

Abstract
Background:
Migration has substantial consequences on the wellness of affected households, thereby exposing children to circumstances that are detrimental for healthy cognitive development. This study evaluates the relationship between conflict and migration during conception or early childhood and childhood cognitive development outcomes among families in Ethiopia. We hypothesized that migration is associated with worse cognitive development outcomes among children and that this association is mediated by educational disparities and caregiver psychological distress.
Methods:
The study used longitudinal data of children enrolled in the Young Lives Study (YLS) conducted in Ethiopia during 2002 (age 1), 2006–2007 (age 5), and 2009–2010 (age 8). We used multivariate linear and logistic regression to analyze the association between migration on cognitive development during middle childhood. Household migration and caregiver psychological distress were measured during round 1, type of education was measured at round 2, and cognitive development was measured at round 3.
Results:
Results of the multivariate regression analysis showed that migrant children achieved lower scores on a test of verbal intelligence after controlling for sex, ethnicity, religion, and caregiver distress (β: −8.09; 95% CI: −15.33, −0.85). Results of the mediation analysis show that the type of schooling that children attended, but not caregiver psychological distress, mediated the association between migration and cognitive development. Migrant children were more likely to attend private schools, which buffered the association between migration and lower cognitive development.
Conclusions:
This study suggests that migration is a key determinant of childhood cognitive development among migrated populations. More research is needed to build the evidence base to support interventions for this growing, underserved population.
Keywords: Cognitive development, migration, conflict, caregiver mental health
Introduction
Forced migration can have long-term consequences on the wellbeing of affected households, ultimately rendering children vulnerable to circumstances that can inhibit healthy cognitive growth. Children affected by complex emergencies are commonly exposed to risk factors for reduced cognitive development, including malnutrition and stunting (Outes-Leon, Porter, & Sanchez, 2011; Sandjaja et al., 2013), socioeconomic challenges and barriers to education (Castro & Rolleston, 2018), toxic exposures (MAL-ED Network Investigators, 2018), trauma and adverse consequences on child mental health (Myles et al., 2018), and poor caregiver mental health (Cogill, Caplan, Alexandra, Robson, & Kumar, 1986).
Despite the documented challenges and heightened risks that children in these contexts face, minimal research has been published on the effects of conflict and migration during conception or early childhood on cognitive development. The paucity of literature on the effect of migration on cognitive impairment and other developmental disabilities among children in fragile settings might be due to (a) the underdiagnosis and lack of services for these conditions in these settings, and (b) the deprioritization of treatment and service provision for developmental conditions in populations with more critical and urgent needs (Durkin, 2002).
Research on the association between migration and cognitive impairments and other developmental disabilities among children is urgently needed, given the unprecedented levels of displacement worldwide (United Nations High Commissioner for Refugees, 2020). In recent years, Ethiopia experienced the highest rate of internal displacement globally, which compounds a complex history of conflict and climate-related displacement. The Eritrean–Ethiopian War, which began in May 1998 and ended in June 2000 (Norwegian Refugee Council/Internal Displacement Monitoring Centre (NRC/IDMC), 2006), contributed substantially to global displacement. In 2000, hundreds of thousands of Ethiopian and Eritrean civilians were internally displaced or deported as a result of this war (NRC/IDMC, 2005). These massive displacement events were compounded by internal disputes that differentially affected particular ethnic and religious groups (Plaut & Gilkes, 1999). Both nations also suffered destruction of crucial infrastructure (NRC/IDMC, 2006), further exacerbating the humanitarian situation that compromises healthy child development.
The catastrophic destruction of infrastructure and the dispossession of hundreds of thousands of civilians during this war fall within a context in which deeply rooted post-colonial divides fuel the continued hostilities between and within the two nations. Presently, the fallout of these issues is intensified by climate crises and the onset of a civil war in November 2020 in the Tigray region, which has resulted in an additional one million internally displaced persons and a worsening humanitarian situation. (Simane et al., 2016). Given the protracted nature of this complex, fragile setting, an increased investment in the identification and protection of children with developmental disabilities is increasingly necessary to ensure the preservation of their, and their caretakers’, physical, mental, and emotional wellbeing.
The mechanisms through which migration affects child cognitive development are not well-characterized; however, mental health and socioeconomic impacts of migration may participate in adverse child development. One study shows that children from displaced households performed significantly worse on tests of cognitive development (Upadhyay, Srivastava, & Paul, 2018). Poor caregiver mental health is a risk factor for reduced cognitive development, and individuals experiencing conflict and crisis are at an increased risk for poor mental health (Baker-Henningham, 2013). Hence, poor caregiver mental health may mediate the association between migration and reduced child cognitive development. Likewise, there are known socioeconomic impacts of conflict and migration, including reduced access to quality education (Forced Migration Review, 2019). Evidence suggests that education quality is associated with varied rates of cognitive development (Borghans et al., 2015). Given that Ethiopia’s education infrastructure was compromised during the Eritrean–Ethiopian War, education can be considered a potential mediator of the association between migration and child cognitive development in Ethiopia.
This study aimed to evaluate the relationship between migration, caregiver mental health, education, and cognitive development among children conceived or born during or after the Ethiopian–Eritrean War. Our research questions included the following: (a) what is the relationship between migration and cognitive development outcomes among children in Ethiopia? (b) if migration and cognitive development are associated, which consequences of migration mediate that association? We hypothesized that migration would be associated with worse cognitive development outcomes among children and that this association would be mediated by education and caregiver psychological distress. We also explored whether the association between migration and cognition is moderated by schooling.
