

Abstract
Background:
Currently, some trauma-informed education practices use “ACE scores,” a number that represents the sum of endorsed items from a survey derived from the Adverse Childhood Experiences (ACEs) study in 1998. We caution that the survey provides limited information within education, and such scores have limited utility for designing and delivering individualized intervention to support students who have experienced adversity.
Objective:
We sought to illustrate why ACEs are not well-suited for use in trauma-informed education, provide definitions for adversity-related terms from which a broader and common understanding of adversity can stem, and provide recommendations for integration of adversity-informed approaches to the educational context.
Methods:
We compiled definitions of adversity-related constructs and made recommendations based on review of relevant research from the fields of psychology and education.
Results:
Rather than tailoring educational practices to specific children based on the “traumatic” events they experience, we recommend educators focus their efforts on building supportive classrooms geared towards supporting students with best practices drawn from the Science of Learning, and with the understanding that early adversity can influence heterogeneous trajectories in student development and behavior. In addition, further research on educational practices, including the use of a shared language for describing and defining adversity-related experiences, are the concrete steps needed to better support a goal of adversity-informed education.
Keywords: education, adversity, ACEs, trauma-informed
Introduction
The inclusion of the descriptor or prefix “trauma-informed” is now found in a number of contexts. This prefix has been widely applied to a range of education-related terms (e.g., teaching, education, educators, schools, school personnel). “Trauma-informed teaching,” for example, has increased in usage, with Google Scholar reporting four published papers that included this phrase from inception to 2012 and annual growth resulting in more than 450 search results in 2022 (Figure 1). Broadly, trauma-informed school personnel have been described as having an “understanding of how trauma affects student learning and behavior in the school environment” (Overstreet & Chafouleas, 2016, p. 2) and being able to support their students with that understanding (Brown, 2021; Scott et al., 2021). Although the prefix “trauma-informed” is used by scholars and practitioners, resources for educators relevant to these ideas include a wide range of childhood events that may be adverse, but do not necessarily meet the definition of trauma (according to the Diagnostic and Statistical Manual of Mental Disorders [DSM-5]; American Psychiatric Association, 2013; Thomas et al., 2019). Indeed, the term “adversity-informed teaching” would more accurately capture the stated sentiment of this framework for understanding and responding to the impact of adverse experiences on student functioning. Yet, if the goal is to change behaviors with an “understanding” of trauma and/or adversity, it appears to be important to know what experiences are and are not included within this category.
Figure 1. Results by year on Google Scholar of “trauma-informed teaching.”.
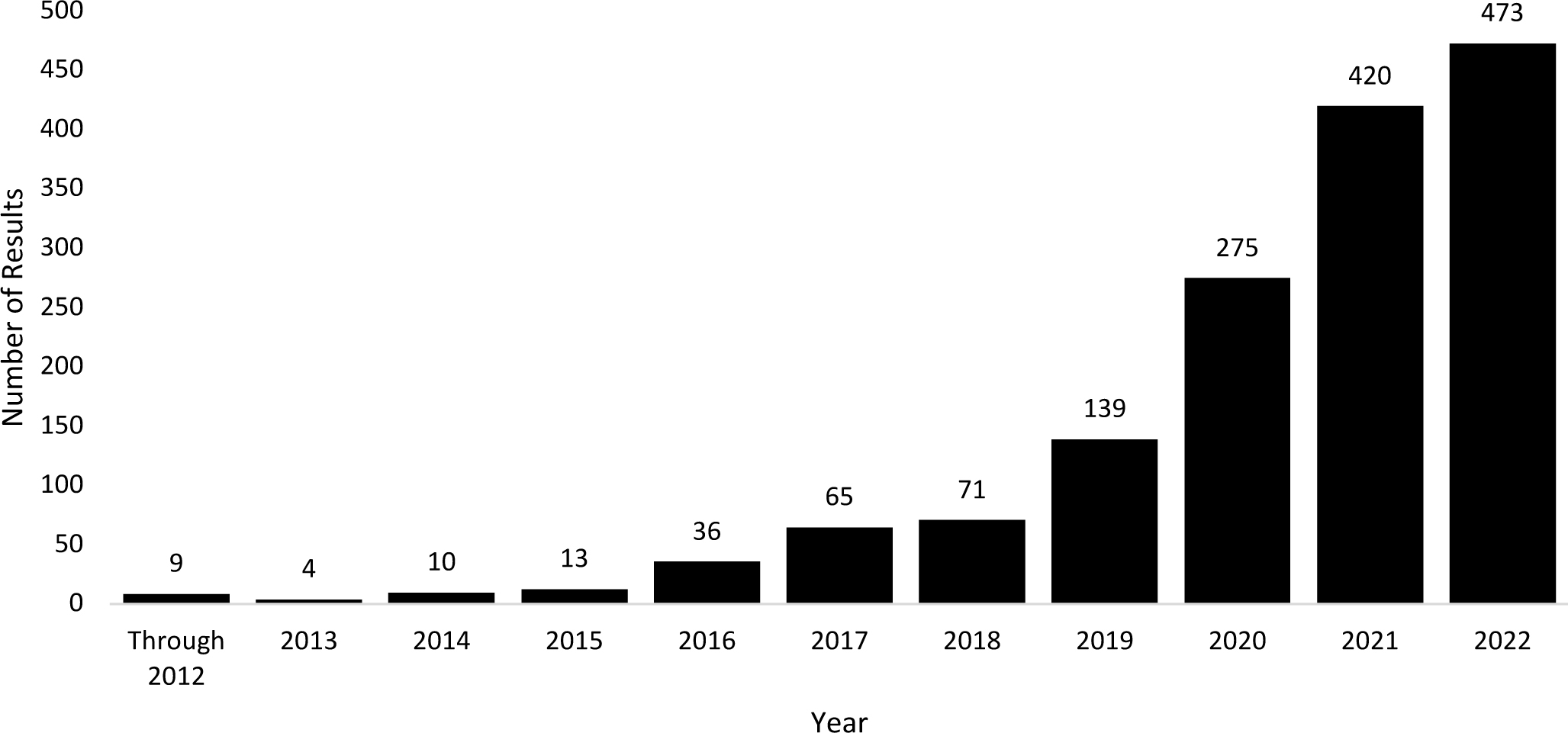
Note: As of February 2, 2023, on Google Scholar, the term “trauma-informed teaching,” excluding appearance in citations, produces nine results through the year 2012. It then produces four more results in only the year 2013, written as (2013–2013) on Google Scholar. The same process was used for the remaining years.
