

Abstract
Background:
Obesity has been a major concern due to its increasing prevalence and associated metabolic complications. Body mass index (BMI) assesses general obesity, but it does not distinguish between muscle and fat accumulations, so using only BMI can lead to an erroneous result. Waist circumference (WC), a marker of central obesity, predicted mortality risk better than BMI. However, WC can be affected by abdominal distension, is time-consuming, and may not be culture-sensitive. Neck circumference (NC) is devoid of these disadvantages and is believed to be an index of upper body fat distribution. This study aimed to assess the association of neck circumference with general and central obesity and to identify the cut-off points for evaluating obesity in young adults using NC.
Material and Methods:
Height, weight, waist, and hip circumference were measured to determine BMI and waist-hip ratio. NC was measured at the level of the mid-cervical spine and mid-anterior neck in a standing position with the arms hanging freely. For males with a laryngeal prominence, NC was measured just below the prominence.
Results:
In total, 357 (170 male and 187 female) young, healthy Indian adults aged 18–25 participated. Neck circumference (NC) is significantly associated with BMI and WC in both genders. We found the best cut-off for male and female participants to be ≥34 cm and ≥30.5 cm, with a sensitivity of 88.3% and 84.4% for assessing obesity.
Conclusion:
NC may be a better alternative to BMI and WC as a marker to assess obesity since it is more practical, simple, inexpensive, time-saving, and less invasive.
Keywords: Body mass index, neck circumference, obesity, waist circumference
INTRODUCTION
Today in the modern era, sedentary lifestyle, industrialization, the imbalance between energy intake and expenditure, and complex interaction of genetic, physiological, behavioral, and environmental factors are continuously expanding the problem of increasing weight in the young population, and it poses a significant risk for the cardiovascular diseases among them.[1-3] According to the NFHS 5 data, the percentage of overweight and obese is 22.9% in male and 24% in female participants, and there are notable increases in the burden of non-communicable diseases (NCDs).[4,5] Overweight and obesity prevalence in India is increasing more rapidly than the world’s average; hence, early diagnosis and prevention are essential priorities for which there is a need for accurate diagnostic methods.
Although there are many methods such as Dual Energy X-ray Absorption (DEXA), Bioelectrical impedance analysis (BIA), Computed tomography (CT), and Magnetic resonance for assessing body composition, which can differentiate muscle and fat accumulations, and their distribution are available, these methods are not commonly employed in a community setting as there is radiation exposure, not cost-effective, and need trained experts.[6]
Body mass index (BMI) or the Quetelet index has been commonly employed for assessing overweight and obesity in the general population but does not represent the actual body composition. It does not differentiate muscle mass, fat mass, or distribution. Literature show that fat distribution has been implicated in cardiovascular risk rather than general obesity. Moreover, the typical Asian Indian phenotype is the “thin-fat Indian,” which means that Asian Indians have greater body fat and lesser muscle mass compared to other ethnic groups such as Caucasians. Asian Indians have thinner limbs, which is suggestive of lesser muscle mass. Despite being thin, they are centrally obese, with a higher waist/hip ratio and higher subscapular/triceps skinfold ratio.[7] So, using BMI as a screening tool for obesity in community settings is inadequate and may pose many practical problems such as the calculation itself can be cumbersome and the lack of calibrated weighing scales.[6] So, other methods such as waist circumference (WC) and waist-to-hip ratios are used to identify central obesity. Several studies have found that WC predicted mortality risk better than BMI. Furthermore, WC is extremely sensitive to the distribution of body fat and body size and correlates with BMI.[8] But it is time-consuming; measurement varies with respiration, and postprandial distension of the abdomen, cannot be used in pregnancy. These measures can be challenging in conservative populations, especially in female population in a community setting, and are culturally sensitive.[9,10]
To prevent obesity and its complications, it is essential to have more accessible and more practical alternative tool for screening obesity in community settings. Neck circumference, devoid of the disadvantages mentioned earlier, is believed to be an index of upper body fat distribution and can be a novel anthropometric alternative for measuring and classifying obese, overweight, and normal weight.[11,12] Neck circumference requires minimal expertise, equipment, and skill to measure and can be done by a health worker in the community setup. It is more culturally acceptable than WC, and most importantly, it has the advantage of predicting many cardiometabolic risks other than obesity.