Materials and methods
Participants and procedures
The Young Lives Study (YLS) is an international longitudinal study exploring the causes and consequences of child poverty over a 15-year period in four low- and middle-income countries, including Ethiopia. Data for the current analysis were restricted to the Ethiopian sample.
Participants in the YLS in Ethiopia were selected using a multistage sampling method (Woldemedihin, 2014). Data collection occurred in 20 sentinel sites that were selected following a three-stage process beginning with purposive sampling of regions (Addis Ababa, Amhara, Oromia, SNNP, and Tigray), followed by woredas (districts) within each region and kebele (neighborhoods) within each district. Each district served as one of the sentinel sites for this country. Nearly 100 younger children and 50 older children were randomly selected from each chosen cluster. In total, 1,999 one-year-old children were selected into the younger cohort and 1,000 eight-year-old children were selected into the older cohort. Participants completed a baseline assessment (round 1) and then two additional follow-up assessments (rounds 2 and 3) at approximately three- to four-year intervals. Assessment measures included childhood welfare outcomes, including data on health, nutrition, development, and emotional wellbeing.
For the present study, we restricted our analysis to data collected from children recruited when they were 6–18 months of age who participated during rounds 1, 2, and 3 of the survey (N = 1,827; see Figure S1).
The YLS study procedures were reviewed by the six partner institutions and received approval from the Ethics Committee at the London School of Hygiene and Tropical Medicine, the University of Oxford and the College of Health, and Addis Ababa University. The YLS data are publicly available and contain no identifying information about participants.
Measures
The measures from the YLS study used in this analysis are summarized in Table 1.
Table 1.
Measures
| Construct | Role in analysis | Describes | Timepoint | Measure used |
|---|---|---|---|---|
| Migration | Exposure | Caregiver | Round 1 | Derived binary variable of migration (experienced or not) based on two items in the YLS survey; described in 2.2.1 |
| Caregiver psychological distress | Mediator | Caregiver | Round 1 | Self-Reporting Questionnaire 20 Item (SRQ20) – questionnaire that screens for psychiatric disturbance in developing countries (Beusenberg & Orley, 1994) |
| Type of schooling the child attended | Mediator | Child | Round 2 | As reported by the caregiver during the survey |
| Caregiver ethnicity | Effect measure modifier | Caregiver | Round 1 | As reported by the caregiver during the survey |
| Caregiver religion | Effect measure modifier | Caregiver | Round 1 | As reported by the caregiver during the survey |
| Cognitive development | Outcome | Child | Round 3 | PPVT – assesses receptive vocabulary ability among individuals 2 ½–90 years of age |
| Reading ability | Outcome | Child | Round 3 | Early Grade Reading Assessment (EGRA) – orally assesses skills required for literacy acquisition |
| Math ability | Outcome | Child | Round 3 | Math-measured quantitative & number notions & mathematics operations with numbers |
Exposure: migration.
The exposure of interest in our study was migration. We classified participants as migrated if the caregiver reported that they experienced a ‘big change or event that decreased the economic welfare of their household’ and (a) they described moving/migrating/or fleeing as part of that event (n = 56) or (b) they described that they fled, moved away from the problem, or migrated to look for work as a result of the big change/event in their household (n = 93). All other participants were considered to not have experienced migration (n = 1,864; see Figure S1).
Cognitive development outcomes: language, math, and reading ability.
Outcome variables of interest measured the children’s performance on three cognitive achievement tests, including the Peabody Picture Vocabulary Test-III (PPVT) (Frey, 2018), the Early Grade Reading Test (EGRA) (Dubeck & Gove, 2015), and the Math Achievement Test (Cueto & Leon, 2012). The PPVT provides an estimate of verbal receptive language by measuring receptive vocabulary in individuals 2.5–90 years of age (Beres, Kaufman, & Perelman, 2000). The test is untimed, norm-referenced, and individually and orally administered (Cueto & Leon, 2012). The EGRA measures the five fundamental reading skills required for literacy acquisition (USAID, 2016). The Math Achievement Test measured the children’s numeracy skills by measuring basic quantitative notions and basic mathematics operations with numbers.
We used data about each of these outcomes from round 3 (2009) of the YLS, when participants were 8 years old. All tests were translated into the local languages (Amharic, Oromifa, and Tigringa), and children were asked to respond to the test in the language with which they felt most comfortable. Tests were also adapted to the Ethiopian context by members of the Ethiopian research team. The PPVT was adapted by in-country experts so that it measured the same constructs with the same level of difficulty as the original version of the test (Cueto & Leon, 2012). Each of these cognitive tests were found to be reliable and valid measures of early reading skills in Ethiopia (Cueto & Leon, 2012).
Mediators: caregiver psychological distress and type of schooling.
Caregiver psychological distress was measured using the Self-Reporting Questionnaire, the SRQ20 (Netsereab et al., 2018; Scholte, Verduin, Lammeren, Rutayisire, & Kamperman, 2011; Westhuizen, Wyatt, Williams, Stein, & Sorsdahl, 2015; Young Lives, 2005). SRQ20 items are scored 0 when the symptom is absent or 1 when the symptom is present. These scores are summarized to obtain a total score, with a cut-off score of 8 indicating the existence of a probable mental disorder (Scholte et al., 2011; Tuan, Harpham, & Huong, 2004). Those who responded “yes” to eight or more questions were considered a case, and those who responded yes to seven or fewer questions were considered non-cases (Young Lives, 2005).
