

Abstract
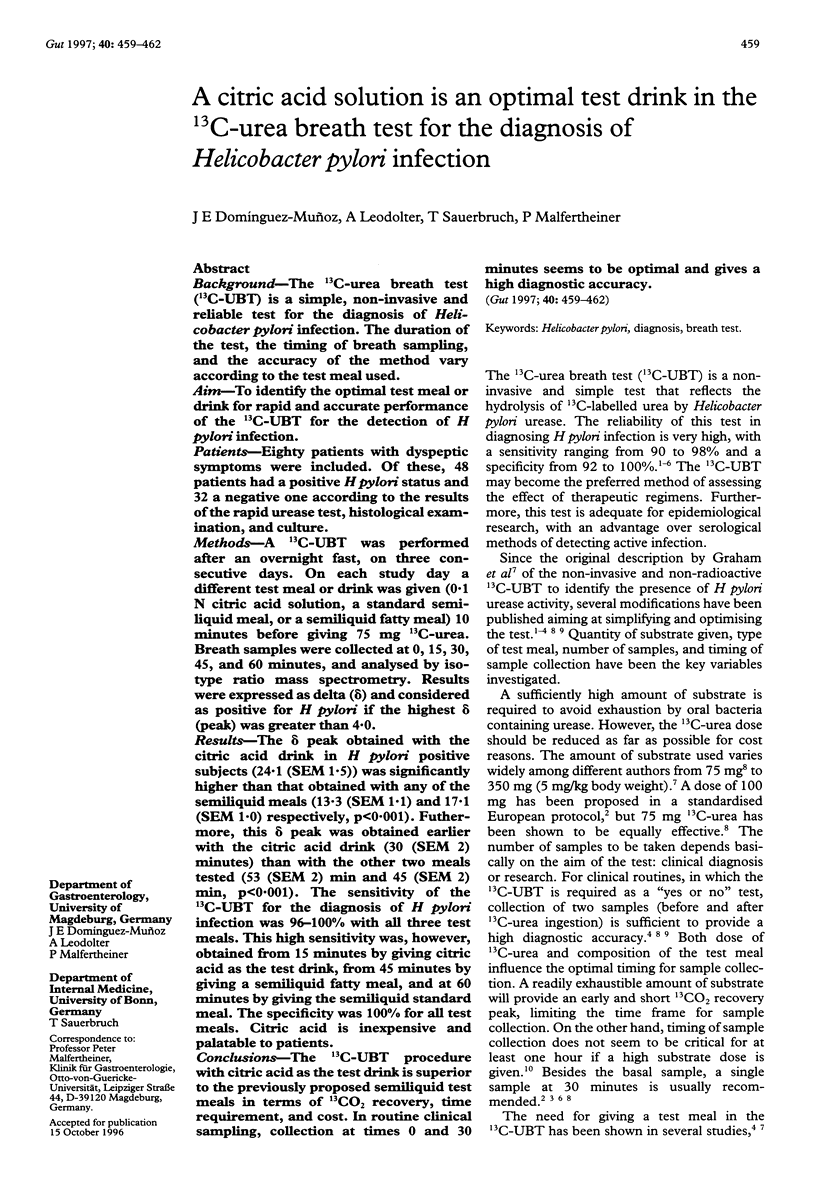
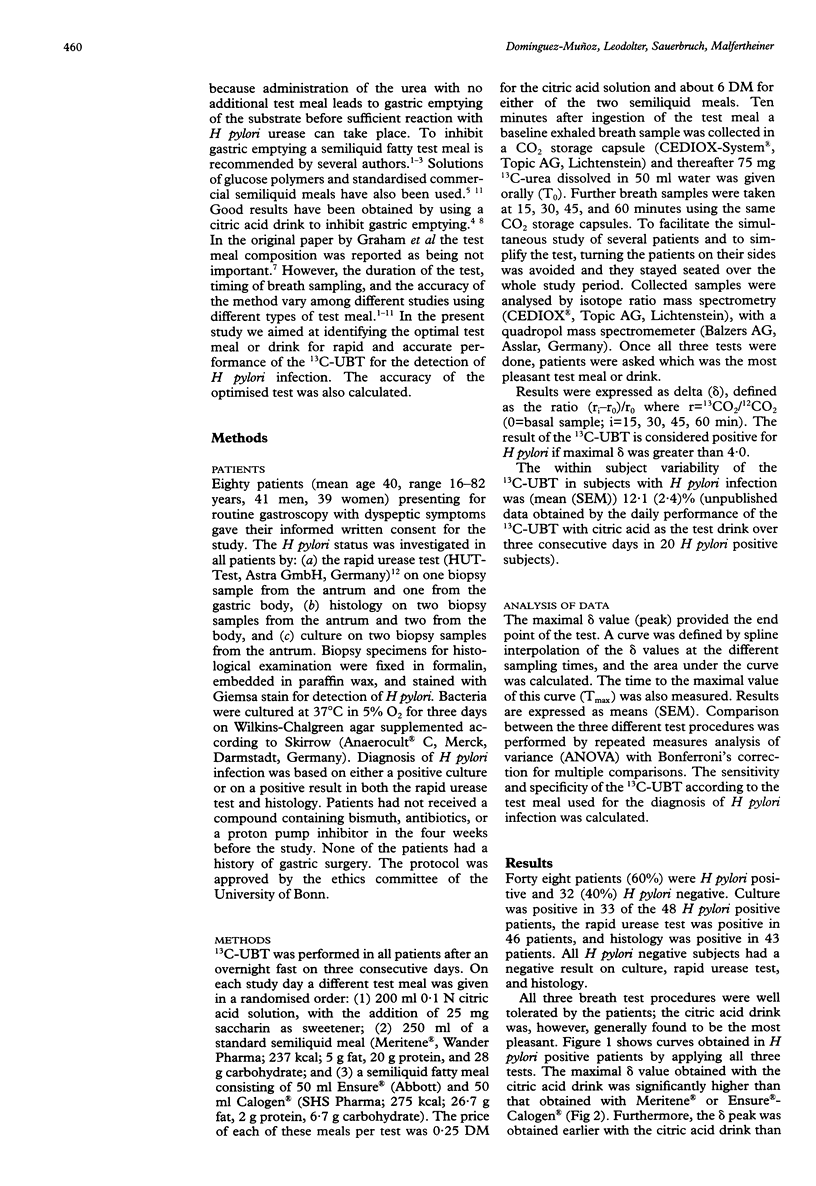
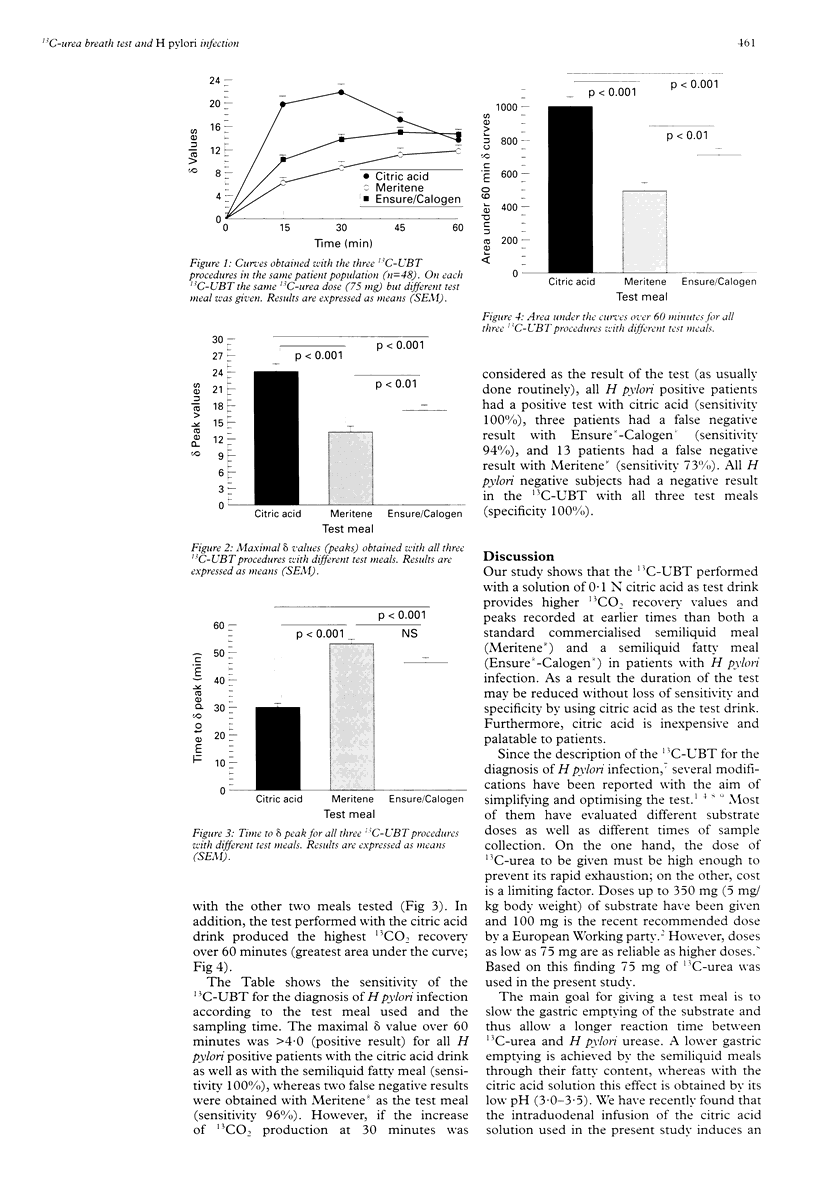
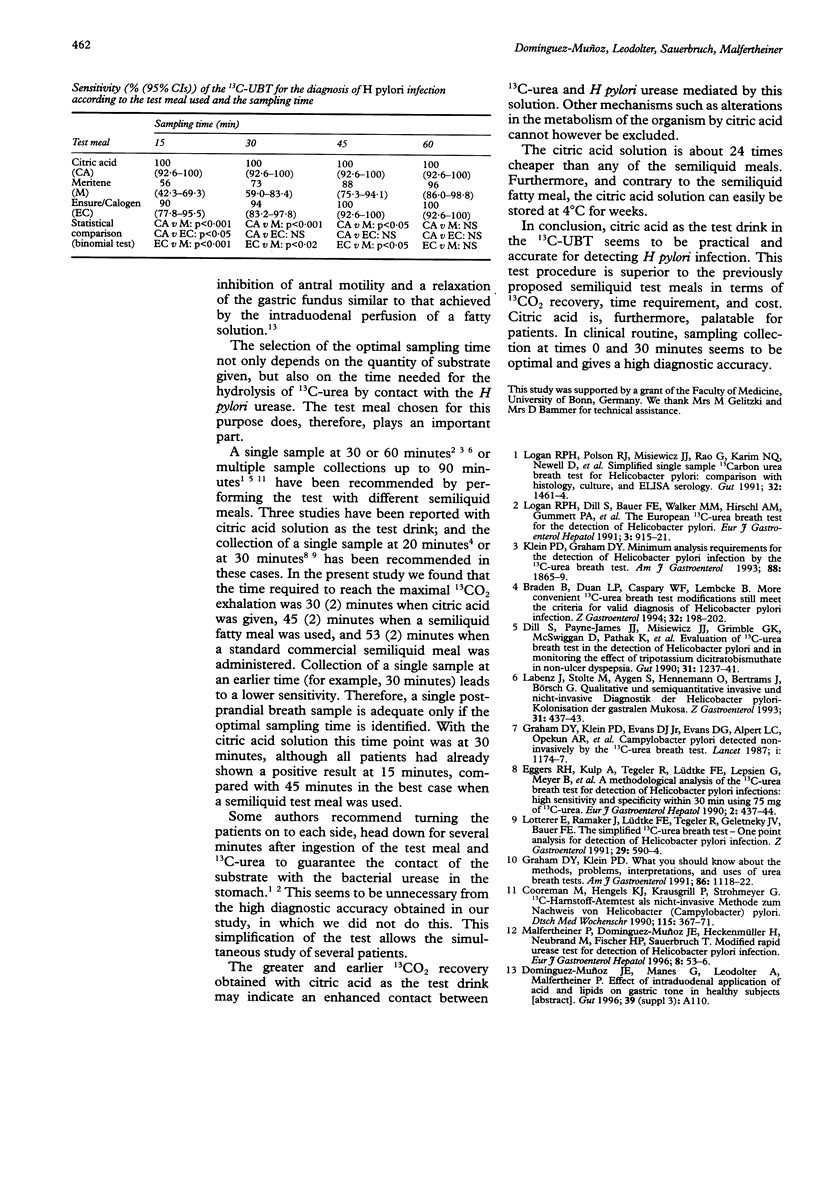
BACKGROUND: The 13C-urea breath test (13C-UBT) is a simple, non-invasive and reliable test for the diagnosis of Helicobacter pylori infection. The duration of the test, the timing of breath sampling, and the accuracy of the method vary according to the test meal used. AIM: To identify the optimal test meal or drink for rapid and accurate performance of the 13C-UBT for the detection of H pylori infection. PATIENTS: Eighty patients with dyspeptic symptoms were included. Of these, 48 patients had a positive H pylori status and 32 a negative one according to the results of the rapid urease test, histological examination, and culture. METHODS: A 13C-UBT was performed after an overnight fast, on three consecutive days. On each study day a different test meal or drink was given (0.1 N citric acid solution, a standard semiliquid meal, or a semiliquid fatty meal) 10 minutes before giving 75 mg 13C-urea. Breath samples were collected at 0, 15, 30, 45, and 60 minutes, and analysed by isotype ratio mass spectrometry. Results were expressed as delta (delta) and considered as positive for H pylori if the highest delta (peak) was greater than 4.0. RESULTS: The delta peak obtained with the citric acid drink in H pylori positive subjects (24.1 (SEM 1.5)) was significantly