Currently, some trauma-informed education practices use “ACE scores” (Portell, 2019), a number that represents the sum of a set of survey items derived from the Adverse Childhood Experiences (ACEs) study (Felitti et al., 1998). ACE scores are meant to represent total childhood adversity exposure. Though researchers have studied the long-term influence of adversity exposure in children (e.g., developmental psychopathology), the seminal ACE findings played an important role in sparking a wider-scale interest in childhood adversity, including from schools (Felitti, 2019). In a 20-year reflection on the ACE study, Felitti stated that following the study, “surprisingly, strong interest and engagement first appeared in school systems, not in medical settings” (2019, p. 789). However, the survey is limited (McLennan et al., 2020) and the score is not informative for individualized intervention (Anda et al., 2020), meaning that the survey’s important place in sparking interest now risks becoming a liability in charting a future path that supports children. In order to have a deep and broad understanding of adversity, educator knowledge should extend beyond the seminal ACE findings—and, we contend—trauma-informed education practices should not include a discussion or measurement of students’ ACE scores. The time to invoke these changes is now—there is a critical opportunity to ground educator knowledge in scientific literature on trauma-related concepts and relevant classroom practices.
Trauma-informed education requires an agreed-upon understanding of adversity-related experiences to support teachers in becoming more critical consumers of scientific literature, better advocates for students, and more able to successfully translate findings to pedagogical practice. Specifically, we advocate deemphasizing the use of “ACE scores” and instead consider a broader view of adversity. Additionally, we encourage the continued use of trauma-informed education practices that will be beneficial for providing supportive classrooms. Specifically, regular use of socioemotional learning practices in the classroom benefits all students (Schonert-Reichl, 2017), and may be especially beneficial for students who have disproportionately experienced early adversity (Scott et al., 2021).
Section 1: Limitations of the ACEs Questionnaire
The ACEs study included two waves of data collection (Dube et al., 2001; Felitti et al., 1998). The seminal ACE findings were published with data from only the first wave, which included 8,506 survey respondents who completed a standardized medical evaluation at Kaiser Permanente’s San Diego Health Appraisal Clinic, from August to November 1995 or January to March 1996 (Felitti et al., 1998). Participants were 52% female, had a mean age of 56.1 years old (range 19–92), and predominantly identified as White (79%) (Felitti et al., 1998). All participants were assigned a score of childhood adversity from 0 (unexposed) to 7 (exposed to all categories), using a 17-question survey the researchers designed with seven categories of early experience. Results indicated group-level associations between the total scores (from 0 to 4 or more) of retrospective reports of discrete adverse experiences in childhood and adult health outcomes, including health risk behaviors and specific disease incidence. Participants with a score of four or more ACEs compared to zero were about twice as likely on average to have a number of disease conditions.
