal AGP); (iii) early convalescence (raised CRP and AGP); and (iv) late convalescence (normal CRP and raised AGP). Corrected values of SF and retinol within inflammation groups were obtained by multiplying values by their respective group corrector factors: SF by 0·77 (incubation), 0·53 (early convalescence) and 0·75 (late convalescence); retinol by 1·13 (incubation), 1·24 (early convalescence) and 1·11 (late convalescence). ID was defined as SF < 15 mg/l for the reference group, SF < 19 mg/l for the incubation group and early convalescence group, and SF < 27 mg/l for the late convalescence group. Iron-deficiency anaemia (IDA) was defined as the combination of anaemia and ID. Subclinical VAD was defined using WHO cut-offs as serum retinol < 20 μg/dl(40–42).
All the respondents were informed about the purpose of the survey and consent was received from all before their participation. The confidentiality of all information released by respondents was assured. The study was approved by the National Ethics Committee for Health Research of Benin. Ethical clearance was obtained from the institutional review boards charged with the protection of human research subjects of the University of Arizona. The analysis portion of the project was additionally approved by the institutional review board of the University of California, San Diego.
Statistical analysis
All statistical analyses were performed using the statistical software package Stata® version 14. Household sociodemographic characteristics, mothers’ age, education and occupation at baseline were compared across the SMG and comparison villages for all households. For clarity in this analysis, households represented in the women’s groups from intervention villages (i.e. primary beneficiary households) are identified as ‘SMG WG’ households and randomly selected households from the same villages as ‘SMG NWG’ households. ‘Comparison WG’ and ‘comparison NWG’ refer to the represented households of women’s groups and randomly selected NWG households from the same comparison villages, respectively. Variables were considered balanced at baseline if P > 0·05 for ANOVA (mean) and χ2 (%) comparing the four groups (SMG WG, comparison WG, SMG NWG, comparison NWG). An analysis of missing data for BMI (18·46 %), HDDS (19·97 %), anaemia (16·35 %), ID (17·96 %), IDA (18·42 %) and VAD (21·30 %) at follow-up using logistic regression and the t test was conducted and revealed that the outcome data were missing completely at random. As a whole, there were no significant differences in BMI, anaemia, ID, IDA and VAD between mothers who attrited and those whose did not attrit. Similar results were also observed for intervention and comparison villages when comparing attrited and non-attrited mothers. The most common reason was that mothers/caregivers were working on their land or moved/travelled out of the village on the day of data collection. In addition, some blood samples were found unsuitable for further processing as a result of the following reasons: 5·74 % due to haemolysis, 0·47 % were specimens without proper requisition slips and 3·23 % had insufficient sample quantity.
Difference-in-differences (DID) impact estimates were used to measure the impact of the SMG on household consumption of individual food groups and household dietary diversity, mothers’ intake of individual food groups and their dietary diversity, mothers’ BMI, and prevalence of underweight, anaemia, ID, IDA and VAD. The DID estimates describe the change in programme indicators between the endline and baseline surveys for the beneficiary women (SMG WG) relative to the non-beneficiary women (v. all: SMG NWG, comparison WG, comparison NWG); within SMG villages (SMG WG v. SMG NWG); and within WG (SMG WG v. comparison WG). The specification for BMI, prevalence of underweight, dietary diversity, anaemia, ID, IDA and VAD was controlled for mother’s age, household size, latrine, electricity connection, health-care insecurity and SES, found significant between the four groups at baseline. The analytic sample was restricted to households or mothers with complete data at baseline and endline for a given indicator. Pregnant women at baseline (n 3) or endline (n 8) were also excluded from analyses. Intent-to-treat protocol was used for the analysis as nineteen SMG WG at baseline became SMG NWG at follow-up and two SMG NWG became SMG WG. Statistical significance is reported at the 10 %, 5 % and 1 % probability levels.
Results
Baseline characteristics of intervention and comparison households and mothers
At baseline, there was no significant difference in household religion, ethnicity, access to an improved source of water, self-reported food insecurity, mothers’ education level and occupation between SMG and comparison groups. The majority of households were Muslim (92·1 %) and primarily engaged in agriculture (80·3 %), and formal education was rare among participating mothers in both SMG and comparison villages (9·7 %). However, a greater proportion of SMG WG households had older mothers, access to latrines, health-care insecurity and high SES compared with the other three groups (P < 0·05). In addition, household size in SMG NWG was lowest compared with the other three groups while the prevalence of access to electricity was greatest (Table 1).
Table 1.
