

Abstract
Background
The primary vectors of the agent of Lyme disease in Canada are Ixodes scapularis and Ixodes pacificus ticks. Surveillance for ticks and the pathogens they can transmit can inform local tick-borne disease risk and guide public health interventions. The objective of this article is to characterize passive and active surveillance of the main Lyme disease tick vectors in Canada in 2019 and the tick-borne pathogens they carry.
Methods
Passive surveillance data were compiled from the National Microbiology Laboratory Branch and provincial public health data sources. Active surveillance was conducted in selected sentinel sites in all provinces. Descriptive analysis of ticks submitted and infection prevalence of tick-borne pathogens are presented. Seasonal and spatial trends are also described.
Results
In passive surveillance, specimens of I. scapularis (n=9,858) were submitted from all provinces except British Columbia and I. pacificus (n=691) were submitted in British Columbia and Alberta. No ticks were submitted from the territories. The seasonal distribution pattern was bimodal for I. scapularis adults, but unimodal for I. pacificus adults. Borrelia burgdorferi was the most prevalent pathogen in I. scapularis (18.8%) and I. pacificus (0.3%). In active surveillance, B. burgdorferi was identified in 26.2% of I. scapularis; Anaplasma phagocytophilum in 3.4% of I. scapularis, and Borrelia miyamotoi and Powassan virus in 0.5% or fewer of I. scapularis. These same tick-borne pathogens were not found in the small number of I. pacificus tested.
Conclusion
This surveillance article provides a snapshot of the main Lyme disease vectors in Canada and their associated pathogens, which can be used to monitor emerging risk areas for exposure to tick-borne pathogens.
Keywords: Ixodes scapularis, Ixodes pacificus, surveillance, Borrelia, Anaplasma, Babesia
Introduction
Ixodes scapularis and Ixodes pacificus are tick vectors capable of transmitting several bacterial, viral and protozoan pathogens to humans ( ( ((1)))). Ixodes scapularis populations are increasing in number and distribution in southern central and eastern Canada ( ( ((2–4)))). Climate (e.g. increasing temperatures, changes in precipitation) and environmental factors (e.g. changes in land use) contribute to the geographic range expansion of ticks, which can enhance exposure to tick-borne diseases (TBD) ( ( ((1,5–7)))). These changes can also create longer seasons for adventitious ticks to become established in new areas and increase human-tick interactions ( ( ((1,4,6–8)))). Continued expansion of the range of ticks in Canada presents a public health challenge, as awareness of TBD risks and capacity for surveillance and testing must also expand to these areas ( ( ((1)))).Lyme disease (LD) is the most commonly reported vector-borne disease in Canada, and incidence of reported cases has increased more than 17-fold from 2009 through 2019 ( ( ((9,10)))). The causative agent of LD, Borrelia burgdorferi, is transmitted by I. scapularis in central and eastern Canada and by I. pacificus in British Columbia. Beyond LD, other TBD including anaplasmosis (caused by the bacterium Anaplasma phagocytophilum), babesiosis (caused by the parasite Babesia microti), hard tick-borne relapsing fever (caused by the bacterium Borrelia miyamotoi) and Powassan virus (POWV) disease are emerging as diseases locally acquired within Canada ( ( ((1,11–15)))).Passive surveillance began in the early 1990s in Canada to detect the occurrence of I. scapularis and I. pacificus tick vectors and their infection with B. burgdorferi ( ( ((16)))). Active surveillance has been ongoing since the 2000s to identify areas where vector tick populations are establishing and, as a result, where LD may become endemic (LD risk areas) ( ( ((17,18)))). This is the first edition of a pan-Canadian annual article summarizing the findings of both passive and active vector surveillance and updating estimates of infection prevalence in ticks. A previous study by Guillot et al. ( ( ((19)))) summarized results of a pan-Canadian study on tick surveillance; however, that study only included active tick surveillance from sentinel sites.The objective of this surveillance article is to provide an epidemiologic summary of the main LD vectors in Canada, I. scapularis and I. pacificus, and their associated pathogens, collected through active and passive surveillance systems in 2019. This article will also summarize the prevalence and spatial distribution of tick-borne pathogens.
Methods
Data sources
This article uses two types of surveillance data from six different sources: 1) passive tick surveillance data from the National Microbiology Laboratory (NML) Branch of the Public Health Agency of Canada, the British Columbia Centre for Disease Control and Alberta Health ( ( ((20)))); and 2) active tick surveillance data from the Canadian Lyme Sentinel Network (CaLSeN), the New Brunswick Department of Health and the University of Ottawa.
Passive tick surveillance
In passive tick surveillance, ticks are collected by the public and submitted to medical clinics, veterinary clinics, or directly to a provincial public health laboratory or other institution (e.g. university laboratory) for species identification ( ( ((16)))). Location of acquisition, history of travel in the past two weeks, date of collection, level of engorgement, tick instar and host are recorded.This article focuses on I. scapularis and I. pacificus ticks collected in Canada, although several other tick species were also collected. Ticks with an international location of acquisition, an imprecise location within Canada that could not be geocoded (e.g. province listed only, multiple locations listed) or history of travel were excluded to create a dataset of locally acquired ticks. Over the years, passive tick surveillance programs have been discontinued in different jurisdictions, i.e. Nova Scotia, southwestern Québec (Montérégie) and eastern Ontario; however, the public continues to submit a relatively small number of ticks acquired in these jurisdictions directly to NML.In 2019, Saskatchewan, Manitoba, Ontario, Québec, Newfoundland and Labrador, New Brunswick, Nova Scotia and Prince Edward Island sent ticks to NML for testing of tick-borne pathogens (A. phagocytophilum, B. burgdorferi and B. microti) using methods described previously ( ( ((21,22)))). Ticks could be submitted singly or in groups of two or more (multiple submission). For laboratory testing, ticks from the same multiple submission were pooled and tested together. In British Columbia ( ( ((23)))) and Alberta ( ( ((24)))), testing was done at provincially funded laboratories on individual ticks for only B. burgdorferi. Ticks are rarely encountered in northern Canada and as a result, formal passive tick surveillance programs for I. scapularis or I. pacificus are not established in the Yukon, Northwest Territories or Nunavut.
Active tick surveillance
Active surveillance involves collection of ticks in the environment through drag sampling or through capture of host mammals that are examined for ticks. This method aims to identify where emerging tick populations are establishing ( ( ((4,18)))). For this article, only I. scapularis and I. pacificus collected by drag sampling were included for analysis, although several other tick species were also collected.
This article collates data from CaLSeN, the New Brunswick Department of Health and the University of Ottawa. The CaLSeN used standardized methods to conduct dragging in 96 sites across all provinces ( ( ((19)))). The New Brunswick Department of Health and the University of Ottawa used similar dragging methods to visit 73 and 15 sites, respectively ( ( ((25)))). Visit date, location of collection (latitude and longitude), tick species and tick instar were recorded for all ticks collected.
