

Abstract
Purpose:
To assess the prevalence, length, and patterns of the anterior loop of the inferior alveolar nerve by panoramic radiography and cone beam computed tomography (CBCT).
Materials and Methodology:
A prospective study was conducted on 300 mental foramen regions by exposing them to panoramic radiography and CBCT scan. Two individual observers evaluated the images to assess the presence of an anterior loop, the mean length of the loop, and the most frequent pattern of the loop in our population.
Result Analysis:
The prevalence of the anterior loop for male patients and female patients by panoramic radiography was 34% and 32% on the right side and 30% and 36% on left side, respectively. By CBCT, the corresponding values were 69% and 72% on the right and left side, respectively, for male patients, and 73% and 81% on the right and left side, for female patients, respectively.
Conclusion:
The results from our study strongly emphasize the need for CBCT imaging before planning for procedures in the mental foramen region because the prevalence, length, and pattern of loop significantly varies with respect to age, sex, and population.
Keywords: anterior loop, cone beam computed tomography, inferior alveolar nerve, mental foramen, panoramic radiography
Introduction
The inferior alveolar nerve occasionally passes below the anterior wall of the mental foramen, and after giving off a small incisive branch, it curves back forming a loop to enter the foramen. This anatomical landmark is known as “the anterior loop” of the inferior alveolar nerve.1
It is essential to comprehensively understand the anatomical structures in the interforaminal region encompassing the anterior loop to avoid neurosensory disturbances. These are due to damage to the neurovascular bundle during surgical procedures such as placement of a dental implant, osteotomy, root end resection, reducing a mandibular fracture, and genioplasty.2
There is a high chance of implant failure if they come in contact with the anterior loop because of increased edema and a lack of hard tissue support together with increasing soft tissue in the area.3 Certain systemic diseases such as diabetes and osteoporosis affect the bone by reducing its mineral density leading to decortication of the nerve canals.4 A safe distance of 5 mm is recommended from the mental foramen for procedures such as implant placement, while planning endodontic surgery and harvesting the chin bone.5
Today, cone beam computed tomography (CBCT) has taken a massive role for imaging of the hard tissues in the maxillofacial area. While CBCT allows imaging of the anatomical structures in axial, coronal, and sagittal planes, it also allows us to interpret the structures without magnification or distortion on oblique and inclined surfaces because of its multiplanar reformation feature.6,7
Before CBCT, panoramic radiography was the only diagnostic imaging modality taken for a long time, but in most of the cases, this modality did not help in accurate identification of the extension of the anterior loop.8
Thus, the purpose of the study was to assess the morphometric variations of the anterior loop by two imaging modalities such as panoramic radiography and CBCT.
Materials and Methodology
This is a prospective study performed on patients visiting the Department of Oral Medicine and Radiology. The study was performed following the fundamental principles of the Declaration of Helsinki (2013). The ethical clearance for this study was obtained from the Institutional Ethical Committee (Approval No: 084). This study was performed in an institution with a time frame of 1 year. The formula used for sample size estimation was n = Z2 P (1-P)/d2. In this formula, n is the sample size, Z is the statistic corresponding to the level of confidence, P is expected prevalence (that can be obtained from similar studies or a pilot study conducted by the researchers), and d is precision (corresponding to effect size). The level of confidence aimed for is usually 99%. The sample size was confirmed using the Raosoft software, 2004. The machine used for obtaining CBCT scan was KODAK 9500 CONE BEAM 3D SYSTEM which works on flat panel amorphous silicon sensor. The patients were scanned in a standing position. The field of view selected for the scan was 18 cm × 20 cm and voxel size of 0.3 mm. The exposure parameters set for the scan was 80 kVp, 12 mA with 14.3 seconds of exposure time. A panoramic scan was taken by PLANMECA proline XC with exposure parameters 66kVp, 6 mA with an exposure time of 18 seconds.