Baseline key sociodemographic characteristics of SMG and comparison households and mothers, Kalalé district, northern Benin (January–March 2014)
| Variable | SMG WG (n 184) |
Comparison WG (n 126) |
SMG NWG (n 228) |
Comparison NWG (n 233) |
P † |
|---|---|---|---|---|---|
| Mother/caregiver characteristics | |||||
| Age (years)‡, mean | 31·92a | 29·69a | 29·41a | 28·74b | <0·001 |
| sd | 7·73 | 6·49 | 6·25 | 6·03 | |
| Mother’s education (%) | NS | ||||
| No formal education | 90·50 | 89·43 | 89·29 | 89·61 | |
| Primary or less | 4·47 | 7·32 | 5·36 | 4·33 | |
| Secondary | 5·03 | 3·25 | 5·36 | 5·63 | |
| University or more | 0 | 0 | 0 | 0·43 | |
| Mother’s occupation§ (%) | NS | ||||
| Agricultural/other labour | 80·33 | 83·18 | 75·20 | 80·52 | |
| Service/business | 18·03 | 13·64 | 20·80 | 16·88 | |
| Others | 1·64 | 3·18 | 4·00 | 2·60 | |
| Household characteristics | |||||
| Household size‡, mean | 7·21a | 8·59a | 6·91b | 7·58a | <0·001 |
| sd | 3·05 | 4·32 | 3·15 | 4·00 | |
| Religion (%) | NS | ||||
| Muslim | 90·66 | 88·80 | 92·02 | 95·20 | |
| Others | 9·34 | 11·20 | 7·98 | 4·80 | |
| Ethnicity (%) | NS | ||||
| Gando | 30·22 | 34·40 | 32·39 | 32·46 | |
| Boo | 39·56 | 35·20 | 35·68 | 29·82 | |
| Peulh | 17·58 | 17·60 | 18·31 | 16·23 | |
| Bariba | 11·54 | 9·60 | 8·92 | 14·91 | |
| Others | 1·10 | 3·20 | 4·69 | 6·58 | |
| Health and sanitation (%) | |||||
| Latrines | 17·98 | 8·26 | 11·85 | 7·59 | 0·007 |
| Improved source of water║ | 73·77 | 74·40 | 69·33 | 68·50 | NS |
| Electricity connection (%) | 13·21 | 2·48 | 10·61 | 2·23 | <0·001 |
| Food insecurity (%) | 17·32 | 16·00 | 12·02 | 20·09 | NS |
| Health-care insecurity (%) | 37·29 | 36·00 | 21·46 | 32·46 | 0·003 |
| Socio-economic status (%) | 0·005 | ||||
| Low | 17·79 | 24·11 | 21·57 | 29·15 | |
| Middle | 49·08 | 53·57 | 48·04 | 54·27 | |
| High | 33·13 | 22·32 | 30·39 | 16·58 | |
SMG, Solar Market Garden; WG, women’s group; NWG, non-women’s group; NS, P > 0·05.
Comparison between SMG and comparison groups using ANOVA (mean) and χ2 (%).
Tukey–Kramer pairwise comparisons; a,bvalues within a row with unlike superscript letters were significantly different (P < 0·05).
Agricultural/other labour = farming, livestock and hunting; services/business = small commerce, services, salaried employees and manual workers; others = students and unemployed/retired.
Improved source of water included water from a tap and other sources that were treated.
Impacts on mothers’ and households’ dietary diversity
As shown in Fig. 2, there was a significantly greater increase in the proportion of SMG households compared with the other three groups that consumed vegetables (DID = 18·8 percentage points (pp); P < 0·01), fish (DID = 14·5 pp; P < 0·05), fruits (DID = 4·9 pp; P < 0·05), eggs (DID = 4·2 pp; P < 0·01) and roots and tubers (DID = 29·2 pp; P < 0·01) between baseline and endline. The percentage of households that reported consuming meats decreased over time for all groups and the decrease was marginally greater for the non-SMG households (DID = 12·0 pp; P < 0·1; Fig. 2). Consequently, significant impacts of the programme were observed on HDDS in SMG WG compared with the other three groups (DID = 0·85; P < 0·01) and compared with the WG in the comparison villages (DID = 0·94; P < 0·01; Table 2).
Fig. 2.

Percentage change in the number of households that consumed individual food groups in the past 24 h at baseline (January–March 2014) and after the 1-year intervention (February–March 2015) among SMG WG ( ) and the other three groups (
) and the other three groups ( ), Kalalé district, northern Benin (n 1274). **P < 0·05, ***P < 0·01 for DID estimate adjusted for age, household size, latrines, electricity connection, health-care insecurity, socio-economic status and type of group (SMG, Solar Market Garden; WG, women’s group; DID, difference-in-differences)
), Kalalé district, northern Benin (n 1274). **P < 0·05, ***P < 0·01 for DID estimate adjusted for age, household size, latrines, electricity connection, health-care insecurity, socio-economic status and type of group (SMG, Solar Market Garden; WG, women’s group; DID, difference-in-differences)
Table 2.