Nymphs and adult I. scapularis and I. pacificus were tested for tick-borne pathogens. Ticks collected by CaLSeN and by the province of New Brunswick were tested for A. phagocytophilum, B. microti, B. burgdorferi, B. miyamotoi and POWV (CaLSeN ticks only) at NML using methods previously described ( ( ((19,21,22)))). Ticks collected by the University of Ottawa were tested for A. phagocytophilum, B. burgdorferi and B. miyamotoi with quantitative polymerase chain reaction (qPCR) assays described previously ( ( ((25)))) using the flaB gene for B. miyamotoi and including a confirmatory assay targeting msp2 in A. phagocytophilum. Testing for B. microti used a qPCR assay targeted towards the cctη gene ( ( ((21)))).
Analysis
Tick characteristics
For passive tick surveillance, we calculated descriptive statistics for province of acquisition, tick species, instar (larva, nymph, adult male or adult female), level of engorgement (unfed, partially engorged or fully engorged), host (human, dog, cat or other) and month of collection. For active tick surveillance, we calculated descriptive statistics for province of acquisition, tick species and instar (larva, nymph or adult). The probable location of acquisition for ticks was mapped using QGIS (version 3.8.1).
Infection prevalence
For ticks submitted through passive surveillance, maximum likelihood estimates (MLE) of prevalence with 95% confidence intervals (CI) were calculated in Excel (version 16.0) using the PooledInfRate add-in (version 4.0) to account for pooled testing ( ( ((26,27)))). Co-infection prevalence was assessed among single submissions only to ensure they were true co-infections (two or more pathogens in the same tick). The prevalence of co-infections was calculated as the number of co-infected ticks divided by the total number of ticks tested. Prevalence in active surveillance was calculated in the same manner as all ticks were tested individually.
Results
Passive surveillance tick characteristics
In 2019, there were 10,549 I. pacificus and I. scapularis ticks submitted from all provinces through passive surveillance (Table 1). The majority of ticks (90.0%) were submitted from three provinces: Ontario, Québec, and New Brunswick (Figure 1). The majority of ticks (94.0%) were single submissions, but there were 242 multiple submissions (range: 2–8 ticks). Nova Scotia had the highest proportion of multiple submissions (13.7%; n=7/51).
Table 1. Number of Ixodes scapularis and Ixodes pacificus ticks and submissions collected through passive surveillance by province, Canada, 2019a.
| Province | Number of ticks | Number of single submissionsb | Multiple submissionsb | ||||
|---|---|---|---|---|---|---|---|
| Ixodes scapularis | Ixodes pacificus | Total | Number of submissions | Median number of ticks per submission | |||
| n | Range | ||||||
| British Columbia | 0 | 690 | 690 | 690 | N/Ac | N/Ac | N/Ac |
| Alberta | 55 | 1 | 56 | 56 | N/Ac | N/Ac | N/Ac |
| Saskatchewan | 3 | 0 | 3 | 3 | 0 | N/A | N/A |
| Manitoba | 175 | 0 | 175 | 149 | 8 | 3 | 2–7 |
| Ontariod | 6,857 | 0 | 6,857 | 6,436 | 167 | 2 | 2–8 |
| Québecd | 1,697 | 0 | 1,697 | 1,618 | 31 | 2 | 2–7 |
| Newfoundland and Labrador | 44 | 0 | 44 | 42 | 1 | 2 | 2 |
| New Brunswick | 941 | 0 | 941 | 868 | 28 | 2 | 2–8 |
| Nova Scotiae | 72 | 0 | 72 | 44 | 7 | 5 | 2–5 |
| Prince Edward Island | 14 | 0 | 14 | 14 | 0 | N/A | N/A |
| Total | 9,858 | 691 | 10,549 | 9,920 | 242 | 2 | 2–8 |
Abbreviation: N/A, not applicable
a No passive surveillance was conducted in Yukon, Northwest Territories or Nunavut for I. scapularis or I. pacificus ticks
b Single submissions consist of one tick; multiple submissions consist of two or more ticks submitted together by the same person
c Province did not report whether ticks were from single or multiple submissions
d Passive tick surveillance has been discontinued in some regions of Ontario and Québec; however, individuals could submit ticks directly to the National Microbiology Laboratory Branch
e Passive tick surveillance has been discontinued in the entire province of Nova Scotia; however, individuals could submit ticks directly to the National Microbiology Laboratory Branch
Figure 1.
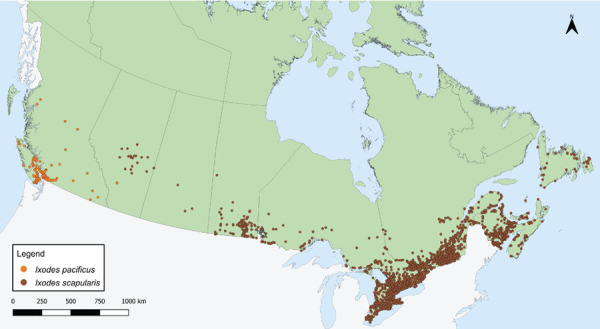
Ixodes pacificus and Ixodes scapularis ticks submitted through passive tick surveillance, Canada, 2019a,b
a Each dot represents the probable location of acquisition for an I. pacificus (n=691) or I. scapularis (n=9,858) tick submitted through passive surveillance
b No passive surveillance was conducted in Yukon, Northwest Territories or Nunavut for I. scapularis or I. pacificus ticks. Passive tick surveillance has been discontinued in the entire province of Nova Scotia, and some regions of Ontario and Québec; however, individuals could submit ticks directly to the National Microbiology Laboratory Branch from these jurisdictions
Data on tick instar, level of engorgement and host were available for 99.9%, 0% and 100% of I. pacificus, respectively. Data on tick instar, level of engorgement and host were available for 99.4%, 99.3% and 99.6% of I. scapularis, respectively. Adult ticks were submitted most frequently, of which most were female (I. scapularis: 89.0%; I. pacificus: 93.8%) (Table 2). Larvae (0.3%; 0.4%) and nymphs (8.1%; 3.3%) were submitted less frequently. Overall, 44.0% of I. scapularis were partially or fully engorged. Humans were the most common host among I. scapularis and I. pacificus (90.3%, 94.4%, respectively), followed by dogs (7.7%, 5.4%, respectively).
