

Abstract
Aim
The purpose of this study was to assess the level of moral courage among nurses in China, and to explore related influential factors, to help nursing managers take measures to improve nurses' moral courage.
Design
A cross‐sectional study.
Methods
The data adopted a convenient sampling method. From September to December 2021, 583 nurses from five hospitals in Fujian Province completed the Chinese version of the Nurses' Moral Courage Scale (NMCS). Data were analysed using descriptive statistics, chi‐square test, T‐test, Pearson correlation analysis and multiple regression analysis.
Results
The Chinese nurses perceived themselves, on average, as morally courageous. The mean NMCS score was 3.64 ± 0.692. The six factors showed statistically significant correlations (p < 0.05) with moral courage. Regression analysis showed that the main factors influencing nurses' moral courage were active learning of ethics knowledge and nursing was a career goal.
Conclusion
This study provides the self‐evaluation level and related influencing factors of Chinese nurses' moral courage. There is no doubt that nurses still need strong moral courage to face unknown ethical problems and challenges in the future. Nursing managers should pay attention to the cultivation of nurses' moral courage, using various forms of educational activities to help nurses alleviate moral problems and improve their moral courage, to maintain patients' access to high‐quality nursing.
Keywords: moral courage, nurses, nursing ethics, virtue ethics
1. INTRODUCTION
Moral courage is related to morality, ethics and rational understanding, which is a part of nurses' ethical competence (Gibson, 2019). However, moral courage as a concept has been debated in nursing since the era of Florence Nightingale (Heggestad et al., 2022). But in China, since the Confucius era, courage must be combined with “righteousness” to be called courageous virtue. Now, the phenomenon of moral courage loss caused by moral indifference and other factors is more and more serious. Therefore, it is of great significance for Chinese nurses to rediscover the concept of moral courage. As nurses face increasingly unpleasant and complex moral problems in nursing practice, moral courage has also received more and more attention. In particular, the COVID‐19 pandemic has intensified the moral distress caused by conflicting professional values (Turale et al., 2020). However, the research on the moral courage of nurses in China is still in its infancy, which is reflected in the lack of research on the measurement results and influencing factors of moral courage. Therefore, this study was an empirical study to better understand the moral courage level of Chinese nurses and how to support them in complex moral challenges. It is expected to provide reference for nursing managers to take targeted measures to improve nurses' moral courage in the future.
2. BACKGROUND
Moral courage was defined as the nurse's ability to rationally defend professional ethical principles and to act accordingly despite the anticipated or real adverse consequences of such action (Numminen et al., 2019). Moral courage is a highly valued element of human morality and today an acknowledged virtue in nursing care (Kleemola et al., 2020). The available evidence shows that nurses may gain many benefits from using moral courage, including effectively dealing with moral dilemmas (Savel & Munro, 2015), resisting the adverse consequences of mental pain (Safarpour et al., 2020), reducing the turnover rate of nurses (Rathert et al., 2016), thus proving patients with safe and high‐quality care (Numminen et al., 2017). If nurses lack moral courage, they will be unable to solve the difficult background factors that prevent them from following moral values (Konings et al., 2022) and undermines nurses' integrity as autonomous moral agents (Numminen et al., 2021).
Given the importance of moral courage in nurses themselves and providing high‐quality nursing, it is important to study nurses' moral courage using effective evaluation tools. Numminen et al. (2019) developed the nurse moral courage scale, which has become an effective tool by which to evaluate nurses' moral courage. The researchers used this tool to measure the moral courage of nurses in several countries, including Finland (Hauhio et al., 2021) and Belgium (Konings et al., 2022). According to the above research reports, the moral standards of nurses in these two countries are at the upper middle level. This result is consistent with that measured by the Moral Courage Scale in Iran (Khoshmehr et al., 2020). However, there are data from China in this field. In 2019, Wang et al. (2019) sinicized the Nurses' Moral Courage Scale and tested its reliability and validity. But she did not report the moral courage level of Chinese nurses in this study. In 2022, she used this scale to report that the moral courage level of Chinese nurses was above average (Wang et al., 2022). But Wang's study only included in three hospitals in one city, which limited the representativeness of the results to a certain extent.