The study population included 150 patients (75 male patients and 75 female patients) of an age group ranging from 20 to 65 years. The study population was divided into three groups based on their age, and each group had an equal number of patients (50 each)—Group I (20–35 years), Group II (36–50 years), and III (51–65 years). Patients were selected from those who were indicated for both panoramic radiography and cone beam CT. For instance, cases with multiple affected molars, for orthodontic and orthognathic surgeries, odontomes or any pathology that did not affect the nerve position, where OPG was taken as a preliminary radiograph followed by additional radiograph aided in further treatment planning. The inclusion criteria included permanent dentition and patients with teeth confined to the mental foramen region from the canine to the first molar. Pregnant women, patients with generalized skeletal disorders, or any pathology/trauma/radiolucent/radiopaque lesion affecting the position of the nerve, mixed dentition, supernumerary teeth, unerupted, or affected teeth were excluded from the study. Radiographs that lack proper exposure or artefact were not included for examination. All selected patients were explained about the need of the study. Individually voluntary informed written consent was obtained from the subjects of the study.
The study focused on evaluating 300 mental foramen regions. Measurements in panoramic radiographs were performed using Planmeca Romexis software and in CBCT using Imaging Software by clicking on the measurement mode present in the tool bar option. Measurements of the anterior loop on panoramic radiographs were assessed by considering the inferior mandibular cortex as the plane of reference. A line was drawn perpendicular to the line passing through the medial border of the mental foramen. Another line was drawn perpendicular to the line passing through the most mesial point of the anterior loop and the mandibular incisive canal. The distance between the two lines drawn was measured and recorded (Fig. 1).9
Figure 1.
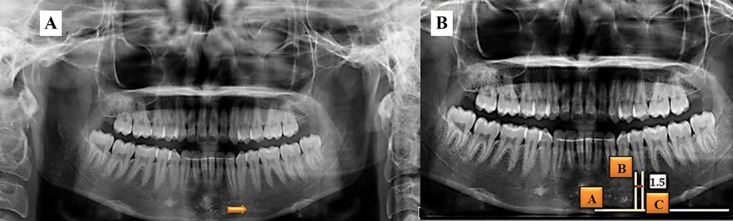
A, Presence of anterior loop on the left side in panoramic radiography. B, Length of anterior loop is measured by (A) lower mandibular cortex as the plane of reference. (B) Line perpendicular to the line passing through the most mesial point of anterior loop of mental nerve. (C) Line was drawn perpendicular to the line passing through the mesial border of mental foramen. The length is calculated by measuring the distance between reference point B and C.
Measurement of anterior extension performed on cone beam computed tomography was done by measuring the horizontal distance between the anterior border of mental foramen and the anterior border of the loop. The pattern of the anterior loop was studied based on the classification given by Solar et al (Fig. 2 and Fig. 3).10 All the measurements were observed by two independent observers.
Figure 2.
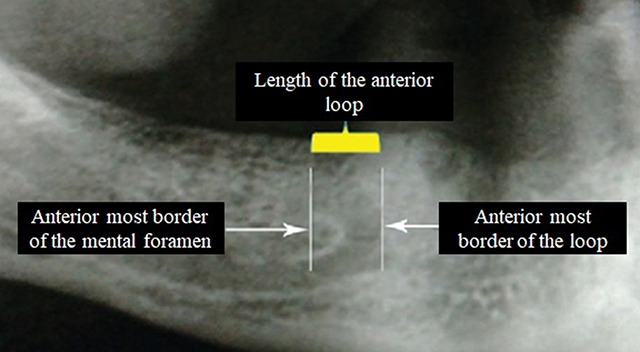
Anterior loop of inferior alveolar nerve.
Figure 3.

A, Presence of anterior loop on CBCT. B, Anterior loop traced. C, D, E: Patterns of the anterior loop on reconstructed panoramic radiography and D volumetric mode.
All the data obtained were added to Microsoft Excel (2010 version of software) and subjected to statistical analysis using SPSS software 20.0. A Z test for two sample means was used to compare the length of the anterior loop of the inferior alveolar nerve by panoramic radiography and CBCT in male patients and female patients and compare between the right and left sides. The prevalence of anterior loop by panoramic radiography and CBCT in male patients and female patients were assessed by the chi-square test. A chi-square test was applied to compare the frequency of anterior loop between different age groups in panoramic radiography and CBCT. Intraclass correlation coefficient was used to determine the interobserver agreement.