1.1: History
Felitti is a physician who was treating obesity when one of his patients, who had lost and then re-gained over 100 pounds, disclosed that she had been sexually abused as a child (Felitti, 2019). Several weeks after this report, there was another sexual abuse case which led Felitti and his colleagues to interview their incoming patients about sexual abuse (Felitti, 2019). They found that 55% of 286 patients in the obesity program acknowledged childhood sexual abuse (Felitti, 2019). These findings and conversations with other doctors and scientists inspired Felitti to conduct the ACEs study (Felitti, 2019).
To create the survey for the seminal ACEs study, Felitti et al. (1998) adapted questions on psychological abuse, physical abuse, and violence against the participant’s mother from the Conflicts Tactics Scale (Straus et al., 1990), contact sexual abuse from the Wyatt (Wyatt, 1985), and exposure to drug or alcohol use from the National Health Interview Survey (National Center for Health Statistics, 1991). The ACEs study sent surveys out in two waves to possible respondents. The seminal paper only used data from the first wave. The survey from the second wave of data collection contained additional questions on emotional and physical neglect (Anda et al., 2006, 2009; Dube et al., 2001) adapted from the Childhood Trauma Questionnaire (Bernstein et al., 1994). Psychometric assessments were not conducted on the ACEs questionnaire at the time (McLennan et al., 2020). Furthermore, questions on the survey asked for a range of information that was not actually used in calculating participants’ ACE scores, such as the onset and offset of some experiences.
Following the study, Felitti et al. (1998) developed a one-page, 10-question version of the ACEs survey to “get people involved” (V. J. Felitti, personal communication, June 18, 2022). This 10-question survey derived from the original ACEs questionnaire grew beyond the population measure used in this study into a tool in trauma-informed care (Portell, 2019). Although slightly different versions of the 10-question survey exist (see Finkelhor et al., 2015; Starecheski, 2015; Watson, 2019; Zarse et al., 2019 for examples of the survey with slight differences and in different platforms) the core questions seem to be based on the categories defined in the second wave (Anda et al., 2006, 2009; Dube et al., 2001). Additional ACEs surveys have been derived (i.e., the CDC adopted an 11-item version of the ACEs questionnaire that elicited yes/no responses in their Behavioral Risk Factor Surveillance System questionnaire in 2009, which differs from the 10-question version in a number of ways), however, the 10-question version is the most commonly used ACE score (Struck et al., 2021). Despite it appearing in the literature as early as 2013 (Corbin et al., 2013), there is not a publication that formally introduces this common 10-question version of the survey (V. J. Felitti, personal communication, June 18, 2022).
The 10-question ACEs questionnaire collapsed items by category from the survey used in the second wave of data collection for the ACEs study (Anda et al., 2006, 2009; Dube et al., 2001), eliminates the preambles from the original ACEs survey (Felitti et al., 1998), and binarizes answers (i.e., yes/no; McLennan et al., 2020). For example, the original ACEs survey states “Sometimes parents or other adults hurt children. While you were growing up, that is, during your first 18 years of life, how often did a parent, step-parent, or adult living in your home:” and then asks “Swear at, insult you, or put you down?” followed by questions including “Act in a way that made you afraid that you might be physically hurt?” Participants received a score of 1 for this category of psychological abuse if they answered often or very often to either of these questions. In contrast, the 10-question survey only contains the preamble “Did a parent or other adult in the household often or very often…” and puts the word “or” between these items, just asking for one yes/no response. Respondents in wave 1 of the ACEs study received an ACE score of 0 to 7. From the 10-question survey, respondents receive an ACE score of 0 to 10 because an additional question on emotional neglect and an additional question on physical neglect were similarly derived and collapsed from wave 2 of the ACEs survey (Anda et al., 2006, 2009; Dube et al., 2001), and the question on parental separation or divorce was asked in the original study, but not counted as an ACE category at the time (Felitti et al., 1998; Finkelhor et al., 2015; Zarse et al., 2019).
