

Abstract
Objective
The nutrition transition model provides an integrated approach to analyse global changes in food consumption and lifestyle patterns. Whether variability in food availability for consumption, lifestyle and sociodemographic factors is associated with the worldwide prevalence distribution of overweight, obesity and hypertension is unclear.
Design
Ecological analysis.
Setting
Country-specific prevalence estimates of overweight, obesity and hypertension were obtained. Prevalence estimates were then matched to year- and country-specific food and energy availability for consumption of cereals, sugar, sweeteners and honey, vegetable oils, fruits, starchy roots, pulses, total vegetables, alcoholic beverages, total meat, animal fat, eggs, milk, and fish and seafood. The per capita Gross Domestic Product (GDP), urbanization rates and prevalence of physical inactivity for each country were also obtained.
Subjects
The overweight, obesity and hypertension databases included information from 128, 123 and seventy-nine countries, respectively.
Results
Consumption of sugar and animal products were directly associated with GDP and urbanization rates. In a multivariate regression model, physical inactivity (B = 0·01, se = 0·005, P = 0·003), cereal consumption (B = −0·02, se = 0·006, P < 0·001) and sugar consumption (B = 0·03, se = 0·01, P = 0·03) were significant predictors of obesity prevalence. Midpoint age (B = 0·21, se = 0·10, P = 0·02), prevalence of overweight (B = 0·18, se = 0·08, P = 0·02) and consumption of cereals (B = −0·22, se = 0·10, P = 0·02) were significant predictors of hypertension. Women appeared to have a significant obesity excess compared with men.
Conclusions
High sugar consumption and sedentary lifestyle are associated with increased obesity prevalence. The non-linear association of sugar consumption with prevalence of obesity suggests that effective strategies to reduce its consumption may have differential effects in countries at different stages of the nutrition transition.
Keywords: Added sugar, Animal products, Obesity, Hypertension, Food balance sheets, Ecological analysis
The WHO predicts that developing countries will increasingly contribute to worldwide cardiovascular mortality over the next two decades( 1 ). Obesity and hypertension are two of the most important cardiovascular risk factors( 2 , 3 ). Between 1980 and 2008, mean BMI worldwide increased by 0·4 kg/m2 per decade for men and 0·5 kg/m2 per decade for women( 4 ). Conversely, the global prevalence of elevated systolic blood pressure (SBP) has decreased slightly since 1980, but trends vary significantly across regions and countries, and SBP is currently highest in low- and middle-income countries( 5 ).
At the proximate level, higher personal income, sedentariness and urbanization are generally considered to play a key role in these upward trends in worldwide chronic disease risk factors( 6 ), but beyond that, it is essential to identify the components of urban living that contribute causally to increased chronic diseases. The term ‘nutrition transition’ is used widely to refer to the shift to Western dietary patterns( 7 ), but again, the specific foods which are important health modifiers remain debated, hindering the identification of clear guidelines for healthy diets.
Changes in the socio-economic status of developing countries including higher personal income and decreased relative food prices suggest that a larger number of consumers are now able to afford a wider variety of food products and in greater quantities( 8 , 9 ). These changes facilitate increased energy intake and the adoption of dietary patterns which are characteristic of Western consumers with a higher level of personal income( 6 ). In addition, rapid urbanization in developing countries affects both sides of the energy balance equation (energy intake and energy expenditure). Specifically, higher energy intake has been directly associated with increased consumption of animal-based products, refined grains, sugar-sweetened beverages and vegetable oils, which have progressively substituted a diet high in vegetal products and fibre( 10 ). Urbanization is also often associated with less physical labour and a more sedentary lifestyle( 11 , 12 ).
The global consumption of sugar and animal products has increased steadily in the last five decades and highly populated, emerging economies have assumed a key role in driving worldwide demand for these food commodities( 13 ). India, East Asia and Latin America continue to drive growth in world sugar consumption and the FAO predicts an increase of about 2·0 % per annum over the next decade( 14 , 15 ). Conversely, per capita sugar consumption in developed countries has continued to decline in the past decade, probably related to health concerns and near saturation of the sugar and sweetener markets( 16 – 18 ). However, per capita sugar consumption in developed countries remains high and, according to recent estimates, it may account for >20 % of the total energy ingested by some individuals( 19 – 21 ).
Similarly, in emerging economies the consumption of animal products has increased progressively as a consequence of the substitution of traditional dietary patterns, based largely on unrefined vegetable products, with Western-style foods with a high content of sugar and animal fat( 9 ). Consumption of animal products has risen steeply in China( 22 , 23 ), India( 24 ) and Latin America( 25 ), but rapid global changes in the marketing and promotion of Western products are now affecting poorer countries at earlier stages of the nutrition transition, e.g. the sub-Saharan Africa region( 26 , 27 ). While increased consumption of animal products in these countries may have beneficial effects on the population's nutritional health by providing high-quality protein and greater intakes of vitamins and minerals( 28 ), there may also be potential for increased risk of non-communicable diseases associated with higher intakes of saturated fat and cholesterol( 29 , 30 ).
We have therefore conducted an ecological analysis to examine the associations between the energy availability for consumption from various food commodities (cereals, sugar, sweeteners and honey, vegetable oil, vegetables, fruits, starchy roots, pulses, alcoholic beverages, meat, animal fat, eggs, milk, and fish and seafood), sociodemographic variables (age, world regions, per capita Gross Domestic Product (GDP), urbanization rates), physical inactivity and global distribution of the prevalence rates of overweight, obesity and hypertension. We also tested for gender-specific differences in overweight, obesity and hypertension prevalence estimates and explored whether the associations between disease prevalence estimates and consumption of sugar varied with per capita GDP.
Methods
The study was undertaken in four consecutive phases. We first developed the study protocol and defined the inclusion and exclusion criteria for the selection of the prevalence estimates of overweight, obesity and hypertension. Second, the most recent prevalence rates for each country were retrieved using the WHO Global Infobase database (https://apps.who.int/infobase/Indicators.aspx). The third step aligned the year- and country-specific Food Balance Sheets (FBS) with the disease estimates. The last phase was dedicated to obtain information on urbanization rates, per capita GDP and physical inactivity. The project was undertaken between June and December 2009. An outline of the different phases of the study is described in the online Supplementary Materials (Figure S1). The corresponding authors could supply these data upon request. A list of the countries included in the analyses is also provided in the online Supplementary Materials.
Prevalence of overweight, obesity and hypertension
The WHO Global Infobase is a databank that collects, stores and displays information on chronic diseases and their risk factors for all WHO Member States. The Infobase specifically assembles non-communicable disease prevalence data collected from WHO Member States using standardized protocols (https://apps.who.int/infobase/Indicators.aspx).
