

Abstract
Purpose:
Lid wiper epithliopathy (LWE) was stuided in symptomatic and asymptomatic dry eye subjects. This is the first such study to be conducted in the Indian population. LWE is a clinical condition associated with vital staining in the lower and upper eyelids on increased friction of the lid margin over to the cornea. Our aim was to study LWE in symptomatic and asymptomatic (control) dry eye subjects.
Methods:
Out of 96 subjects screened, 60 subjects were enrolled in the study and were divided into two groups, symptomatic and asymptomatic dry eye subjects, based on the Standard Patient Evaluation of Eye Dryness (SPEED) questionnaire and the Ocular Surface Disease Index (OSDI) scores. The subjects were examined to rule out clinical dry eye findings and assessed for LWE with two different dyes (fluorescein and lissamine green). Descriptive analysis was done and Chi-square test was used for statistical analysis.
Results:
A total of 60 subjects were enrolled in a study with a mean age of 21.33 ± 1.88 years, out of which the majority of LWE patients (99.8%) was seen in the symptomatic group than the asymptomatic group (73.3%); the difference was statistically significant (p = 0.00) and also clinically significant. LWE was found to be significantly higher in symptomatic dry eye subjects (99.8%) compared to asymptomatic dry eye subjects (73.3%). LWE severity was also found to be more (56.6% of grade 3) among symptomatic dry eye subjects compared to asymptomatic subjects (40% of grade 2).
Conclusion:
It is important to assess the lid wiper region (LWR) and treat LWE in routine clinical practice.
Keywords: Dry eye, lid wiper epitheliopathy, lid wiper region
Lid acts as a wiper during eye blinking.[1-3] The anatomical area of the lid wiper region (LWR) is the palpebral marginal conjunctiva of the upper and lower eyelids, which is in contact with the globe.[4] The upper lid wiper acts as a wiping mechanism for spreading tear film over the ocular surface. There is also a lid wiper in the lower lid, but its role in spreading tears is uncertain.[1-3,5] The disturbance to the lid wiper structure is considered as lid wiper epitheliopathy (LWE) and was first described by Korb et al. in 2002.[2] It is a clinical condition observed as vital staining of the upper and lower lid margin regions that are in contact with the globe. It is believed to be the result of an increase in friction among the palpebral lid, the opposing bulbar conjunctiva, the cornea, and/or the contact lens.[1] Though the exact cause of LWE is unknown, it is postulated that inadequate lubrication results in frictional damage and inflammation of the marginal conjunctiva of the LWR, leading to epitheliopathy, which is typically observed using vital dyes.[6-8] Study shows that the LWR is affected in symptomatic and asymptomatic dry eye subjects as well as contact lens wearers.[1-3] The stress or damage to the lid wiper cell is considered to be a cause for LWE.[9,10] Lid wiper may traumatize the corneal epithelium and increase the sensitivity of the cornea and could be a cause of symptoms in non-dry eye test findings.
It has been hypothesized that the irregularities in the LWR can lead to greater friction during blinks, which translates to a corresponding increase in ocular discomfort and dryness.[1-3,11]
Methods
A prospective study was conducted with two groups of subjects: symptomatic and asymptomatic. Subjects were asked to complete the Standard Patient Evaluation of Eye Dryness (SPEED) and Ocular Surface Disease Index (OSDI) questionnaires. A total of 96 subjects were screened, and 60 subjects were enrolled in this study. They were divided into two groups (symptomatic and asymptomatic), and each group had 30 subjects. The study was approved by the Institutional Ethics Committee of Sankara Eye Hospital, Bangalore, and informed consent was taken from all participants. Symptomatic and asymptomatic (control) dry eye subjects were determined based on the OSDI and SPEED questionnaires. The age of subjects included in the study was in the range of 18–40 years. Subjects under topical or any systemic medication that may alter tear film, dry eye–associated syndromes, subjects with corneal or any other ocular pathologies, clinical dry eye patients, patients with systemic diseases (arthritis, thyroid), and patients allergic to fluorescein and lissamine green were excluded based on a comprehensive eye examination of the anterior segment. After that, the questionnaires regarding SPEED[11] and OSDI[12] were administered. Selection and classification of subjects were based on dry eye symptoms (SPEED and OSDI scores) as follows:
SPEED:[2,8,11] Subjects with scores ≥10 were considered symptomatic on a scale of 0–28. Subjects with a SPEED score of 0–1 were considered asymptomatic, and scores between 2 and 9 were not included in either group.[5]
OSDI:[1,13] The OSDI consists of 12 questions, with scores ranging from 0 to 48. A score of ≥12 was considered as symptomatic dry eye and a score <12 was considered as asymptomatic. Dry eye severity was calculated using the OSDI formula. The baseline measurement of tear quality and quantity (tear breakup time [TBUT], tear meniscus height, and Schirmer’s I and II) was carried out. Subjects were examined for LWE with fluorescein and followed by lissamine green.