Type of schooling the child attended was also considered a potential mediator. In round 2, caregivers were asked “What type of school is [the child] attending?”. Responses to this question included ‘private’, ‘public’, community’, ‘government-funded’. We recoded the type of schooling to a binary variable of public (initial response of ‘public,’ ‘community,’ or ‘government funded’) or private (initial response of ‘private’).
Other variables.
Demographic characteristics that were considered in the bivariate analysis include caregiver ethnicity and caregiver religion. To determine caregiver ethnicity, we used responses to the question, “What is your ethnic group?”. Responses to that question included ‘Agew’, ‘Amhara’, ‘Gurage’, ‘Hadiya’, ‘Kambata’, ‘Oromo’, ‘Sidama’, ‘Tigrian’, ‘Wolvata’, and ‘other’. We recoded caregiver ethnicity to include the categories with frequencies of 5 or less in the ‘Other’ category, resulting in the following recoded categories: ‘Amhara’, ‘Gurage’, ‘Oromo’, ‘Tigrian’, ‘Wolvata’, and ‘Other’.
To determine caregiver religion, we used responses to the question, “What is your religion?”. Responses to that question included: ‘Muslim’, ‘Catholic’, ‘Orthodox’, ‘Evangelist’, ‘Protestant’, and ‘Other’. We recoded caregiver religion to include the categories with frequencies of 5 or less in the ‘Other’ category, resulting in the following recoded categories: ‘Muslim’, ‘Protestant’, ‘Orthodox’, and ‘Other’.
Other variables were included in the bivariate analysis due to their hypothesized relationship with cognitive development, as shown by previous studies. These variables were wealth (poor, middle, and rich) (Moriguchi & Shinohara, 2019); location of residence (urban or rural) (Hermida et al., 2019); social support (low, medium, and high) (Kang, Boss, & Clowtis, 2016); child serious illness/ injury (yes or no), chronic condition (yes or no) (Figlio, Guryan, Karbownik, & Roth, 2014); caregiver education (completed primary school or did not complete primary school) (Vilaseca et al., 2019); and stunting (not stunted, moderately stunted, or severely stunted) (Alam et al., 2020).
Statistical analysis
Bivariate analyses, using chi-square and independent two sample t-tests, were performed to compare the baseline and cognitive characteristics of the migrant and non-migrant households. Covariates that were significantly associated with migration (p < .05) or considered important potential confounders based on previous literature were included in the multivariable regression models.
A series of multivariable linear and logistic regression models were estimated to evaluate the association between migration and cognitive development and to explore potential mediators of this association. Model 1 (i.e., fully adjusted model; mediation path c) estimated the total effect of migration on cognitive development outcome(s) adjusting for covariates (Figure 1a) (Baron & Kenny, 1986). Model 2a estimated the value of mediators (type of schooling and caregiver distress) as a function of migration and covariates (mediation path a; Figure 1b). Model 2b estimated the association between cognitive development and mediators (mediation path b; Figure 1c). Model 2c added mediators to the fully adjusted model (Model 1) to estimate the direct effect of migration on cognitive development outcomes (mediation path c’; Figure 1d; Baron & Kenny, 1986). We estimated the indirect effect of migration on cognitive development outcomes via type of schooling and caregiver distress by calculating the difference between coefficients from Models 1 and 2c (Figure 1e). We reported adjusted coefficients and 95% confidence intervals. As a secondary analysis, we examined whether the association between migration and cognitive development is modified by the type of education. We included an interaction term between migration and type of schooling to Model 1 (i.e., total effect). All regression models were constructed using a complete case analysis approach, given the low levels of missing data (7.7%). Statistical computations were performed in STATA 16.0 (StataCorp, 2019).
Figure 1.
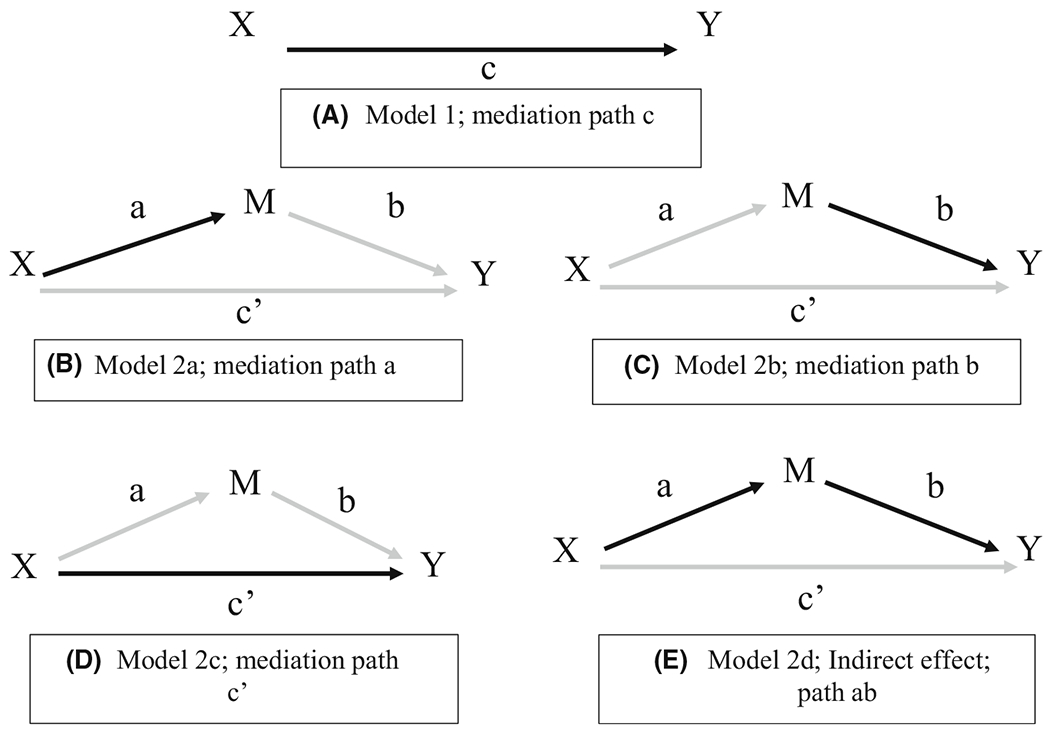
Directed acyclic graphs (DAGs) representing the causal assumptions described under section 2.3
Results
Baseline characteristics of participants stratified by migration status are listed in Table 2. Results show that 6.7% of households had migrated due to some disastrous event that occurred since the pregnancy of the index child. On average, children were 11.7 months of age at the time of the baseline interview. Caregiver depression was more common among the migrant households (40.5%) as than non-migrant households (32.6%; χ2 = 3.21, p = .073). Children attending private school was more common among migrant households (14.9%) relative to non-migrant households (10.3%); however, this did not reach statistical significance (χ2 = 2.41, p = .120).