Table 2. Instar, level of engorgement and host of Ixodes scapularis and Ixodes pacificus ticks submitted through passive surveillance, Canada, 2019a,b.
| Characteristic | Tick species | |||
|---|---|---|---|---|
| Ixodes scapularis | Ixodes pacificus | |||
| n | % | n | % | |
| Instar | ||||
| Larva | 27 | 0.3 | 3 | 0.4 |
| Nymph | 795 | 8.1 | 23 | 3.3 |
| Adult female | 8,719 | 89.0 | 647 | 93.8 |
| Adult male | 256 | 2.6 | 17 | 2.5 |
| Total | 9,797 | 100 | 690 | 100 |
| Level of engorgementc | ||||
| Fully engorged | 113 | 1.2 | N/A | N/A |
| Partially engorged | 4,188 | 42.8 | N/A | N/A |
| Unfed | 5,485 | 56.0 | N/A | N/A |
| Total | 9,786 | 100 | N/A | N/A |
| Host | ||||
| Human | 8,870 | 90.3 | 652 | 94.4 |
| Dog | 761 | 7.7 | 37 | 5.4 |
| Cat | 119 | 1.2 | 1 | 0.1 |
| Otherd | 72 | 0.7 | 1 | 0.1 |
| Total | 9,822 | 100 | 691 | 100 |
Abbreviation: N/A, not applicable
a Data are presented for all ticks where available, regardless of whether the tick was part of a single or a multiple submission
b No passive surveillance was conducted in Yukon, Northwest Territories or Nunavut for I. scapularis or I. pacificus ticks. Passive tick surveillance has been discontinued in the entire province of Nova Scotia, and some regions of Ontario and Québec; however, individuals could submit ticks directly to the National Microbiology Laboratory Branch from these jurisdictions
c Level of engorgement was not reported for I. pacificus
d Includes environment, horse, rabbit, deer, skunk and other unspecified animal
Month of acquisition was available for 99.9% of I. pacificus and 99.4% of I. scapularis. Locally acquired ticks were submitted in every month of the year (Figure 2). Submissions of I. scapularis adults peaked in May and October, while there was a single peak for I. pacificus adults in May. Ixodes scapularis nymph submissions peaked in June and July, while I. pacificus nymph submissions peaked in May.
Figure 2.
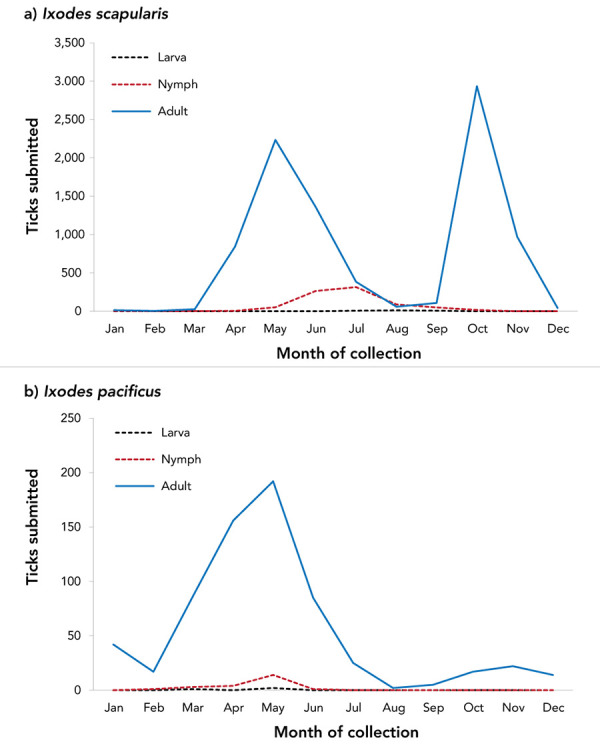
Number of Ixodes scapularis and Ixodes pacificus ticks submitted through passive surveillance, by month and tick instar, Canada, 2019a,b
a Data are presented for I. scapularis (n=9,797) and I. pacificus (n=690) ticks submitted through passive surveillance. Month of submission or tick instar was not available for I. scapularis (n=61) and I. pacificus (n=1)
b No passive surveillance was conducted in Yukon, Northwest Territories or Nunavut for I. scapularis or I. pacificus ticks. Passive tick surveillance has been discontinued in the entire province of Nova Scotia, and some regions of Ontario and Québec; however, individuals could submit ticks directly to the National Microbiology Laboratory Branch from these jurisdictions
Passive surveillance infection prevalence
Data on laboratory testing were available for 97.4% of I. pacificus and 99.0%–99.5% of I. scapularis, depending on the pathogen. The most prevalent tick-borne pathogen was B. burgdorferi, found in 18.8% of I. scapularis (95% CI: 18.00–19.55), but only 0.3% of I. pacificus (95% CI: 0.05–0.97). Other tick-borne pathogens and co-infections were less prevalent (Table 3).
Table 3. Prevalence of Borrelia burgdorferi, Anaplasma phagocytophilum and Babesia microti infection in Ixodes pacificus and Ixodes scapularis ticks submitted through passive surveillance, Canada, 2019a,b.
| Pathogen | Infection prevalence | |||
|---|---|---|---|---|
| Ixodes pacificus | Ixodes scapularis | |||
| Single agent | Maximum likelihood estimatec | |||
| % | 95% CI | % | 95% CI | |
| Borrelia burgdorferi | 0.3 | 0.05–0.97 | 18.8 | 18.00–19.55 |
| Anaplasma phagocytophilum | N/A | N/A | 1.4 | 1.22–1.70 |
| Babesia microti | N/A | N/A | 0.1 | 0.07–0.22 |
| Any of above | 0.3 | 0.05–0.97 | 20.0 | 19.23–20.83 |
| Co-infection | Co-infection rated | |||
| % | Number co-infected ticks/number ticks tested | % | Number co-infected ticks/number ticks tested | |
| Borrelia burgdorferi + Anaplasma phagocytophilum | N/A | N/A | 0.28 | 26/9,171 |
| Borrelia burgdorferi + Babesia microti | N/A | N/A | 0.02 | 2/9,171 |
| Anaplasma phagocytophilum + Babesia microti | N/A | N/A | 0.01 | 1/9,171 |
| Any co-infection | N/A | N/A | 0.32 | 29/9,171 |
Abbreviations: CI, confidence interval; N/A, not tested
a All I. pacificus (n=691) and all I. scapularis from Alberta (n=55) were not tested for A. phagocytophilum and B. microti
b No passive surveillance was conducted in Yukon, Northwest Territories or Nunavut for I. scapularis or I. pacificus ticks. Passive tick surveillance has been discontinued in the entire province of Nova Scotia, and some regions of Ontario and Québec; however, individuals could submit ticks directly to the National Microbiology Laboratory Branch from these jurisdictions
c Maximum likelihood estimates of infection prevalence were used to account for pooled testing
d Co-infection rate was calculated only among single submissions of ticks
Prevalence of B. burgdorferi was higher in I. scapularis from multiple submissions (24.5%, 95% CI: 20.64–28.69) than from single submissions (18.5%, 95% CI: 17.71–19.29) (Table 4). Prevalence did not significantly differ by submission type for any other pathogens.