We extracted the most recent disease prevalence estimates for each country until 2007 and this upper limit was set by the unavailability of data on food consumption from the FBS after 2007. The aggregate prevalence rate for both sexes was obtained and, when available, we also included the prevalence estimates for males and females. Information on the age range, sample size, survey identification code and the type of survey (national/sub-national) was obtained. Age was calculated as the midpoint of the age range of the survey (midpoint age). Prevalence estimates from national surveys were entered first and sub-national data were utilized if nationally representative estimates were unavailable.
Prevalence estimates for overweight (BMI ≥ 25·0 kg/m2) and obesity (BMI ≥ 30·0 kg/m2) were obtained. We did not exclude countries based on the diagnostic protocols (physical measurement, self-reported) used in each survey for the assessment of overweight and obesity status.
The criteria for the inclusion of country-specific prevalence estimates for hypertension were more selective. Countries were included in the database if hypertension diagnosis was based on: (i) SBP ≥140 mmHg and/or diastolic blood pressure (DBP) ≥90 mmHg; or (ii) SBP ≥140 mmHg and/or DBP ≥90 mmHg or on antihypertensive medication. Countries were excluded if the prevalence estimates were either derived from self-reported diagnosis of hypertension or used SBP ≥160 mmHg and/or DBP ≥95 mmHg as diagnostic criteria for hypertension.
Food availability for consumption
The FAOSTAT database developed by the FAO was accessed to obtain year-specific data from FBS on food availability consumption for each country until 2007 (http://faostat.fao.org/site/368/default.aspx#ancor).
FBS present a comprehensive picture of the pattern of a country's food supply during a specified reference period. The FBS shows the availability for human consumption for each food commodity which corresponds to the sources of supply and its utilization. The estimates are derived from the total quantity of foodstuffs produced in a country added to the total quantity imported and adjusted to any change in stocks that may have occurred since the beginning of the reference period, which gives the supply available during a specific period. The per capita supply of each food item available for human consumption is then obtained by dividing the respective quantity by the related data on the population size( 31 ). Data on per capita food supplies are expressed in terms of quantity (kg/capita per year) and, by applying appropriate food composition factors, also in terms of dietary energy value (kJ/capita per d).
Information on energy availability for consumption was extracted from FBS for the following selected commodities: (i) cereals – excluding beer; (ii) sugar and sweeteners and honey; (iii) sugar; (iv) sweeteners, other; (v) honey; (vi) vegetable oil; (vii) vegetables, total; (viii) fruits – excluding wine; (ix) starchy roots; (x) pulses; (xi) alcoholic beverages; (xii) meat, total; (xiii) animal fat; (xiv) eggs; (xv) milk; and (xvi) fish and seafood.
Sugar included energy available for consumption from sugar beets and sugar cane. Honey was classified as a separate product. Sweeteners comprised products used for sweetening that are derived from sugar crops, cereals, fruits or milk, which included maple sugar and syrups, caramel, golden syrup, artificial and natural honey, maltose, glucose, dextrose, isoglucose (also known as high-fructose corn syrup), other types of fructose, sugar confectionery and lactose. Total sugar consumption (all sugar = sugar + sweeteners + honey) was used in the analyses to investigate the association between sugar consumption and disease prevalence estimates. We found that the associations between sugar intake and disease prevalence estimates were unaffected when sugar consumption (sugar beets + sugar cane) was included in the analysis. A schematic representation of the classification of the food products used in the analysis is provided in the online Supplementary Materials (Figure S2).
Per capita Gross Domestic Product
The World Bank database (http://data.worldbank.org/indicator/NY.GDP.PCAP.CD) was utilized to obtain the year-specific per capita GDP (in $US) for each country. Per capita GDP is GDP divided by midyear population. GDP is the sum of the gross value added by all resident producers in the economy plus any product taxes and minus any subsidies not included in the value of the products. Per capita GDP was used to categorize countries in low (<$US 1000), lower middle ($US 1000–3999), upper middle ($US 4000–11 999) and high income (≥$US 12 000) groups.
World geographical location
Countries were categorized in the following world regions: CA = Central Asia; EA = East Asia; EU = Europe; LA = Latin America; NA = North America; NAF = North Africa; AUA = Australasia and Pacific Islands; and SSA = sub-Saharan Africa.
Urbanization
The percentage urbanization of each country was obtained from the UN Population Division database (http://esa.un.org/unpd/wup/CD-ROM/Urban-Rural-Population.htm). Urbanization was defined as the percentage of the population living in urban areas. The database reported statistics in five-year periods and therefore we calculated the average of the urbanization statistics for each country between 1990 and 2010.
Insufficient physical activity
The WHO Global Health Observatory Data Repository database (http://apps.who.int/ghodata/?vid=2469) was utilized to obtain the prevalence of physical inactivity for each country. Physical inactivity was defined as not meeting any of the following criteria: (i) at least 30 min of moderate-intensity activity daily on at least 5 d/week; (ii) at least 20 min of vigorous-intensity activity daily on at least 3 d/week; or (iii) an equivalent combination( 32 ). The WHO Global Health Observatory Data Repository included only those surveys that captured activity across all domains of life including work/household, transport and leisure time. Data had to come from a random sample of the general population, with clearly indicated survey methods (http://www.who.int/gho/ncd/methods/en/index.html).
Statistical analyses
The Mann–Whitney U test was used to test for gender differences in prevalence estimates of obesity and hypertension. The Kruskall–Wallis test was used to test differences in sugar and animal products consumption between countries stratified by per capita GDP and world regions. Spearman rank correlation analyses was used to evaluate the strength and direction of the associations between food availability for consumption and prevalence estimates of overweight, obesity and hypertension.
Stepwise multiple linear regression modelling was performed to identify predictors of overweight, obesity and hypertension prevalence estimates (dependent variables). Variables were checked for normality of distribution (Q–Q plots) and appropriate transformations were applied to correct for skewness. Per capita GDP showed a significant deviation from normality and therefore it was log-transformed before each analysis. The coefficient of determination R 2 was estimated to measure the proportion of variability in the data set that was accounted for by the linear regression models. The normality of the error distribution was tested using normal probability plots. Overweight and obesity prevalence estimates were log-transformed to improve the linearity of the models, whereas no transformation was required for hypertension prevalence estimates. Independent variables entered into the models were: age, urbanization, per capita GDP, and energy availability from animal products, cereals, fruit, total vegetables, all sugar and vegetable oils. Overweight prevalence was also added to the hypertension model.