Studies evaluating the possible use of NC as an indicator of overweight and obesity using modified Asian BMI cut-off in a healthy young population are limited. The purpose of this study is to find the association of neck circumference with general obesity and central obesity and identify the cut-off points for assessing obesity in young adults using NC.
SUBJECTS AND METHODS
This is a cross-sectional study on 357 young, healthy adults aged 18 and 25 years who consented to participate in the study and were recruited by a convenient random sampling technique. Subjects with thyroid enlargement, thyroid nodules, neck abnormalities, and pregnant women were excluded from the study.
Sample size calculation: The sensitivity and specificity of the neck circumference to measure overweight and obesity was assumed to be 50%. The prevalence of overweight and obesity in India was taken as 40% as per a study conducted by Venkatrao M.[13] An allowable error of 10% and with 5% precision was taken at a 95% confidence interval. The minimum number of samples required was 357.
This study was approved by the Institutional Research Committee and the Institutional Human Ethics committee (IHEC No: MGMCRI/IRC/04/2020/32/IHEC/179). The Declaration of Helsinki and National Ethical Guidelines for Biomedical and Health Research 2017 by the Indian Council of Medical Research were followed throughout the study.
Anthropometric measurement
The study participant’s weight was measured using a digital weighing scale (Salter, Kent, England) with accuracy to the nearest 100 gm, in minimal clothing, with the subject standing in the center of the scale without support and with the weight distributed evenly on both feet.
Height was measured by a calibrated stadiometer on hard and level ground with the subject standing upright with feet together, the back in contact with the stadiometer, and the head in the Frankfort plane.
A non-stretchable tape was used for measuring WC at the midpoint between the lower costal (10th rib) border and the iliac crest at the end of a gentle, normal expiration with abdomen muscles relaxed with the subject standing and with forearms crossed over the thorax.
Hip circumference was measured at the widest portion of the buttocks with the subject standing and forearms crossed over the thorax, gluteal muscles relaxed, and feet together.
NC was measured at the mid-cervical spine and mid-anterior neck level in a standing position with the arms hanging freely. For male participants with a laryngeal prominence, NC was measured just below the prominence.
All measurements were done as per the International Society for the Advancement of Kinanthropometry (ISAK) recommendation.
Asian BMI criterion was considered the standard for defining overweight and obesity. A BMI of 18.5 to 22.99 kg/m2 was considered normal. A BMI of 23–24.99 kg/m2 was categorized as overweight, and BMI more than or equal to 25 kg/m2 was defined as obese.[14] Central obesity was defined by Asian cut-off points of WC ≥90 cm in male and ≥80 cm in female participants.[15]
Statistical analyses were done using SPSS 17.0 (IBM Corp., Armonk, NY, USA) software. The Shapiro–Wilk test was done to check for data normality. All normally distributed data were represented as mean and standard deviation. Pearson correlation coefficient was done to find the association between NC and other anthropometric parameters. Linear regression was done to find the effect of NC on BMI and WC; Receiver operating characteristic (ROC) analysis was used to determine the gender-specific optimal cut-off value for NC to identify obesity and to determine the sensitivity and specificity. P-value of <0.05 was considered statistically significant.
RESULTS
In this study, 357 (48% male and 52% female participants) young, healthy Indian adults between 18 and 25 years participated. Table 1 provides the baseline characteristics of the study population. Male participants were heavier and taller than female participants. Age and BMI were comparable between male and female participants. WC was higher in male participants, but HC and WHR were not statistically different. NC was lesser in female compared to male participants.
Table 1.
Characteristics of the study population
| Parameter | Male (n=170) | Female (n=187) | P |
|---|---|---|---|
| Age (year) | 21.14±2.3 | 20.95±2.4 | 0.447 |
| Height (cm) | 171±13.81 | 158.2±6.1* | <0.01 |
| Weight (kg) | 75.55±12.9 | 63.14±13.07* | <0.01 |
| #BMI (kg/m2) | 25.85±4.3 | 25.4±5.1 | 0.410 |
| Waist circumference (cm) | 85.3±11.1 | 80.57±11.4* | <0.01 |
| Hip circumference (cm) | 100.6±8.7 | 99.1±13.5 | 0.233 |
| Waist-Hip ratio | 0.84±0.06 | 0.79±0.06 | 0.225 |
| Neck circumference (cm) | 35.4±3.2 | 30.4±2.23* | <0.01 |
#BMI - Body Mass Index, *Statistically significant
Table 2 shows the BMI category of the study population which shows that 50.7% of the study population was obese.
