

To the Editor: Recent epidemiologic data are lacking for invasive cutaneous adnexal carcinoma arising from apocrine, eccrine, and sebaceous gland structures.
We analyzed data from 18 US population-based registries in the Surveillance, Epidemiology, and End Results (SEER) database of primary tumors diagnosed from 2000 to 2018 with the following International Classification of Diseases for Oncology Third Edition codes: 8200, 8390, 8400–8403, 8407–8410, 8413, 8480, 8940; consistent with a prior study.1 Incidence estimates were calculated using SEER*Stat version 8.3.9.2 SEER database information is available elsewhere.2,3 Incidence rates (IRs) were age-adjusted except in age-stratified analyses. IRs were estimated by race/ethnicity and IR ratios (IRRs) were estimated for non-Hispanic blacks versus non-Hispanic whites. Annual percent change (APC) in IRs were estimated using SEER*Stat.2 Segmented APCs (sAPCs) were estimated within time subintervals for sebaceous carcinoma using Joinpoint (Version 4.9.0.1).4 Apocrine and eccrine tumor types were combined due to small numbers in age-stratified and APC analyses. IRB approval was not required for the study (non-human subjects research).
A total of 9,646 tumors were identified (57% male; median age at diagnosis: 64 years) with an overall age-adjusted IR of 5.9 per million person-years (Table I). Crude IRs increased >200-fold with age: from 0.2 cases per million person-years in individuals <30 to 49.4 in individuals >84 years of age (eTable I). Although most tumors had higher incidences in non-Hispanic whites, mucinous adenocarcinoma incidence was over 2-fold higher in non-Hispanic blacks (IRR = 2.18, 95% CI: 1.68 to 2.78) (eTable II).
Table I.
Incidence of invasive cutaneous adnexal tumors in the SEER registry database from 2000 to 2018 in the United States (n = 9,646)
| Histologic type | ICD-O-3 Codes | No. cases (%) | Median age at diagnosis (IQR)d | % Male | % Non-Hispanic white | IR per million person-years (95% CI)e |
|---|---|---|---|---|---|---|
| Apocrine and eccrine neoplasms | ||||||
| Adenoid cystic carcinoma | 8200 | 339 (3.5) | 63 (53–75) | 45 | 73 | 0.20 (0.18–0.23) |
| Apocrine adenocarcinoma | 8401 | 260 (2.7) | 68 (53–78) | 64 | 64 | 0.16 (0.14–0.18) |
| Eccrine adenocarcinomaa | 8408, 8413 | 780 (8.1) | 51 (40–62) | 56 | 76 | 0.47 (0.44–0.51) |
| Hidradenocarcinomab | 8400,8402 | 737 (7.6) | 58 (44–69) | 54 | 70 | 0.45 (0.42–0.48) |
| Malignant mixed tumor | 8940 | 67 (0.7) | 63 (48–76) | 60 | 72 | 0.04 (0.03–0.05) |
| Microcystic adnexal carcinomac | 8407 | 813 (8.4) | 67 (55–77) | 44 | 84 | 0.49 (0.46–0.53) |
| Mucinous adenocarcinoma | 8480 | 493 (5.1) | 67 (60–77) | 43 | 59 | 0.29 (0.27–0.32) |
| Porocarcinoma | 8409 | 733 (7.6) | 73 (59–83) | 57 | 74 | 0.45 (0.42–0.48) |
| Spiradenocarcinoma | 8403 | 113 (1.2) | 66 (54–77) | 50 | 72 | 0.07 (0.06–0.08) |
| Sebaceous adenocarcinoma | 8410 | 4,144 (43.0) | 73 (62–82) | 62 | 78 | 2.52 (2.44–2.59) |
| Skin appendage carcinoma NOS | 8390 | 1,167 (12.1) | 73 (60–82) | 59 | 81 | 0.71 (0.67–0.76) |
| All combined | 9,646 | 64 (53–74) | 57 | 76 | 5.86 (5.75–5.97) |
CI, confidence interval; ICD-O-3, International Classification of Diseases for Oncology Third Edition; IR, incidence, rate; NOS, not-otherwise specified; SEER, Surveillance, Epidemiology, and End Results Program
Includes “eccrine papillary adenocarcinoma” (8408) and “eccrine adenocarcinoma” (8413).