In addition, some demographic factors affecting nurses' moral courage have also been reported, including nurses' work experience (Callwood et al., 2019), gender (Hauhio et al., 2021), present work role (Hauhio et al., 2021) and moral education (Krautscheid, 2017). China was deeply influenced by Confucianism and attaches great importance to moral courage, Confucius and Mencius have described this. Therefore, to improve the research field of moral courage in a multi‐cultural way, it is necessary to understand the moral courage of nurses in traditional Chinese culture and better deal with future moral challenges and moral dilemmas.
3. METHODS
3.1. Measurements
3.1.1. Participants' sociodemographic
Self‐designed questionnaires were used to collect data on the sociodemographics of nurses. The nurse's sociodemographic information included gender, age, highest degree, work experience, title, working unit, income, type of employment, ethics training, active acquisition of ethics knowledge, career goal and frequency of moral courage.
3.1.2. A visual analogy scale
This was a subjective evaluation. The respondents were asked to assess their overall moral courage on a visual analog scale (VAS) 0–10, in which 0 indicates never and 10 indicates always acting morally courageously.
3.1.3. The Chinese version of NMCS
The original scale has 21 items distributed across the following four dimensions (sub‐scales) of moral courage: (1) compassion and true presence (5 items), (2) moral responsibility (4 items), (3) moral integrity (7 items), and (4) commitment to good care (5 items). The Chinese version of the moral courage scale was translated and revised by Wang et al. (2019) to measure the moral courage of clinical nurses' self‐assessment. The Cronbach's alpha values of the total scale in the Chinese NMCS were 0.905. In this study, Cronbach's α was 0.957. The items are assessed according to a five‐point Likert scale (1 = does not describe me at all to 5 = describes me very well), and item scores are summed to give the scores for each dimension and the average of the total score; higher scores indicate better moral courage.
3.2. Study design and participants
This study applied a cross‐sectional survey design. The data were adopted a convenient sampling method and collected from September to December 2021 from five tertiary hospitals in Fujian Province, China. This study was approved by the relevant department of each hospital. The selected departments were (1) intensive care, including comprehensive and specialized intensive care units; (2) internal medicine; (3) surgery; (4) operating room; (5) other, including gynaecology, obstetrics and paediatrics. According to the size of the department and the willingness of nurses to participate, this approach provided a representative sample of nurses from different care contexts.
Inclusion criteria for the participants were (1) registered nurses; (2) currently employed by tertiary hospitals; (3) informed consent and voluntary participation.
According to Kendall's clinical research sample size estimation formula, the sample size is five to ten times the number of variables.14 Considering 20% invalid questionnaires, the sample size determined in this study is 420. A total of 582 questionnaires were distributed in this study, excluding those with less than 90 s response time and the options were all the same answer, resulting in 533 valid questionnaires with a valid recovery rate of 91.58%.
Because of China's COVID‐19 policy, an electronic version of the questionnaire was required (Website: https://www.wjx.cn/vj/YFAYWwz.aspx). The QR code of the questionnaire was posted by the head nurse or the nurse in charge of scientific research at each Department on the Department's WeChat group, and the nurses completed it voluntarily. The questionnaire instructions clarified the concept of moral courage, and provided information about the purpose of the study, voluntary participation and a guarantee of participant anonymity. When completing the questionnaire, nurses could ask any questions in the Wechat group, and the researchers responded directly online. The purpose was to minimize misunderstanding of the online questions.
3.3. Data analysis
The data were analysed using SPSS version 21.0 (IBM Corporation). The normal P–P diagram method was used to test whether the data obey the normal distribution. The measurement data conforming to the normal distribution were expressed as mean ± SD, and the measurement data not conforming to the normal distribution were expressed as median (M) and interquartile spacing (Q25 and Q75). Count data were statistically described by frequency, percentage or constituent ratio. T‐test and analysis of variance were used for continuous variables conforming to normal distribution and homogeneity of variance, the chi‐square test was used for counting data, and Pearson correlation analysis was used for correlation analysis of measurement data. The statistical significance level was set at p‐value <0.05.
4. RESULTS
According to the results, most of the points of the “total score” can be distributed in a straight line, and the straight‐line trend is obvious (Figure 1). It can be considered that the continuous data is subject to a normal distribution.
FIGURE 1.