Table 4. Prevalence of Borrelia burgdorferi, Anaplasma phagocytophilum and Babesia microti infections in Ixodes scapularis ticks submitted through passive surveillance by submission type and host, Canada, 2019a.
| Characteristic | Infection prevalence Maximum likelihood estimate |
|||||||
|---|---|---|---|---|---|---|---|---|
| Borrelia burgdorferi | Anaplasma phagocytophilum | Babesia microti | Any of above | |||||
| % | 95% CI | % | 95% CI | % | 95% CI | % | 95% CI | |
| Submission typeb | ||||||||
| Single | 18.5 | 17.71–19.29 | 1.4 | 1.20–1.69 | 0.1 | 0.07–0.22 | 19.7 | 18.92–20.55 |
| Multiple | 24.5 | 20.64–28.69 | 1.7 | 0.89–3.06 | 0.2 | 0.01–0.82 | 26.3 | 22.31–30.70 |
| Hostc | ||||||||
| Human | 19.2 | 18.39–20.04 | 1.3 | 1.11–1.59 | 0.1 | 0.07–0.23 | 20.4 | 19.54–21.23 |
| Non-humand | 14.7 | 12.44–17.13 | 2.6 | 1.68–3.85 | 0.1 | 0.01–0.57 | 16.7 | 14.31–19.29 |
Abbreviation: CI, confidence interval
a No passive surveillance was conducted in Yukon, Northwest Territories or Nunavut for I. scapularis or I. pacificus ticks. Passive tick surveillance has been discontinued in the entire province of Nova Scotia, and some regions of Ontario and Québec; however, individuals could submit ticks directly to the National Microbiology Laboratory Branch from these jurisdictions
b Single submissions consist of one tick. Multiple submissions consist of two or more ticks submitted together by the same person. All I. scapularis from Alberta were considered single submissions
c Excludes I. scapularis where host is unknown or missing (n=43)
d Non-human hosts include dog, cat, environment, horse, rabbit, deer, skunk or other unspecified animal
Ixodes scapularis submitted from human hosts had higher prevalence of B. burgdorferi infection (19.2%, 95% CI: 18.39–20.04) than those submitted from non-human hosts (14.7%, 95% CI: 12.44–17.13) (Table 4). However, I. scapularis submitted from non-human hosts had higher prevalence of A. phagocytophilum infection (2.6%, 95% CI: 1.68–3.85) than those submitted from human hosts (1.3%, 95% CI: 1.11–1.59). Both B. burgdorferi-infected I. pacificus ticks were from human hosts.
Tick-borne pathogens were commonly found in ticks submitted from southern Manitoba, northwestern Ontario, southern and eastern Ontario, southern Québec and southern New Brunswick (Figure 3 and Figure 4). Over two-thirds of B. burgdorferi-infected tick submissions were within previously identified LD risk areas (72.1%; n=1,313/1,821) (Figure 3). The majority of multiple submissions came from LD risk areas (76.9%; n=186/242), of which approximately half were infected with B. burgdorferi (51.4%; n=90/175). Newfoundland and Labrador, Nova Scotia and Québec all had higher infection prevalence of B. burgdorferi than the national average for I. scapularis (Table 5). Manitoba had the highest prevalence of A. phagocytophilum and B. microti infection among all provinces.
Figure 3.
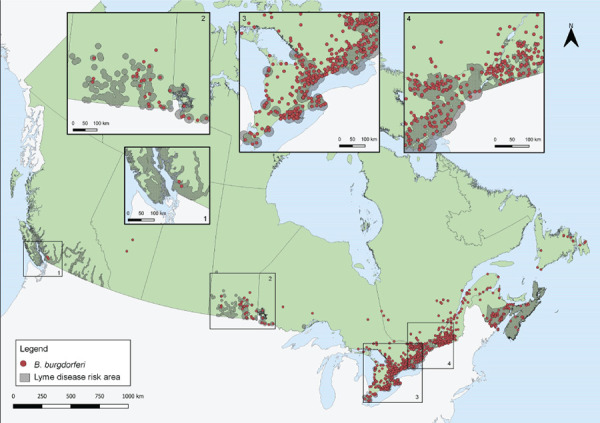
Ixodes pacificus and Ixodes scapularis ticks submitted through passive surveillance that were infected with Borrelia burgdorferi, Canada, 2019a,b,c
a Each dot represents the probable location of acquisition of at least one I. pacificus (n=2) or I. scapularis (n=1,819) single or multiple tick submission submitted through passive surveillance that was infected with B. burgdorferi
b Lyme disease risk areas are identified by the provinces as of 2020 using the methods described in the 2016 national Lyme disease case definition (28))))
c No passive surveillance was conducted in Yukon, Northwest Territories or Nunavut for I. scapularis or I. pacificus ticks. Passive tick surveillance has been discontinued in the entire province of Nova Scotia, and some regions of Ontario and Québec; however, individuals could submit ticks directly to the National Microbiology Laboratory Branch from these jurisdictions
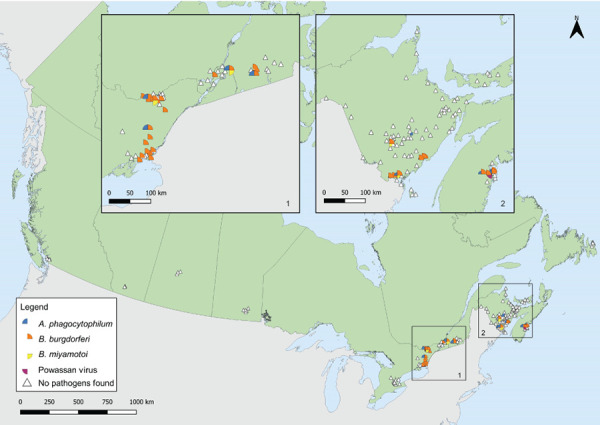
Figure 4.

Ixodes scapularis ticks submitted through passive surveillance that were infected with Anaplasma phagocytophilum, Babesia microti and co-infections, Canada, 2019a,b
a Each symbol represents the probable location of acquisition of an I. scapularis single or multiple tick submission submitted through passive surveillance that tested positive for A. phagocytophilum (n=141), B. microti (n=13) or a co-infection (n=29). Co-infections were limited to only single submissions of I. scapularis, and include B. burgdorferi + A. phagocytophilum (n=26), B. burgdorferi + B. microti (n=2) and A. phagocytophilum + B. microti (n=1)
b No passive surveillance was conducted in Yukon, Northwest Territories or Nunavut for I. scapularis or I. pacificus ticks. Passive tick surveillance has been discontinued in the entire province of Nova Scotia, and some regions of Ontario and Québec; however, individuals could submit ticks directly to the National Microbiology Laboratory Branch from these jurisdictions
Table 5. Prevalence of Borrelia burgdorferi, Anaplasma phagocytophilum and Babesia microti infection in Ixodes scapularis and Ixodes pacificus ticks submitted through passive surveillance, by province, Canada, 2019a.