Mean dietary diversity scores at baseline (January–March 2014) and after the 1-year intervention (February–March 2015), and DID impact estimates for these indicators, among SMG and comparison households and mothers†, Kalalé district, northern Benin
| SMG villages | Comparison villages | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WG | NWG | WG | NWG | SMG WG v. all | Within SMG villages‡ | Within WG§ | ||||||||
| Variable | Mean | sd | Mean | sd | Mean | sd | Mean | sd | DID | see | DID | see | DID | see |
| HDDS | ||||||||||||||
| n | 282 | 358 | 214 | 420 | 1070 | 536 | 423 | |||||||
| Baseline | 6·07 | 1·26 | 6·62 | 1·17 | 6·05 | 1·26 | 6·51 | 1·12 | ||||||
| Endline | 6·50 | 1·23 | 6·14 | 1·41 | 6·24 | 1·24 | 5·69 | 1·41 | 0·85*** | 0·18 | 0·06 | 0·25 | 0·94*** | 0·24 |
| WDDS-10 | ||||||||||||||
| n | 286 | 322 | 220 | 382 | 1017 | 510 | 430 | |||||||
| Baseline | 4·06 | 1·06 | 4·58 | 1·04 | 4·87 | 0·98 | 4·83 | 0·97 | ||||||
| Endline | 5·28 | 1·01 | 4·91 | 0·97 | 4·43 | 1·07 | 4·01 | 1·12 | 0·77*** | 0·15 | 0·16 | 0·15 | 0·83*** | 0·19 |
SMG, Solar Market Garden; WG, women’s group; NWG, non-women’s group; did, difference-in-differences; see, standard error of the estimate; HDDS, Household Dietary Diversity Score; n, total number of women involved in the analysis; WDDS-10, Women’s Dietary Diversity Score (ten food groups).
P < 0·01 for DID estimate.
DID impact estimates between comparison and intervention groups controlled for age, household size, latrines, electricity connection, health-care insecurity, socio-economic status and type of group. ‡Within SMG villages = SMG WG v. SMG NWG.
Within WG = SMG WG v. comparison WG.
Similar patterns of changes from baseline to endline were observed in mothers’ intake of individual food groups as well as in their overall dietary diversity in SMG WG compared with the other three groups. SMG WG mothers had a significantly greater increase of other vegetables intake (DID = 25·31 pp; P < 0·01) in the past 24 h, a significantly greater increase in flesh foods intake (DID = 10·14 pp; P < 0·1) and a significantly greater increase in beans and peas intake (DID = 23·95 pp; P < 0·01; Fig. 3). There was also a significant positive effect of the programme on increasing WDDS-10 in SMG WG compared with the other three groups (DID = 0·74; P < 0·01) and comparison WG (DID = 0·82; P < 0·01). However, no significant differences were observed between SMG WG and SMG NWG (Table 2).
Fig. 3.

Percentage change in number of women who consumed individual food groups in the past 24 h at baseline (January–March 2014) and after the 1-year intervention (February–March 2015) among SMG WG ( ) and the other three groups (
) and the other three groups ( ), Kalalé district, northern Benin (n 1210). *P < 0·1, **P < 0·05, ***P < 0·01 for DID estimate adjusted for age, household size, latrines, electricity connection, health-care insecurity, socio-economic status and type of group (SMG, Solar Market Garden; WG, women’s group; DID, difference-in-differences)
), Kalalé district, northern Benin (n 1210). *P < 0·1, **P < 0·05, ***P < 0·01 for DID estimate adjusted for age, household size, latrines, electricity connection, health-care insecurity, socio-economic status and type of group (SMG, Solar Market Garden; WG, women’s group; DID, difference-in-differences)
Impacts on mothers’ BMI and prevalence of underweight
After 1 year of participating in the SMG programme, SMG WG mothers had a significantly greater increase of mean BMI than did those living in the other three groups (DID = 0·44 kg/m2; P < 0·05) and WG mothers living in comparison villages (DID = 0·43 kg/m2; P < 0·1) in which the mean BMI remained the same (21·72 kg/m2 pre-intervention v. 21·74 kg/m2 post-intervention). However, the overall impact on the prevalence of underweight was not statistically significant. In addition, when comparing both outcomes within SMG villages, there was no significant difference in the impacts of the SMG programme on mothers’ BMI and prevalence of underweight between SMG WG women and SMG NWG women (BMI: DID = 0·25 kg/m2; P > 0·1; underweight: DID = 1·42 pp; P > 0·1; Table 3). We further stratified our analysis by SES and found that there was a tendency for the SMG systems to benefit underweight mothers within the middle-SES households (DID = 0·53; standard error of the estimate = 0·31; P < 0·1).
Table 3.
Mean BMI and prevalence of underweight (BMI < 18·5 kg/m2) at baseline (January–March 2014) and after the 1-year intervention (February–March 2015), and DID impact estimates for these indicators, among SMG and comparison mothers†, Kalalé district, northern Benin
| SMG villages | Comparison villages | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WG | NWG | WG | NWG | SMG WG v. all | Within SMG villages‡ | Within WG§ | ||||||||
| Variable | Mean or % | sd | Mean or % | sd | Mean or % | sd | Mean or % | sd | DID | see | DID | see | DID | see |
| BMI (kg/m2) | ||||||||||||||
| n | 256 | 252 | 167 | 279 | 811 | 429 | 359 | |||||||
| Baseline | 21·89 | 2·93 | 23·01 | 3·97 | 21·72 | 2·94 | 22·03 | 3·14 | ||||||
| Endline | 22·10 | 2·90 | 22·95 | 3·73 | 21·74 | 3·11 | 21·69 | 3·24 | 0·44** | 0·17 | 0·25 | 0·21 | 0·43* | 0·24 |
| Prevalence of underweight (%) | ||||||||||||||
| n | 256 | 252 | 167 | 279 | 811 | 429 | 359 | |||||||
| Baseline | 9·16 | – | 4·88 | – | 12·79 | – | 6·57 | – | ||||||
| Endline | 8·80 | – | 3·10 | – | 12·35 | – | 14·08 | – | 0·26 | 0·23 | 0·10 | 0·42 | –0·22 | 0·27 |
SMG, Solar Market Garden; WG, women’s group; NWG, non-women’s group; DID, difference-in-differences; see, standard error of the estimate; n, total number of women involved in the analysis.