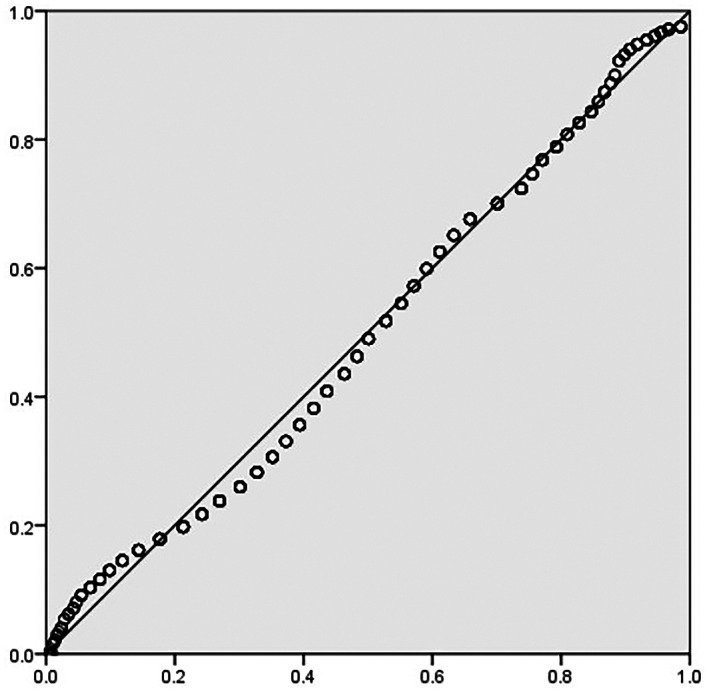
Test results of normal distribution.
4.1. Nurses' self‐assessed moral courage level
On the VAS (0–10), the mean of nurses' assessment of their overall level of moral courage was 8.29 (SD = 1.783).
The NMCS score was more than the intermediate value, at the medium‐upper level (mean = 3.64; SD = 0.692). Of the four dimensions, the scores on compassion and true presence, commitment to good care, moral integrity and moral responsibility were 3.75 ± 0.719, 3.47 ± 0.751, 3.66 ± 0.738 and 3.64 ± 0.743, respectively (Table 1).
TABLE 1.
Average score and standard deviation of four dimensions on the nurse moral courage scale
| Variables | No. of items | Score range | Mean score (mean ± SD) |
|---|---|---|---|
| NMCS | 21 | 21–105 | 3.64 ± 0.692 |
| Compassion and true presence | 5 | 5–25 | 3.75 ± 0.719 |
| Commitment to good care | 5 | 5–25 | 3.47 ± 0.751 |
| Moral integrity | 7 | 7–35 | 3.66 ± 0.738 |
| Moral responsibility | 4 | 4–20 | 3.64 ± 0.743 |
Abbreviations: NMCS, nurse moral courage scale; SD, standard deviation.
According to the results of the t‐test and analysis of variance, the factors affecting the total score of NMCS are in Table 2. The demographic factors of using VAS with nurses to assess their overall moral courage were shown in Table 3. According to the results, common influencing factors include: (1) Work experience; (2) Income; (3) Hospital organization ethics training; (4) Active acquisition of ethics knowledge; (5) Nursing was a career goal; (6) Frequency of facing situations that require moral courage at work.
TABLE 2.
The correlation between demographic factors and the total score of NMCS (N = 533)
| Variables | t/F | p |
|---|---|---|
| Gender, n (%) a | 1.296 | 0.195 |
| Age (years) b | 2.572 | 0.053 |
| Highest degree b | 0.274 | 0.844 |
| Work experience (years) b | 3.925 | 0.004* |
| Title b | 1.801 | 0.146 |
| Working unit b | 1.017 | 0.398 |
| Monthly income b | 2.566 | 0.037* |
| Is there a hospital‐authorized strength a | 2.028 | 0.043* |
| Hospital organization ethics training a | 4.615 | <0.001* |
| Active acquisition of ethics knowledge a | 5.668 | <0.001* |
| Nursing was a career goal a | 3.640 | <0.001* |
| Frequency of facing situations that require moral courage at work b | 5.674 | <0.001* |
Abbreviation: SD, standard deviation.
*p < 0.05 are statistically significant.
Independent t test.
One‐way analysis of variance.
TABLE 3.