Table 2.
Body Mass index category of the study population
| BMI category | Male (170) | Female (187) | ||
|---|---|---|---|---|
|
|
|
|||
| Frequency (n) | Proportion (%) | Frequency (n) | Proportion (%) | |
| Normal | 54 | 31.8% | 73 | 39% |
| Overweight | 19 | 11.2% | 30 | 16% |
| Obese | 97 | 57% | 84 | 45% |
#BMI - Body Mass Index
Table 3 shows the positive correlation of weight, height, BMI, WC, and waist-hip ratio with neck circumference and revealed a positive correlation with all variables except waist-hip ratio in female participants and height in both genders.
Table 3.
Association between neck circumference and other anthropometric indices
| Anthropometric measures | Male | Female | ||
|---|---|---|---|---|
|
|
|
|||
| r | P | r | P | |
| Weight (Kg) | 0.734 | <0.01* | 0.711 | <0.01* |
| Height (Cm) | 0.005 | 0.997 | 0.000 | 0.997 |
| #BMI (Kg/m2) | 0.761 | <0.01* | 0.725 | <0.01* |
| Waist circumference (cm) | 0.744 | <0.01* | 0.849 | <0.01* |
| Hip circumference (cm) | 0.661 | <0.01* | 0.582 | <0.01* |
| Waist Hip ratio | 0.445 | <0.01* | 0.139 | 0.58 |
#BMI=Body Mass Index, *Statistically significant
Linear regression analysis shows a significant positive association of neck circumference with BMI, a measure of general obesity, and WC, a measure of central obesity in both male and female participants, as shown in Table 4.
Table 4.
Linear regression analysis evaluating neck circumference association with general and central obesity
| Parameter | R 2 | β-coefficient | P |
|---|---|---|---|
| Male | |||
| #BMI | 0.579 | 0.761 | <0.01* |
| Waist circumference | 0.554 | 0.744 | <0.01* |
| Female | |||
| #BMI | 0.523 | 0.725 | <0.01* |
| Waist circumference | 0.721 | 0.849 | <0.01* |
#BMI - Body Mass Index, *Statistically significant.
ROC analysis was done separately for male and female participants. The area under the curve for male and female participants of NC with BMI was 0.891 (0.880-0.913) and 0.812 (0.743-0.881), and WC was 0.866 (0.814–0.918) and 0.900 (0.856–0.945), respectively [Figures 1 and 2]. So, neck circumference can be used to evaluate obesity in both male and female participants. We found the best cut-off for male and female participants to be 34 cm and 30.5 cm, respectively. Furthermore, using these cut-offs, we found that the sensitivity and specificity for male participants are depicted in Table 5, and for female participants are depicted in Table 6.
Figure 1.
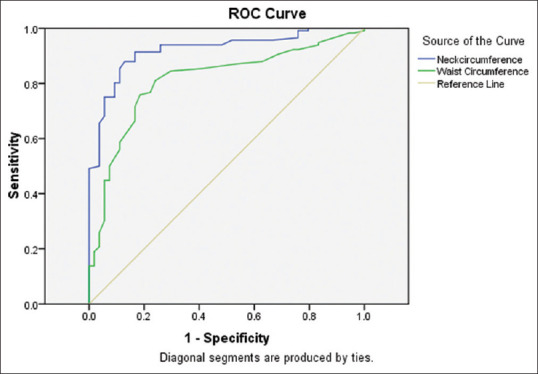
Receiver operating characteristic analysis for male participants.
Figure 2.
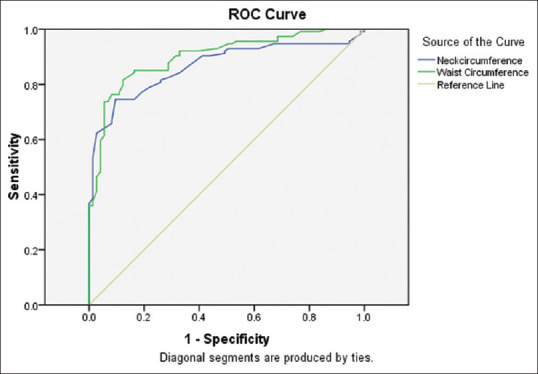
Receiver operating characteristic analysis for female participants.