| Province | Infection prevalence Maximum likelihood estimate |
|||||
|---|---|---|---|---|---|---|
| Borrelia burgdorferi | Anaplasma phagocytophilum | Babesia microti | ||||
| % | 95% CI | % | 95% CI | % | 95% CI | |
| Ixodes pacificus | ||||||
| British Columbia | 0.3 | 0.05–0.97 | N/A | N/A | N/A | N/A |
| Ixodes scapularis | ||||||
| Albertab | 5.5 | 1.45–14.01 | N/A | N/A | N/A | N/A |
| Saskatchewan | 0.0 | 0–56.15 | 0.0 | 0–56.15 | 0.0 | 0–56.15 |
| Manitoba | 18.3 | 12.94–24.68 | 10.4 | 6.38–15.81 | 2.4 | 0.78–5.63 |
| Ontario | 18.3 | 17.37–19.22 | 0.9 | 0.73–1.18 | 0.1 | 0.02–0.14 |
| Québec | 24.2 | 22.18–26.30 | 1.9 | 1.32–2.63 | 0.1 | 0.02–0.39 |
| Newfoundland and Labrador | 29.5 | 17.63–44.01 | 4.6 | 0.82–14.28 | 0.0 | 0–8.02 |
| New Brunswick | 12.8 | 10.80–15.10 | 2.6 | 1.70–3.74 | 0.3 | 0.08–0.87 |
| Nova Scotia | 26.2 | 15.38–39.82 | 3.9 | 0.70–12.31 | 0.0 | 0–6.82 |
| Prince Edward Island | 0.0 | 0–21.53 | 0.0 | 0–21.53 | 0.0 | 0–21.53 |
| Total | 18.8 | 18.00–19.55 | 1.5 | 1.22–1.70 | 0.1 | 0.07–0.22 |
Abbreviations: CI, confidence interval; N/A, not tested
a No passive surveillance was conducted in Yukon, Northwest Territories or Nunavut for I. scapularis or I. pacificus ticks. Passive tick surveillance has been discontinued in the entire province of Nova Scotia, and some regions of Ontario and Québec; however, individuals could submit ticks directly to the National Microbiology Laboratory Branch from these jurisdictions
b Excludes I. pacificus found in the province (n=1) which tested negative for B. burgdorferi
Active surveillance tick characteristics
In active surveillance, I. scapularis and I. pacificus were found at 78 of 184 surveillance sites (range of ticks found: n=0–130). Ixodes scapularis (n=1,156) were found in Manitoba, Ontario, Québec, New Brunswick, Nova Scotia and Prince Edward Island, while I. pacificus (n=10) were found in British Columbia. Regarding the instar, 51.5% (n=601/1,166) of ticks were identified as nymphs, 29.5% (n=344/1,166) were adults and 19.0% (n=221/1,166) were larvae.
Active surveillance infection prevalence
Data on laboratory testing were available for 100% of I. pacificus collected and 73.8%–98.3% of I. scapularis nymphs and adults collected, depending on the pathogen. No tick-borne pathogens were found in I. pacificus (Table 6). In I. scapularis, B. burgdorferi was identified in 26.2% of ticks tested and in four provinces: Ontario, Québec, New Brunswick, and Nova Scotia. Anaplasma phagocytophilum was identified in the same four provinces in 3.4% of I. scapularis. Borrelia miyamotoi and POWV were found in 0.5% or fewer. Figure 5 shows the locations of ticks with tick-borne pathogens collected in active surveillance.
Table 6. Infection prevalence of Ixodes scapularis and Ixodes pacificus ticks collected in active surveillance, by province, Canada, 2019a,b.
| Province | Infection prevalence | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Anaplasma phagocytophilum | Babesia microti | Borrelia burgdorferi | Borrelia miyamotoi | Powassan virus | ||||||
| Number positive tick/number tick tested | % | Number positive tick/number tick tested | % | Number positive tick/number tick tested | % | Number positive tick/number tick tested | % | Number positive tick/number tick tested | % | |
| Ixodes pacificus | ||||||||||
| British Columbia | 0/10 | 0 | 0/10 | 0 | 0/10 | 0 | 0/10 | 0 | 0/10 | 0 |
| Ixodes scapularis | ||||||||||
| Manitoba | 0/3 | 0 | 0/3 | 0 | 0/3 | 0 | 0/3 | 0 | 0/3 | 0 |
| Ontario | 14/406 | 3.5 | 0/397 | 0 | 126/410 | 30.7 | 1/410 | 0.2 | 0/188 | 0 |
| Québec | 2/141 | 1.4 | 0/141 | 0 | 28/141 | 19.8 | 1/141 | 0.7 | 0/141 | 0 |
| New Brunswick | 8/194 | 4.1 | 0/194 | 0 | 41/194 | 21.1 | 3/194 | 1.6 | 0/194 | 0 |
| Nova Scotia | 7/169 | 4.1 | 0/169 | 0 | 46/169 | 27.2 | 0/169 | 0 | 1/169 | 0.6 |
| Prince Edward Island | 0/2 | 0 | 0/2 | 0 | 0/2 | 0 | 0/2 | 0 | 0/2 | 0 |
| Total | 31/915 | 3.4 | 0/906 | 0 | 241/919 | 26.2 | 5/919 | 0.5 | 1/697 | 0.1 |
a No I. scapularis or I. pacificus ticks were collected or tested in Alberta, Saskatchewan or Newfoundland and Labrador through active surveillance. No active surveillance was conducted in Yukon, Northwest Territories or Nunavut for I. scapularis or I. pacificus ticks
b Infection prevalence is influenced by varying level of effort of active surveillance between provinces and seasonal variation when active surveillance took place. Infection prevalence should be interpreted with caution as not all active surveillance conducted in 2019 in Canada is included
Figure 5.
Ixodes scapularis and Ixodes pacificus ticks with associated pathogens collected through active surveillance, Canada, 2019a,b
a Each symbol represents an active surveillance site where B. burgdorferi (n=38), A. phagocytophilum (n=12), B. miyamotoi (n=4), or Powassan virus (n=1) were found in I. scapularis ticks. There were 142 sites where no tick-borne pathogens were identified in ticks, including sites where no I. scapularis or I. pacificus were found (n=108). No active surveillance was conducted in Yukon, Northwest Territories or Nunavut for I. scapularis or I. pacificus ticks. The presence or absence of infected I. scapularis ticks is influenced by varying level of effort of active surveillance between provinces and seasonal variation when active surveillance took place. Infection prevalence should be interpreted with caution as not all active surveillance conducted in 2019 in Canada is included
b Number of ticks tested: British Columbia (n=10), Alberta n=(0), Saskatchewan (n=0), Manitoba (n=3), Ontario (n=188–406 depending on pathogen), Québec (n=141), Newfoundland and Labrador (n=0), New Brunswick (n=194), Nova Scotia (n=169) and Prince Edward Island (n=2)
Discussion
In 2019, 9,858 I. scapularis and 691 I. pacificus were submitted in passive surveillance in eight provinces. Of these, 20.0% of I. scapularis and 0.3% of I. pacificus were infected with at least one of the tick-borne pathogens tested, including B. burgdorferi, A. phagocytophilum or B. microti. Active surveillance identified four tick-borne pathogens among I. scapularis collected in four provinces, and no tick-borne pathogens among the few I. pacificus collected.
In passive surveillance, one I. pacificus with no travel history was identified in Alberta, outside of British Columbia where reproducing populations are known to be established. Ixodes pacificus have been found in the province before on migratory birds ( ( ((29)))), or from human or animal hosts mostly associated with travel ( ( ((20)))).