Locally weighted scatter plot smoothed (LOWESS, bandwidth = 0·5, epanechnikov function) curves were fitted to identify the nature of the relationship between exposure (energy from all sugar and animal products consumption) and outcome (overweight, obesity and hypertension prevalence) variables.
A curve-fitting analysis was then performed to identify the best fit to the data on disease prevalence estimates and sugar energy availability for consumption. The selection of the best model was based on the value of the coefficient of determination R 2, regression coefficients and P values of the models. Analyses were undertaken using Excel® 2007 for Windows and SPSS 17 for Windows. Statistical significance was set at P < 0·05.
Results
The databases for overweight, obesity and hypertension analyses included 128, 123 and seventy-nine countries, respectively. The distribution of the per capita GDP was skewed, as more than 60 % of the countries were in either the low or lower-middle income category. In addition, the income stratification of the countries highlighted a distinctive clustering with regard to sugar consumption, such that high-income and Westernized countries were characterized by a greater consumption of sugar (Figure S3A and S3B, online Supplementary Materials). Per capita GDP and urbanization rates were directly significantly associated with all food commodities, whereas an inverse association was observed for cereals, starchy roots and pulses consumption. Physical inactivity was inversely associated with cereals consumption and it showed a significant direct correlation with urbanization and per capita GDP (Table 1).
Table 1.
Correlation analysis between disease prevalence estimates, per capita GDP, urbanization rates and percentage of energy available for consumption
| Prevalence (%) | ||||||
|---|---|---|---|---|---|---|
| Overweight | Obesity | Hypertension | Urbanization (%) | Inactivity (%) | ||
| Percentage of energy availability for consumption | (BMI = 25·0–29·9 kg/m2) | (BMI ≥ 30·0 kg/m2) | (SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg) | Per capita GDP ($US) | (percentage of the population living in urban areas) | (percentage of the population inactive) |
| Number of countries | 128 | 132 | 79 | 137 | 137 | 98 |
| Cereals – excluding beer | −0·31*** | −0·22** | −0·40*** | −0·56*** | −0·45*** | −0·27** |
| Sugar & sweeteners & honey | 0·37*** | 0·31*** | 0·31** | 0·46*** | 0·40*** | 0·17 |
| Sugar, raw equivalent | 0·38*** | 0·32*** | 0·31** | 0·41*** | 0·34*** | 0·17 |
| Sweeteners, other | 0·35*** | 0·31*** | 0·35** | 0·56*** | 0·40*** | 0·20* |
| Honey | 0·29** | 0·16 | 0·17 | 0·49*** | 0·41*** | 0·14 |
| Vegetable oils | 0·18* | 0·12 | 0·15 | 0·35*** | 0·40*** | 0·28** |
| Fruits – excluding wine | 0·25** | 0·20* | 0·01 | 0·17* | 0·14 | 0·29** |
| Starchy roots | −0·19* | −0·10 | −0·05 | −0·22** | −0·10 | −0·17 |
| Pulses | −0·01 | 0·008 | −0·06 | −0·39*** | −0·32*** | 0·01 |
| Vegetables, total | 0·34*** | 0·25** | 0·34*** | 0·39*** | 0·33*** | 0·21* |
| Alcoholic beverages | 0·09 | 0·001 | 0·34*** | 0·47*** | 0·26** | 0·08 |
| Meat, total | 0·32*** | 0·28*** | 0·32*** | 0·60*** | 0·43*** | 0·35*** |
| Animal fat | 0·34*** | 0·26** | 0·38*** | 0·60*** | 0·46*** | 0·16 |
| Eggs | 0·27** | 0·09 | 0·39*** | 0·62*** | 0·49*** | 0·21 |
| Milk | 0·37*** | 0·27** | 0·42*** | 0·58*** | 0·41*** | 0·21 |
| Fish & seafood | 0·01 | 0·01 | 0·12 | 0·31*** | 0·16 | 0·15 |
| Per capita GDP ($US) | 0·50*** | 0·36*** | 0·43*** | – | 0·73*** | 0·34*** |
| Urbanization (%) | 0·39*** | 0·28** | 0·32** | – | – | 0·33*** |
| Physical inactivity (%) | 0·27** | 0·34*** | 0·21 | 0·34*** | 0·33*** | – |
| (n 93)† | (n 94)† | (n 62)† | (n 98)† | (n 98)† | ||
GDP, Gross Domestic Product; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Spearman rank coefficients of correlation are reported. *P<0·05; **P<0·01; ***P<0·001.
†Number of countries included in the analyses of physical inactivity (%).
Correlation analyses
All sugar consumption was directly associated with overweight (ρ = 0·37, P < 0·001), obesity (ρ = 0·31, P < 0·001) and hypertension (ρ = 0·31, P < 0·001) prevalence estimates. Sugar consumption (sugar beets + sugar cane) showed a similar pattern of association. Consumption of cereals was inversely associated with overweight (ρ = −0·31, P < 0·001), obesity (ρ = −0·22, P < 0·01) and hypertension (ρ = −0·40, P < 0·001), whereas a higher consumption of starchy roots was indirectly associated with overweight (ρ = −0·19, P < 0·05). We found that meat, animal fat and milk consumption were directly associated with obesity and hypertension prevalence estimates. Consumption of alcoholic beverages (ρ = 0·34, P < 0·001) and eggs (ρ = 0·39, P < 0·001) were directly associated with hypertension. Surprisingly, fruit and vegetables consumption was directly correlated with obesity (fruit, ρ = 0·20, P < 0·05; vegetables, ρ = 0·25, P < 0·01) and hypertension (vegetables, ρ = 0·34, P < 0·001) prevalence estimates. However, the associations were not significant after adjustment for per capita GDP (data not shown). Per capita GDP and urbanization rates were significantly associated with obesity and hypertension prevalence estimates and physical inactivity showed a significant correlation with obesity prevalence estimates (Table 1).
Multiple linear regression analyses
When sociodemographic and food consumption variables were entered into the regression model, we found that energy from all sugar (B = 0·04, se = 0·01, P = 0·009) and fish and seafood products (B = −0·12, se = 0·06, P = 0·03) consumption were significant predictors of obesity prevalence (Table 2, Model 1). Midpoint age (B = 0·30, se = 0·12, P = 0·01) and eggs consumption (B = 0·21, se = 0·06, P < 0·001) were significant predictors of hypertension prevalence estimates (Table 2, Model 1). The inclusion of physical inactivity improved the robustness of the models (increase in coefficients of determination R 2) and all sugar consumption (B = 0·03, se = 0·01, P = 0·03), cereals consumption (B = −0·02, se = 0·006, P < 0·001) and physical inactivity (B = 0·01, se = 0·005, P = 0·003) were significantly associated with obesity prevalence estimates. Cereals consumption (B = −0·22, se = 0·10, P = 0·02) was again a significant predictor of hypertension prevalence estimates, together with midpoint age (B = 0·21, se = 0·10, P = 0·02) and overweight prevalence (B = 0·18, se = 0·08, P = 0·02; Table 2, Model 2).