Results
In this study, there was excellent reliability for intraobserver and interobserver performances because the intraclass correlation coefficient was found to be ranging from 0.83 to 0.96. Prevalence length and pattern of the anterior loop of the inferior alveolar nerve were assessed and measured. Data collected were coded in an Excel sheet and analyzed. Percentage, mean, standard deviation, Z test, and chi-square were used to analyze the data.
The prevalence of the anterior loop for both sexes was analyzed by panoramic radiography and CBCT. Both sexes showed a higher prevalence on the left side. Because the P-value is <0.05, there is a statistically significant difference in the prevalence of loop when assessed by panoramic radiography and CBCT both in male patients and female patients (Table 1).
TABLE 1.
Prevalence of anterior loop on panoramic radiography and CBCT
| Gender | Group | Visibility | Not visible | Visible | Total | Chi-square | Chi-square with yates correction | P | ||
| N | % | N | % | |||||||
| Male | Right | CBCT | 23 | 30 | 52 | 69 | 75 | 18.05 | 16.69 | .001* |
| Panoramic | 49 | 65 | 26 | 34 | 75 | |||||
| Left | CBCT | 21 | 28 | 54 | 72 | 75 | 25.64 | 24.01 | .001* | |
| Panoramic | 52 | 69 | 23 | 30 | 75 | |||||
| Female | Right | CBCT | 20 | 26 | 55 | 73 | 75 | 25.69 | 24.06 | .001* |
| Panoramic | 51 | 68 | 24 | 32 | 75 | |||||
| Left | CBCT | 14 | 18 | 61 | 81 | 75 | 31.78 | 29.93 | .001* | |
| Panoramic | 48 | 64 | 27 | 36 | 75 | |||||
Since the P value is less than .001, there is statistically significant difference both the imaging modalities while comparing the prevalence with respect to sides and gender.
The mean length of the loop for male patients and female patients by panoramic radiography and CBCT were assessed. Both sexes showed a longer loop on the left side which was found to be statistically significant (P<.05) while comparing the mean length of the loop by panoramic imaging and CBCT in both sexes (Table 2).
TABLE 2.
Comparison of length of anterior loop by panoramic radiography and cone beam computed tomography
| Gender | Side | Group | N | Mean (mm) | SD | Z | P |
| Male | Right | CBCT | 52 | 1.20 | 0.10 | 50.781 | <.001* |
| Panoramic | 52 | 0.10 | 0.12 | ||||
| Left | CBCT | 54 | 1.23 | 0.12 | 49.36 | <.001* | |
| Panoramic | 54 | 0.09 | 0.12 | ||||
| Female | Right | CBCT | 55 | 1.18 | 0.09 | 50.19 | <.001* |
| Panoramic | 55 | 0.11 | 0.13 | ||||
| Left | CBCT | 61 | 1.22 | 0.11 | 51.37 | <.001* | |
| Panoramic | 61 | 0.10 | 0.13 |
Since the P value is less than .001, there is statistically significant difference both the imaging modalities while comparing the length of the loop with respect to sides and gender.
While evaluating the pattern of the loop, the Type III pattern was seen more in male patients (68%), followed by the Type I pattern (19%) and the least common was Type II (13%). On contrary, in female patients, Type I was more frequently seen (61%), followed by Type III (29%), and least seen was Type II (10%).
While comparing the frequency of anterior loop between different age groups between panoramic radiography and CBCT, Group 1 age group showed a greater prevalence of anterior loop followed by group 2 and least in Group 3. Because the P-value was <0.05, there was a statistically significant difference between the three age groups for the prevalence of loop on both the imaging modalities (Table 3).
Table 3.