Ticks were submitted through passive surveillance in every month, highlighting the potential year-round risk (depending on location and weather) of exposure to ticks, which may or may not be infected with tick-borne pathogen(s). Ixodes spp. ticks, for example, were often found in western Canada in the winter but were rarely infected ( ( ((23)))). The single peak of I. pacificus tick submissions in the spring has historically been observed in British Columbia ( ( ((23)))) and in the western United States ( ( ((30)))), as nymphs and adults are both active during the cooler spring months ( ( ((31)))). Bimodal peaks for adult I. scapularis in late spring and autumn have been previously observed in central and eastern Canada ( ( ((3,16,32)))), and are consistent with adult I. scapularis activity in a 3 to 4-year lifecycle extended, in part, by cooler spring temperatures ( ( ((31,33)))). Nymphs of both species, which are most implicated in LD transmission ( ( ((34)))), peak during the late spring to summer months when LD onset in humans also peaks ( ( ((9)))).
Compared to most recent estimates, infection prevalence of B. burgdorferi among I. pacificus ticks in British Columbia (0.3%) was consistent with annual rates from 2002 to 2018 between 0.1 and 0.4% ( ( ((23)))). In Manitoba, infection prevalence among I. scapularis was lower (18.3%) than the 2018 minimum infection rate of 20.7% ( ( ((35)))). In Ontario, infection prevalence among I. scapularis increased to 18.3% from the 2011–2017 rate of 15.8% ( ( ((36)))). In Québec, infection prevalence also increased to 24.2% from 17.6% in I. scapularis adults from 2009 to 2015 ( ( ((37)))). Inter and intra-provincial variability in annual prevalence is influenced, however, by annual variation in weather, effort of surveillance, history of established vector populations and habitat suitability.
Prevalence of I. scapularis being infected with at least one of the tick-borne pathogens tested was higher in multiple submissions than single submissions. As multiple submissions are indicators of tick establishment in a given area ( ( ((38)))), this suggests higher infection prevalence among established tick populations.
Over two-thirds of B. burgdorferi-infected ticks had probable locations of acquisition within LD risk areas. The LD risk areas are identified by the provinces using the methods described in the 2016 national LD case definition ( ( ((28)))) and are regularly updated to incorporate new surveillance data. Borrelia burgdorferi-infected ticks collected outside of these known LD risk areas may be adventitious ticks, brought to these areas by migratory birds or terrestrial hosts ( ( ((18)))). Public health authorities and clinicians should be aware that risk of exposure to infected ticks exists outside of known LD risk areas. Increasing the collaborative effort of active surveillance can support the timely recognition of new LD risk areas. Promptly identifying and removing ticks, regardless of their locality of acquisition, can prevent transmission of tick-borne pathogens.
In active surveillance, there was geographic variability in infection prevalence, similar to findings from passive surveillance. Conducting standardized and consistent active surveillance across the country can help identify new LD-risk areas and detect other emerging tick-borne pathogens in known LD-risk areas, thereby informing local risk of exposure to TBD.
While B. burgdorferi was the most prevalent tick-borne pathogen in both passive and active surveillance, A. phagocytophilum, B. microti, B. miyamotoi and POWV were also detected. All provinces, however, had lower infection prevalence than hyper-endemic areas in the northeastern United States. For example, I. scapularis adults collected in Maine through passive surveillance had B. burgdorferi, A. phagocytophilum and B. microti infection prevalence of 42.4%, 11.1% and 6.5%, respectively ( ( ((39)))).
Ongoing climate and environmental changes affect TBD risk in a variety of ways, by altering populations of ticks and their animal hosts, as well as increasing human exposure to ticks ( ( ((1)))). As current projections predict an increased risk of TBD from expansion of Ixodes spp. habitat in the future ( ( ((1,5,40)))), continued surveillance can monitor changes in tick distribution and infection prevalence. More studies are also needed to understand the emergence and ecology of other tick-borne pathogens across Canada, which may differ from B. burgdorferi, for example, in their enzootic transmission cycles ( ( ((41)))).
Strengths and limitations
This inaugural article combining active and passive tick surveillance presents a national snapshot of tick vectors and their emerging associated pathogens. By integrating the two types of surveillance, the strengths and weaknesses of the individual systems are complemented. Whereas active surveillance is resource-intensive and therefore limited in geographic scope, passive surveillance programs can be implemented on a larger geographic scale; however, passive surveillance lacks specificity as it often collects adventitious ticks seeded by migratory birds, especially ticks collected from companion animal hosts which readily acquire ticks from the environment ( ( ((18,38)))).
There are several limitations to this study. Provincial passive surveillance programs, and the effort and timing of active surveillance, vary across Canada due to resource limitations or logistics. Passive tick surveillance has been discontinued or limited to specific hosts in several regions. Further, passive tick surveillance can be limited by public awareness, and geographic or host-specific biases in tick submissions ( ( ((3,42,43)))). Not all active surveillance conducted in Canada in 2019 was included in this study; data from the many groups that conduct active surveillance, which includes university researchers, Indigenous communities and local or provincial public health units, was not all available. These limitations lead to underestimating the number of ticks, which affects the accuracy of infection prevalence. Lastly, it may be inappropriate to pool data from multiple active and passive surveillance systems due to differences in methodology between sources.
Conclusion
Passive and active surveillance identified both I. scapularis and I. pacificus across Canada in varying amounts depending on location, including some ticks which were infected with tick-borne pathogen(s). Both passive and active tick surveillance have utility in signalling and confirming new LD risk areas, which can be used to inform public health authorities where environmental risk for LD occurs. This information is used to communicate the local risk of LD and TBD to the public as well as to healthcare workers. Continued surveillance will be crucial for monitoring any expansion of areas at risk of exposure to ticks and tick-borne pathogens, and to appropriately target public health interventions such as education and awareness campaigns towards at-risk areas.
Acknowledgements
We thank all those involved with tick collection and testing at regional, provincial and national levels, including members of the public who submitted ticks. Yann Pelcat created the Lyme disease risk area shapefile in Figure 3. Drag sampling in New Brunswick was a collaboration between the New Brunswick Department of Health; the New Brunswick Department of Agriculture, Aquaculture and Fisheries; and the University of New Brunswick.
Competing interests: None.
Funding: This study was supported by Public Health Agency of Canada (PHAC). Passive surveillance from British Columbia was supported by the BC Centre for Disease Control Foundation. Active surveillance conducted by the Canadian Lyme Sentinel Network (CaLSeN), which is part of the Canadian Lyme Disease Research Network, was funded by the Canadian Institutes of Health Research. The Institut national de santé publique du Québec (INSPQ) and Ministère de la Santé et des Services sociaux (MSSS) funded data collection in 12 sampling sites in Québec as part of annual surveillance activities. Active surveillance conducted by the New Brunswick Department of Health and the University of Ottawa were funded by PHAC.