Table 2.
Baseline characteristics of the study sample stratified by migration status (n = 1,999)
| Total sample (n = 1,819) | Not migrated (n = 1,698) | Migrated (n = 121) | t / χ2 | p | |
|---|---|---|---|---|---|
| Mean (SD) | |||||
| Age (months) | 1,819 | 11.7 (3.57) | 11.2 (3.55) | 1.7291 | .0840 |
| EGRA | 1,817 | 5.16 (3.05) | 5.0 (3.18) | 0.5445 | .5862 |
| Math | 1,750 | 6.57 (5.35) | 6.54 (5.93) | 0.0736 | .9413 |
| PPVT | 1,819 | 79.8 (44.2) | 69.7 (43.3) | 2.4255 | .0154 |
| n (%) | |||||
| Child’s gender | |||||
| Male | 954 (52.5) | 887 (52.2) | 67 (55.4) | 0.4448 | .505 |
| Female | 865 (47.6) | 811 (47.8) | 54 (44.6) | ||
| Caregiver depression | |||||
| Non-case | 1,217 (66.9) | 1,145 (67.4) | 72 (59.5) | 3.2064 | .073 |
| Case | 602 (33.1) | 553 (32.6) | 49 (40.5) | ||
| Caregiver ethnic group | |||||
| Other | 204 (11.2) | 195 (11.5) | 9 (7.4) | 25.1549 | <.0001 |
| Amhara | 512 (28.2) | 491 (28.9) | 21 (17.4) | ||
| Gurage | 150 (8.3) | 132 (7.8) | 18 (14.9) | ||
| Oromo | 384 (21.1) | 346 (20.4) | 38 (31.4) | ||
| Tigrian | 393 (21.6) | 363 (21.4) | 30 (24.8) | ||
| Wolvata | 176 (9.7) | 171 (10.1) | 5 (4.13) | ||
| Caregiver religion | |||||
| Muslim | 303 (16.7) | 274 (16.1) | 29 (23.9) | 15.994 | .001 |
| Protestant | 199 (10.94) | 195 (11.5) | 4 (3.3) | ||
| Orthodox | 1,287 (70.75) | 1,204 (70.9) | 83 (68.6) | ||
| Other | 30 (1.65) | 25 (1.47) | 5 (4.13) | ||
| Type of schooling attended (binary) | |||||
| Private | 194 (10.7) | 176 (10.3) | 18 (14.9) | 2.4123 | .120 |
| Public, Community, & Gov’t | 1,625 (89.3) | 1,522 (89.6) | 103 (85.1) |
Ethnic groups common among migrant children were Tigrian (24.8%) and Oromo (31.4%), and the groups common among those that did not undergo migration were the Amhara (28.9%), and Other (11.5%). Caregiver religion had a significant association with migration as children from Muslim households were more likely to migrate, and children from Protestant households were less likely to migrate (χ2 = 15.99, p = .001). Children in urban residences were more likely to have migrated than children in rural residences (χ2 = 2.32, p = .013) (Table S1). Wealth, gender, caregiver education, social support, and child stunting did not differ by migration history.
The PPVT was the only cognitive development outcome associated with migration in bivariate models. Figures S2a–c illustrate the mean PPVT, EGRA, and math scores obtained by migrant and non-migrant children. Figure S2a shows that migrant children scored significantly lower on the PPVT than non-migrant children (t = 2.02, p = .043). Figures S2b and c exhibit the comparability of the mean EGRA and math scores, respectively, between migrant and non- migrant households. The mean PPVT, EGRA, and math scores for migrant children were 71.5 (SD: 43.2), 5.01 (SD: 3.2), and 6.6 (SD: 5.9), while the mean scores of non-migrant children were 79.7 (SD: 44.3), 5.2 (SD: 3.1), and 6.6 (SD: 5.4), respectively.
Table 3 displays the results of the multivariate regression analyses of Models 1 and 2, which measure the strength of the association between migration prior to round 1 and cognitive development in Ethiopia during round 3.
Table 3.