Fluorescein dye test:[6] Two fluorescein strips were moistened with 0.45% serum saline and applied to the lower fornix. The same procedure was repeated 1 min after the first application and 3 min after the second application. The upper eyelid was everted. The LWR in the palpebral conjunctiva was checked for fluorescein staining. A slit lamp using 16× magnification and a beam width of 5 mm and a height of 10 mm were used for visualization. The lid was everted back to its anatomical position.
Lissamine green:[6] Two lissamine green strips were used and the same procedure was followed as mentioned above. Photographs of the lid wiper area were captured by everting lids and by using a photo slit lamp with each of the diagnostic dyes. Grading was done based on the horizontal length and sagittal width.
LWE grading:[1,2,8,11] The horizontal (superior punctum to lateral canthus) staining and sagittal height of the stained LWR were examined and graded.
The horizontal staining was graded as follows: grade 0- less than 2 mm staining; grade 1- 2–4 mm staining; grade 2- 5–9 mm staining; grade 3- more than 10 mm staining.
The sagittal staining was graded as follows: grade 0- less than 25% staining of the width of wiper; grade 1- between 25% and 50% staining; grade 2- 50%–75% staining; and grade 3- 75% staining of the width of wiper.
Total horizontal and sagittal staining grades were averaged and classified as follows: grade 1 LWE- mild (mean between 0.25 and 1.0); grade 2 LWE- moderate (mean between 1.25 and 2.0); grade 3 LWE- severe (mean between 2.25 and 3.0), as shown in Fig. 1.
Figure 1.

Grading of lid wiper epitheliopathy between symptomatic and asymptomatic dry eye subjects
Statistical analysis
All the data were analyzed using the Statistical Package for Social Sciences (SPSS) software, version 21.00. Descriptive analysis was done to find the mean and standard deviation of TBUT, Tear Meniscus Height (TMH), Schirmer’s I, II, and LWE between symptomatic and asymptomatic (control) groups. A Chi-square test was performed to compare the LWE severity between symptomatic and asymptomatic dry eye subjects. A P value less than 0.05 was considered as statistically significant.
Results
Out of a total of 96 subjects who were screened, 60 were selected for the study as per the exclusion and inclusion criteria. A total of 30 symptomatic dry eye subjects and 30 asymptomatic subjects were enrolled based on the inclusion criteria. Out of the 36 subjects who were excluded, 24 subjects had TBUT ≤10 s, four subjects had Schirmer’s II ≤15 mm, three subjects were using artificial tears, and five scored between 2 and 10 in the SPEED questionnaire.[3] Accordingly, a total of 60 subjects were enrolled in this study with a mean age of 21.33 ± 1.88 years and a female-to-male ratio of 65:35.
The SPEED score was 12.97 ± 0.86 in the asymptomatic group and 1.26 ± 0.86 in the asymptomatic group. The OSDI score was 20.48 ± 9.13 in the symptomatic group and 3.63 ± 2.88 in the asymptomatic group [Fig. 2]. Higher scores were seen in both the SPEED (12.97) and OSDI (20.48) questionnaires in symptomatic subjects.
Figure 2.