References
- 1.Bouchard C, Dibernardo A, Koffi J, Wood H, Leighton PA, Lindsay LR. N Increased risk of tick-borne diseases with climate and environmental changes. Can Commun Dis Rep 2019;45(4):83–9. 10.14745/ccdr.v45i04a02 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ogden NH, Lindsay LR, Morshed M, Sockett PN, Artsob H. The emergence of Lyme disease in Canada. CMAJ 2009;180(12):1221–4. 10.1503/cmaj.080148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Nelder MP, Russell C, Lindsay LR, Dhar B, Patel SN, Johnson S, Moore S, Kristjanson E, Li Y, Ralevski F. Population-based passive tick surveillance and detection of expanding foci of blacklegged ticks Ixodes scapularis and the Lyme disease agent Borrelia burgdorferi in Ontario, Canada. PLoS One 2014;9(8):e105358. 10.1371/journal.pone.0105358 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ogden NH, Koffi JK, Pelcat Y, Lindsay LR. Environmental risk from Lyme disease in central and eastern Canada: a summary of recent surveillance information. Can Commun Dis Rep 2014;40(5):74–82. 10.14745/ccdr.v40i05a01 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Leighton PA, Koffi JK, Pelcat Y, Lindsay LR, Ogden NH. Predicting the speed of tick invasion: an empirical model of range expansion for the Lyme disease vector Ixodes scapularis in Canada. J Appl Ecol 2012;49(2):457–64. 10.1111/j.1365-2664.2012.02112.x [DOI] [Google Scholar]
- 6.Ogden NH, Ben Beard C, Ginsberg HS, Tsao JI. Possible effects of climate change on Ixodid ticks and the pathogens they transmit: predictions and observations. J Med Entomol 2021;58(4):1536–45. 10.1093/jme/tjaa220 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ogden NH, Mechai S, Margos G. Changing geographic ranges of ticks and tick-borne pathogens: drivers, mechanisms and consequences for pathogen diversity. Front Cell Infect Microbiol 2013;3:46. 10.3389/fcimb.2013.00046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ogden NH, Lindsay LR. Effects of climate and climate change on vectors and vector-borne diseases: ticks are different. Trends Parasitol 2016;32(8):646–56. 10.1016/j.pt.2016.04.015 [DOI] [PubMed] [Google Scholar]
- 9.Gasmi S, Ogden NH, Lindsay LR, Burns S, Fleming S, Badcock J, Hanan S, Gaulin C, Leblanc MA, Russell C, Nelder M, Hobbs L, Graham-Derham S, Lachance L, Scott AN, Galanis E, Koffi JK. Surveillance for Lyme disease in Canada: 2009-2015. Can Commun Dis Rep 2017;43(10):194–9. 10.14745/ccdr.v43i10a01 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Public Health Agency of Canada. Lyme disease surveillance in Canada: Preliminary annual report 2019. Ottawa, ON: PHAC; 2022 (accesssed 2022-03-30). https://www.canada.ca/en/public-health/services/publications/diseases-conditions/lyme-disease-surveillance-report-2019.html
- 11.Kulkarni MA, Berrang-Ford L, Buck PA, Drebot MA, Lindsay LR, Ogden NH. Major emerging vector-borne zoonotic diseases of public health importance in Canada. Emerg Microbes Infect 2015;4:e33. 10.1038/emi.2015.33 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Nelder MP, Russell CB, Lindsay LR, Dibernardo A, Brandon NC, Pritchard J, Johnson S, Cronin K, Patel SN. Recent emergence of Anaplasma phagocytophilum in Ontario, Canada: early serological and entomological indicators. Am J Trop Med Hyg 2019;101(6):1249–58. 10.4269/ajtmh.19-0166 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bullard JM, Ahsanuddin AN, Perry AM, Lindsay LR, Iranpour M, Dibernardo A, Van Caeseele PG. The first case of locally acquired tick-borne Babesia microti infection in Canada. Can J Infect Dis Med Microbiol 2014;25(6):e87–9. 10.1155/2014/209521 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kadkhoda K, Dumouchel C, Brancato J, Gretchen A, Krause PJ. Human seroprevalence of Borrelia miyamotoi in Manitoba, Canada, in 2011-2014: a cross-sectional study. CMAJ Open 2017;5(3):E690–3. 10.9778/cmajo.20170070 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bogaty C, Drebot M. Powassan virus - an emerging public health concern. CMAJ 2018;190(15):E472. 10.1503/cmaj.171305 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ogden NH, Trudel L, Artsob H, Barker IK, Beauchamp G, Charron DF, Drebot MA, Galloway TD, O’Handley R, Thompson RA, Lindsay LR. Ixodes scapularis ticks collected by passive surveillance in Canada: analysis of geographic distribution and infection with Lyme borreliosis agent Borrelia burgdorferi. J Med Entomol 2006;43(3):600–9. 10.1093/jmedent/43.3.600 [DOI] [PubMed] [Google Scholar]
- 17.Bouchard C, Leonard E, Koffi JK, Pelcat Y, Peregrine A, Chilton N, Rochon K, Lysyk T, Lindsay LR, Ogden NH. The increasing risk of Lyme disease in Canada. Can Vet J 2015;56(7):693–9. [PMC free article] [PubMed] [Google Scholar]
- 18.Ogden NH, Bouchard C, Kurtenbach K, Margos G, Lindsay LR, Trudel L, Nguon S, Milord F. Active and passive surveillance and phylogenetic analysis of Borrelia burgdorferi elucidate the process of Lyme disease risk emergence in Canada. Environ Health Perspect 2010;118(7):909–14. 10.1289/ehp.0901766 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Guillot C, Badcock J, Clow K, Cram J, Dergousoff S, Dibernardo A, Evason M, Fraser E, Galanis E, Gasmi S, German GJ, Howse DT, Jardine C, Jenkins E, Koffi J, Kulkarni M, Lindsay LR, Lumsden G, McKay R, Moore K, Morshed M, Munn D, Nelder M, Nocera J, Ripoche M, Rochon K, Russell C, Slatculescu A, Talbot B, Thivierge K, Voordouw M, Bouchard C, Leighton P. Sentinel surveillance of Lyme disease risk in Canada, 2019: Results from the first year of the Canadian Lyme Sentinel Network (CaLSeN). Can Commun Dis Rep 2020;46(10):354–61. 10.14745/ccdr.v46i10a08 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Government of Alberta. Tick surveillance - Interactive map. Tableau Public; 2020 (accessed 2021-07-15). https://public.tableau.com/app/profile/ellehojpublic/viz/Ticks_in_AB/AlbertaTicks