Results of the regression analysis
| Fully adjusted model (total effect) | Mediation models (path a, b, and direct effect c’) | ||||
|---|---|---|---|---|---|
|
|
|||||
| Model 1 | Model 2ai | Model 2aii | Model 2b | Model 2c | |
| Outcome | PPVT | Caregiver distress | Type of schooling | PPVT | PPVT |
| Migration | −8.09 (−15.33, −0.85) | 0.35 (−.04, 0.74) | −0.67 (−1.26, −0.07) | −11.10 (−18.0, −4.20) | |
| Sex (ref = male) | −0.96 (−4.57, 2.65) | 0.10 (−0.24, 0.17) | 0.20 (−0.14, 0.54) | −0.08 (−3.50, 3.34) | −0.20 (−3.61, 3.22) |
| Caregiver ethnicity (ref = Amhara) | |||||
| Gurage | −8.28 (16.49, −0.21) | −0.46 (−0.96, 0.04) | −1.06 (−1.82, −0.30) | −12.55 (−20.98, −4.12) | −17.12 (−25.55, −8.69) |
| Oromo | −1.79 (−7.06, 3.48) | −0.23 (−0.52, 0.06) | 0.06 (−0.44, 0.56) | −2.42 (−7.41, 2.56) | −2.02 (−6.94, 2.90) |
| Tigrian | 2.39 (−2.73, 7.52) | −0.41 (−0.69, −0.12) | 0.81 (0.22, 1.41) | 3.80 (−1.07, 8.67) | 5.06 (0.25, 9.86) |
| Wolvata | 6.59 (−2.65, 12.2) | 0.004 (−0.39, 0.41) | −1.05 (−1.60 – 0.49) | 0.69 (−6.41, 7.78) | 0.07 (−6.91, 7.05) |
| Other | −8.35 (−16.49, −0.21) | −0.64 (−1.11, −0.17) | 0.36 (−0.43, 1.15) | −7.54 (−15.25, 0.17) | −6.85 (−14.44, 0.74) |
| Caregiver religion (ref = Orthodox) | |||||
| Muslim | −13.10 (−19.64, −6.56) | 0.06 (−0.31, 0.42) | 0.99 (0.31, 1.67) | −10.43 (−16.63, 8.84) | −10.15 (−16.34, −3.96) |
| Protestant | 3.81 ( −3.72,11.34) | −0.32 (−0.75, 0.11) | −0.49 (−1.07, 0.09) | 1.70 (−5.43, 8.84) | 1.48 (−5.63, 8.60) |
| Other | 24.54 (9.95, 39.12) | 0.76 (−0.006, 1.53) | −0.27 (−1.54, 1.01) | 22.39 (8.61, 36.17) | 23.70 (9.93, 37.47) |
| Public school (ref = private school) | −45.14 (−51.28, −39.01) | −45.62 (−51.76, −39.50) | |||
| Intercept | 118.06 (110.02, 126.10) | 119.14 (111.10, 127.19) | |||
Model 1: total effect of migration on cognitive development; Model 2a/ Mediation path ai: effect of migration on caregiver distress; Model 2aii/ Mediation path a: effect of migration on type of schooling; Model 2b/ Mediation path b: effect of type of schooling on PPVT; Mode 2c/ Mediation path c: indirect effect of migration of cognitive development.
Model 1: Total effect of migration on the PPVT
Results from Model 1 revealed that migrated children had lower scores on the PPVT when 8 years old (β = −8.09; 95% CI: −15.33, −0.85).
Models 2a–c: Examining caregiver distress and type of schooling as mediators of the association between migration and the PPVT
In Model 2a, we found a marginally significant association between migration and type of schooling, but no association between migration and caregiver psychological distress after controlling for sex, caregiver ethnicity, and caregiver religion was found. Results from Model 2ai show that caregiver psychological distress did not significantly differ between those who migrated and those who did not (β = 0.35; 95% CI: −0.04, 0.74) after controlling for sex, ethnicity, and religion. In Model 2aii, type of schooling the child enrolled in differed as a factor of migration (β = −0.67; 95% CI: −1.26, −0.07) after controlling for sex, caregiver ethnicity, and caregiver religion. In Model 2b, we found that private schooling was significantly associated with the PPVT after controlling for sex, caregiver ethnicity, and caregiver religion. Children who went to private school outperformed those who attended public, community, or government-funded schools on verbal language level (β = −45.14; 95% CI: −51.28, −39.01).
Results from Model 2c show a significant direct effect of migration on the PPVT, such that migrated children had lower scores on the PPVT when 8 years old relative to non-migrant children (β = −11.10; 95% CI: −18.0, −4.20).
Indirect effect
The total effect of migration on childhood cognitive development in this study was−8.09, the direct effect was −11.1, and the indirect effect was 3.01 (Figure S3). Therefore, the proportion of the association between migration and cognitive development that was mediated by the type of schooling was 37.2%.
Secondary analysis
Results of the moderation analysis revealed a significant interaction between type of schooling and migration status on PPVT scores (B = 41.51; 95% CI: 27.43, 55.60). Consistent with the findings from Model 2b, children attending public school displayed lower PPVT scores for both migrant and non-migrant children. However, the difference in the PPVT by migration status was similar in private school settings (Mean Difference in PPVT Scores = 14.03) relative to public school settings (Mean Difference in PPVT Scores = 12.32) (Figure S4).
Discussion
This study analyzed the impact of migration on the cognitive development of children in Ethiopia. Findings suggested that children who migrated had scored lower on a test of verbal cognitive ability, the PPVT, than children who did not migrate. These results, which were the first to our knowledge to show a significant association between migration and child PPVT scores, were robust and consistent across models adjusting for potential confounders, including those known to be associated with child cognitive development. However, we did not identify any differences in math or reading ability between migrant and non-migrant children.