*P < 0·1, **P < 0·05 for DID estimate.
DID impact estimates between comparison and intervention groups controlled for age, household size, latrines, electricity connection, health-care insecurity, socio-economic status and type of group.
Within SMG villages = SMG WG v. SMG NWG.
Within WG = SMG WG v. comparison WG.
Impacts on anaemia and micronutrient status
The SMG programme significantly decreased the prevalence of anaemia in SMG WG by 12·86 pp compared with the three other groups (DID = –1·16; P < 0·01) and by 16·63 pp compared with WG in the comparison villages (DID = –1·25; P < 0·05). However, no significant impacts were found for the changes in prevalence of ID, IDA and VAD between the WG SMG households compared with the other households (Table 4).
Table 4.
Prevalence of anaemia, iron and vitamin A deficiency at baseline (January–March 2014) and after the 1-year intervention (February–March 2015), and DID impact estimates for these indicators, among SMG and comparison mothers†, Kalalé district, northern Benin
| Variable | SMG villages | Comparison villages | SMG WG v. all | Within SMG villages‡ | Within WG§ | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| WG | NWG | WG | NWG | DID | SEE | DID | SEE | DID | SEE | |
| Anaemia (%) | ||||||||||
| n | 289 | 319 | 194 | 334 | 342 | 164 | 126 | |||
| Baseline | 49·32 | 44·23 | 49·00 | 45·73 | ||||||
| Endline | 36·88 | 41·10 | 53·19 | 47·65 | –1·16*** | 0·45 | –0·89 | 0·53 | –1·25** | 0·58 |
| Iron deficiency (%) | ||||||||||
| n | 243 | 289 | 175 | 305 | 202 | 114 | 68 | |||
| Baseline | 15·32 | 21·83 | 17·98 | 16·56 | ||||||
| Endline | 13·45 | 16·33 | 12·79 | 16·23 | 0·24 | 0·52 | 0·67 | 0·64 | –0·11 | 0·83 |
| Iron-deficiency anaemia (%) | ||||||||||
| n | 240 | 282 | 170 | 282 | 108 | 56 | 40 | |||
| Baseline | 6·56 | 12·23 | 13·79 | 7·91 | ||||||
| Endline | 4·24 | 7·69 | 8·43 | 6·29 | –0·27 | 0·89 | 0·09 | 1·09 | –0·99 | 1·40 |
| Vitamin A deficiency (%) | ||||||||||
| n | 248 | 292 | 172 | 308 | 182 | 78 | 60 | |||
| Baseline | 14·29 | 16·67 | 20·22 | 25·17 | ||||||
| Endline | 5·74 | 9·46 | 10·84 | 13·38 | –0·26 | 0·66 | –0·54 | 0·77 | 0·54 | 0·95 |
SMG, Solar Market Garden; WG, women’s group; NWG, non-women’s group; DID, difference-in-differences; see, standard error of the estimate; n, total number of women involved in the analysis.
P < 0·05, ***P < 0·01 for DID estimate.
DID impact estimates between comparison and intervention groups controlled for age, household size, latrines, electricity connection, health-care insecurity, socio-economic status and type of group.
Within SMG villages = SMG WG v. SMG NWG.
Within WG = SMG WG v. comparison WG.
Discussion
Our results confirm, as others have, that drip irrigation farming programmes are successful in increasing household consumption and mothers’ dietary intake of nutrient-rich foods(14,24,28). However, our results add to this literature by demonstrating – and for the first time, to our knowledge, through a quasi-experimental design – that these programmes can also directly improve mothers’ nutritional status and anaemia levels. Our study showed a significant increase in mean BMI among SMG WG mothers compared with the other three groups over a period of only 1 year. The SMG programme also had a positive impact on the prevalence of anaemia, which decreased by 12·9 % among SMG WG mothers compared with the other three groups (SMG NWG, comparison WG, comparison NWG). These benefits not only represent positive changes for the mothers themselves but can also potentially improve their ability to care for their children and, in turn, contribute to improving their children’s health and nutrition(2,43). Overall, there was little evidence of a spillover effect within the present study both within and between villages. When the SMG WG group increased its dietary diversity and BMI and decreased its prevalence of anaemia, there was little change for the women in the SMG NWG group. However, it will be important to examine these relationships in future analysis and to also assess potential unintended negative effects of the SMG programme on women’s time use and ability to care for their children, as observed by Von Braun et al.(24) and Steiner-Asiedu et al.(44).