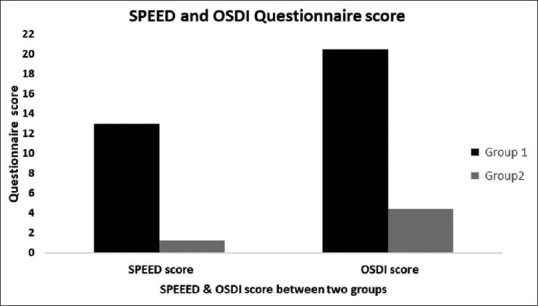
Group 1 is symptomatic and group 2 is asymptomatic (control). Higher scores were obtained in both SPEED (12.97) and OSDI (20.48) questionnaires among symptomatic subjects. OSDI = Ocular Surface Disease Index, SPEED = Standard Patient Evaluation of Eye Dryness
The clinical dry eye test findings such as TBUT, TMH, and Schirmer’s I and II were within the normal range in both symptomatic and asymptomatic groups [Table 1].
Table 1.
Mean and standard deviation of tear film evaluation
| Group 1 | Group 2 | |
|---|---|---|
| TBUT (s) | ||
| OD | 11.90±2.13 | 12.33±2.17 |
| OS | 12.56±3.25 | 12.37±2.71 |
| TMH (mm) | ||
| OD | 0.26±0.04 | 0.27±0.04 |
| OS | 0.27±0.04 | 0.27±0.047 |
| Schirmer I (mm) | ||
| OD | 33.66±2.98 | 34.40±1.63 |
| OS | 33.90±5.026 | 34.60±1.13 |
| Schirmer II (mm) | ||
| OD | 25.16±5.43 | 24.90±4.90 |
| OS | 24.90±4.90 | 27.03±6.08 |
TBUT=tear breakup time. The data represent the mean and standard deviation of tear assessment between both the groups. It shows that all the clinical dry eye test findings, that is, TBUT, TMH, and Schirmer’s I and II, in both symptomatic and asymptomatic group subjects were within the normal range. Lid wiper staining showed 3.3% of symptomatic subjects and 26.7% of asymptomatic subjects were normal with grade 0 staining
The severity of LWE was 56.6% of grade 3 in the symptomatic group and 40% of grade 2 in the symptomatic group. There was a significant difference in the severity of LWE between symptomatic and asymptomatic dry eye subjects (p = 0.00) [Table 2].
Table 2.
Grading of LWE
| Grading | Group 1 (symptomatic) | Group 2 (asymptomatic) |
|---|---|---|
| Grade 1 | 6.6% | 23.3% |
| Grade 2 | 36.6% | 40.0% |
| Grade 3 | 56.6% | 10.0% |
| Total % | 99.8% | 73.3% |
LWE=lid wiper epitheliopathy. Represents the grading of severity of LWE between the two groups. It shows the difference in severity of LWE: 56.6% of grade 3 in the symptomatic group and 40% of grade 2 in the asymptomatic group. There was a significant difference in the severity of LWE between symptomatic and asymptomatic dry eye subjects (p=0.0)
Discussion
Dry eye is mainly diagnosed based on symptoms, even in the absence of clinical findings.[10] However, Beherens et al. concluded that clinical signs and symptoms should be given primary importance in the diagnosis of dry eye disease, and additional tests were proposed to confirm and quantify the diagnosis.[1,7,14]
In the current study, LWE was seen among 99.8% of symptomatic dry eye subjects, which is higher than that reported by Korb et al.[2] on LWE and dry eye symptoms, who found a prevalence of 76% of LWE among symptomatic dry eye subjects. Our observation of 73.3% LWE in asymptomatic subjects is higher compared to that reported by Korb et al. (12%).[2] This could be because of the difference in the age group of subjects in both the studies.
The current study found 56.6% of grade 3 LWE in the symptomatic group, whereas Korb et al.[2] observed a higher occurrence of grade 1 LWE (44%). The damaged LWR could be due to many factors like blinking patterns, lid friction, lid force, and lubricating mechanism.[7]
Even among the asymptomatic group subjects, the current study found grade I (23.3%) and II (40%) LWE in young subjects, which is in variance with the results of Korb et al.,[2] where severity of grade I and II was only 8% and 4%, respectively. This could be again due to age factor and blinking patterns. Subjects might have incomplete or complete blink patterns, which could also affect the LWR. Incomplete blink is one of the risk factors for LWE.[12] Further study can be done to understand the effect of blink pattern on LWR.