Table 5.
Comparison between neck circumference and BMI in male participants
| Males | Obese (NC ≥34 cm) | Non-Obese (NC <34 cm) | Total | Sensitivity and specificity |
|---|---|---|---|---|
| Obese (BMI ≥23 kg/m2) | 99 | 17 | 116 | Sensitivity=88.3% |
| Non-obese (BMI <23 kg/m2) | 13 | 41 | 54 | Specificity=70.6% |
| Total | 112 | 58 | 170 |
BMI - Body Mass Index, NC - Neck Circumference
Table 6.
Comparison between neck circumference and BMI in female participants
| Females | Obese (NC ≥30.5 cm) | Non-Obese (NC <30.5 cm) | Total | Sensitivity and specificity |
|---|---|---|---|---|
| Obese (BMI ≥23 kg/m2) | 92 | 22 | 114 | Sensitivity=84.4% |
| Nonobese BMI <23 kg/m2) | 17 | 56 | 73 | Specificity=71.7% |
| Total | 109 | 78 | 187 |
BMI=Body Mass Index, NC=Neck Circumference
Neck circumference was found to have a good discriminatory power to predict obesity as per modified Asian criteria of BMI classification on ROC analysis.
DISCUSSION
Neck circumference (NC) has been validated to be a simple measure of upper body subcutaneous fat deposition and a predictor of cardiovascular risk factors. Our study shows a positive association of NC with BMI, an indicator of general obesity, and WC, an indicator of central obesity; the upper body distribution of fat, especially with increased visceral adipose tissue, is considered to have an independent role in predicting cardiometabolic conditions.
In healthy individuals, after puberty, any change in the neck circumference is due to the accumulation of fat mass in the soft tissue space, which is present surrounding the vertebral column and cartilages of the upper part of the respiratory tract.[16] An increased upper-body fat has been associated with adverse metabolic complications and correlates positively with changes in systolic and diastolic blood pressure and type II diabetes mellitus with an increase in insulin resistance.[17]
Although limited studies that evaluated NC values in young adults exist, it is not utilized widely due to the lack of proper evidence to support the use of NC as a screening tool. Our results are in concordance with studies conducted by Hingorjo et al.[18] in 150 Pakistani dental students, which demonstrated significant gender differences with regard to NC values and showed a positive association between NC with BMI (male r = 0.861, female r = 0.703) and WC (male r = 0.861, female r = 0.703) in both genders; similarly Zaciragic et al.,[19] also in young adults, demonstrated a positive association of NC with BMI (male r = 0.70, female r = 0.53) and WC (male r = 0.48, female r = 0. 38), respectively. In a study by Özkaya et al.[20] in university students reported a positive association between NC with BMI (male r = 0.684, female r = 0.482) and WC (male r = 0.686, female r = 0.479) in both genders. Similar results in our study compared to other studies may be due to similarity in the study participants as they are all young adults.
The present study infers that neck circumference correlates with weight, BMI, WC, and hip circumference. Based on ROC curve analysis, it can be interpreted that neck circumference is a fair test to evaluate general obesity and central obesity in young adults of both genders. Furthermore, many have reported different population-specific cut-offs to assess the prevalence of excess adiposity using NC. Such differences in cut-off estimation could be attributed to different diagnostic standards and population variations. In a study by Hingorjo et al.[18] in 150 Pakistani dental students aged between 18 and 20 years, a similar cut-off of NC >35.7 cm (in men) and >32.2 cm (in women) was reported to assess overweight/obesity prevalence among Asian-origin adults. Patnaik et al.[21] in adolescent boys and girls had a cut-off value of 30.75 (sensitivity 79.2% and specificity 68%) and 29.75 (sensitivity 72.5% and specificity 77.1%). Verma et al.[9] in adults aged 20 and 60 years had a cut-off value of >37 cm (sensitivity 63.2% and specificity 84.8%) and 34 cm (sensitivity 66.9% and specificity 86.6%) in male and female participants, respectively. Aswathappa et al.[22] in adults between 18 and 65 years had a cut-off of NC >36 cm (sensitivity 71.2% and specificity 80.6%) in male and >32 cm (sensitivity 63.9% and specificity 68%) in female participants.