Includes “sweat gland adenocarcinoma” (8400) and “malignant nodular hidradenoma” (8402).
Also known as “sclerosing sweat duct carcinoma”.
Age imputed as 90 for individuals with ages coded as ‘85+ years’ in SEER.
Incidence rates provided are per million person-years and age-adjusted to the 2000 US standard population (19 age groups - Census P25–1130).
Sebaceous carcinoma incidence increased by 47% between 2000–2018, while apocrine and eccrine tumor incidences did not appreciably change (Figure 1; data in eTable III). APCs were +0.5% for apocrine-eccrine carcinoma (95% CI: −0.3% to 1.3%) and +2.8% for sebaceous carcinoma (95% CI: 1.8% to 3.7%) (eTable IV). In subinterval analyses, sebaceous carcinoma IRs statistically significantly increased between 2000–2015 (sAPC +3.8%) and non-significantly decreased thereafter (eTable V).
Figure I. “Cutaneous adnexal tumor incidence trends in the United States (2000–2018)”.
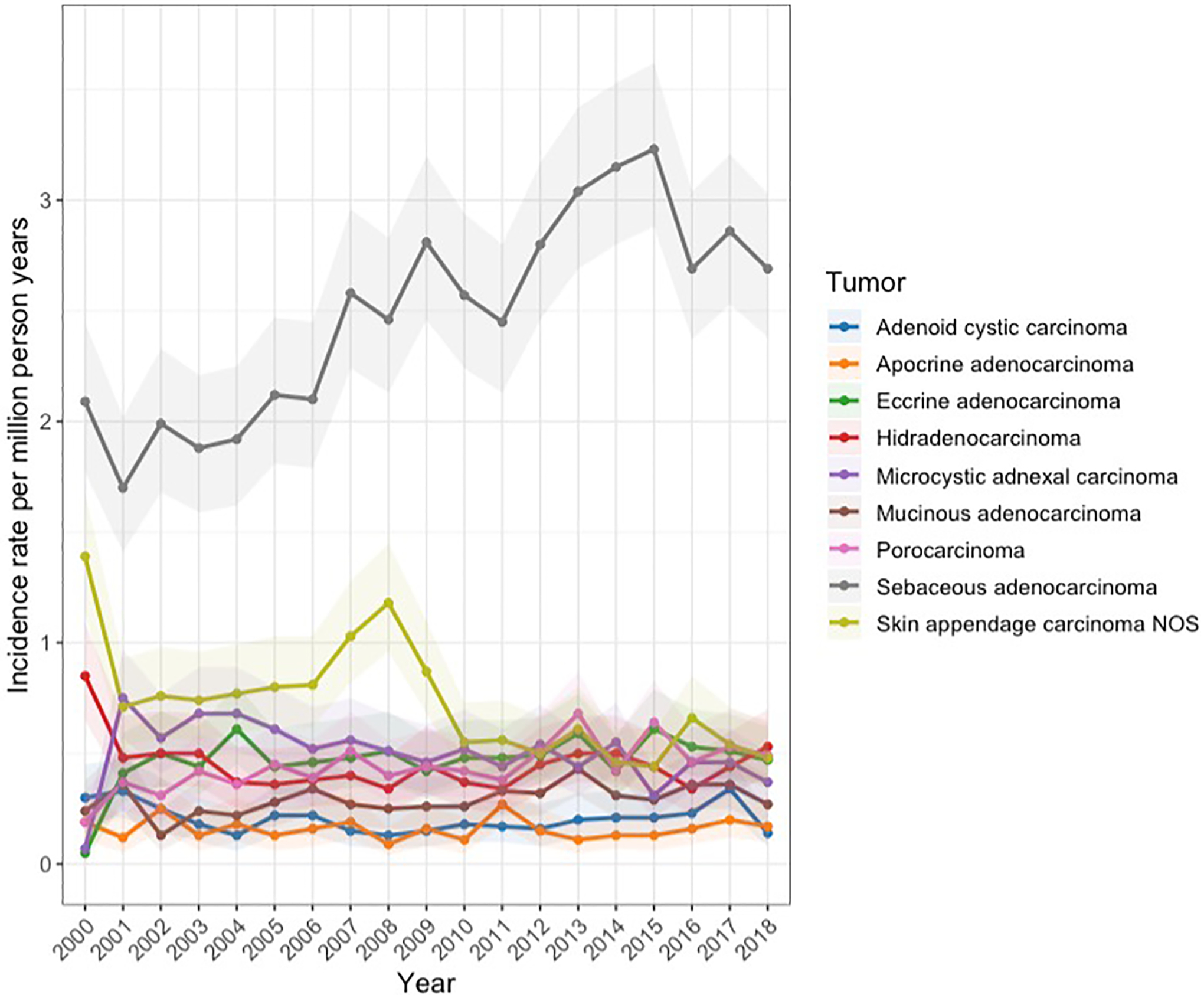
Age-standardized cutaneous adnexal tumor incidence rates per million person-years by histologic type in the Surveillance, Epidemiology, and End Results (SEER) database from 2000 to 2018; 95% confidence intervals (CIs) indicated by the shaded portions. Malignant mixed tumor and spiradenocarcinoma are excluded as their annual incidence and 95% CIs were unable to be calculated for all years due to an insufficient number of cases.
In a prior SEER analysis age-adjusted IRs increased for apocrine-eccrine carcinoma and sebaceous carcinoma by 170% and 217%, respectively, between 1987–2005.1 However, between 2000–2018, we found that only sebaceous carcinoma incidence increased, driven by increasing rates through 2015. The reasons for this are unclear but deserve further study as it may help elucidate causes of different adnexal tumors and guide future prevention efforts. While the aging population may, in part, contribute to rising sebaceous carcinoma cases, IRs were age-adjusted to control for this. “Not-otherwise-specified” tumor incidence decreased between 2000–2018, which may reflect advances in histopathologic techniques and diagnostic precision.