Comparison of frequency of anterior loop of inferior alveolar nerve between different age groups in panoramic radiography and cone beam computed tomography
| Group | Visibility | Age group | Total | Chi-square | P | |||||
| 20–35 | % | 36–50 | % | 51–65 | % | |||||
| Right | CBCT | 47 | 44 | 39 | 36 | 21 | 20 | 107 | 6.64 | .03 |
| Panoramic | 33 | 66 | 11 | 22 | 6 | 12 | 50 | |||
| Left | CBCT | 49 | 43 | 40 | 35 | 26 | 23 | 115 | 12.09 | .002 |
| Panoramic | 36 | 72 | 9 | 18 | 5 | 1 | 50 | |||
Since the P value is greater than .05, there is no statistical significant difference between both the imaging modalities while comparing the frequency of the loop with respect to age groups and sides.
Discussion
Dentists face limitations in treatments related to mandible because of difficulty in identifying the course of the inferior alveolar nerve, location or anatomical variations of the mandibular foramen, mandibular canal, and mental foramen.11 A dental implant placement, endodontic procedures are the upcoming treatment modalities as patients are more focused on preserving their teeth. Accidental injury to the inferior alveolar nerve can cause neurosensory disturbances and hemorrhagic complications.
In this study, two imaging modalities were considered to assess the loop with respect to age and sex, and the values were then compared. In the literature, widely differing ranges are provided for the frequency of the anterior loop. In panoramic studies, the prevalence varied from 6.26% to 57%. In CBCT studies, the range is 49%–83%.12-16
300 mandibular canal and mental foramen were evaluated, and an anterior loop was detected in 69% by CBCT on the right side and 72% on the left while 34% by panoramic radiography on the right side and 30% on the left side in male patients. More than half (52%) of the anterior loop was not detected in panoramic radiography. In our study, female patients had higher prevalence of anterior loop (81%). A similar study was conducted by Parnia et al, which reported the highest prevalence of the anterior loop. This anatomical landmark was observed in 84% of 96 CBCT examinations with a mean length of 3.54 mm ± 1.41. Luci et al had similar prevalence results of 85.2%. These frequencies were higher than the findings of our study.17
A comparable study was conducted by Aleksandar et al (2015) where the mental loop was identified in 36% of PR and 48.8% of CBCT.5 Couto-Filho et al (2015) identified the frequencies of AL through PR and CBCT. In PR, the loop was identified in 42.6% of cases. By contrast, the loop was detected in 29.8% of the samples using CBCT. They concluded that PR led to false-positive diagnostics of the loop.3 The frequencies of identifying the anterior loop in the studies by Arzouman et al, Kuzmanovic et al, Jacobs et al, Yosue, and Brooks were found as 12%, 27%, 11%, and 21%, respectively.5
In this study, the mean length of the loop by CBCT in male patients and female patients were higher on the left side 1.23 mm and 1.22 mm, respectively. The mean length of Luci et al coincided with our study (1.46 ± 1.25 mm). Apostolakis and Brown evaluated 93 CBCT, and the mean length was 0.89 mm ranging from 0 to 5.7 mm.17 Shi Kang Wong et al (2018) studied the Malaysian population, and the loop length ranged with a mean length of 3.69 ± 1.75 mm on left side and 3.85 ±1.73 mm on right side.18 Moghaddam MR et al (2017) and Antoinette et al (2021) found mean anterior loop length was 2.77 ± 1.56 and ranged between 0.87 ± 1.81 and 7.25 ± 2.02 mm, respectively.19,20 Jae-Young Kim reported in their study that a 4–6 mm safety margin from the anterior border of mental foramen has been recommended.21 The literature reveals the longest length of anterior loop was around 11 mm.19
While evaluating the loop pattern, a similar study performed by Osama et al (2020) where Type I was frequently and type III least seen in both sexes.22 Om Prakash et al (2018) found Type III pattern in 50% of the study population. The result was in agreement with the study conducted by Demir et al (2015) in Turkish population where type I was seen in 29% and Type II in 21% of their study population.23 This variation is attributed to anatomical variations of different study populations.