The findings of our analysis of the PPVT are consistent with those of a previous study that explored the association between the consequences of forced migration and child cognitive wellbeing (Upadhyay et al., 2018). One explanation for the difference of test performance between children who had migrated compared to that of those who had not could be that the PPVT, a test of verbal intelligence, was administered to the children in languages in which they were not fluent. Although the PPVT was adapted to the Ethiopian context and administered to the children in three common languages in Ethiopia, those who had migrated were possibly from other regions where other languages were spoken. This may have differentially impacted the test performance among children with a primary language other than the three most common languages in Ethiopia.
The relationship between migration after conception or during early childhood and verbal cognitive ability is mediated by the type of schooling the child attended. As Table 3 illustrates, type of schooling was significantly associated with migration and reduced cognitive development at age 8. The statistical significance of the relationship between migration and cognitive wellbeing, after controlling for type of schooling as the mediator, suggests that schooling partially mediates this association (Figure S3). Hence, results of the mediation analysis show that migration has both direct and indirect effects on child verbal intelligence. The indirect effect of the observed association suggested that attending private schools buffered the association between migration and child verbal intelligence. Only the type of schooling the child attended, and not caregiver psychological distress, mediated the association between migration and cognitive development.
The moderation analysis revealed schooling to be a moderator of the association between migration and cognitive development. The disparity in scores of between public and private schooled children was observed across migration status (Figure S5), but migrant children in public schools did perform worse. These results indicate that public school educated children face unaccounted for disadvantages that may be more prevalent among migrant children.
Additionally, the association between migration and type of schooling the child attended could provide another explanation for the disparity in verbal intelligence and the discrepancy between the significance of the indicators used to assess cognitive development: PPVT, EGRA, and math. Since the type of schooling the child attended was associated with migration, we know that children who migrated received a different kind of education compared to that received by the children who had not migrated. Table 2 shows that migrant children were more likely to attend private schools, and the regression results from model 2b show that those who attended private schools outperformed those who went to public schools. Hence, some migrant children had higher verbal intelligence scores than non-migrant children. However, the results of the bivariate analysis revealed that migrant children had, on average, lower scores on the test of verbal intelligence. These results suggest that migrant children had access to better education, which may have buffered the negative associations between migration and verbal intelligence. This is consistent with other studies that support the notion that children who had access to more resources performed better on tests of verbal intelligence than children with less privilege (Stumm, Rimfeld, Dale, & Plomin, 2020).
Interestingly, we did not observe a significant association between migration and childhood stunting, which is common among migrant children (Engidaw & Gebremariam, 2019), and has been shown to lead to reduced cognitive development (Sandjaja et al., 2013). This insignificant association could also be accounted for by the explanation given above: that some migrant children had better access to resources, explaining why stunting was not associated with verbal ability in our study.
Although our study showed a robust and consistent association between migration and verbal cognitive ability, the following limitations should be considered. First, the association between migration and cognitive development could be confounded by many contextual factors that we could not consider in our analysis. Such contextual factors might include diet, environmental exposures, family size, and student motivation to perform well (Kusurkar, Ten Cate, Vos, Westers, & Croiset, 2013; MAL-ED Network Investigators, 2018). It may be that those unknown or improperly measured variables could have driven migration, thereby rendering migration a mediator of some other associations.
Additionally, the only metric of caregiver psychological distress that was provided in the YLS data was caregiver depression, which is an outcome determined by the SRQ20. While this has been validated as a measure of psychiatric disturbances in Ethiopia (Hanlon et al., 2008), the YLS does not provide a more detailed panel of psychiatric disorders that could have been a consequence of migration and a cause of the reduced cognitive verbal capacities of migrant children. Therefore, the narrow scope of the psychiatric assessment of caregivers could be a reason that we did not observe an association between caregiver mental health and cognitive wellbeing of migrant children. Additionally, it is unclear in the YLS data and other literature what constitutes community education in Ethiopia, but it was assumed that it is a type of public schooling and classified as such. Also, children’s mother tongue was not reported in YLS data; however, this information may have played a key role in understanding why there was no association between migration and cognitive outcomes other than the PPVT.
It is also possible that the mediation approach we used may be underpowered to detect significant indirect effects. Longitudinal studies with large samples of migrant youth are limited. However, future research examining these associations in a larger sample and using methods with greater statistical power could improve the estimation the relationships described in this article (MacKinnon, Lockwood, Hoffman, West, & Sheets, 2002). Finally, given that 7.7% of all observations are missing, conducting a complete case analysis as the missingness is low is enough to avoid introducing substantial emigrative selection bias. However, not addressing missingness in the mediation analysis may have exposed the study to the said bias.
Conclusion
Migration is known to stunt the physical and mental development of affected children. However, little research previously focused on the impact of migration on childhood cognitive development specifically, leaving out an important factor in the pursuit of the identification and service provision for children with developmental disabilities living in fragile settings.
We observed differences in cognitive development and in educational access and outcomes among children in Ethiopia by their migration status. Although these disparities were inconsistent across tests, they persisted seven years after migration. Our unexpected findings highlight that more research is needed to discern the relationship between migration and child cognitive development, and future studies should consider the measurement limitations we experienced in our study. Research on childhood cognitive wellbeing is especially pertinent when presuming the lasting implications of migration, particularly among individuals with disabilities.
Supplementary Material
Figure S1. Study population flow chart.
Figure S2. Mean scores on cognitive tests compared between children from displaced and non- displaced households.
Figure S3. Associations between displacement and cognitive development.
Figure S4. Comparison of mean PPVT scores of public and private school students.