- 21.Schillberg E, Lunny D, Lindsay LR, Nelder MP, Russell C, Mackie M, Coats D, Berry A, Young Hoon KN. Distribution of Ixodes scapularis in northwestern Ontario: results from active and passive surveillance activities in the Northwestern Health Unit catchment area. Int J Environ Res Public Health 2018;15(10):2225. 10.3390/ijerph15102225 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Dibernardo A, Cote T, Ogden NH, Lindsay LR. The prevalence of Borrelia miyamotoi infection, and co-infections with other Borrelia spp. in Ixodes scapularis ticks collected in Canada. Parasit Vectors 2014;7:183. 10.1186/1756-3305-7-183 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Morshed MG, Lee MK, Boyd E, Mak S, Fraser E, Nguyen J, Dykstra EA, Otterstatter M, Henry B, Galanis E. Passive tick surveillance and detection of Borrelia species in ticks from British Columbia, Canada: 2002-2018. Vector Borne Zoonotic Dis 2021;21(7):490–7. 10.1089/vbz.2020.2743 [DOI] [PubMed] [Google Scholar]
- 24.Government of Alberta. Tick surveillance 2019: Summary. Edmonton, AB: Gov’t Alberta; 2020 (accessed 2021-09-15). https://open.alberta.ca/dataset/f0b7698f-03d4-4d32-858f-141ec7c3c108/resource/91920d4a-96df-4796-93f2-91262d748c68/download/health-tick-surveillance-2019-summary-report.pdf
- 25.Burrows H, Talbot B, McKay R, Slatculescu A, Logan J, Thickstun C, Lindsay LR, Dibernardo A, Koffi JK, Ogden NH, Kulkarni MA. A multi-year assessment of blacklegged tick (Ixodes scapularis) population establishment and Lyme disease risk areas in Ottawa, Canada, 2017-2019. PLoS One 2021;16(2):e0246484. 10.1371/journal.pone.0246484 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Biggerstaff BJ. West Nile virus. Mosquito Surveillance Software. Atlanta (GA): CDC; 2009. https://www.cdc.gov/westnile/resourcepages/mosqSurvSoft.html [Google Scholar]
- 27.Walter SD, Hildreth SW, Beaty BJ. Estimation of infection rates in population of organisms using pools of variable size. Am J Epidemiol 1980;112(1):124–8. 10.1093/oxfordjournals.aje.a112961 [DOI] [PubMed] [Google Scholar]
- 28.Public Health Agency of Canada. Lyme disease 2016 case definition. Ottawa, ON: PHAC; 2017 (accessed 2021-10-22). https://www.canada.ca/en/public-health/services/diseases/lyme-disease/surveillance-lyme-disease/case-definition.html
- 29.Morshed MG, Scott JD, Fernando K, Beati L, Mazerolle DF, Geddes G, Durden LA. Migratory songbirds disperse ticks across Canada, and first isolation of the Lyme disease spirochete, Borrelia burgdorferi, from the avian tick, Ixodes auritulus. J Parasitol 2005;91(4):780–90. 10.1645/GE-3437.1 [DOI] [PubMed] [Google Scholar]
- 30.Xu G, Pearson P, Dykstra E, Andrews ES, Rich SM. Human-biting Ixodes ticks and pathogen prevalence from California, Oregon, and Washington. Vector Borne Zoonotic Dis 2019;19(2):106–14. 10.1089/vbz.2018.2323 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Eisen RJ, Eisen L, Ogden NH, Beard CB. Linkages of weather and climate with Ixodes scapularis and Ixodes pacificus (Acari: Ixodidae), enzootic transmission of Borrelia burgdorferi, and Lyme disease in North America. J Med Entomol 2016;53(2):250–61. 10.1093/jme/tjv199 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Gasmi S, Ogden NH, Leighton PA, Lindsay LR, Thivierge K. Analysis of the human population bitten by Ixodes scapularis ticks in Quebec, Canada: increasing risk of Lyme disease. Ticks Tick Borne Dis 2016;7(6):1075–81. 10.1016/j.ttbdis.2016.09.006 [DOI] [PubMed] [Google Scholar]
- 33.Ogden NH, Lindsay LR, Beauchamp G, Charron D, Maarouf A, O’Callaghan CJ, Waltner-Toews D, Barker IK. Investigation of relationships between temperature and developmental rates of tick Ixodes scapularis (Acari: Ixodidae) in the laboratory and field. J Med Entomol 2004;41(4):622–33. 10.1603/0022-2585-41.4.622 [DOI] [PubMed] [Google Scholar]
- 34.Mead PS. Epidemiology of Lyme disease. Infect Dis Clin North Am 2015. Jun;29(2):187–210. 10.1016/j.idc.2015.02.010 [DOI] [PubMed] [Google Scholar]
- 35.Government of Manitoba. Manitoba Health, Seniors and Active Living, Population Health Division, Population and Public Health Branch CDC. Manitoba Annual Tick-borne Disease Report 2018. Winnipeg, MB: Government of Manitoba; 2020 (accessed 2021-09-29). https://www.gov.mb.ca/health/publichealth/cdc/tickborne/docs/tbd_report2018.pdf
- 36.Nelder MP, Russell CB, Dibernardo A, Clow KM, Johnson S, Cronin K, Patel SN, Lindsay LR. Monitoring the patterns of submission and presence of tick-borne pathogens in Ixodes scapularis collected from humans and companion animals in Ontario, Canada (2011-2017). Parasit Vectors 2021;14(1):260. 10.1186/s13071-021-04750-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Gasmi S, Ogden NH, Ripoche M, Leighton PA, Lindsay RL, Nelder MP, Rees E, Bouchard C, Vrbova L, Rusk R, Russell C, Pelcat Y, Mechai S, Kotchi SO, Koffi JK. Detection of municipalities at-risk of Lyme disease using passive surveillance of Ixodes scapularis as an early signal: A province-specific indicator in Canada. PLoS One 2019;14(2):e0212637. 10.1371/journal.pone.0212637 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Gasmi S, Bouchard C, Ogden NH, Adam-Poupart A, Pelcat Y, Rees EE, Milord F, Leighton PA, Lindsay RL, Koffi JK, Thivierge K. Evidence for increasing densities and geographic ranges of tick species of public health significance other than Ixodes scapularis in Québec, Canada. PLoS One 2018;13(8):e0201924. 10.1371/journal.pone.0201924 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Rounsville TF, Dill GM, Bryant AM, Desjardins CC, Dill JF. Statewide passive surveillance of Ixodes scapularis and associated pathogens in Maine. Vector Borne Zoonotic Dis 2021;21(6):406–12. 10.1089/vbz.2020.2724 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Koffi JK, Leighton PA, Pelcat Y, Trudel L, Lindsay LR, Milord F, Ogden NH. Passive surveillance for I. scapularis ticks: enhanced analysis for early detection of emerging Lyme disease risk. J Med Entomol 2012;49(2):400–9. 10.1603/ME11210 [DOI] [PubMed] [Google Scholar]
- 41.Eisen RJ, Eisen L. The blacklegged tick, Ixodes scapularis: an increasing public health concern. Trends Parasitol 2018;34(4):295–309. 10.1016/j.pt.2017.12.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Johnson JL, Ginsberg HS, Zhioua E, Whitworth UG Jr, Markowski D, Hyland KE, Hu R. Passive tick surveillance, dog seropositivity, and incidence of human lyme disease. Vector Borne Zoonotic Dis 2004;4(2):137–42. 10.1089/1530366041210710 [DOI] [PubMed] [Google Scholar]
- 43.Ogden NH, Feil EJ, Leighton PA, Lindsay LR, Margos G, Mechai S, Michel P, Moriarty TJ. Evolutionary aspects of emerging Lyme disease in Canada. Appl Environ Microbiol 2015;81(21):7350–9. 10.1128/AEM.01671-15 [DOI] [PMC free article] [PubMed] [Google Scholar]