In addition to its association with general and central obesity, NC is also associated with metabolic syndrome, cardiometabolic risk, obstructive sleep apnea, and perioperative adverse respiratory events, a feature that increases its potential application to the identification of other chronic NCDs.[23-25]
Measuring neck circumference is a socially acceptable, time-saving, and less cumbersome method to screen for obesity compared to measuring WC or BMI. From a financial point of view, it is a very cost-effective method. Thus, this method can be used in a developing country like India, facing a double burden of nutrition transition; neck circumference will be a feasible method to screen for obesity in adults. Our study has the advantage that we categorized the subjects based on Asian BMI criteria.
Limitations
The cross-sectional design of the study limits the causality of association. The study population is only young adults, so we cannot generalize the result to all populations.
In future studies, the association of neck circumference with radiological-determined fat distribution and blood parameters is recommended.
CONCLUSION
Neck circumference positively correlates with BMI, a measure of general obesity, and WC, a measure of central obesity. The cut-off of 34 cm in male and 30.5 cm in female participants will help screen the young adult population of Asian Indian origin. The sensitivity of this screening test for this cut-off was 88.39% in male and 84.4% in female participants, with a specificity of 70.6% in male and 71.7% in female participants. Neck circumference can be used as a screening tool in the community setting.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
The authors acknowledge their gratitude to all the participants of this study.
REFERENCES
- 1.Fox A, Feng W, Asal V. What is driving global obesity trends? Globalization or “modernization”? Global Health. 2019;15:32. doi: 10.1186/s12992-019-0457-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Romieu I, Dossus L, Barquera S, Blottière HM, Franks PW, Gunter M, et al. Energy balance and obesity: What are the main drivers? Cancer Causes Control. 2017;28:247–58. doi: 10.1007/s10552-017-0869-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Powell-Wiley TM, Poirier P, Burke LE, Després JP, Gordon-Larsen P, Lavie CJ, et al. Obesity and cardiovascular disease: A scientific statement from the American Heart Association. Circulation. 2021;143:e984–1010. doi: 10.1161/CIR.0000000000000973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.International Institute for Population Sciences. National Family Health Survey (NFHS-5) [Last accessed on2021 Jan 31]. Available from: http://rchiips.org/nfhs/factsh eet_NFHS-5.shtml .
- 5.Luhar S, Timæus IM, Jones R, Cunningham S, Patel SA, Kinra S, et al. Forecasting the prevalence of overweight and obesity in India to 2040. PLoS One. 2020;15:e0229438. doi: 10.1371/journal.pone.0229438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Borga M, West J, Bell JD, Harvey NC, Romu T, Heymsfield SB, et al. Advanced body composition assessment: From body mass index to body composition profiling. J Investig Med. 2018;66:1–9. doi: 10.1136/jim-2018-000722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kurpad AV, Varadharajan KS, Aeberli I. The thin-fat phenotype and global metabolic disease risk. Curr Opin Clin Nutr Metab Care. 2011;14:542–7. doi: 10.1097/MCO.0b013e32834b6e5e. [DOI] [PubMed] [Google Scholar]
- 8.Nuttall FQ. Body mass index: Obesity, BMI, and health: A critical review. Nutr Today. 2015;50:117–28. doi: 10.1097/NT.0000000000000092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Verma M, Rajput M, Sahoo SS, Kaur N. Neck circumference: Independent predictor for overweight and obesity in adult population. Indian J Community Med. 2017;42:209–13. doi: 10.4103/ijcm.IJCM_196_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Higgins PB, Comuzzie AG. Handbook of Anthropometry. New York, NY: Springer; 2012. Measures of waist circumference; pp. 881–91. [Google Scholar]