Significant positive effects of the SMG systems were found on household consumption of nutrient-rich foods among SMG WG, particularly of fruits, vegetables, meats and fish, which were consistent with changes in food purchases and use of food from stores observed in our pilot study conducted between November 2007 and 2008(26,28). Impacts on mothers’ dietary intake of individual food groups and diversity largely reflected impacts at the household level, which were significant for fruits, vegetables, fish and dietary diversity scores, and marginally significant for meats including poultry. Within the limits of the available data that did not include the amount of food consumed, the parallel findings on households’ and mothers’ dietary intake and diversity are in line with mixed-methods research conducted in Benin that illustrates that women and children may be favoured in the intra-household distribution of foods(45). Similarly, Nanama and Frongillo(46) demonstrated that men are the first to cut back on food intake and that woman have their own stores of foods that they can access when the household is facing cereal shortages in Burkina Faso. A similar trend has been observed among pastoralists in Kenya where men are the first to suffer the effects of food shortages, whereas women and children tend to be more protected(47).
To our knowledge, the present study is the first evaluation of an SMG programme to demonstrate a positive impact on mothers’ mean BMI, which increased by 0·44 kg/m2 in SMG WG compared with other groups and by 0·43 kg/m2 compared with comparison WG, although no effect was found on the prevalence of underweight. Of the two studies that have looked at the impact of these types of programmes, neither evaluated their effect on mothers’ BMI or prevalence of underweight(14,25). Both studies analysed the impact of drip irrigation on well-being or other socio-economic aspects and food security with gender considerations. As for the two studies that have looked at the impact of other types (pump and tidal or dams) of irrigation systems on mothers’ weight, BMI or prevalence of underweight, Von Braun et al.(24) found that women’s body weight fluctuated by at least 2·20 kg in 1 year between the wet season and the dry season, while the prevalence of women underweight decreased by 20 % after 10 years of operation in the study of Benefice and Simondon(23). These results suggest that the SMG programme can benefit the most vulnerable mothers after a long-term adoption. This is consistent with our results suggesting that underweight started to improve in the middle-SES households who may have had the means to incorporate the SMG programme sooner. Finally, it is possible that drip irrigation systems such as the SMG, being a labour-saving energy access to pump irrigation water(26,48), could reduce women’s energy expenditure and thus partially explain the increase of BMI in the SMG WG group.
The SMG programme also significantly decreased the prevalence of anaemia among SMG WG mothers compared with other groups, suggesting that the increased consumption of fruits, vegetables, meats and fish, and mothers’ dietary diversity discussed earlier have direct positive effect on the micronutrient security of individuals. Women’s Hb levels in SMG WG increased by 0·37 g/dl, which is a rather modest but highly significant contribution, with implications for anaemia in women of reproductive age. Consequently, the prevalence of anaemia was significantly reduced by more than 12 % among SMG WG mothers. Our result is in line with Kabunga et al.’s(22) findings in rural Uganda, where fruit and vegetable intake and household food security effects, as a direct result of fruit and vegetable production, had positive effects on anaemia levels for women living in producer households. These results are not implausible since fruits and vegetables are not only important and cheap sources of micronutrients when consumed to supplement high-energy staples(49,50), but they also act as alternative food sources for households and individuals that face poverty and famine in most African communities. Finally, the reduction of the physical activity of women with the SMG systems might be a possible explanation for the reduction of anaemia as observed by Wouthuyzen-Bakker and van Assen(51) in young adults.
It is important to note that a programme such as SMG systems could be particularly important for safeguarding mothers’ access to food in this context by building or protecting their food stores through the additional food produced because of programme inputs as well as by increasing food availability(26). Stores of food are likely to be most important during the planting or lean season in rural Benin when cereal shortages are common, which can cause the prevalence of underweight to increase(4,10,11). In addition, increased availability of food through increased production is likely to be important during the harvest season to make up for any deficits accrued during the pre-harvest season. In our study conducted during the pre-harvest season in both 2014 and 2015, the significant positive impact of the SMG systems on increasing the mean BMI among SMG WG mothers by 0·34 kg/m2 and reducing the prevalence of anaemia by more than 12 % is plausible given the demonstrated impact of the SMG systems on increasing mothers’ agricultural production, household income and nutritional intake(26,28), as well as due to the improvements to mothers’ dietary intake of nutrient-rich foods and diversity observed in the present study. Finally, increasing women’s income might improve their diet diversity and/or their health status as observed in our pilot study in 2007–2008, where 57 % of the women in SMG WG used their additional income on food and 54 % used it on health care(28).
Although we found significant positive impacts of SMG on the mother’s prevalence of anaemia, no significant impacts of the programme were observed on iron and vitamin A status. The lack of impact can be partially explained by the persistently low consumption of meats and fish, which are expensive and rich in micronutrients, despite their statistically significant increase in SMG WG compared with other groups. In addition, nutritional status depends not only on food consumption and dietary adequacy but on other factors such as diseases and intestinal parasites that contribute to poor absorption of nutrients(52). A decrease in the anaemia prevalence without a significant improvement in iron status could also have occurred due to an underlying folate deficiency, which was improved with an increase in vegetable consumption(53). Additionally, improving vitamin A status using a plant-based approach also requires a sufficient fat consumption to support β-carotene absorption and its subsequent conversion to vitamin A(54), which decreased at endline. Unfortunately, we do not have data to identify which of these factors caused the anaemia in the present survey. Beyond dietary factors, the majority of mothers in the study area have no formal education and the literature shows that maternal education could lead to improve their nutritional status(55). The right to education and information also directly or indirectly impacts positively on their right to access health care, which further enhances nutrition and health(56).
