

Abstract
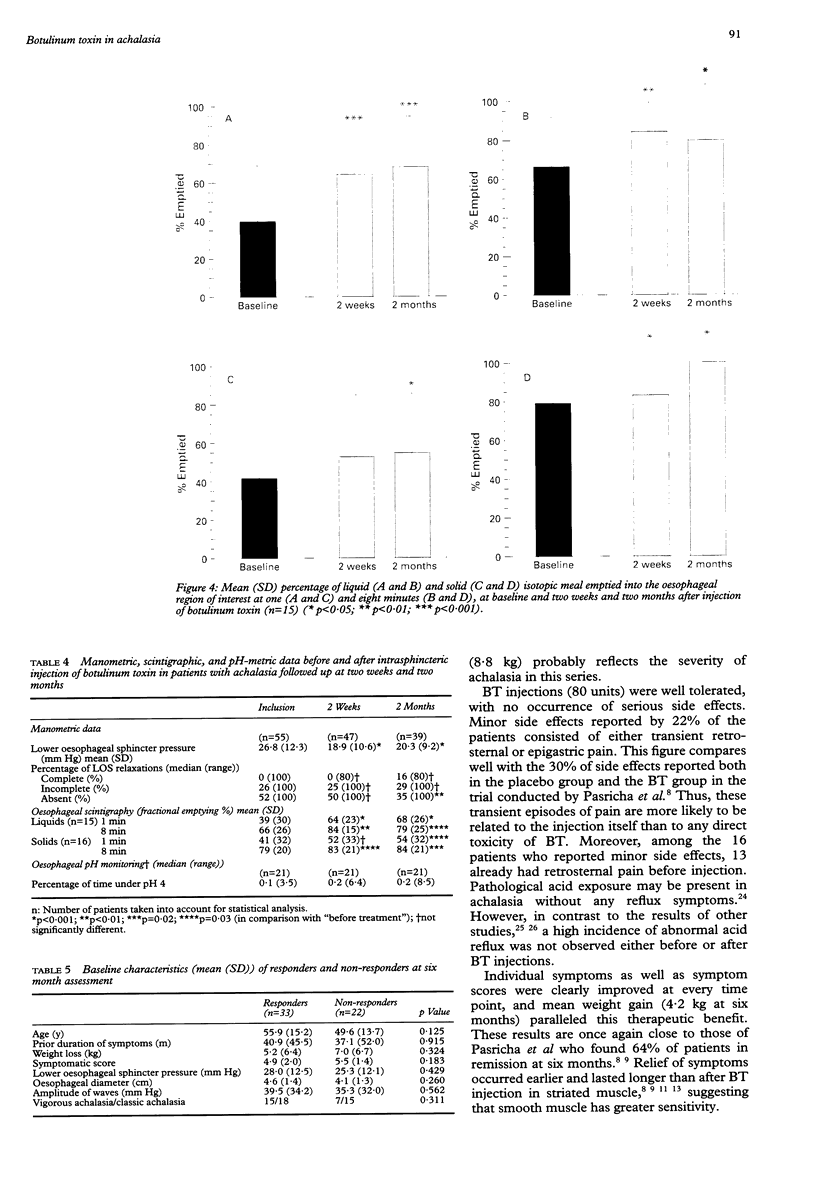
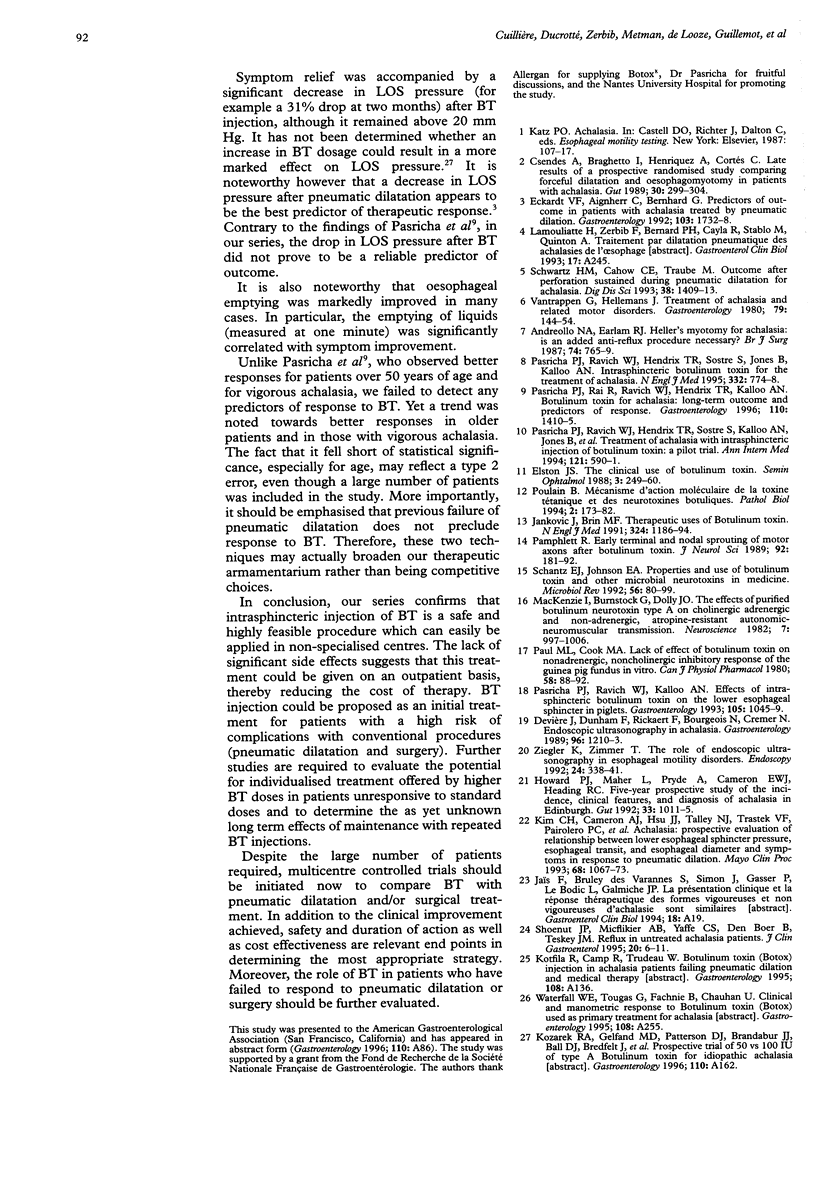
BACKGROUND: To evaluate the safety and clinical efficacy of botulinum toxin (BT) in patients with achalasia followed up for six months. METHODS: Fifty five symptomatic patients with manometrically proven achalasia were included in a multicentre prospective trial. Before and two weeks and two months after intrasphincteric injection of BT, symptoms of dysphagia, regurgitation, and chest pain were scored on a 0-3 scale, and lower oesophageal sphincter pressure (LOSP) was assessed. The symptom score was determined again at six months, clinical improvement being defined by < or = 3, relapse by > 3, and failure as a relapse after two injections or loss to follow up. RESULTS: Except for transient chest or epigastric pain (22%), no side effects were observed. There was a significant decrease in LOSP after treatment. Symptom scores were significantly improved at two weeks (2.0 (SD 1.6)), two months (1.7 (1.8)), and six months (1.9 (2.0)) compared with pretreatment values (5.1 (1.8), p < 0.001). At six months, 33 patients had clinical improvement (27 after one injection), 17 were considered failures, and five had just relapsed. Although there was a trend for age (older patients being more responsive), age, sex, prior duration of symptoms, initial symptom score, weight loss, LOSP, magnitude of oesophageal contractions, vigorous or non-vigorous achalasia, previous dilatations, and radiological features were not predictive of results. CONCLUSIONS: This multicentre series confirms that intrasphincteric injection of BT is a safe procedure, resulting in clinical improvement in 60% of patients with achalasia at six months. The therapeutic role of BT in achalasia needs further evaluation with regard to other alternatives.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Andreollo N. A., Earlam R. J. Heller's myotomy for achalasia: is an added anti-reflux procedure necessary? Br J Surg. 1987 Sep;74(9):765–769. doi: 10.1002/bjs.1800740903. [DOI] [PubMed] [Google Scholar]