Table 2.
Results of stepwise multiple linear regression analyses to identify dietary, lifestyle and sociodemographic predictors of overweight, obesity and hypertension prevalence estimates
| Overweight† | Obesity† | Hypertension | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | se | P | B | se | P | B | se | P | |||||||
| Model 1 | (n 128) | (n 132) | (n 70)‡ | ||||||||||||
| R 2 | 0·37 | 0·23 | 0·24 | ||||||||||||
| Per capita GDP ($US) | 0·09 | 0·03 | 0·006 | 0·17 | 0·04 | <0·001 | – | – | – | ||||||
| Energy from milk (%) | 0·02 | 0·01 | 0·008 | – | – | – | – | – | – | ||||||
| Energy from vegetables (%) | 0·07 | 0·03 | 0·04 | – | – | – | – | – | – | ||||||
| Energy from all sugar (%) | 0·02 | 0·01 | 0·02 | 0·04 | 0·01 | 0·009 | – | – | – | ||||||
| Energy from fish & seafood products (%) | – | – | – | −0·12 | 0·06 | 0·03 | – | – | – | ||||||
| Energy from eggs (%) | – | – | – | – | – | – | 0·21 | 0·06 | <0·001 | ||||||
| Midpoint age (years) | – | – | – | – | – | – | 0·30 | 0·12 | 0·01 | ||||||
| Model 2 | (n 93) | (n 98) | (n 57)‡ | ||||||||||||
| R 2 | 0·49 | 0·35 | 0·33 | ||||||||||||
| Per capita GDP ($US) | 0·19 | 0·02 | <0·001 | – | – | – | – | – | – | ||||||
| Energy from all sugar (%) | – | – | – | 0·03 | 0·01 | 0·03 | – | – | – | ||||||
| Energy from cereals (%) | – | – | – | −0·02 | 0·006 | <0·001 | −0·22 | 0·10 | 0·02 | ||||||
| Midpoint age (years) | – | – | – | – | – | – | 0·21 | 0·10 | 0·02 | ||||||
| Overweight prevalence (%) | – | – | – | – | – | – | 0·18 | 0·08 | 0·02 | ||||||
| Physical inactivity (%) | – | – | – | 0·01 | 0·005 | 0·003 | – | – | – | ||||||
B, unadjusted regression coefficient; R 2, explained variance; n, number of countries; GDP, Gross Domestic Product.
Results are shown for significant variables. Independent variables entered into Model 1 were: midpoint age, urbanization, per capita GDP, energy from cereals, fruit, total vegetables, all sugar, vegetable oils, starchy roots, pulses, alcoholic beverages, meat, animal fat, eggs, milk, and fish and seafood. Model 2 = Model 1+physical inactivity. Overweight prevalence was also added to the hypertension model. Age was calculated as the midpoint of the reported age range (online Supplementary Materials).
†Dependent variable log-transformed to fit linearity assumptions of the regression models (see Methods for details).
‡Missing data on overweight prevalence estimates determined the lower number of cases.
When we examined the relationship between sugar consumption, disease prevalence estimates and GDP, we found that the nature of the association was essentially curvilinear (Fig. 1(a) to (c)). A steeper increase in overweight and obesity prevalence was noticed for sugar consumption in the lower range, which coincidentally clustered with countries with low and middle income. Conversely, in more affluent countries, overweight and obesity prevalence estimates tended to be less strongly associated with sugar consumption (Fig. 1(a) and (b)). A similar pattern was found between hypertension prevalence and consumption of sugar (Fig. 1(c)). Specifically, the latter showed a steeper rise in hypertension prevalence for sugar consumption less than 20 %, a level of intake generally observed in low-income countries. We confirmed the non-linearity of the associations by testing the best models fitting the all sugar consumption and disease prevalence data sets (obesity, hypertension). The analyses showed that an exponential model appeared to provide the best fit to the obesity and all sugar consumption data sets, whereas the association between all sugar consumption and hypertension was best explained by a cubic model (Table S1 and Figure S4A and S4B, online Supplementary Materials).
Fig. 1.
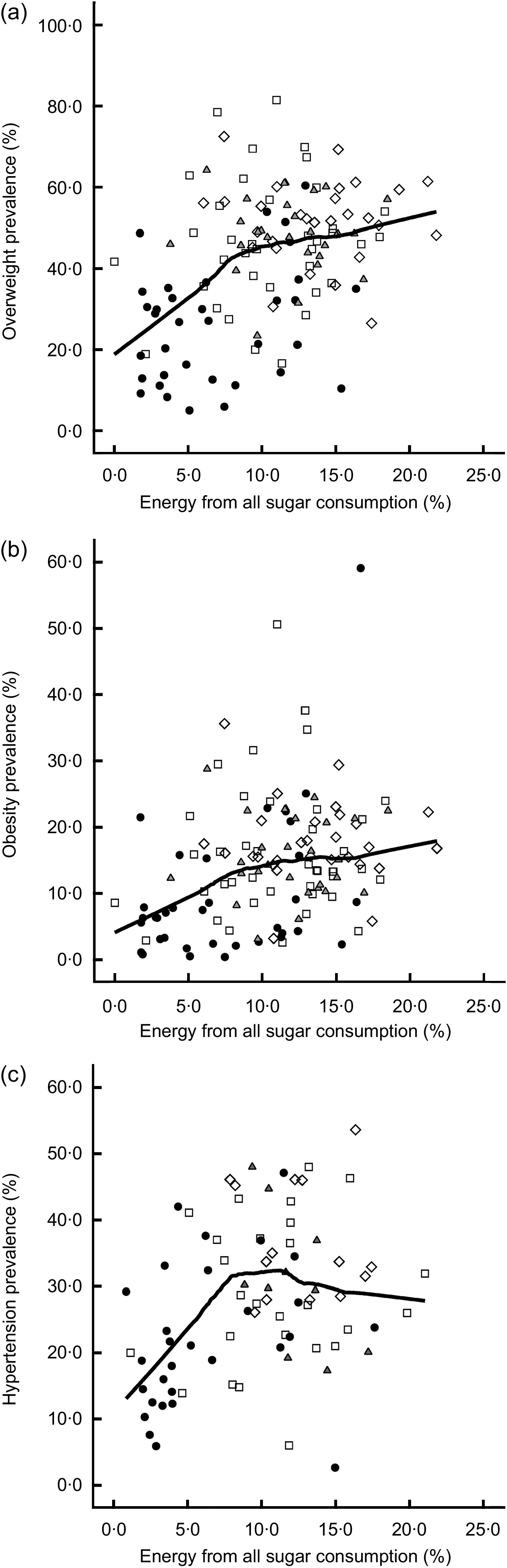
Evaluation of the relationship between all sugar consumption and (a) overweight, (b) obesity and (c) hypertension prevalence estimates according to per capita Gross Domestic Product ( , <$US 1000 (low);
, <$US 1000 (low);  , $US 1000–3999 (lower middle);
, $US 1000–3999 (lower middle);  , $US 4000–11 999 (upper middle);
, $US 4000–11 999 (upper middle);  , ≥$US 12 000 (high)).