In our study, we observed a trend toward decreasing frequency of anterior loop of inferior alveolar nerve with increasing age because the samples in the study were equally divided in each age group. Similar findings were observed in a study performed by Ramya Katyayani et al (2019)21 and Ngeow et al (2009)24 where they noted the prevalence of anterior loop decreased as the age progresses.
On assessing the sex influence in our study, female patients had more prevalence of anterior loop while the length of anterior loop was more for male patients. A differing result was seen in the study by Smriti et al (2019)25 and Nascimento et al (2016) where they found the loop significantly more prevalent in male patients.26
Conclusion
Radiographs have always been the primary source of diagnostic information on the oral and maxillofacial complex. In our study, there was significantly high difference between panoramic radiography and CBCT in assessing the loop which emphasizes the limitation of panoramic radiographs.
The use of CBCT holds the promise of overcoming these hurdles. A minimum of 3-mm safety margin should be maintained because we found the mean length of the anterior loop to be 1.23 mm in male patients and 1.22 mm in female patients.
This study is one among the few studies present in the literature focusing on the various patterns of anterior loop and its prevalence among the South Indian population, and we found Type I was the most common variant in female patients and Type III in male patients. There are numerous studies performed in Indian population that have evaluated the prevalence of anterior loop but have failed to compare the variations on right and left sides and also the variations with regard to age and sex.
Further studies with larger samples are required by focusing on the potential of CBCT in accurately assessing the anterior loop and its variations and also to enlighten the safety margins to be followed before planning a procedure in the interforaminal region.
REFERENCES
- [1].Velasco-Torres M, Padial-Molina M, Avila-Ortiz G, García-Delgado R, Catena A, Galindo-Moreno P. Inferior alveolar nerve trajectory, mental foramen location and incidence of mental nerve anterior loop. Med Oral Patol Oral Cir Bucal. 2017;22(5):e630-e635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Yu SK, Kim S, Kang SG, et al. Morphological assessment of the anterior loop of the mandibular canal in Koreans. Anat Cell Biol. 2015;48: 75-80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Couto-Filho CE, DE Moraes PH, Alonso M, Haiter-Neto F, Olate S. Accuracy in the diagnosis of the mental nerve loop. A comparative study between panoramic radiography and cone beam computed tomography. Int J Morphol. 2015;33(1):327-.332. [DOI] [PubMed] [Google Scholar]
- [4].Jonasson G, Rythén M. Alveolar bone loss in osteoporosis: a loaded and cellular affair? Clin Cosmet Investig Dentistry. 2016;8:95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Vujanovic-Eskenazi A, Valero-James JM, Sánchez-Garcés MA, Gay-Escoda C. A retrospective radiographic evaluation of the anterior loop of the mental nerve: comparison between panoramic radiography and cone beam computerized tomography. Med Oral Patol Oral Cir Bucal. 2015; 20 (2):239-245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Wyatt WM. Accessory mandibular canal: literature review and presentation of an additional variant. Quintessence Int. 1996; 27(2):111-113. [PubMed] [Google Scholar]
- [7].Venkatesh E, Elluru SV. Cone beam computed tomography: basics and applications in dentistry. J Istanbul Univ Fac Dentistry. 2017;51(3 Suppl 1):102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Kuzmanovic DV, Payne AG, Kieser JA, Dias GJ. Anterior loop of the mental nerve: a morphological and radiographic study. Clin Oral Implants Res. 2003;14:464–471. [DOI] [PubMed] [Google Scholar]