The correlation between demographic factors and nurses' moral courage with VAS
| Variables | t/F | p |
|---|---|---|
| Gender, n (%) a | 1.081 | 0.280 |
| Age (years) b | 0.574 | 0.632 |
| Highest degree b | 0.783 | 0.504 |
| Work experience (years) b | 4.080 | 0.003* |
| Title b | 0.695 | 0.555 |
| Working unit b | 0.834 | 0.544 |
| Monthly income b | 2.471 | 0.044* |
| Is there a hospital‐authorized strength a | 2.224 | 0.823 |
| Hospital organization ethics training a | 4.026 | <0.001* |
| Active acquisition of ethics knowledge a | 4.562 | <0.001* |
| Nursing was a career goal a | 3.346 | 0.001* |
| Frequency of facing situations that require moral courage at work b | 5.129 | <0.001* |
Abbreviation: SD, standard deviation.
*p < 0.05 are statistically significant.
Independent t test.
One‐way analysis of variance.
4.2. Multiple linear regression analysis of factors influencing nurses' moral courage
Six variables (Work experience; Income; Hospital organization ethics training; Active acquisition of ethics knowledge; Nursing was career goal; Frequency of facing situations that require moral courage at work) were significantly associated with moral courage in univariate analysis. These variables were therefore entered as independent variables in multiple linear regression analysis. Collinearity diagnosis showed the tolerance of each model to be 0.6 ~ 0.9, Durbin‐Watson = 1.943, and no multicollinearity was found between independent variables. Finally, the predicted factors affecting Chinese nurses' moral courage include: (1) Active learning; and (2) Nursing was a career goal (Table 4). These two independent variables can predict 10.7% of the change in moral courage.
TABLE 4.
Variables related to nurses' moral courage (multiple linear regression analysis, N = 533)
| Variables | Total MNCS score | ||||
|---|---|---|---|---|---|
| B | Standard error | β | T | p | |
| Active learning | −6.235 | 1.414 | −0.205 | −4.410 | <0.001 |
| Nursing was career goal | −4.514 | 1.255 | −0.152 | −3.597 | <0.001 |
| R | 0.325 | ||||
| R 2 | 0.106 | ||||
| F | 8.863 | ||||
Note: p < 0.05 are statistically significant.
4.3. The correlation coefficient between the visual analogy scale and the nurse moral courage scale
The VAS scale and nurses' moral courage scale were analysed by Pearson correlation analysis. The results showed that nurses' moral courage and its four dimensions showed significant weak correlation with VAS (Table 5).
TABLE 5.
The correlation coefficient between VAS and the MNCS
| Variables VAS | Total MNCS score | Compassion and true presence | Commitment to good care | Moral integrity | Moral responsibility |
|---|---|---|---|---|---|
| r a | 0.374 | 0.371 | 0.339 | 0.345 | 0.349 |
| p | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
Note: p < 0.05 are statistically significant.
Pearson correlation coefficient: 0.2–0.4 is a weak correlation.
5. DISCUSSION
5.1. The Chinese nurses perceived themselves on average as morally courageous
According to the findings of this study, the Chinese nurses perceived themselves on average as morally courageous (mean NMCS total score = 3.64; mean VAS = 8.29). This was similar to the research results of Wang et al. (2022). Nurses are faced daily with moral dilemmas requiring acts of courage (Jiawei, 2021), so they need a high level of moral courage. The average moral courage score of Chinese nurses is lower than that of nurses in Finland and Belgium (Hauhio et al., 2021; Konings et al., 2022). The result was similar compared with studies using other moral courage scales, for example, nurses in Iran reportedly have high moral courage (Khodaveisi et al., 2021).
Among the results of the four dimensions, “commitment to good care” scored the lowest, only 3.47 ± 0.751. This dimension relates to care situations that threaten good care due to inadequate resources or poor professional competence, harmful and compromised practices or coercion (Numminen et al., 2019). This means that in these situations nurses lack the courage to defend their patients or their ultimate interests. This could be because moral courage is a form of prosocial behaviour with high social costs and no direct reward for the actor (Numminen et al., 2019). Moreover, the brave behaviour of nurses may bring a series of risks, such as being retaliated (Dinndorf‐Hogenson, 2015) and ostracized (Wiisak et al., 2022). For example, China has a shortfall of 800,000 nurses (Jiawei, 2021) and those who ask for this human resources deficit to be corrected may be ostracized by management. Therefore, from their relatively low‐level position, nurses dare not speak for patients.