, ≥$US 12 000 (high)).  shows the fit line for total. Data on overweight, obesity and hypertension from 128, 123 and seventy-nine countries, respectively, which were fit using the LOWESS model with a bandwidth of 0·5
shows the fit line for total. Data on overweight, obesity and hypertension from 128, 123 and seventy-nine countries, respectively, which were fit using the LOWESS model with a bandwidth of 0·5
Gender and income effects
Overweight and obesity prevalence estimates showed significant between-gender differences and a close association with per capita GDP groups. Women were more likely to be overweight in countries with low income (Fig. 2(a)) and the gap was even more pronounced in the obese group, as almost all countries showed an obesity excess in women (Fig. 2(b)). The significant link between income, gender and prevalence rates for overweight and obesity was also confirmed by the greater overweight prevalence rates in men living in high-income countries (per capita GDP ≥$US 12 000) and by the similar prevalence rates for obesity in men (14·7 %) and women (16·0 %; Table S2, online Supplementary Materials). Overall, a significant gender difference was observed for obesity (P < 0·001) and not for overweight prevalence rates (P = 0·21; Table S3, online Supplementary Materials). Although we observed a greater overlap of men and women for hypertension, men seemed to be characterized by a marginal excess of hypertension which was not modified by per capita GDP (Fig. 2(c)). The association between level of income and hypertension prevalence was significant only in men (P = 0·006), which was reflected in greater overall hypertension prevalence rates compared with women (P = 0·04; Tables S4 and S5, online Supplementary Materials).
Fig. 2.
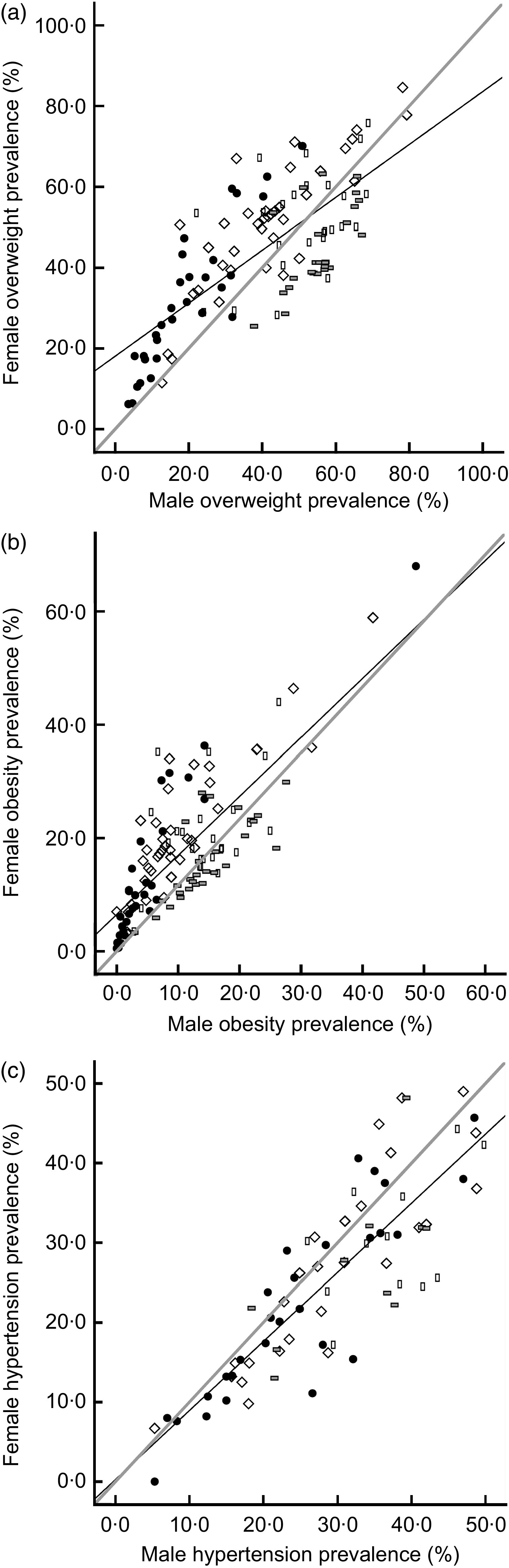
Gender differences in (a) overweight, (b) obesity and (c) hypertension prevalence estimates according to per capita Gross Domestic Product ( , <$US 1000 (low);
, <$US 1000 (low);  , $US 1000–3999 (lower middle);
, $US 1000–3999 (lower middle);  , $US 4000–11 999 (upper middle);
, $US 4000–11 999 (upper middle);  , ≥$US 12 000 (high)).
, ≥$US 12 000 (high)).  shows the regression fit line for total;
shows the regression fit line for total;  shows the identity line; coefficient of determination R
2 = 0·547 for overweight, 0·603 for obesity and 0·712 for hypertension. Data on overweight, obesity and hypertension from 128, 123 and seventy-nine countries, respectively
shows the identity line; coefficient of determination R
2 = 0·547 for overweight, 0·603 for obesity and 0·712 for hypertension. Data on overweight, obesity and hypertension from 128, 123 and seventy-nine countries, respectively
Discussion
To improve world health the WHO has recommended limiting the consumption of added sugars to less than 10 % of total energy intake( 1 , 32 ) and engaging in regular, moderate and/or vigorous physical activity( 33 , 34 ). More recently, the American Heart Association has further lowered the upper limit for added sugar intake to ∼6·0 %( 21 ). In addition, current dietary recommendations emphasize the importance of increasing the consumption of whole grains, fruit and vegetables and of lowering the intake of animal products to reduce saturated fat and cholesterol intakes( 1 , 35 ).