Study strengths include its sample size and population-based case ascertainment representative of the US population. As with other SEER studies, limitations include lack of centralized pathologic review and likely underestimation of incidence due to incomplete reporting. While the classification of tumors is standardized across SEER registries using ICDO-3 codes, validation studies of this coding system in capturing cutaneous adnexal tumors are lacking.
Given the aging US population and exponential increase in incidence of these tumors with age, dermatologists should be prepared to see more adnexal tumors, particularly sebaceous carcinoma.
Supplementary Material
Acknowledgements:
We thank Dr. Kevin Ward (Department of Epidemiology, Rollins School of Public Health, Emory University) for his input and guidance regarding the Surveillance, Epidemiology, and End Results (SEER) database.
Funding sources:
This work was supported by the National Cancer Institute (F30CA236231 to D.C.G.) and the National Institute of Arthritis and Musculoskeletal and Skin Diseases (K23AR075888 and L30AR076081 to H.Y.).
Funding Disclosure:
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Department of Veterans Affairs.
Footnotes
Conflicts of Interest: None declared.
IRB approval status: This project does not require IRB review as it does not meet the definitions of “human subjects research” (DHHS) or “clinical investigation” (FDA).
References
- 1.Blake PW, Bradford PT, Devesa SS, Toro JR. Cutaneous appendageal carcinoma incidence and survival patterns in the United States: a population-based study. Arch Dermatol. 2010;146(6):625–632. [DOI] [PubMed] [Google Scholar]
- 2.Introduction to SEER*Stat. https://seer.cancer.gov/seerstat/WebHelp/seerstat.htm. AccessedJune 16, 2021.
- 3.Tiwari RC, Clegg LX, Zou Z. Efficient interval estimation for age-adjusted cancer rates. Stat Methods Med Res. 2006;15(6):547–569. [DOI] [PubMed] [Google Scholar]
- 4.Clegg LX, Hankey BF, Tiwari R, Feuer EJ, Edwards BK. Estimating average annual per cent change in trend analysis. Stat Med. 2009;28(29):3670–3682. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.