higher than that obtained with any of the semiliquid meals (13.3 (SEM 1.1) and 17.1 (SEM 1.0) respectively, p < 0.001). Furthermore, this delta peak was obtained earlier with the citric acid drink (30 (SEM 2) minutes) than with the other two meals tests (53 (SEM 2) min and 45 (SEM 2) min, p < 0.001). The sensitivity of the 13C-UBT for the diagnosis of H pylori infection was 96-100% with all three test meals. This high sensitivity was, however, obtained from 15 minutes by giving citric acid as the test drink, from 45 minutes by giving a semiliquid fatty meal, and at 60 minutes by giving the semiliquid standard meal. The specificity was 100% for all test meals. Citric acid is inexpensive and palatable to patients. CONCLUSIONS: The 13C-UBT procedure with citric acid as the test drink is superior to the previously proposed semiliquid test meals in terms of 13CO2 recovery, time requirement, and cost. In routine clinical sampling, collection at times 0 and 30 minutes seems to be optimal and gives a high diagnostic accuracy.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Braden B., Duan L. P., Caspary W. F., Lembcke B. More convenient 13C-urea breath test modifications still meet the criteria for valid diagnosis of Helicobacter pylori infection. Z Gastroenterol. 1994 Apr;32(4):198–202. [PubMed] [Google Scholar]