Our results have corroborated the validity of these recommendations across countries by verifying empirically, on a worldwide scale, the significant association of all sugar and cereal products consumption and physical inactivity with obesity and hypertension prevalence estimates. However, our results challenge the between-country generalizability of these recommendations and, based on the observations reported herein, we speculate that a reduction of sugar consumption may be more likely to determine greater reductions in overweight, obesity and hypertension prevalence in countries with a lower income because of (i) the steeper association of sugar consumption with obesity and hypertension prevalence estimates and (ii) the greater number of people living in low- and middle-income countries.
The present cross-sectional analysis highlighted that exposure to unhealthy dietary habits should be a major global concern. Societies across the globe are exposed continuously to economic, technological and cultural forces( 36 ). Personal income and the proportion of individuals living in urban areas are proxy indicators of changes that have occurred under the pressure of financial interests and global mobility( 37 , 38 ). In line with the nutrition transition paradigm, our analyses showed that consumption of animal products, added sugar and vegetable oils, representing Western dietary habits, increase in proportion with national GDP and with the proportion of the population living in urban areas. Fruit and vegetables consumption showed a similar trend and only cereals intake was inversely associated with urbanization and per capita GDP. These may have explained the significant correlation of fruit and vegetables consumption with obesity and hypertension prevalence estimates and how the association was removed after adjustment for per capita GDP.
Secular trends in sugar consumption have been linked with the epidemic of obesity and metabolic syndrome( 20 ) and possibly dementia( 39 ). Research from longitudinal observational studies has found repeatedly that high added sugar intake from sugar-sweetened beverages, confectionery and bakery products is associated with metabolic and cardiovascular function impairment( 40 – 42 ). In contrast, results from clinical trials testing the effects of fructose and added sugar intake on risk of weight gain and hypertension have been inconsistent. Studies with longer duration have overall reported significant effects of sugar intake on cardiometabolic health( 43 – 46 ). Several authors have recently proposed models to emphasize the capacity of fructose and fructose-derived sweeteners (sucrose, high-fructose corn syrup) to perturb cellular metabolism( 47 – 49 ). For example, Lustig( 47 ) suggested that hyperinsulinaemia has a critical role in the dysfunction of the energy balance pathway, which may be linked to autonomic dysfunction, leptin signalling or hepatic and/or skeletal muscle insulin resistance. Wells and Siervo( 48 ) similarly discussed how the modification of cellular energy levels, activation of AMP kinase and compensatory mechanisms favour adipose tissue accretion, increased appetite and lower physical activity. These conceptual models all implicate chronic hyperinsulinaemia in the presence of a paradoxical state of ‘cellular starvation’ as a key driver of the metabolic modifications leading to the continuous weight gain( 48 , 49 ).
The direct association of sugar consumption with hypertension may be explained by the effects of excessive glucose and fructose intake on metabolic and vascular health( 50 ). A high fructose and glucose intake has been linked mechanistically to an impairment of insulin signalling( 45 ), increased lipogenesis( 51 ) and disruption of vascular homeostasis( 52 , 53 ). In the International Study of Macro/Micronutrients and Blood Pressure (INTERMAP) study, sugar-sweetened beverages were significantly associated with an increased SBP and DBP and the association remained statistically significant after adjusting for differences in body mass( 54 ). Sugar intake was correlated with hypertension in our analysis but the effect was removed in the fully adjusted regression model. Overweight and physical inactivity may be on the causal pathway and explain the lack of association between sugar consumption and hypertension.
Wells et al.( 55 ) recently conducted an ecological analysis of gender disparity in obesity prevalence and our results are in line with these previous findings. Both analyses showed that the prevalence of female obesity was greater than male obesity, but this sex effect differed between populations and was greater in countries characterized by lower GDP. The greater risk for hypertension in males suggests that other factors may be explaining this reversed trend. For example, a greater prevalence of smoking observed in men living in developing countries( 56 ) as well as biological factors such as the protective effects of female sexual hormones and a greater predisposition for central adiposity in men may explain the male excess hypertension prevalence( 57 ).
Taxation of sugar-sweetened beverages has been advocated as a potential public health strategy to curb the obesity epidemic. Our findings could contribute to substantiate the link between sugar consumption and obesity, but more importantly they have emphasized the fact that policies should not be limited to high-income economies. Indeed, a rise in sugar consumption is expected in poorer countries as part of nutrition transition trends. We have observed a typical association between Westernized diets (high sugar, high fat, low vegetable intake) with geographical, demographic (gender, urbanization rates) and wealth indicators. A recent between-country comparison between retail price and availability of soft drinks in urban areas in the UK and India has recorded high accessibility to soft drinks in both countries. However, accessibility to low-energy drinks was limited in India compared with the UK, which seems to imply that sugar intake from soft drinks could rapidly rise in middle-income countries( 58 ).
The present ecological study design has several intrinsic limitations (conceptualized as ecological fallacy). Additional dietary and lifestyle factors (i.e. birth weight, psychosocial stress) could contribute to the increase in worldwide prevalence of obesity and hypertension. FBS provide estimates of energy and food availability for consumption and therefore the data may not be a robust surrogate for individual energy and food intakes. Food available for consumption is calculated by adding total food production (plus imports, minus exports) and net losses from processing at the mill level and food fed to animals. These data are a reasonable approximation of the trends in food consumption at the national level but they do not reflect actual consumption. The reliability of this dietary assessment method may also vary when it is applied to data obtained from developing and developed countries. However, the comparison of food disappearance data with household and individual food intakes suggested that disappearance data measured 20–27 % more food available for consumption. Use of a single cut-off for obesity will produce conservative findings in respect to obesity-related health outcomes, because in some countries (in particular those in Asia) the adverse effects of overweight occur at lower levels of BMI. Finally, the use of different methods for the identification of prevalent cases of obesity and hypertension may have introduced a potential bias in our analyses. However, a high correlation exists between estimates of body size (weight and height) that are self-reported and obtained by physical measurements, and the exclusion of surveys based on self-reported diagnosis of hypertension surveys may have minimized the error.
Conclusion
Our results suggest that, at a global level, high consumption of sugar, low consumption of cereals and physical inactivity could be significant contributors to the worldwide non-communicable disease epidemic. Major shifts in dietary habits are currently occurring in developing countries and resources should be invested globally to limit sugar intake and maintain traditional dietary habits rich in wholegrain products. Our results seem to suggest that the biggest benefits in terms of lowered chronic disease prevalence might occur in lower-income countries, as the association between sugar intake and disease risk is steeper for lower levels of sugar consumption.