The dimension with the highest score was “compassion and true presence”. This dimension focuses on the direct interpersonal relationship with patients, in which nurses can devote themselves to the core values of nursing (Konings et al., 2022). A higher score on this dimension indicates an active role in patient‐facing nursing work. These low‐ and high‐scoring dimensions may reflect risks such as interpersonal relationships affecting the extent to which nurses display moral courage, and this opportunity is worth further verification.
5.2. Factors that influence moral courage in Chinese nurses
The results of this study demonstrate that self‐perceived moral courage increases with work experience. The moral courage of nurses with more than 16 years of work experience was significantly higher than that of nurses with fewer years of work experience. However, one research results show no significant association between work experience and nurses' moral courage, which is inconsistent with the present study (Hauhio et al., 2021). Other studies have shown a significant positive correlation between work experience and nurses' moral courage (Hauhio et al., 2021; Khoshmehr et al., 2020; Konings et al., 2022; Moosavi & Izadi, 2017). Interestingly, the results of the present study show that nurses who have worked for 11–15 years have the lowest scores. This may be related to empathy since a study in China showed that nurses in this age group have the lowest empathy satisfaction and the highest empathy fatigue (Cong et al., 2022). Some nurses who have worked for a long time have not been promoted to senior professional titles, and their work enthusiasm has decreased, resulting in low empathy satisfaction, limiting nurses' empathy investment and their ability to experience the pain of patients and their families. However, the relationship between moral courage and empathy needs further verification in the future.
In addition, the results showed that both the ethical education organized by the hospital and the self‐study of ethical knowledge would affect the moral courage of nurses. This finding is consistent with most previous research results (Edmonson, 2015; Gibson, 2018; Numminen et al., 2019) and may indicate that nurses' moral courage can be improved through training and learning and provide a theoretical basis for the future development of a nurses' moral courage intervention program. However, the numbers of hospitals that organized training and nurses who took the initiative to learn were low. Another cross‐sectional study based on 218 schools in the United States found that: a slight majority of programs threaded ethics content throughout the nursing program rather than offering a standalone ethics course (Copeland, 2022). This phenomenon does not only occur in one country. In Turkey, 61% of nurses did not participate in any ethics training, 78.4% of the sample had faced an ethical dilemma in the workplace, and only 6.8% followed scientific papers on ethics (Palazoğlu & Koç, 2019). As Feeney said: knowledge we are told is power—knowledge we did not have—which meant we were often powerless (Feeney, 2013). Therefore, the value of ethical education in enhancing nurses' moral courage should not be ignored.
Nurses for whom nursing was a professional goal have higher moral courage. Nurses with positive career goals prefer to play a role in various situations (Pakizekho & Barkhordari‐Sharifabad, 2022). For example, their goal is to do good for patients, so they possess the strength to act in a morally courageous way, which they consider meaningful (Fahlberg, 2015). They may have some good moral qualities before they become nurses, but after they become nurses, these good moral qualities cannot be brought into play due to the limitations of the working environment. This can be understood as that they bravely exercising their internal morality, not out of the identity of a nurse.
The last factor is the frequency with which moral courage is required at work. The results showed that nurses who chose two extreme cases, never and very often, scored higher in moral courage. Other studies have shown that nurses who often face situations requiring moral courage at work have higher moral courage than those who face such situations less frequently (Hauhio et al., 2021; Krautscheid, 2017; Nash et al., 2016).
5.3. Different related factors of NMCS score and VAS score
According to the results of this study, the form of nurse employment will affect the NMCS score, but will not affect the VAS score. In other studies, it has also been found that different forms of employment also have an impact on nurses' moral courage (Wang et al., 2022). The reason for this inconsistency may be due to the impact of social expectations. Because moral courage is a highly appreciated human characteristic, individuals hope to show themselves in a socially or professionally acceptable way. According to the NMCS score, nurses with hospital employment have higher moral courage than those on a contract system. In China, the personnel management of employed nurses is under the jurisdiction of the local health government, while contract nurses are under the jurisdiction of the hospital. Therefore, compared with contract nurses, employed nurses have more stable jobs, and they will not be easily dismissed by the hospital, which may explain why they dare to act for patients without fear of risk.