- Csendes A., Braghetto I., Henríquez A., Cortés C. Late results of a prospective randomised study comparing forceful dilatation and oesophagomyotomy in patients with achalasia. Gut. 1989 Mar;30(3):299–304. doi: 10.1136/gut.30.3.299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Devière J., Dunham F., Rickaert F., Bourgeois N., Cremer M. Endoscopic ultrasonography in achalasia. Gastroenterology. 1989 Apr;96(4):1210–1213. doi: 10.1016/0016-5085(89)91644-2. [DOI] [PubMed] [Google Scholar]
- Eckardt V. F., Aignherr C., Bernhard G. Predictors of outcome in patients with achalasia treated by pneumatic dilation. Gastroenterology. 1992 Dec;103(6):1732–1738. doi: 10.1016/0016-5085(92)91428-7. [DOI] [PubMed] [Google Scholar]
- Howard P. J., Maher L., Pryde A., Cameron E. W., Heading R. C. Five year prospective study of the incidence, clinical features, and diagnosis of achalasia in Edinburgh. Gut. 1992 Aug;33(8):1011–1015. doi: 10.1136/gut.33.8.1011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim C. H., Cameron A. J., Hsu J. J., Talley N. J., Trastek V. F., Pairolero P. C., O'Connor M. K., Colwell L. J., Zinsmeister A. R. Achalasia: prospective evaluation of relationship between lower esophageal sphincter pressure, esophageal transit, and esophageal diameter and symptoms in response to pneumatic dilation. Mayo Clin Proc. 1993 Nov;68(11):1067–1073. doi: 10.1016/s0025-6196(12)60900-8. [DOI] [PubMed] [Google Scholar]
- MacKenzie I., Burnstock G., Dolly J. O. The effects of purified botulinum neurotoxin type A on cholinergic, adrenergic and non-adrenergic, atropine-resistant autonomic neuromuscular transmission. Neuroscience. 1982 Apr;7(4):997–1006. doi: 10.1016/0306-4522(82)90056-2. [DOI] [PubMed] [Google Scholar]
- Pamphlett R. Early terminal and nodal sprouting of motor axons after botulinum toxin. J Neurol Sci. 1989 Sep;92(2-3):181–192. doi: 10.1016/0022-510x(89)90135-4. [DOI] [PubMed] [Google Scholar]
- Pasricha P. J., Rai R., Ravich W. J., Hendrix T. R., Kalloo A. N. Botulinum toxin for achalasia: long-term outcome and predictors of response. Gastroenterology. 1996 May;110(5):1410–1415. doi: 10.1053/gast.1996.v110.pm8613045. [DOI] [PubMed] [Google Scholar]