Supplementary Material
For Supplementary Materials for this article, please visit https://doi.org/10.1017/S1368980013000141
Acknowledgements
Sources of funding: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. Conflicts of interest: The authors have no conflict of interests to declare. Ethics: Ethical approval was not required. Authors’ contributions: M.S. contributed to the design of the study, collection and analysis of the data, and wrote the manuscript. C.M. contributed to the collection of the data and to the critical revision of the manuscript. J.C.M. contributed to the interpretation of the results and to the critical revision of the manuscript. K.R.S. contributed to the data collection and interpretation of results. B.C.M.S. contributed to the statistical analysis and to the critical revision of the manuscript. J.C.K.W. designed the study and revised the final version of the manuscript.
References
- 1. World Health Organization (2003) Diet, Nutrition and the Prevention of Chronic Diseases. Joint WHO/FAO Expert Consultation. WHO Technical Report Series no. 916. Geneva: WHO. [PubMed] [Google Scholar]
- 2. Padwal R, Straus SE & McAlister FA (2001) Cardiovascular risk factors and their effects on the decision to treat hypertension: evidence based review. BMJ 322, 977–980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Lavie CJ, Milani RV & Ventura HO (2009) Obesity and cardiovascular disease: risk factor, paradox, and impact of weight loss. J Am Coll Cardiol 53, 1925–1932. [DOI] [PubMed] [Google Scholar]
- 4. Finucane MM, Stevens GA, Cowan MJ et al. (2011) National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9·1 million participants. Lancet 377, 557–567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Danaei G, Finucane MM, Lin JK et al. (2011) National, regional, and global trends in systolic blood pressure since 1980: systematic analysis of health examination surveys and epidemiological studies with 786 country-years and 5·4 million participants. Lancet 377, 568–577. [DOI] [PubMed] [Google Scholar]
- 6. Kearney J (2010) Food consumption trends and drivers. Phil Trans R Soc Lond B Biol Sci 365, 2793–2807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Popkin BM (2004) The nutrition transition: an overview of world patterns of change. Nutr Rev 62, 7 Pt 2, S140–S143. [DOI] [PubMed] [Google Scholar]
- 8. Popkin B & Ng SW (2007) The nutrition transition in high- and low-income countries: what are the policy lessons? Agric Econ Res 37, 199–211. [Google Scholar]
- 9. Popkin BM (2006) Global nutrition dynamics: the world is shifting rapidly toward a diet linked with noncommunicable diseases. Am J Clin Nutr 84, 289–298. [DOI] [PubMed] [Google Scholar]
- 10. Hu FB (2011) Globalization of diabetes. Diabetes Care 34, 1249–1257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Ng SW, Norton EC & Popkin BM (2009) Why have physical activity levels declined among Chinese adults? Findings from the 1991–2006 China Health and Nutrition Surveys. Soc Sci Med 68, 1305–1314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Popkin BM (1999) Urbanization, lifestyle changes and the nutrition transition. World Dev 27, 1905–1916. [Google Scholar]
- 13. Schmidhuber J & Shetty P (2005) The nutrition transition to 2030. Why developing countries are likely to bear the major burden. Food Econ Acta Agric Scand Sect C 2, 150–166. [Google Scholar]
- 14. Organisation for Economic Co-operation and Development & Food and Agriculture Organization of the United Nations (2011) Sugar. In OECD–FAO Agricultural Outlook 2011–2020, pp. 119–132. Paris: OECD/FAO. [Google Scholar]
- 15. Popkin BM & Nielsen SJ (2003) The sweetening of the world's diet. Obes Res 11, 1325–1332. [DOI] [PubMed] [Google Scholar]
- 16. Food and Agriculture Organization of the United Nations, Economic and Social Development Department (2006) Sugar. Rome: FAO. [Google Scholar]
- 17. Barclay A & Brand-Miller J (2011) The Australian paradox: a substantial decline in sugars intake over the same timeframe that overweight and obesity have increased. Nutrients 3, 491–504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Welsh JA, Sharma AJ, Grellinger L et al. (2011) Consumption of added sugars is decreasing in the United States. Am J Clin Nutr 94, 726–734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Lustig RH, Schmidt LA & Brindis CD (2012) Public health: the toxic truth about sugar. Nature 482, 27–29. [DOI] [PubMed] [Google Scholar]
- 20. Bray G, Nielsen SJ & Popkin BM (2004) Consumption of high-fructose corn syrup in beverages may play a role in the epidemic of obesity. Am J Clin Nutr 79, 537–543. [DOI] [PubMed] [Google Scholar]
- 21. Johnson RK, Appel LJ, Brands M et al. (2009) Dietary sugars intake and cardiovascular health: a scientific statement from the American Heart Association. Circulation 120, 1011–1020. [DOI] [PubMed] [Google Scholar]
- 22. Du S, Mroz TA, Zhai F et al. (2004) Rapid income growth adversely affects diet quality in China – particularly for the poor! Soc Sci Med 59, 1505–1515. [DOI] [PubMed] [Google Scholar]
- 23. Du S, Lu B, Zhai F et al. (2002) A new stage of the nutrition transition in China. Public Health Nutr 5, 169–174. [DOI] [PubMed] [Google Scholar]
- 24. Misra A, Singhal N, Sivakumar B et al. (2011) Nutrition transition in India: secular trends in dietary intake and their relationship to diet-related non-communicable diseases. J Diabetes 3, 278–292. [DOI] [PubMed] [Google Scholar]
- 25. Rivera JA, Barquera S, González-Cossío T et al. (2004) Nutrition transition in Mexico and in other Latin American countries. Nutr Rev 62, 7 Pt 2, S149–S157. [DOI] [PubMed] [Google Scholar]
- 26. Amuna P & Zotor FB (2008) Epidemiological and nutrition transition in developing countries: impact on human health and development. Proc Nutr Soc 67, 82–90. [DOI] [PubMed] [Google Scholar]
- 27. Vorster HH, Kruger A & Margetts BM (2011) The nutrition transition in Africa: can it be steered into a more positive direction? Nutrients 3, 429–441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Walker P, Rhubart-Berg P, McKenzie S et al. (2005) Public health implications of meat production and consumption. Public Health Nutr 8, 348–356. [DOI] [PubMed] [Google Scholar]