The current study has some limitations. First, although the reduction in the prevalence of underweight is plausible given the multiple positive documented impacts of the SMG programme on relevant outcomes, it is possible that other unmeasured factors also contributed to increasing mean BMI such as changes in use of health-care services, morbidity or workload. Second, although dietary diversity has been associated with women’s BMI during the post-harvest season(10), more comprehensive measures of dietary intake may have shed further light as to how changes in mothers’ dietary intake were related to the changes seen in mean BMI. Last, it should be noted that the study’s findings are relevant for villages with similar characteristics as those included in the study, which, most important in this context, is access to water for agricultural production.
Conclusion
In conclusion, the present study examined the impact of a solar-powered drip irrigation farming programme on women’s anaemia and micronutrient status in addition to household consumption and women’s dietary diversity. Our findings showed that SMG can increase mean BMI, household and mother’s dietary diversity as well as consumption of fruits and vegetables, and marginally increase consumption of meats and fish. In addition, SMG decreased the prevalence of anaemia. However, the absence of impact on mother’s prevalence of underweight, ID and VAD suggest that incorporating nutrition and health programming with agricultural interventions and taking a more long-term approach to obtaining and measuring outcomes may also be needed to demonstrate the full impact of SMG systems(2). Adding food and nutrition education components to trainings on how to operate and maintain irrigation systems would help reinforce the pathway from improved agricultural productivity to better nutrition and health. Recommendations on which crops to plant to improve nutrition and how to better preserve and cook irrigated crops are two examples that could be incorporated into nutrition education programmes. Finally, the improvement of mother’s nutritional status and anaemia levels in SMG WG confirms the critical need to integrate gender considerations into policy design in order to favour women’s involvement in irrigated horticulture.
Acknowledgements
Acknowledgements: The authors thank the participants and the village delegates, nurses and enumerators for their support in carrying out this research. They wish to express their very special appreciation to ADESCA-ONG team whose contribution was central to this project. Financial support: This work was supported by the University of Stanford, the Hellman Fellows Programme at the University of California, San Diego and the University of Arizona. The funders had no role in the design, analysis or writing of this article. Conflict of interest: There are no conflicts of interest. Authorship: H.A. led the data collection activities and designed the evaluation with input from D.T. and J.B., and analyaed data. All the authors participated in drafting and revising the manuscript. Ethics of human subject participation: The study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the National Ethics Committee for Health Research of Benin. Ethical clearance was obtained from the institutional review boards charged with the protection of human research subjects of the University of Arizona. All women were informed verbally about the aims and procedures of the study, and informed consent was obtained from all women and children, via their mother or guardian approval for the latter, before enrolment.
References
- 1. van den Bold M, Quisumbing A & Gillespie S (2013) Women’s Empowerment and Nutrition: An Evidence Review. IFPRI Discussion Paper no. 01294. Washington, DC: International Food Policy Research Institute.
- 2. Olney DK, Bliznashka L, Pedehombga A et al. (2016) A 2-year integrated agriculture and nutrition program targeted to mothers of young children in Burkina Faso reduces underweight among mothers and increases their empowerment: a cluster-randomized controlled trial. J Nutr 146, 1109–1117. [DOI] [PubMed] [Google Scholar]
- 3. Alaofe H, Zhu M, Burney J et al. (2017) Association between women’s empowerment and maternal and child nutrition in Kalale District of Northern Benin. Food Nutr Bull 38, 302–318. [DOI] [PubMed] [Google Scholar]
- 4. Institut National de la Statistique et de l’Analyse Economique & ICF International (2013) Enquête Démographique et de Santé du Bénin 2011–2012. Calverton, MD: INSAE and ICF International. [Google Scholar]
- 5. Food and Agriculture Organization of the United Nations (2011) Profil nutritionnel du pays: Republique du Benin. http://www.fao.org/3/a-bc623f.pdf (accessed November 2017).
- 6. Alaofè H, Zee J, Dossa R et al. (2008) Iron status of adolescent girls from two boarding schools in southern Benin. Public Health Nutr 11, 737–746. [DOI] [PubMed] [Google Scholar]
- 7. Trading Economics (2019) Benin – rural population. https://tradingeconomics.com/benin/rural-population-percent-of-totalpopulation-wb-data.html (accessed June 2019).
- 8. Burney JA, Naylor RL & Postel SL (2013) The case for distributed irrigation as a development priority in sub-Saharan Africa. Proc Natl Acad Sci 110, 12513–12517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Domenech L (2015) Improving irrigation access to combat food insecurity and undernutrition: a review. Glob Food Sec 6, 24–33. [Google Scholar]
- 10. Savy M, Martin-Prével Y, Traissac P et al. (2006) Dietary diversity scores and nutritional status of women change during the seasonal food shortage in rural Burkina Faso. J Nutr 136, 2625–2632. [DOI] [PubMed] [Google Scholar]
- 11. Bhandari S, Sayami JT, Thapa P et al. (2016) Dietary intake patterns and nutritional status of women of reproductive age in Nepal: findings from a health survey. Arch Public Health 74, 2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Food and Agriculture Organization of the United Nations (2011) State of Food and Agriculture. Women and Agriculture: Closing the Gender Gap for Development. http://www.fao.org/3/i2050e/i2050e.pdf (accessed June 2019).