- Cooreman M., Hengels K. J., Krausgrill P., Strohmeyer G. 13C-Harnstoff-Atemtest als nicht-invasive Methode zum Nachweis von Helicobacter (Campylobacter) pylori. Dtsch Med Wochenschr. 1990 Mar 9;115(10):367–371. doi: 10.1055/s-2008-1065016. [DOI] [PubMed] [Google Scholar]
- Dill S., Payne-James J. J., Misiewicz J. J., Grimble G. K., McSwiggan D., Pathak K., Wood A. J., Scrimgeour C. M., Rennie M. J. Evaluation of 13C-urea breath test in the detection of Helicobacter pylori and in monitoring the effect of tripotassium dicitratobismuthate in non-ulcer dyspepsia. Gut. 1990 Nov;31(11):1237–1241. doi: 10.1136/gut.31.11.1237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graham D. Y., Klein P. D., Evans D. J., Jr, Evans D. G., Alpert L. C., Opekun A. R., Boutton T. W. Campylobacter pylori detected noninvasively by the 13C-urea breath test. Lancet. 1987 May 23;1(8543):1174–1177. doi: 10.1016/s0140-6736(87)92145-3. [DOI] [PubMed] [Google Scholar]
- Graham D. Y., Klein P. D., Evans D. J., Jr, Evans D. G., Alpert L. C., Opekun A. R., Boutton T. W. Campylobacter pylori detected noninvasively by the 13C-urea breath test. Lancet. 1987 May 23;1(8543):1174–1177. doi: 10.1016/s0140-6736(87)92145-3. [DOI] [PubMed] [Google Scholar]
- Klein P. D., Graham D. Y. Minimum analysis requirements for the detection of Helicobacter pylori infection by the 13C-urea breath test. Am J Gastroenterol. 1993 Nov;88(11):1865–1869. [PubMed] [Google Scholar]