- [9].De Brito AC, Nejaim Y, De Freitas DQ, de Oliveira Santos C. Panoramic radiographs underestimate extensions of the anterior loop and mandibular incisive canal. Imaging Sci Dent. 2016; 46(3):159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Alyami OS, Alotaibi MS, Koppolu P, et al. Anterior loop of the mental nerve in Saudi sample in Riyadh, KSA. A cone beam computerized tomography study. Saudi Dent J. 2021; 33(3):124-130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Chen JC, Lin LM, Geist JR, Chen JY, Chen CH, Chen YK. A retrospective comparison of the location and diameter of the inferior alveolar canal at the mental foramen and length of the anterior loop between American and Taiwanese cohorts using CBCT. Surg Radiologic Anat. 2013; 35(1):11-18. [DOI] [PubMed] [Google Scholar]
- [12].Benninger B, Miller D, Maharathi A, Carter W. Dental implant placement investigation: is the anterior loop of the mental nerve clinically relevant? J Oral Maxillofac Surg. 2011; 69:182-185. [DOI] [PubMed] [Google Scholar]
- [13].Neiva RF, Gapski R, Wang HL. Morphometric analysis of implant-related anatomy in Caucasian skulls. J Periodontol. 2004;75:1061-1067. [DOI] [PubMed] [Google Scholar]
- [14].Arzouman MJ, Otis L, Kipnis V, Levine D. Observations of the anterior loop of the inferior alveolar canal. Int J Oral Maxillofac Implants. 1993;8:295-300. [PubMed] [Google Scholar]
- [15].Apostolakis D, Brown JE. The anterior loop of the inferior alveolar nerve: prevalence, measurement of its length and a recommendation for interforaminal implant installation based on cone beam CT imaging. Clin Oral Implants Res. 2012;23:1022-1030. [DOI] [PubMed] [Google Scholar]
- [16].Parnia F, Moslehifard E, Hafezeqoran A, Mahboub F, Mojaver-Kahnamoui H. Characteristics of anatomical landmarks in the mandibular interforaminal region: a cone-beam computed tomography study. Med Oral Patol Oral Cir Bucal. 2012;17:420-425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Prados-Frutos JC, Salinas-Goodier C, Manchón Á, Rojo R. Anterior loop of the mental nerve, mental foramen and incisive nerve emergency: tridimensional assessment and surgical applications. Surg Radiol Anat. 2017;39(2):169-175. [DOI] [PubMed] [Google Scholar]
- [18].Wong SK, Patil PG. Measuring anterior loop length of the inferior alveolar nerve to estimate safe zone in implant planning: a CBCT study in a Malaysian population. J Prosthet Dent. 2018;120(2):210-213. [DOI] [PubMed] [Google Scholar]
- [19].Moghddam MR, Davoudmanesh Z, Azizi N, Rakhshan V, Shariati M. Prevalence and length of the anterior loop of the inferior alveolar nerve in Iranians. J Oral Implantol. 2017;43(5):333-336. [DOI] [PubMed] [Google Scholar]
- [20].Pelé A, Berry PA, Evanno C, Jordana F. Evaluation of mental foramen with cone beam computed tomography: a systematic review of literature. Radiol Res Pract. 2021;2021;8897275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Kim JY, Han MD, Jeon KJ, Huh JK, Park KH. Three-dimensional assessment of the anterior and inferior loop of the inferior alveolar nerve using computed tomography images in patients with and without mandibular asymmetry. BMC Oral Health. 2021;21(1):1-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Kastala RK, David CM, Jayapal N. Momentousness of the mental loop: a comparative study. Contemp Clin Dent. 2019;10(1):86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Prakash O, Srivastava PK, Jyoti B, Mushtaq R, Vyas T, Usha P. Radiographic evaluation of anterior loop of inferior alveolar nerve: a cone-beam computer tomography study. Niger J Surg. 2018;24(2):90-94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Ngeow WC, Dionysius DD, Ishak H, Nambiar P. A radiographic study on the visualization of the anterior loop in dentate subjects of different age groups. J Oral Sci. 2009;51:231-237. [DOI] [PubMed] [Google Scholar]
- [25].Sinha S, Kandula S, Sangamesh NC, Rout P, Mishra S, Bajoria AA. Assessment of the anterior loop of the mandibular canal using cone-beam computed tomography in Eastern India: a record-based study. J Int Soc Prev Community Dent. 2019; 9(3):290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].do Nascimento EH, Dos Anjos Pontual ML, Dos Anjos Pontual A, et al. Assessment of the anterior loop of the mandibular canal: a study using cone-beam computed tomography. Imaging Sci Dent. 2016;46(2):69-75. [DOI] [PMC free article] [PubMed] [Google Scholar]