Generally, in healthy eye, hydrodynamic lubrication mechanism is maintained, in which the thickness of the lubricating fluid film between the opposing tissues is adequate to separate the surfaces. However, inadequate lubrication or boundary lubrication, in which the thickness of the lubricating film in the lid ocular interface is inadequate to separate the two surfaces, results in frictional damage and inflammation of the marginal conjunctiva of the LWR, which leads to epitheliopathy. Damage of the cytoarchitecture of the LWR can be observed even in asymptomatic subjects using vital staining techniques like fluorescein staining, lissamine green, or rose bengal staining.[2,4,7,8]
Damaged LWR could be the cause of symptoms in subjects, even though the clinical findings are normal. Irregular LWR may traumatize the anterior layer of cornea, which might be the cause of patients’ discomfort.[9] Early detection of LWE in subjects of the asymptomatic group may prevent or protect them from becoming symptomatic.
The research also shows that the prevalence of LWE is six times higher in dry eye group.[13] Tear volume, tear film stability, and blink should be considered as factors determining LWE severity.[14-18]
Symptoms can vary in severity and type based on environmental factors (e.g., air conditioners, indoor and outdoor activities) and working conditions (e.g., computer usage). An incomplete blink causes inadequate lubrication at the lid wiper–ocular surface interface.[6] It may also increase the sensitivity of the cornea or lid ocular interface, resulting in dry eye symptoms. This might be one of the reasons for the higher incidence of LWE in subjects with dry eye symptoms but without positive dry eye test findings.[2,8,9] Also, there exists an association between LWE and tear film instability.[17] Blinking exercise can improve the ocular surface.[19]
Conclusion
In this study, LWE was found to be significantly more in symptomatic dry eye subjects (99.8%) than in asymptomatic dry eye subjects (73.3%).
The severity of LWE severity was more (56.6% of grade 3) among symptomatic dry eye subjects compared to symptomatic subjects (40% of grade 2). However, it has to be noted that over 70% of asymptomatic subjects also showed the presence of LWE, albeit with reduced severity. LWE can lead to discomfort and dry eye in future. Early detection of LWE can help relieve the symptoms of the subjects. So, it is important to assess the Lid wiper region (LWR) in routine clinical practice.
Consent
Consent was taken from all the subjects.
Ethics approval
Ethical approval was taken from the Institutional Review Board.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
We would like to acknowledge Dr. T. R. Raju for constant support and guidance. Director, Research, Sankara Academy of Vision, Bengaluru.
References
- 1.Yeniad B, Beginoglu M, Lale K. Lid-wiper epitheliopathy in contact lens user and patient with dry eye. Eye Contact Lens. 2010;36:140–3. doi: 10.1097/ICL.0b013e3181d94e82. [DOI] [PubMed] [Google Scholar]
- 2.Korb DR, Herman JP, Greiner JV, Scaffidi RC, Finnemore VM, Exford JM, Blackie CA, Douglass T. Lid wiper epitheliopathy and dry eye symptoms. Eye & contact lens. 2005;31:2–8. doi: 10.1097/01.icl.0000140910.03095.fa. [DOI] [PubMed] [Google Scholar]
- 3.Carlson NB, Kurtz D. 4th ed. New work: McGraw Hill; 2016. Clinical Procedure in Ocular Examination. [Google Scholar]
- 4.Knop E, Knop N, Zhivov A, Kraak R, Korb DR, Blackie C, et al. The lid wiper and muco-cutaneous junction anatomy of the human eyelid margins: An in vivo confocal and histological study. J Anat. 2011;218:449–61. doi: 10.1111/j.1469-7580.2011.01355.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Contact Lens Spectrum, Volume: 30, Issue: November 2015, page(s): 36-38, 40, 41. https://www.clspectrum.com/issues/2015/november-2015/what-is-lid-wiper-epitheliopathy.