Figure S5. Comparison of mean PPVT scores of migrant and non-migrant children by schooling type.
Table S1. Additional baseline characteristics of the study sample stratified by displacement status (n = 1,999).
Key points.
Migrant children experience challenging circumstances that can prohibit healthy cognitive growth.
Migration during conception or early childhood is associated with worse cognitive development outcomes.
Migrant children who attended private schools were more likely to have better cognitive development outcomes.
Caregiver psychological distress did not mediate the association between migration and childhood development outcomes.
Discerning the implications of migration on childhood development is needed to address the needs of children with developmental disabilities in conflict-affected settings.
Acknowledgements
The authors have declared that they have no competing or potential conflicts of interest.
Footnotes
Supporting information
Additional supporting information may be found online in the Supporting Information section at the end of the article:
Conflict of interest statement: No conflicts declared.
References
- Alam MA, Richard SA, Fahim SM, Mahfuz M, Nahar B, Das S, … & Ahmed T (2020). Impact of early-onset persistent stunting on cognitive development at 5 years of age: Results from a multi-country cohort study. PLoS One, 15, e0227839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baker-Henningham H (2013). The role of early childhood education programmes in the promotion of child and adolescent mental health in low- and middle-income countries. International Journal of Epidemiology, 43, 407–433. [DOI] [PubMed] [Google Scholar]
- Baron RM, & Kenny DA (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173–1182. 10.1037/0022-3514.51.6.1173 [DOI] [PubMed] [Google Scholar]
- Beres KA, Kaufman AS, & Perelman MD (2000). Chapter 4 – Assessment of child intelligence. In Goldstein G & Hersen M (Eds.), Handbook of psychological assessment (3rd edn, pp. 65–96). Oxford, UK: Elsevier Science. [Google Scholar]
- Beusenberg M, & Orley J (1994). A user’s guide to the Self Reporting Questionnaire (SRQ). World Health Organization. Available from: https://apps.who.int/iris/bitstream/handle/10665/61113/WHO_MNH_PSF_94.8.pdf?sequence=1 [last accessed 31 December 2020]. [Google Scholar]
- Borghans L, Golsteyn BH, & Zölitz U (2015). School quality and the development of cognitive skills between age four and six. PloS one, 10(7), e0129700. 10.1371/journal.pone.0129700 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Castro JF, & Rolleston C (2018). The contribution of early childhood and schools to cognitive gaps: New evidence from Peru. Economics of Education Review, 64, 144–164. [Google Scholar]
- Cogill SR, Caplan HL, Alexandra H, Robson KM, & Kumar R (1986). Impact of maternal postnatal depression on cognitive development of young children. BMJ, 292, 1165–1167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cueto S, & Leon J (2012). Psychometric characteristics of cognitive development and achievement instruments in Round 3 of Young Lives (Young Lives Technical Note No. 25). Young Lives. Available from: https://www.younglives.org.uk/sites/www.younglives.org.uk/files/YL-TN25_Cueto.pdf [Google Scholar]
- Dubeck MM, & Gove A (2015). The early grade reading assessment (EGRA): Its theoretical foundation, purpose, and limitations. International Journal of Educational Development, 40, 315–322. [Google Scholar]
- Durkin M (2002). The epidemiology of developmental disabilities in low-income countries. Mental Retardation and Developmental Disabilities Research Reviews, 8, 206–211. [DOI] [PubMed] [Google Scholar]
- Engidaw MT, & Gebremariam AD (2019). Prevalence and associated factors of stunting and thinness among adolescent Somalian Refugee girls living in Eastern Somali refugee camps, Somali regional state, Southeast Ethiopia. Conflict and Health, 13, 13–17. 10.1186/s13031-019-0203-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Figlio D, Guryan J, Karbownik K, & Roth J (2014). The effects of poor neonatal health on children’s cognitive development. American Economic Review, 104, 3921–3955. [DOI] [PubMed] [Google Scholar]
- Frey B (2018). The SAGE encyclopedia of educational research, measurement, and evaluation (Vol. 1–4). Thousand Oaks, CA: SAGE Publications Inc. [Google Scholar]
- Hanlon C, Medhin G, Alem A, Araya M, Abdulahi A, Hughes M, … & Prince M (2008). Detecting perinatal common mental disorders in Ethiopia: Validation of the self-reporting questionnaire and Edinburgh postnatal depression scale. Journal of Affective Disorders, 108, 251–262. [DOI] [PubMed] [Google Scholar]
- Hermida MJ, Shalom DE, Segretin MS, Goldin AP, Abril MC, Lipina SJ, & Sigman M (2019). Risks for child cognitive development in rural contexts. Frontiers in Psychology, 9, 2735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kang D-H, Boss L, & Clowtis L (2016). Social support and cognition: Early childhood versus older adulthood. Western Journal of Nursing Research, 38, 1639–1659. [DOI] [PubMed] [Google Scholar]
- Kusurkar RA, Ten Cate TJ, Vos CM, Westers P, & Croiset G (2013). How motivation affects academic performance: A structural equation modelling analysis. Advances in Health Sciences Education: Theory and Practice, 18, 57–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, Hoffman JM, West SG, & Sheets V (2002). A comparison of methods to test mediation and other intervening variable effects. Psychological Methods, 7, 83–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MAL-ED Network Investigators. (2018). Early childhood cognitive development is affected by interactions among illness, diet, enteropathogens and the home environment: Findings from the MAL-ED birth cohort study. BMJ Global Health, 3, 1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moriguchi Y, & Shinohara I (2019). Socioeconomic disparity in prefrontal development during early childhood. Scientific Reports, 9(1). 10.1038/s41598-019-39255-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Myles P, Swenshon S, Haase K, Szeles T, Jung C, Jacobi F, & Rath B (2018). A comparative analysis of psychological trauma experienced by children and young adults in two scenarios: Evacuation after a natural disaster vs forced migration to ESCAPE armed conflict. Public Health, 158, 163–175. [DOI] [PubMed] [Google Scholar]
- Netsereab TB, Kifle MM, Tesfagiorgis RB, Habteab SG, Weldeabzgi YK, & Tesfamariam OZ (2018). Validation of the WHO self-reporting questionnaire-20 (SRQ-20) item in primary health care settings in Eritrea. International Journal of Mental Health Systems, 12, 1–9. 10.1186/s13033-018-0242-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Norwegian Refugee Council/Internal Displacement Monitoring Centre (NRC/IDMC). (2005). Map of regional distribution of IDPs in Ethiopia. Available from: https://www.refworld.org/docid/4821c912d.html [last accessed 24 February 2021].