- Pasricha P. J., Ravich W. J., Hendrix T. R., Sostre S., Jones B., Kalloo A. N. Intrasphincteric botulinum toxin for the treatment of achalasia. N Engl J Med. 1995 Mar 23;332(12):774–778. doi: 10.1056/NEJM199503233321203. [DOI] [PubMed] [Google Scholar]
- Pasricha P. J., Ravich W. J., Hendrix T. R., Sostre S., Jones B., Kalloo A. N. Treatment of achalasia with intrasphincteric injection of botulinum toxin. A pilot trial. Ann Intern Med. 1994 Oct 15;121(8):590–591. doi: 10.7326/0003-4819-121-8-199410150-00006. [DOI] [PubMed] [Google Scholar]
- Pasricha P. J., Ravich W. J., Kalloo A. N. Effects of intrasphincteric botulinum toxin on the lower esophageal sphincter in piglets. Gastroenterology. 1993 Oct;105(4):1045–1049. doi: 10.1016/0016-5085(93)90947-b. [DOI] [PubMed] [Google Scholar]
- Paul M. L., Cook M. A. Lack of effect of botulinum toxin on nonadrenergic, noncholinergic inhibitory responses of the guinea pig fundus in vitro. Can J Physiol Pharmacol. 1980 Jan;58(1):88–92. doi: 10.1139/y80-015. [DOI] [PubMed] [Google Scholar]
- Poulain B. Mécanisme d'action moléculaire de la toxine tétanique et des neurotoxines botuliques. Pathol Biol (Paris) 1994 Feb;42(2):173–182. [PubMed] [Google Scholar]
- Schantz E. J., Johnson E. A. Properties and use of botulinum toxin and other microbial neurotoxins in medicine. Microbiol Rev. 1992 Mar;56(1):80–99. doi: 10.1128/mr.56.1.80-99.1992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz H. M., Cahow C. E., Traube M. Outcome after perforation sustained during pneumatic dilatation for achalasia. Dig Dis Sci. 1993 Aug;38(8):1409–1413. doi: 10.1007/BF01308596. [DOI] [PubMed] [Google Scholar]
- Shoenut J. P., Micflikier A. B., Yaffe C. S., Den Boer B., Teskey J. M. Reflux in untreated achalasia patients. J Clin Gastroenterol. 1995 Jan;20(1):6–11. doi: 10.1097/00004836-199501000-00004. [DOI] [PubMed] [Google Scholar]
- Vantrappen G., Hellemans J. Treatment of achalasia and related motor disorders. Gastroenterology. 1980 Jul;79(1):144–154. [PubMed] [Google Scholar]
- Ziegler K., Zimmer T. The role of endoscopic ultrasonography in esophageal motility disorders. Endoscopy. 1992 May;24 (Suppl 1):338–341. doi: 10.1055/s-2007-1010495. [DOI] [PubMed] [Google Scholar]