In the 20 years following the study’s publication (from 1998 to 2018), 789 articles appeared in peer-reviewed journals (Struck et al., 2021). The number of bills introduced that directly reference ACEs has increased every year for the past two decades, totaling 425 pieces of legislation by mid-August 2021 (Crowley et al., 2022). The influence has also reached classrooms, as reference to these findings and the 10-question survey have influenced teacher training and pedagogy (Portell, 2019; Scott et al., 2021). As aforementioned, in a 20-year reflection on the ACE study, Felitti stated that following the study, “surprisingly, strong interest and engagement first appeared in school systems, not in medical settings” (2019, p. 789).
1.2: Limitations
Despite its role in increasing awareness of the association between adversity in childhood and later health outcomes, the ACEs questionnaire has limited scientific or practical utility, particularly in the potential to guide prevention and intervention. While some research groups have proposed changes to improve or adapt the questionnaire (Bernard et al., 2021; Briggs et al., 2021; Finkelhor et al., 2015; Karatekin & Hill, 2019; McKelvey et al., 2017), others advocate abandoning the measure (McLennan et al., 2020). Briefly, the ACEs survey: (1) is not well-able to capture children’s actual experiences and instead often includes exposures that conflate social address with experience (i.e., two people who indicate on the survey that a household member went to prison may have had very different experiences related to that event), (2) includes a select and non-theoretically determined set of items, (3) uses cumulative scoring that undervalues the potential for specificity in the influence of some types of adversity. We detail each of these points below.
1.3: Survey Items
If the goal of the assessment is to capture the variation of experiences relevant to adversity, it must do so in a comprehensive manner. Yet, the 10-item ACEs questionnaire captures information that is not well-suited for these goals.
The questions on the widely-used 10-item survey are not comprehensive to all forms of adversity (McLennan et al., 2020). As noted by others (Bernard et al., 2021; Briggs et al., 2021; Finkelhor et al., 2015; Karatekin & Hill, 2019; McLennan et al., 2020), many relevant forms of adversity are not captured by this tool (e.g., community violence exposure, food insecurity, peer victimization, peer isolation/rejection, socioeconomic status, separation from family members, and forms of discrimination like racial discrimination). Bernard et al. (2021) recommended that racism be considered an ACE exposure risk factor, a discrete ACE category, and a determinant of post-ACE mental health outcomes. In studies using expanded ACE questionnaires with added questions on topics including community violence, racial discrimination, and foster care placement, racial and ethnic minority adults and youth endorsed more ACEs (Bernard et al., 2021; Cronholm et al., 2015; Maguire-Jack et al., 2020). If the survey is lacking in comprehensiveness for relevant forms of adversity, some adverse experiences are not being accounted for and, if the score is used as an indicator for intervention, this underestimation means that some children may not receive necessary support.
Additionally, to understand variance in outcomes following adverse experiences, it may be useful to assess the presence of protective factors (Anda et al., 2020). Resilience following adversity is common and can be explained in part by a combination of internal and external factors (Eaton et al., 2022; Humphreys et al., 2020). However, the survey does not ask about the availability of such buffers that promote resilience to adversity, such as secure attachment relationships and supportive adults (e.g., teachers, religious group members, neighbors, and extended family; Gartland et al., 2019; Masten, 2001).
1.4: Scoring
ACE scores are computed by summing the number of endorsed events to obtain a total. Notably, the scores obtained do not take into account: (1) when the event occurred, (2) the severity of the experience, (3) the “dimension” of adversity experiences. The onset and offset of experiences may be important for understanding whether events occurred during important periods in development (e.g., sensitive periods). Furthermore, the measure does not capture the severity of experiences—each item is assigned either 0 or 1. This means that a single incident of spanking that left a mark is given the same weight as a parent beating their child to physical injury daily, despite differences in likely impact (though some participants might not endorse the first experience as physical abuse, creating additional difficulties from a measurement perspective). Finally, whether experiences are postulated to affect the human body in a similar manner (e.g., experiences of threat vs. experiences of deprivation) may be relevant for parsing cause–effect relationships of adversity (McLaughlin et al., 2021). ACE scores notably lack a clear mapping onto experience in these ways.