- 29. Song Y, Manson JE, Buring JE et al. (2004) A prospective study of red meat consumption and type 2 diabetes in middle-aged and elderly women. Diabetes Care 27, 2108–2115. [DOI] [PubMed] [Google Scholar]
- 30. Popkin BM & Du S (2003) Dynamics of the nutrition transition toward the animal foods sector in China and its implications: a worried perspective. J Nutr 133, 11 Suppl. 2, 3898S–3906S. [DOI] [PubMed] [Google Scholar]
- 31. Food and Agriculture Organization of the United Nations (2001) Food Balance Sheets. A Handbook. Rome: FAO. [Google Scholar]
- 32. Ruxton CH, Gardner EJ & McNulty HM (2010) Is sugar consumption detrimental to health? A review of the evidence 1995–2006. Crit Rev Food Sci Nutr 50, 1–19. [DOI] [PubMed] [Google Scholar]
- 33. World Health Organization (2010) Global Recommendations on Physical Activity for Health. Geneva: WHO. [PubMed] [Google Scholar]
- 34. Kohl HW, Craig CL, Lambert EV et al. (2012) The pandemic of physical inactivity: global action for public health. Lancet 380, 294–305. [DOI] [PubMed] [Google Scholar]
- 35. Lichtenstein AH, Appel LJ, Brands M et al. (2006) Diet and lifestyle recommendations revision 2006. Circulation 114, 82–96. [DOI] [PubMed] [Google Scholar]
- 36. McMichael A (2000) The urban environment and health in a world of increasing globalization: issues for developing countries. Bull World Health Organ 78, 1117–1225. [PMC free article] [PubMed] [Google Scholar]
- 37. Wells JC (2012) Obesity as malnutrition: the role of capitalism in the obesity global epidemic. Am J Hum Biol 24, 261–276. [DOI] [PubMed] [Google Scholar]
- 38. Guillén MF (2001) Is globalization civilizing, destructive or feeble? A critique of five key debates in the social science literature. Annu Rev Sociol 27, 235–260. [Google Scholar]
- 39. Stephan BC, Wells JC, Brayne C et al. (2010) Increased fructose intake as a risk factor for dementia. J Gerontol A Biol Sci Med Sci 65, 809–814. [DOI] [PubMed] [Google Scholar]
- 40. Malik VS, Popkin BM, Bray GA et al. (2010) Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes. Diabetes Care 33, 2477–2483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. de Koning L, Malik VS, Kellogg MD et al. (2012) Sweetened beverage consumption, incident coronary heart disease, and biomarkers of risk in men/clinical perspective. Circulation 125, 1735–1741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Stanhope KL (2012) Role of fructose-containing sugars in the epidemics of obesity and metabolic syndrome. Annu Rev Med 63, 329–343. [DOI] [PubMed] [Google Scholar]
- 43. Ha V, Sievenpiper JL, de Souza RJ et al. (2012) Effect of fructose on blood pressure: a systematic review and meta-analysis of controlled feeding trials. Hypertension 59, 787–795. [DOI] [PubMed] [Google Scholar]
- 44. Sievenpiper JL, de Souza RJ, Mirrahimi A et al. (2012) Effect of fructose on body weight in controlled feeding trials: a systematic review and meta-analysis. Ann Intern Med 156, 291–304. [DOI] [PubMed] [Google Scholar]
- 45. Stanhope KL, Schwarz JM, Keim NL et al. (2009) Consuming fructose-sweetened, not glucose-sweetened, beverages increases visceral adiposity and lipids and decreases insulin sensitivity in overweight/obese humans. J Clin Invest 119, 1322–1334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Aeberli I, Gerber PA, Hochuli M et al. (2011) Low to moderate sugar-sweetened beverage consumption impairs glucose and lipid metabolism and promotes inflammation in healthy young men: a randomized controlled trial. Am J Clin Nutr 94, 479–485. [DOI] [PubMed] [Google Scholar]
- 47. Lustig RH (2006) Childhood obesity: behavioral aberration or biochemical drive? Reinterpreting the First Law of Thermodynamics. Nat Clin Pract Endocrinol Metab 2, 447–458. [DOI] [PubMed] [Google Scholar]
- 48. Wells JC & Siervo M (2011) Obesity and energy balance: is the tail wagging the dog? Eur J Clin Nutr 65, 1173–1189. [DOI] [PubMed] [Google Scholar]
- 49. Taubes G (2009) The Diet Delusion: Challenging the Conventional Wisdom on Diet, Weight Loss and Disease. London: Vermilion. [Google Scholar]
- 50. Johnson RK, Appel LJ, Brands M et al. (2009) Dietary sugars intake and cardiovascular health. Circulation 120, 1011–1020. [DOI] [PubMed] [Google Scholar]
- 51. Samuel VT (2011) Fructose induced lipogenesis: from sugar to fat to insulin resistance. Trends Endocrinol Metab 22, 60–65. [DOI] [PubMed] [Google Scholar]
- 52. Mah E, Noh SK, Ballard KD et al. (2011) Postprandial hyperglycemia impairs vascular endothelial function in healthy men by inducing lipid peroxidation and increasing asymmetric dimethylarginine:arginine. J Nutr 141, 1961–1968. [DOI] [PubMed] [Google Scholar]
- 53. Siervo M, Corander M, Stranges S et al. (2011) Post-challenge hyperglycaemia, nitric oxide production and endothelial dysfunction: the putative role of asymmetric dimethylarginine (ADMA). Nutr Metab Cardiovasc Dis 21, 1–10. [DOI] [PubMed] [Google Scholar]
- 54. Brown IJ, Stamler J, Van Horn L et al. (2011) Sugar-sweetened beverage, sugar intake of individuals, and their blood pressure. Hypertension 57, 695–701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Wells JCK, Marphatia AA, Cole TJ et al. (2012) Associations of economic and gender inequality with global obesity prevalence: understanding the female excess. Soc Sci Med 75, 482–490. [DOI] [PubMed] [Google Scholar]
- 56. Collishaw N & Lopez A (1995) Prevalence of cigarette smoking in developing countries. Tob Control 4, 327–328. [Google Scholar]
- 57. Klein S, Allison DB, Heymsfield SB et al. (2007) Waist circumference and cardiometabolic risk: a consensus statement from Shaping America's Health: Association for Weight Management and Obesity Prevention; NAASO, The Obesity Society; the American Society for Nutrition; and the American Diabetes Association. Am J Clin Nutr 85, 1197–1202. [DOI] [PubMed] [Google Scholar]
- 58. Taylor FC, Satija A, Khurana S et al. (2011) Pepsi and Coca Cola in Delhi, India: availability, price and sales. Public Health Nutr 14, 653–660. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
For Supplementary Materials for this article, please visit https://doi.org/10.1017/S1368980013000141