- 13. Ruel MT & Alderman H (2013) Nutrition-sensitive interventions and programs: how can they help to accelerate progress in improving maternal and child nutrition? Lancet 382, 536–551. [DOI] [PubMed] [Google Scholar]
- 14. Namara R, Upadhyay B & Nagar RK (2005) Adoption and Impacts of Micro Irrigation Technologies: Empirical Results from Selected Localities of Maharashtra and Gujarat State of India. Colombo: International Water Management Institute. [Google Scholar]
- 15. Burney JA, Davis SJ & Lobell DB (2010) Greenhouse gas mitigation by agricultural intensification. Proc Natl Acad Sci 107, 12052–12057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Aseyehegn K, Yirga C & Rajan S (2011) Effect of small-scale irrigation on the income of rural farm households: the case of Laelay Maichew district, central Tigray, Ethiopia. J Stored Prod Postharvest Res 2, 208–215. [Google Scholar]
- 17. Dowgert MF (2010) The impact of irrigated agriculture on a stable food supply. In Proceedings of the 22nd Annual Central Plains Irrigation Conference, Kearney, NE, February 24–25, 2010. https://www.ksre.k-state.edu/irrigate/oow/p10/Dowgert10.pdf (accessed June 2019).
- 18. Gordon-Larsen P (2014) Food availability/convenience and obesity. Adv Nutr 5, 809–817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Njuki J, Waithanji E, Sakwa B et al. (2014) Can Market-Based Approaches to Technology Development and Dissemination Benefit Women Smallholder Farmers? A Qualitative Assessment of Gender Dynamics in the Ownership, Purchase, and Use of Irrigation Pumps in Kenya and Tanzania. IFPRI Discussion Paper no. 01357. Washington, DC: International Food Policy Research Institute.
- 20. Olney DK, Talukder A, Iannotti LL et al. (2009) Assessing impact and impact pathways of a homestead food production program on household and child nutrition in Cambodia. Food Nutr Bull 30, 355–369. [DOI] [PubMed] [Google Scholar]
- 21. Namara RE, Awuni JA, Barry B et al. (2011) Smallholder Shallow Ground Water Irrigation Development in the Upper East Region of Ghana. Research Report no. 134. Colombo: International Water Management Institute.
- 22. Kabunga N, Ghosh S & Griffiths JK (2014) Can Smallholder Fruit and Vegetable Production Systems Improve Household Food Security and Nutritional Status of Women? Evidence from Rural Uganda. IFPRI Discussion Paper no. 01346. Washington, DC: International Food Policy Research Institute.
- 23. Benefice E & Simondon K (1993) Agricultural development and nutrition among rural populations: a case study of the middle valley in Senegal. Ecol Food Nutr 31, 45–66. [Google Scholar]
- 24. Von Braun J, Puetz D & Webb P (1989) Irrigation Technology and the Commercialization of Rice in the Gambia: Effects on Income and Nutrition. IFPRI Research Report no. 75. Washington, DC: International Food Policy Research Institute.
- 25. Upadhyay B, Samad M & Giordano M (2005) Livelihoods and Gender Roles in Drip Irrigation Technology: A Case of Nepal. Working Paper no. 87. Colombo: International Water Management Institute.
- 26. Burney J, Woltering L, Burke M et al. (2010) Solar-powered drip irrigation enhances food security in the Sudano-Sahel. Proc Natl Acad Sci 107, 1848–1853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Solar Electric Light Fund (SELF) (2010) Solar Market Garden. https://web.stanford.edu/group/solarbenin/data/SolarMarketGardenInfo/Solar%20Market%20Garden.pdf (accessed March 2018).