1.5: Individual use
Despite efforts that advocate for the use of ACE scores in individual screening (Purewal et al., 2016), Anda et al. (2020) note that the survey is “not suitable for screening individuals and assigning risk for use in decision making about need for services or treatment” (p. 293). In a study on two cohorts from birth to adulthood, researchers found that ACE scores poorly predicted an individual’s risk of later health problems, despite forecasting average group differences in health (Baldwin et al., 2021). In other words, while the survey indicated associations relevant to risk at a group level, these associations are not transferable to use at the individual level. More plainly, not only might two individuals with non-overlapping experiences receive the same ACE score, but also those with the same experiences differ widely in their outcomes. This is explained by a combination of differences in the variation in the severity, timing, and dimensions of adverse experiences, in the protective factors available to buffer against adversity (Humphreys et al., 2022), and individual vulnerability at the genetic level (Ellis & Boyce, 2008). Consequently, ACE scores should not be “used to infer knowledge about individual risk for health outcomes” (Anda et al., 2020, p. 294). Distinct interventions are relevant based on the types of adverse experiences (see Guyon-Harris et al., 2021), and using a nonspecific ACE score would provide no useful information to practitioners seeking to support children.
1.6: Recommendations
Given the limitations of the 10-question ACEs survey, we strongly advise against its use in decision-making regarding individualized plans for trauma-informed education. Educators should consider a broader view of adversity, rather than using ACE scores in their practice. Additionally, we encourage specificity when using the term “ACEs.” This term is sometimes used to refer to the 1998 study led by Felitti, sometimes used to indicate scores from the 10-item survey (Zarse et al., 2019), or sometimes used interchangeably with the construct of early adversity. Given the multiple uses, we encourage reserving “ACEs” for the ACE study and questionnaire and “early adversity” for discussions of the broader construct.
Section 2: Important Terms for Conceptualizing Childhood Adversity
McLaughlin (2016) called for the use of agreed-upon definitions for terms related to childhood adversity and a broad view of adversity can be rooted in the following terms and concepts rather than ACE scores. In Table 1, we provide a list of these terms and guidance for usage. Common definitions allow for findings to be synthesized across studies and translated into meaningful progress in the field, particularly education. Shared definitions also benefit practitioners building from this research. This section provides options for creating a common language among researchers and practitioners to establish a shared understanding of adversity-related constructs. The broader goal of this effort is to improve translation from research to practice.
Table 1.
Definitions of Adversity-Related Terms
| Terms | Definitions | Source |
|---|---|---|
| Early Experience | Experience-expectant is the idea that there is information to which most people are exposed at a certain time and as neural mechanisms have evolved to account for that exposure, these experiences may play a role in sensitive periods. Experience-dependent is the unique individual exposure to information that happens at varied time points. | Greenough et al. (1987) |
| Adverse Childhood Experiences | There is the Adverse Childhood Experiences Study from 1998 and the related Adverse Childhood Experiences 10-question Survey derived from the study. These are distinct from the range of childhood experiences that could be considered adverse. When people refer to ACEs it is not always clear whether they are referring to the 10-item questionnaire or the larger umbrella category. | Felitti et al. (1998) |
| Childhood Adversity | Exposure during childhood or adolescence to environmental circumstances that are likely to require significant psychological, social, or neurobiological adaptation by an average child | Frankenhuis & Amir (2022); McLaughlin (2016) |
| Threat | Exposure to harmful events or events involving the threat of harm | Sheridan & McLaughlin (2014) |
| Psychological Deprivation | Reduced opportunities for learning due to a lack of cognitive and social environmental input | Sheridan & McLaughlin (2014) |
| Harshness | External sources of morbidity-mortality, encompasses threat and deprivation and includes proximal and distal levels of developmental adaptation | Ellis et al. (2009, 2022); McLaughlin et al. (2021) |
| Unpredictability | Random variations in external sources of illness and death | Ellis et al. (2009) |
| Trauma | Exposure to actual or threatened death, serious injury, or sexual violence by experiencing it directly, witnessing it in person, learning that the event occurred to close family or friends (in the case of death the events must have been violent or accidental), or experiencing repeated or extreme exposure of adverse details of the traumatic events | American Psychiatric Association (2013) |
| Stress | Adaptation of an organism to specific circumstances that change over time | Szabo et al. (2012) |
| Allostatic Load | Wear and tear on the biological systems responsible for balancing systems in response to changes in the environment | Danese & McEwen (2012); Jensen et al. (2017) |
| Toxic Stress | The prolonged activation of the stress response without the buffer of a supportive adult | Johnson et al., (2013); Shonkoff & Garner (2012) |
| Coping | The thoughts and actions that people use to manage stressful events | Folkman & Lazarus (1986) |