- Norwegian Refugee Council/Internal Displacement Monitoring Centre (NRC/IDMC). (2006). Ethiopia: Government recognition of conflict IDPs crucial to addressing their plight. A profile of the internal displacement situation. Available from: https://www.refworld.org/docid/4455beb64.html [last accessed 24 February 2021].
- Outes-Leon I, Porter C, & Sanchez A (2011). Early nutrition and cognition in Peru. SSRN Electronic Journal. 10.2139/ssrn.1972106 [DOI] [Google Scholar]
- Plaut M, & Gilkes P (1999, March 31). Conflict in the horn: Why Eritrea and Ethiopia are at war – Eritrea. Available from: https://reliefweb.int/report/eritrea/conflict-horn-why-eritrea-and-ethiopia-are-war [last accessed 24 February 2021]. [Google Scholar]
- Sandjaja, Poh BK, Rojroonwasinkul N, Le Nyugen BK, Budiman B, Ng LO, … & Parikh P (2013). Relationship between anthropometric indicators and cognitive performance in Southeast Asian school-aged children. British Journal of Nutrition, 110, S57–S64. [DOI] [PubMed] [Google Scholar]
- Scholte WF, Verduin F, Lammeren AV, Rutayisire T, & Kamperman AM (2011). Psychometric properties and longitudinal validation of the self-reporting questionnaire (SRQ-20) in a Rwandan community setting: A validation study. BMC Medical Research Methodology, 11, 1–10. 10.1186/1471-2288-11-116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simane B, Beyene H, Deressa W, Kumie A, Berhane K, & Samet J (2016). Review of climate change and health in Ethiopia: Status and gap analysis. The Ethiopian Journal of Health Development, 30, 28–41. [PMC free article] [PubMed] [Google Scholar]
- StataCorp. (2019). Stata statistical software: Release 16. College Station, TX: StataCorp LLC. [Google Scholar]
- Stumm S, Rimfeld K, Dale PS, & Plomin R (2020). Preschool verbal and nonverbal ability mediate the association between socioeconomic status and school performance. Child Development, 91, 705–714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tuan T, Harpham T, & Huong NT (2004). Validity and Reliability of the Self-reporting Questionnaire 20 Items in Vietnam. Hong Kong Journal of Psychiatry, 14, 15–18. [Google Scholar]
- United Nations High Commissioner for Refugees. (2020, December). Refugee statistics. Available from: https://www.unhcr.org/refugee-statistics/ [last accessed 19 March 2021].
- University of Oxford, Refugee Studies Center. (2019). Education: Needs, rights, and access in displacement. Forced Migration Review, 60. [Google Scholar]
- Upadhyay A, Srivastava S, & Paul C (2018). Consequences of forced migration during early childhood on cognitive wellbeing in later childhood in Andhra Pradesh, India. International Journal of Population Studies, 3, 16. [Google Scholar]
- USAID. (2016). Early Grade Reading Assessment (EGRA) toolkit. Available from: https://pdf.usaid.gov/pdf_docs/PA00M4TN.pdf [last accessed 25 October 2020].
- Vilaseca R, Rivero M, Bersabé RM, Cantero MJ, Navarro-Pardo E, Valls-Vidal C, & Ferrer F (2019). Demographic and parental factors associated with developmental outcomes in children with intellectual disabilities. Frontiers in Psychology, 10, 872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Westhuizen CV, Wyatt G, Williams JK, Stein DJ, & Sorsdahl K (2015). Validation of the Self Reporting Questionnaire 20-Item (SRQ-20) for use in a low- and middle-income country emergency centre setting. International Journal of Mental Health and Addiction, 14, 37–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woldemedihin L (2014). Young Lives survey design and sampling in Ethiopia. Young Lives. Available from: https://www.younglives.org.uk/sites/www.younglives.org.uk/files/ETH-SurveyDesign-Factsheet.pdf
- Young Lives. (2005). Caregiver depression. In Young lives: An International Study of Childhood Poverty: Round 1, 2002 – Data Dictionary (p. 136). [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1. Study population flow chart.
Figure S2. Mean scores on cognitive tests compared between children from displaced and non- displaced households.
Figure S3. Associations between displacement and cognitive development.
Figure S4. Comparison of mean PPVT scores of public and private school students.
Figure S5. Comparison of mean PPVT scores of migrant and non-migrant children by schooling type.
Table S1. Additional baseline characteristics of the study sample stratified by displacement status (n = 1,999).