5.4. Demographic factors that do not affect moral courage
The nurses' gender, age, highest educational background, professional title and work unit were unrelated to their self‐rated moral courage level. Other studies have also found that gender does not influence nurses' moral courage (Hensel & Laux, 2014), but Hauhio found stronger compassion and true presence in female than male nurses (Hauhio et al., 2021). The lack of significant association with gender in the present study may be explained by the small sample size of male nurses. Future research should confirm whether gender is a factor in moral courage using data from large samples.
The results of this study show no significant difference in moral courage with age, in contrast with one study which showed higher NMCS scores in older than younger nurses (Konings et al., 2022). Work experience should correlate with age, but according to the results of the present study, work experience will affect moral courage, while age will not. This deserves further discussion in the future.
Khoshmehr et al. (2020) found that nurses with higher education demonstrate moral courage, but the present study found no association between the highest degree and moral courage. This discrepancy may be due to the vast majority of respondents in the present study having graduated from college or undergraduate, but not higher level, and a lack of focus on moral courage specifically in their curricula.
In addition, a study found that the work unit was the influencing factor of moral courage, and the moral courage level of ICU and emergency department nurses was higher (Wang et al., 2022). The patients in these work units were in critical condition, and the nursing task was heavy. Nurses often need to make moral decisions involving ethical issues. According to the research results, people often have higher moral courage when they are faced with situations that require moral courage in their work. According to this logic, different work units should have different moral courage. However, there was a contradiction between this result and logic, which needs to be further verified in future research.
6. LIMITATIONS
Some limitations of this study need to be considered in future research. First, this study used an online questionnaire, and nurses could seek clarification through the WeChat network, but they could not communicate face‐to‐face, which may have introduced some information errors. Second, this study was only carried out in five hospitals in Fujian Province and not in other hospitals, so the results cannot be extended to all nurse groups. Finally, the risk of social desirability response bias should be acknowledged concerning self‐assessment instruments.
7. CONCLUSION
This study provides the self‐evaluation level and related influencing factors of Chinese nurses' moral courage. The Chinese nurses perceived themselves on average as morally courageous and related to six factors. There is no doubt that nurses still need strong moral courage to face unknown ethical problems and challenges in the future. They need to receive solid moral education to assist them in their work. This study also provides some reference value for future intervention programs to build moral courage. Nursing managers should pay attention to the cultivation of nurses' moral courage, using various forms of educational activities to help nurses alleviate moral problems and improve their moral courage from the six aforementioned factors, so as to maintain patients' access to high‐quality nursing.
AUTHOR CONTRIBUTIONS
HMT contributed to the work design, data analysis and data interpretation, drafted the article, revised important intellectual content of the article and made the final approval of the version to be submitted. DWH and ZQQ contributed to data collection and data acquisition, drafted the article and made the final approval of the version to be submitted. MN contributed to the work design and data interpretation, revised important intellectual content of the article and made the final approval of the version to be submitted.
FUNDING INFORMATION
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by a grant from the 14th 5‐year plan of Educational Science in Fujian Province (Project No. FJJKBK21‐107) and by the General Projects of Social Science Planning in Fujian Province (Project No. FJ2022B148).
CONFLICT OF INTEREST STATEMENT
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
RESEARCH ETHICS COMMITTEE APPROVAL
Ethical approval was obtained from the biomedical ethics review committee of Fujian Medical University (No. 138, 30 August 2021) and approval was ratified by the relevant departments of the hospitals. Ethical principles and scientific guidelines were followed throughout the research process.
ACKNOWLEDGEMENTS
The authors sincerely thank the administrative personnel, nurse leaders and all the nurses who participated in this study, whose contribution and interest made it possible to carry out this study. The authors are particularly grateful to Professor Chen Min, Dr. Chen Yin, the PhD student Wei Yitao from Fujian Medical University for their guidance on this study.
Huang, M. , Dong, W. , Zhao, Q. , & Mo, N. (2023). Factors associated with the moral courage of nurses in China: A cross‐sectional study. Nursing Open, 10, 4305–4312. 10.1002/nop2.1672
Contributor Information
Mingtao Huang, Email: 645767311@qq.com.