| Resilience | When people recover to typical functioning or show minimal change in functioning following adversity likely due to a combination of internal and external factors | Humphreys et al. (2022) |
| Socioeconomic Status | Based on objective indicators such as income, wealth, and level of education | Diemer et al. (2013) |
| Subjective Social Status | One’s perception of their social class | Diemer et al. (2013) |
| Trauma-Informed Teaching | Trauma-informed teachers have an understanding of trauma-related concepts and are able to support their students with that understanding | Brown (2021); Scott et al. (2021) |
2.1: Defining Early Experiences, Adversity, Trauma, and Stress
Though experiences of stress and adversity have demonstrated associations with more negative child outcomes, operationalizing when an “experience” becomes “adverse” is more complex. How should researchers and practitioners make meaning of the variation that exists in types of early experiences? McLaughlin defined childhood adversity as “exposure during childhood or adolescence to environmental circumstances that are likely to require significant psychological, social, or neurobiological adaptation by an average child and that represent a deviation from the expectable environment” (2016, pp. 4–5). This definition includes three key components: (1) development stage: during childhood or adolescence, (2) response to the experience: likely requires adaptation, (3) usualness: differing from what would be expected. More recently, Frankenhuis and Amir (2022) compellingly argued that humans have historically experienced high levels of threatening experiences such as infanticide, violent conflict, and predation, as well as a lack of social, cognitive, and nutritional input. Thus, many of the hardships we call “adverse” would not be distinguished by the degree to which they were generally expected to occur in our species. Incorporating this suggestion to remove the third component of the definition, childhood adversity can be defined as exposure during childhood or adolescence to environmental circumstances that are likely to require significant psychological, social, or neurobiological adaptation by an average child. This definition removes the requirement for an individual to experience a specific response to an adversity, and rather considers that response generally expected to occur. In other words, for an experience to be considered adverse, the judgment is based on the likelihood of an average person’s reaction, rather than a specific person’s response.
This idea that individual responses differ, but one can understand how the average person may typically respond, is paralleled by the reasonably prudent person (RPP) standard in law. The RPP standard is the consideration of what most people, or a typical person, would do in the same circumstances as the person in question and is often used in law to provide jurors with an objective basis for assessing liability in certain cases including those of negligence (Alicke & Weigel, 2021). Similarly, adverse experiences can be categorized by experiences likely to require significant adaptation by an average person rather than an individual’s given response.
Scientists and practitioners have also used the terms developmental risk factors and social determinants of health to refer to experiences of childhood adversity. The definition of developmental risk factors describes experiences that can disrupt a child’s healthy neural environment, which frames the adaptations in a negative lens (Jensen et al., 2017). Similarly, the term social determinants of health implies that the experiences in question negatively impact one’s health. Although children who experience adversity have an increased risk of developing a mental health disorder, not all exposure to adversity results in negative outcomes (Ellis & Boyce, 2008; Kessler et al., 2010). Thus, not all adaptations that may take place are necessarily negative. Based on McLaughlin’s definition, childhood adversity refers to the circumstances or event, and not the specific individual adaptation that may take place.
In defining adversity, it is also important to distinguish adversity from related terms. Adversity is not the same as trauma or stress (see McLaughlin, 2016). Traumatic events are defined in the DSM-5 as exposure to actual or threatened death, serious injury, or sexual violence by experiencing it directly, witnessing it in person, learning that the event occurred to close family or friends (in the case of death the events must have been violent or accidental), or experiencing repeated or extreme exposure to adverse details of the traumatic events (American Psychiatric Association, 2013). This definition diverges from a broader set of experiences used outside of the specific mental health context. Cultural references to the word trauma have not only become more general and watered down (e.g., “My football team lost: That was traumatic”), but also more prevalent, with Google searches for the term steadily rising every year since 2003 and peaking in 2021 as of January 2022 (Pandell, 2022). For example, even “trauma-informed education” appears to be using trauma to capture a wider set of experiences that are not inherently traumatic (e.g., the Child Trauma Toolkit for Educators from The National Child Traumatic Stress Network [2017, p. 7] is a resource that lists “living in chronically chaotic environments in which housing and financial resources are not consistently available” as a situation that can be traumatic; Thomas et al., 2019). Notably, this description does not fit the definition in the DSM-5 (American Psychiatric Association, 2013). Thus, well-meaning parties are using the term “trauma” in different ways, making it more difficult for a shared definition to be established and construing the meaning of trauma across resources and groups.