- 11.Yan Q, Sun D, Li X, Zheng Q, Li L, Gu C, Feng B. Neck circumference is a valuable tool for identifying metabolic syndrome and obesity in Chinese elder subjects: A community-based study. Diabetes Metab Res Rev. 2014;30:69–76. doi: 10.1002/dmrr.2464. [DOI] [PubMed] [Google Scholar]
- 12.Kroll C, Mastroeni SS, Czarnobay SA, Ekwaru JP, Veugelers PJ, Mastroeni MF. The accuracy of neck circumference for assessing overweight and obesity: A systematic review and meta-analysis. Ann Hum Biol. 2017;44:667–77. doi: 10.1080/03014460.2017.1390153. [DOI] [PubMed] [Google Scholar]
- 13.Venkatrao M, Nagarathna R, Majumdar V, Patil SS, Rathi S, Nagendra H. Prevalence of obesity in India and its neurological implications: A multifactor analysis of a nationwide cross-sectional study. Ann Neurosci. 2020;27:153–61. doi: 10.1177/0972753120987465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Misra A, Chowbey P, Makkar BM, Vikram NK, Wasir JS, Chadha D, et al. Consensus statement for diagnosis of obesity, abdominal obesity and the metabolic syndrome for Asian Indians and recommendations for physical activity, medical and surgical management. J Assoc Physicians India. 2009;57:163–70. [PubMed] [Google Scholar]
- 15.Alberti KG, Zimmet P, Shaw J. Metabolic syndrome – A new world-wide definition. A consensus statement from the International Diabetes Federation. Diabet Med. 2006;23:469–80. doi: 10.1111/j.1464-5491.2006.01858.x. [DOI] [PubMed] [Google Scholar]
- 16.Moore KL, Persaud TV, Torchia MG. The Developing Human-e-book: Clinically Oriented Embryology. Elsevier Health Sciences. 2018:343. [Google Scholar]
- 17.Stabe C, Vasques AC, Lima MM, Tambascia MA, Pareja JC, Yamanaka A, Geloneze B. Neck circumference as a simple tool for identifying the metabolic syndrome and insulin resistance: Results from the Brazilian Metabolic Syndrome Study. Clin Endocrinol (Oxf) 2013;78:874–81. doi: 10.1111/j.1365-2265.2012.04487.x. [DOI] [PubMed] [Google Scholar]
- 18.Hingorjo MR, Qureshi MA, Mehdi A. Neck circumference as a useful marker of obesity: A comparison with body mass index and waist circumference. J Pak Med Assoc. 2012;62:36–40. [PubMed] [Google Scholar]
- 19.Zaciragic A, Elezovic M, Avdagic N, Babic N, Dervisevic A, Lepara O, et al. Relationship between the neck circumference, standard anthropometric measures, and blood pressure in Bosnian young adults. Eurasian J Med. 2019;51:150–3. doi: 10.5152/eurasianjmed.2018.18197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Özkaya İ, Tunçkale A. Neck circumference positively related with central obesity and overweight in Turkish university students: A preliminary study. Cent Eur J Public Health. 2016;24:91–4. doi: 10.21101/cejph.a4555. [DOI] [PubMed] [Google Scholar]
- 21.Patnaik L, Pattnaik S, Rao EV, Sahu T. Validating neck circumference and waist circumference as anthropometric measures of overweight/obesity in adolescents. Indian Pediatr. 2017;54:377–80. doi: 10.1007/s13312-017-1110-6. [DOI] [PubMed] [Google Scholar]
- 22.Aswathappa J, Garg S, Kutty K, Shankar K. Utility of neck circumference, a simple and novel measure as anthropometric marker of obesity in adults. World J Pharm Pharm Sci. 2014;3:1618–29. [Google Scholar]
- 23.Bochaliya RK, Sharma A, Saxena P, Ramchandani GD, Mathur G. To evaluate the association of neck circumference with metabolic syndrome and cardiovascular risk factors. J Assoc Physicians India. 2019;67:60–2. [PubMed] [Google Scholar]
- 24.Loh JM, Toh ST. Rethinking neck circumference in STOP-BANG for Asian OSA. Proc Singapore Healthc. 2019;28:105–9. [Google Scholar]
- 25.Raub D, Santer P, Nabel S, Platzbecker K, Munoz-Acuna R, Xu X, et al. BOSTN bundle intervention for perioperative screening and management of patients with suspected obstructive sleep apnea: A hospital registry study. Anesth Analg. 2020;130:1415–24. doi: 10.1213/ANE.0000000000004294. [DOI] [PubMed] [Google Scholar]