Nan Mo, Email: gmn841002@163.com.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Callwood, A. , Groothuizen, J. E. , & Allan, H. T. (2019). The "values journey" of nursing and midwifery students selected using multiple mini interviews; year two findings. Journal of Advanced Nursing, 75(5), 1074–1084. 10.1111/jan.13941 [DOI] [PubMed] [Google Scholar]
- Cong, S. N. , Zhang, A. X. , Liu, Y. , et al. (2022). Analysis of influencing factors and impact path of compassion fatigue in nurses from maternity hospitals in Jiangsu. Chinese Journal of Nursing, 57(8), 977–984. 10.3761/j.issn.0254-1769.2022.08.013 [DOI] [Google Scholar]
- Copeland, D. (2022). Liberal arts and ethics education in nursing: A national survey. Journal of Professional Nursing: Official Journal of the American Association of Colleges of Nursing, 42, 73–88. 10.1016/j.profnurs.2022.06.007 [DOI] [PubMed] [Google Scholar]
- Dinndorf‐Hogenson, G. A. (2015). Moral courage in practice: Implications for patient safety. Journal of Nursing Regulation, 6(2), 10–16. 10.1016/S2155-8256(15)30381-1 [DOI] [Google Scholar]
- Edmonson, C. (2015). Strengthening moral courage among nurse leaders. Online Journal of Issues in Nursing, 20(2), 9. 10.3912/OJIN.Vol20No02PPT01 [DOI] [PubMed] [Google Scholar]
- Fahlberg, B. (2015). Moral courage: A step beyond patient advocacy. Nursing, 45(6), 13–14. 10.1097/01.NURSE.0000464991.63854.51 [DOI] [PubMed] [Google Scholar]
- Feeney, C. (2013). Student nurse let loose on the wards. Kai Tiaki Nursing New Zealand, 19, 26–27. [PubMed] [Google Scholar]
- Gibson, E. (2018). Student courage: An essential for today's health education. Nursing Forum, 53(3), 369–375. 10.1111/nuf.12254 [DOI] [PubMed] [Google Scholar]
- Gibson, E. (2019). Longitudinal learning plan for developing moral courage. Teaching and Learning in Nursing, 14(2), 122–124. 10.1016/j.teln.2018.12.012 [DOI] [Google Scholar]
- Hauhio, N. , Leino‐Kilpi, H. , Katajisto, J. , & Numminen, O. (2021). Nurses' self‐assessed moral courage and related socio‐demographic factors. Nursing Ethics, 28, 1402–1415. 10.1177/0969733021999763 [DOI] [PubMed] [Google Scholar]
- Heggestad, A. , Konow‐Lund, A. S. , Christiansen, B. , & Nortvedt, P. (2022). A vulnerable journey towards professional empathy and moral courage. Nursing Ethics, 29(4), 927–937. 10.1177/09697330221074013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hensel, D. , & Laux, M. (2014). Longitudinal study of stress, self‐care, and professional identity among nursing students. Nurse Educator, 39, 227–231. 10.1097/NNE.0000000000000057 [DOI] [PubMed] [Google Scholar]
- Jiawei, L. (2021). The first declaration on high quality nursing development was issued in Shanghai: Clarifying the role orientation of nursing in the future. The Paper . https://www.thepaper.cn/newsDetail_forward_12575975
- Khodaveisi, M. , Oshvandi, K. , Bashirian, S. , Khazaei, S. , Gillespie, M. , Masoumi, S. Z. , & Mohammadi, F. (2021). Moral courage, moral sensitivity and safe nursing care in nurses caring of patients with COVID‐19. Nursing Open, 8(6), 3538–3546. 10.1002/nop2.903 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khoshmehr, Z. , Barkhordari‐Sharifabad, M. , Nasiriani, K. , & Fallahzadeh, H. (2020). Moral courage and psychological empowerment among nurses. BMC Nursing, 19, 43. 10.1186/s12912-020-00435-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kleemola, E. , Leino‐Kilpi, H. , & Numminen, O. (2020). Care situations demanding moral courage: Content analysis of nurses' experiences. Nursing Ethics, 27(3), 714–725. 10.1177/0969733019897780 [DOI] [PubMed] [Google Scholar]
- Konings, K. J. , Gastmans, C. , Numminen, O. H. , Claerhout, R. , Aerts, G. , Leino‐Kilpi, H. , & de Casterlé, B. D. (2022). Measuring nurses' moral courage: An explorative study. Nursing Ethics, 29(1), 114–130. 10.1177/09697330211003211 [DOI] [PubMed] [Google Scholar]