Another point of discussion is clarifying what the objective experience is and what the biological consequences are that follow from that experience. Some definitions of “stress” conflate the experience and the effect. For example, as first characterized by Selye in the 1930s, stress was defined as a bodily response triggered by physical, chemical, or psychological factors/agents, which he called stressors (Szabo et al., 2012). In other words, stress is an individual biological response. Since then, different types of stress have been studied at length. Life stress is the adaptation of an organism to specific circumstances that change over time (Monroe, 2008). This definition includes the event, adaptation by the organism, and change over time. In contrast, childhood adversity only refers to the environmental aspect of stress and does not describe the individual adaptation that may (or may not) occur in response (McLaughlin, 2016).
There are a variety of terms associated with the biological effects of chronic stress. Stress activates the hypothalamic-pituitary-adrenal (HPA) axis, which leads to a release of cortisol and then briefly increases energy use, cognitive abilities, and immune reactions (McEwen, 2002). When the nervous, endocrine, and immune systems typically activated by stress experience prolonged activation, physiological abnormalities in these systems can appear, which is called allostatic load (Danese & McEwen, 2012; Jensen et al., 2017). So called “toxic stress” has been defined as the prolonged activation of the stress response without the buffer of a supportive adult (Johnson et al., 2013; Shonkoff & Garner, 2012). Although toxic stress sounds similar to allostatic load, the requirement of an inadequate “buffer” in the definition of toxic stress differentiates them. In other words, allostatic load refers to an endogenous biological, measurable phenomenon whereas toxic stress attempts to also capture exogenous factors.
2.2: Measuring Early Adversity
Considerations for measuring adversity can be informative when it comes to conceptualizing how differences in experience may affect outcomes and understanding why the 10-question ACEs survey is not well-suited for measuring adversity.
Theoretical Models
A recent summary of childhood adversity literature outlines three primary models: specificity model, cumulative risk model, and dimensional models (see McLaughlin et al., 2021). The specificity model entails studying the outcomes following a specific type of adverse experience (e.g., physical abuse). The cumulative risk model sums the number of adverse experiences an individual has experienced (regardless of type). Dimensional models group experiences postulated to be alike in their consequences (e.g., threatening, depriving, or unpredictable experiences) and characterize scores along each relevant dimension (from not present to severe).
Source
Sources of information regarding exposure to childhood adversity can include the individual, their parent/caregiver, or additional informants (e.g., teacher). Objective information is the actual event a person experienced, often from formal reports such as court records or those from child protective services, whereas subjective information comes from reported perceived experiences (Baldwin & Degli Esposti, 2021). Some have argued that how stressful the individual perceived the experience to be is important for understanding the impact of the event (McLaughlin et al., 2021; Smith & Pollak, 2021), and indeed subjective experiences of childhood adversity have been found to be associated with the risk of psychopathology, independent of the objective experience (Baldwin & Degli Esposti, 2021). For deprivation, however, the changes in the brain that are driven by an absence of inputs are not necessarily dependent on one’s interpretation of events as depriving (McLaughlin et al., 2021). Survey questions can be retrospective, meaning participants are asked to remember events from their past, or they can be prospective, meaning participants are asked about current events. Often a time scale is used to distinguish between prospective and retrospective reports (i.e., “did you experience this in the past year” versus “have you experienced this is your life”; Moffitt et al., 2010), but it is important to note that every assessment of experiences, apart from those that only ask about ongoing events are retrospective to some degree. Prospective data can also come from formal records, such as those from child protective services. Baldwin et al. (2019) found relatively low agreement between prospective and retrospective reports of childhood maltreatment, but that agreement was higher when participants were interviewed, rather than surveyed, about their retrospective experiences. Baldwin et al. (2019) note that this difference could be explained by factors including memory biases and motivation of reporters. It is understandable that asking, for example, a 10-year-old to describe something that happened to them in the last year may be subject to fewer lapses in memory than asking a 20-year-old to describe something that happened to them when they were 10, but there may also be numerous other reasons that someone would disclose an experience at age 20 that they did not disclose at age 10.
Timing
There are three prevalent models used to test models about the effects of adversity as a function of timing (or developmental stage; see Dunn et al., 2018). The sensitive period model posits that experiences during particular developmental time periods have the strongest effects. The accumulation of risk model posits that more years of exposure to an adverse experience are associated with an increased risk of poor health, regardless of when those years took place. The recency model posits that events that happened most recently are associated with the strongest effects.