- 28. Alaofè H, Burney J, Naylor R et al. (2016) Solar-powered drip irrigation impacts on crops production diversity and dietary diversity in Northern Benin. Food Nutr Bull 37, 164–175. [DOI] [PubMed] [Google Scholar]
- 29. Frenken K (2005) Irrigation in African Figures. AQUASTAT Survey – 2005. Rome: FAO. [Google Scholar]
- 30. Moyo R, Love D, Mul M et al. (2006) Impact and sustainability of low-head drip irrigation kits, in the semi-arid Gwanda and Beitbridge Districts, Mzingwane Catchment, Limpopo Basin, Zimbabwe. Phys Chem Earth 31, 885–892. [Google Scholar]
- 31. Belder P, Rohrbach D, Twomlow S et al. (2007) Can Drip Irrigation Improve the Livelihoods of Smallholders? Lessons Learned from Zimbabwe. Bulawayo: International Crops Research Institute for the Semi-Arid Tropics. [Google Scholar]
- 32. Burney J, Alaofe H, Naylor R et al. (2017) Impact of a rural solar electrification project on the level and structure of women’s empowerment. Environ Res Lett 12, 095007. [Google Scholar]
- 33. Vyas S & Kumaranayake L (2016) Constructing socio-economic status indices: how to use principal components analysis. Health Policy Plan 21, 59–468. [DOI] [PubMed] [Google Scholar]
- 34. Gwatkin DR, Rutstein S, Johnson K et al. (2007) Socio-economic differences in health, nutrition, and population within developing countries: an overview. Niger J Clin Pract 10, 272–282. [PubMed] [Google Scholar]
- 35. Kennedy G, Ballard T & Dop M (2011) Guidelines for Measuring Household and Individual Dietary Diversity. Rome: FAO, Nutrition and Consumer Protection Division. [Google Scholar]
- 36. Food and Agriculture Organization of the United Nations & FHI 360 (2016) Minimum Dietary Diversity for Women: A Guide for Measurement. Rome: FAO. [Google Scholar]
- 37. World Health Organization (1995) Physical Status: The Use and Interpretation of Anthropometry. Report of a WHO Expert Committee. WHO Technical Report Series no. 854. Geneva: WHO. [PubMed]
- 38. Craft NE, Bulux J, Valdez C et al. (2000) Retinol concentrations in capillary dried blood spots from healthy volunteers: method validation. Am J Clin Nutr 72, 450–454. [DOI] [PubMed] [Google Scholar]
- 39. Craft NE, Haitema T, Brindle LK et al. (2000) Retinol analysis in dried blood spots by HPLC. J Nutr 130, 882–885. [DOI] [PubMed] [Google Scholar]
- 40. World Health Organization & Food and Agriculture Organization of the United Nations (2006) Guidelines on Food Fortification with Micronutrients. Joint WHO/FAO Expert Consultation. Geneva: WHO. [Google Scholar]
- 41. Thurnham DI, McCabe LD, Haldar S et al. (2010) Adjusting plasma ferritin concentrations to remove the effects of subclinical inflammation in the assessment of iron deficiency: a meta-analysis. Am J Clin Nutr 92, 546–555. [DOI] [PubMed] [Google Scholar]
- 42. Thurnham DI, McCabe GP, Northrop-Clewes CA, et al. (2003) Effects of subclinical infection on plasma retinol concentrations and assessment of prevalence of vitamin A deficiency: meta-analysis. Lancet 362, 2052–2058. [DOI] [PubMed] [Google Scholar]
- 43. Walker SP, Wachs TD, Grantham-McGregor S et al. (2011) Inequality in early childhood: risk and protective factors for early child development. Lancet 378, 1325–1338. [DOI] [PubMed] [Google Scholar]
- 44. Steiner-Asiedu M, Abu BAZ, Setorglo J et al. (2012) The impact of irrigation on the nutritional status of children in the Sissala West District of Ghana. Curr Res J Soc Sci 4, 86–92. [Google Scholar]
- 45. Van Liere MJ, Brouwer ID & den Hartog AP (1996) A food ethnography of the Otammari in north-western Benin: a systematic approach. Ecol Food Nutr 34, 293–310. [Google Scholar]
- 46. Nanama S & Frongillo E (2012) Altered social cohesion and adverse psychological experiences with chronic food insecurity in the non-market economy and complex households of Burkina Faso. Soc Sci Med 74, 444–451. [DOI] [PubMed] [Google Scholar]
- 47. Villa KM, Barrett CB & Just DR (2011) Whose fast and whose feast? Intrahousehold asymmetries in dietary diversity response among East African pastoralists. Am J Agric Econ 93, 1062–1081. [Google Scholar]
- 48. Narayanamoorthy A, Devika N & Bhattarai M (2016). More crop and profit per drop of water: drip irrigation for empowering distressed small farmers. IIM Kozhikode Soc Manage Rev 5, 83–90. [Google Scholar]
- 49. Slavin JL & Lloyd B (2012) Health benefits of fruits and vegetables. Adv Nutr 3, 506–516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Miller DD & Welch RM (2013) Food system strategies for preventing micronutrient malnutrition. Food Policy 42, 115–128. [Google Scholar]
- 51. Wouthuyzen-Bakker M & van Assen S (2015) Exercise-induced anaemia: a forgotten cause of iron deficiency anaemia in young adults. Br J Gen Pract 65, 268–269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Gillespie S, Haddad L, Mannar V et al. (2013) The politics of reducing malnutrition: building commitment and accelerating progress. Lancet 382, 552–569. [DOI] [PubMed] [Google Scholar]
- 53. Ndiaye NF, Idohou-Dossou N, Diouf A et al. (2018) Folate deficiency and anemia among women of reproductive age (15–49 years) in Senegal: results of a national cross-sectional survey. Food Nutr Bull 39, 65–74. [DOI] [PubMed] [Google Scholar]
- 54. Ribaya-Mercado JD (2002) Influence of dietary fat on beta-carotene absorption and bioconversion into vitamin A. Nutr Rev 60, 104–110. [DOI] [PubMed] [Google Scholar]
- 55. Alderman H & Headey DD (2017) How important is parental education for child nutrition? World Dev 94, 448–464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Feinstein L (2006) The Effects of Education on Health: Concepts, Evidence and Policy Implications: A Review for the OECD Centre for Educational Research and Innovation (CERI). Paris: Organisation for Economic Co-operation and Development. [Google Scholar]