- 6.Li W, Yeh TN, Leung T, Yuen T, Lerma M, Lin MC. The relationship of lid wiper epitheliopathy to ocular surface signs and symptoms. Invest Ophthalmol Vis Sci. 2018;59:1878–87. doi: 10.1167/iovs.17-23639. [DOI] [PubMed] [Google Scholar]
- 7.Keir N, Ngo W, Situ P, Korb D, Blackie C, Simpson T. Evaluation of the standard patient evaluation of eye dryness (SPEED) questionnaire. Investigative Ophthalmology & Visual Science. 2013;54:6028. doi: 10.1097/ICO.0b013e318294b0c0. [DOI] [PubMed] [Google Scholar]
- 8.Korb DR, Greiner JV, Herman JP, Hebert E, Finnemore VM, Exford JM, et al. Lid-wiper epitheliopathy and dry-eye symptoms in contact lens wearers. CLAO J. 2002;28:211–6. doi: 10.1097/01.ICL.0000029344.37847.5A. [DOI] [PubMed] [Google Scholar]
- 9.Elliott David B Clinical Procedure in Primary Eye Care. 3rd ed. Edinburgh London, New York: Elsevier Limited; 2007. [Google Scholar]
- 10.Korb DR, Herman JP, Finnemore VM, Exford JM, Blackie CA. An evaluation of the efficacy of fluorescein, rose bengal, lissamine green, and a new dye mixture for ocular surface staining. Eye Contact Lens. 2008;34:61–4. doi: 10.1097/ICL.0b013e31811ead93. [DOI] [PubMed] [Google Scholar]
- 11.Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. The ocular surface disease index (OSDI) reliability and validity. Arch Ophthalmol. 2000;118:615–21. doi: 10.1001/archopht.118.5.615. [DOI] [PubMed] [Google Scholar]
- 12.Suchecki JK, Donshik P, Ehlers WH. Contact lens complications. Ophthalmology Clinics of North America. 2003;16:471–84. doi: 10.1016/s0896-1549(03)00056-7. [DOI] [PubMed] [Google Scholar]
- 13.Korb DR, Herman JP, Blackie CA, Scaffidi RC, Greiner JV, Exford JM, et al. Prevalence of lid wiper epitheliopathy in subjects with dry eye signs and symptoms. Cornea. 2010;29:377–83. doi: 10.1097/ICO.0b013e3181ba0cb2. [DOI] [PubMed] [Google Scholar]
- 14.McMonnies CW. Incomplete blinking: Exposure keratopathy, lid wiper epitheliopathy, dry eye, refractive surgery, and dry contact lenses. Contact Lens Anterior Eye. 2007;30:37–51. doi: 10.1016/j.clae.2006.12.002. [DOI] [PubMed] [Google Scholar]
- 15.Behrens A, Doyle JJ, Stern L, Chuck RS, McDonnell PJ, Azar DT, et al. Dysfunctional tear syndrome: a Delphi approach to treatment recommendations. Cornea. 2006;25:900–7. doi: 10.1097/01.ico.0000214802.40313.fa. [DOI] [PubMed] [Google Scholar]
- 16.Kato H, Yokoi N, Watanabe A, Komuro A, Sonomura Y, Sotozono C, et al. Clinical factors for determining the severity of lid wiper epitheliopathy in dry eye. Cornea. 2022;41:545–51. doi: 10.1097/ICO.0000000000002879. [DOI] [PubMed] [Google Scholar]
- 17.Wang MT, Tien L, Han A, Lee JM, Kim D, Markoulli M, et al. Impact of blinking on the ocular surface and tear film parameters. Ocul Surf. 2018;16:424–9. doi: 10.1016/j.jtos.2018.06.001. [DOI] [PubMed] [Google Scholar]
- 18.Bakkar MM, Shihadeh WA, Haddad MF, Khader YS. Epidemiology of symptoms of dry eye diseases (DED) in Jordan: A cross-sectional non-clinical population-based study. Cont Lens Anterior Eye. 2016;39:197–202. doi: 10.1016/j.clae.2016.01.003. [DOI] [PubMed] [Google Scholar]
- 19.Kim AD, Muntz A, Lee J, Wang MT, Craig JP. Therapeutic benefits of blinking exercises in dry eye disease. Contact Lens Anterior Eye. 2021;44:101329. doi: 10.1016/j.clae.2020.04.014. [DOI] [PubMed] [Google Scholar]