- Krautscheid, L. C. (2017). Embedding microethical dilemmas in high‐Fidelity simulation scenarios: Preparing nursing students for ethical practice. The Journal of Nursing Education, 56(1), 55–58. 10.3928/01484834-20161219-11 [DOI] [PubMed] [Google Scholar]
- Moosavi, S. , & Izadi, A. (2017). Comparison of moral courage of the nurses and nursing managers working in hospitals affiliated to Shahid Beheshti University of Medical Sciences. Medical Ethics Journal, 11(41), 17–24. http://dsp.sbmu.ac.ir/xmlui/handle/123456789/68177 [Google Scholar]
- Nash, W. , Mixer, S. J. , McArthur, P. M. , & Mendola, A. (2016). The moral courage of nursing students who complete advance directives with homeless persons. Nursing Ethics, 23(7), 743–753. 10.1177/0969733015583926 [DOI] [PubMed] [Google Scholar]
- Numminen, O. , Katajisto, J. , & Leino‐Kilpi, H. (2019). Development and validation of Nurses' moral courage scale. Nursing Ethics, 26, 2438–2455. 10.1177/0969733018791325 [DOI] [PubMed] [Google Scholar]
- Numminen, O. , Konings, K. , Claerhout, R. , Gastmans, C. , Katajisto, J. , Leino‐Kilpi, H. , & de Casterlé, B. D. (2021). Validation of the Dutch‐language version of Nurses' moral courage scale. Nursing Ethics, 28(5), 809–822. 10.1177/0969733020981754 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Numminen, O. , Repo, H. , & Leino‐Kilpi, H. (2017). Moral courage in nursing: A concept analysis. Nursing Ethics, 24(8), 878–891. 10.1177/0969733016634155 [DOI] [PubMed] [Google Scholar]
- Pakizekho, S. , & Barkhordari‐Sharifabad, M. (2022). The relationship between ethical leadership, conscientiousness, and moral courage from nurses' perspective. BMC Nursing, 21(1), 164. 10.1186/s12912-022-00941-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palazoğlu, C. A. , & Koç, Z. (2019). Ethical sensitivity, burnout, and job satisfaction in emergency nurses. Nursing Ethics, 26, 809–822. 10.1177/0969733017720846 [DOI] [PubMed] [Google Scholar]
- Rathert, C. , May, D. R. , & Chung, H. S. (2016). Nurse moral distress: A survey identifying predictors and potential interventions. International Journal of Nursing Studies, 53, 39–49. 10.1016/j.ijnurstu.2015.10.007 [DOI] [PubMed] [Google Scholar]
- Safarpour, H. , Ghazanfarabadi, M. , Varasteh, S. , Bazyar, J. , Fuladvandi, M. , & Malekyan, L. (2020). The association between moral distress and moral courage in nurses: A cross‐sectional study in Iran. Iranian Journal of Nursing and Midwifery Research, 25, 533–538. 10.4103/ijnmr.IJNMR_156_19 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Savel, R. H. , & Munro, C. L. (2015). Moral distress, moral courage. American Journal of Critical Care, 24(4), 276–278. 10.4037/ajcc2015738 [DOI] [PubMed] [Google Scholar]
- Turale, S. , Meechamnan, C. , & Kunaviktikul, W. (2020). Challenging times: Ethics, nursing and the COVID‐19 pandemic. International Nursing Review, 67(2), 164–167. 10.1111/inr.12598 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang, S. , Jiang, W. , Liu, C. , Shang, Q. , Yang, H. , Zhang, Y. , & Wei, L. (2022). The current status and influence factors of nurses' moral courage. Chinese Journal of Nursing Education, 8, 732–736. [Google Scholar]
- Wang, S. , Wei, L. , Zhang, Y. , et al. (2019). The reliability and validity of the Chinese version Nurses' moral courage scale. International Journal of Nursing Sciences, 34, 92–95. 10.3870/j.issn.1001-4152.2019.21.092 [DOI] [Google Scholar]
- Wiisak, J. , Suhonen, R. , & Leino‐Kilpi, H. (2022). Whistle‐blowers ‐ morally courageous actors in health care? Nursing Ethics, 29(6), 1415–1429. 10.1177/09697330221092341 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.