

Abstract
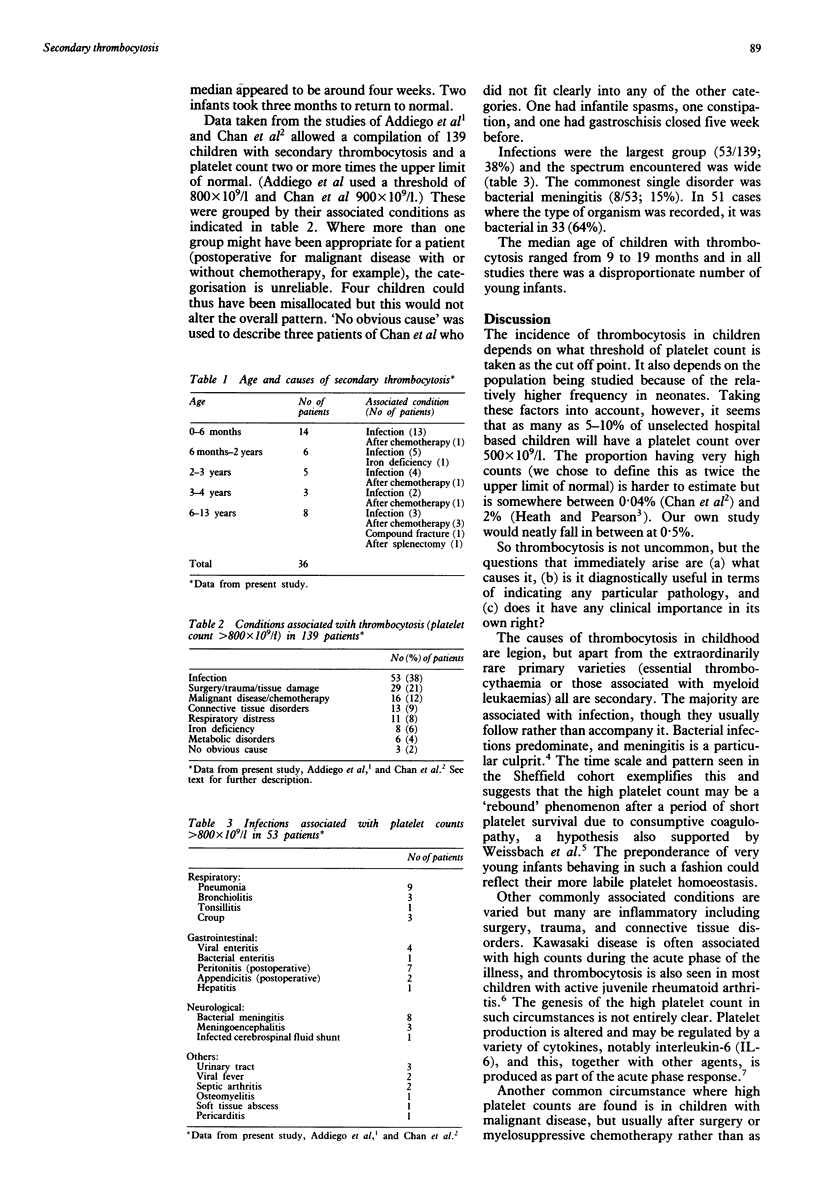
To estimate the incidence and causes of secondary thrombocytosis in children, a 12 month study of all patients attending a children's hospital and discovered to have a platelet count over two times the upper normal limit (> 800 x 10(9)/l) was undertaken. Data so obtained were analysed both separately and together with those from two previous studies to gain as broad a perspective as possible. Of 7916 children who had platelet counts during the study period, 36 (0.5%) produced a value > 800 x 10(9)/l; there were 19 boys and 17 girls. There was a preponderance of young infants (median age 13 months). Twenty seven of the 36 had some sort of associated infection, bacterial in 18 and viral in nine. The other nine were either recovering from anti-neoplastic chemotherapy (n = 6), were post-operative (n = 2), or simply iron deficient (n = 1). Combining these patients with those described in previous studies allowed a review of 139 unselected children with very high platelet counts. Fifty three (38%) had infections, 29 (20%) had traumatic or surgical tissue damage, 16 (11%) had malignant disease undergoing chemotherapy or surgery, and 13 (9%) had connective tissue or autoimmune disorders. Secondary thrombocytosis is not rare and is most frequently seen in very young infants after infection. It can arise in a wide variety of other circumstances including rebound from myelosuppression, iron lack, or as part of an acute phase response. It is clinically unimportant in terms of morbidity and requires no treatment other than that for the primary condition.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Addiego J. E., Jr, Mentzer W. C., Jr, Dallman P. R. Thrombocytosis in infants and children. J Pediatr. 1974 Dec;85(6):805–807. doi: 10.1016/s0022-3476(74)80345-8. [DOI] [PubMed] [Google Scholar]
- Chan K. W., Kaikov Y., Wadsworth L. D. Thrombocytosis in childhood: a survey of 94 patients. Pediatrics. 1989 Dec;84(6):1064–1067. [PubMed] [Google Scholar]
- Davis W. M., Ross A. O. Thrombocytosis and thrombocythemia: the laboratory and clinical significance of an elevated platelet count. Am J Clin Pathol. 1973 Feb;59(2):243–247. doi: 10.1093/ajcp/59.2.243. [DOI] [PubMed] [Google Scholar]
- Frenkel E. P. The clinical spectrum of thrombocytosis and thrombocythemia. Am J Med Sci. 1991 Jan;301(1):69–80. doi: 10.1097/00000441-199101000-00013. [DOI] [PubMed] [Google Scholar]
- GROSS S., KEEFER V., NEWMAN A. J. THE PLATELETS IN IRON-DEFICIENCY ANEMIA. I. THE RESPONSE TO ORAL AND PARENTERAL IRON. Pediatrics. 1964 Sep;34:315–323. [PubMed] [Google Scholar]
- Heath H. W., Pearson H. A. Thrombocytosis in pediatric outpatients. J Pediatr. 1989 May;114(5):805–807. doi: 10.1016/s0022-3476(89)80141-6. [DOI] [PubMed] [Google Scholar]
- Thomas G. A., O'Brien R. T. Thrombocytosis in children with Hemophilus influenzae meningitis. Clin Pediatr (Phila) 1986 Dec;25(12):610–611. doi: 10.1177/000992288602501204. [DOI] [PubMed] [Google Scholar]