- Labenz J., Stolte M., Aygen S., Hennemann O., Bertrams J., Börsch G. Qualitative und semiquantitative invasive und nicht-invasive Diagnostik der Helicobacter pylori-Kolonisation der gastralen Mukosa. Z Gastroenterol. 1993 Jul-Aug;31(7-8):437–443. [PubMed] [Google Scholar]
- Logan R. P., Polson R. J., Misiewicz J. J., Rao G., Karim N. Q., Newell D., Johnson P., Wadsworth J., Walker M. M., Baron J. H. Simplified single sample 13Carbon urea breath test for Helicobacter pylori: comparison with histology, culture, and ELISA serology. Gut. 1991 Dec;32(12):1461–1464. doi: 10.1136/gut.32.12.1461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Logan R. P., Polson R. J., Misiewicz J. J., Rao G., Karim N. Q., Newell D., Johnson P., Wadsworth J., Walker M. M., Baron J. H. Simplified single sample 13Carbon urea breath test for Helicobacter pylori: comparison with histology, culture, and ELISA serology. Gut. 1991 Dec;32(12):1461–1464. doi: 10.1136/gut.32.12.1461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lotterer E., Ramaker J., Lüdtke F. E., Tegeler R., Geletneky J. V., Bauer F. E. The simplified 13C-urea breath test--one point analysis for detection of Helicobacter pylori infection. Z Gastroenterol. 1991 Nov;29(11):590–594. [PubMed] [Google Scholar]
- Malfertheiner P., Enrique Domínguez-Muñoz J., Heckenmüller H., Neubrand M., Fischer H. P., Sauerbruch T. Modified rapid urease test for detection of Helicobacter pylori infection. Eur J Gastroenterol Hepatol. 1996 Jan;8(1):53–56. doi: 10.1097/00042737-199601000-00010. [DOI] [PubMed] [Google Scholar]