Socioeconomic Context
Socioeconomic status is based on objective indicators such as income, wealth, and level of education whereas subjective social status is one’s perception of their social class (Diemer et al., 2013). Though sometimes used as a proxy for adversity, it is important to note that the actual experiences of children at the same socioeconomic status vary greatly (Bronfenbrenner, 1996; Chaudry & Wimer, 2016). Therefore, a child’s social address should not be solely used as an indicator of their exposure to adversity.
2.3: Protective Factors
There is not a one-to-one association between exposure to early adversity and negative outcomes (Kessler et al., 2010). Not only do people vary in their sensitivity to environmental influences (Ellis & Boyce, 2008), but some adaptions to adversity are likely healthy and even beneficial. Further, the ability to be resilient to stress (i.e., when people recover to typical functioning or show minimal change in functioning following adversity) is due to a combination of internal and external factors (Humphreys et al., 2022). External, and therefore modifiable, factors that promote resilience to adversity include secure and supportive relationships with adults, such as parents, teachers, and extended family (Gartland et al., 2019).
Section 3: Translating the Understanding of Childhood Adversity into Classroom Pedagogical Practice
Despite the constraints of conceptualizing adversity through the lens of the ACEs study, it was a noteworthy endeavor that brought an awareness of trauma within education. So much so that policymakers have introduced changes to ensure that the academic needs of children with adverse histories are met. For example, attention at the federal level has ushered forth the Trauma-Informed Schools Act of 2019 (H.R.4146), which proposes to amend the Elementary and Secondary Education Act of 1965 (20 U.S.C § 7801) and would allow federal funds to be used for evidence-based trauma-informed interventions in schools. Unfortunately, such laudable efforts are pushing for the implementation of trauma-informed education at a rate that is outpacing the evidence for its efficacy and/or effectiveness (Maynard et al., 2019). Such shortcomings are attributable to several reasons that include the following: a lack of theoretical frameworks (Thomas et al., 2019), failure to consider complexities of schools (Fondren et al., 2020), limited information on capacity to serve diverse populations (Herrenkohl et al., 2019), exclusion of educators (Berger & Martin, 2021; Thomas et al., 2019) limited examination of teacher-related outcomes such as training effectiveness (Berger, 2019), and limited use of student-related academic outcomes (Fondren et al., 2020). Given the already complex nature of conceptualizing and understanding early childhood adversity, the poor state of the evidence for effective trauma-informed education practices, and the preponderance of different types of trauma-informed education programs, it becomes a daunting task to expect teachers to become more critical consumers of scientific literature and successfully translate research findings into pedagogical practice. It is therefore worthwhile considering how to address such challenges by applying the science of learning and instruction to trauma-informed education.
3.1: The Science of Learning
Drawn from different disciplines that include psychology, education, and neuroscience, to name a few, the Science of Learning (SoL) provides an understanding of how to improve active learning wherein people seek to understand complex content and transfer such knowledge to new problems and settings (Bransford et al., 2000). Specifically, the advancement of fundamental knowledge about learning, for children and adults, is done through the integration of transdisciplinary research, connected to specific challenges in education and the workforce (e.g., professional development), and translated into research and practice (Bransford et al., 2000). In other words, the SoL is a specific approach to understanding how people foster knowledge and transferable problem-solving skills, which emphasizes the onus of each person to lead their own learning (Bransford et al., 2000). Teachers and students can therefore be considered active learners who are integral parts of a community of practice within the classroom, school, and broader community. This means that the conceptualization of trauma-informed education necessitates the consideration of both the student and teacher as learners in the endeavor of learning and instruction within the context of adversity.
Adversity and the impact on student learning
For teachers to better engage in trauma-informed teaching, there is a need to understand how adversity impacts student learning beyond simple categorization of “trauma” based on ACEs. However, to date, there is still a paucity of work in understanding how learning processes are indeed affected. Burgeoning evidence suggests that rather than specific traumatic or adverse events, it is the response to the event (i.e., symptoms) that significantly predicts decreased academic performance in students (Ferrara & Panlilio, 2020; Mullins & Panlilio, 2021). Given the salience of event response in academic performance, it is therefore necessary to delve deeper into why or how such a relationship exists.
Specific learning mechanisms can be explicated by understanding what Mayer (2018) termed, “psychologies of subject matter,” which include theories of how students learn to read, learn mathematics, or learn science. Understanding students’ prior knowledge (e.g., phonological awareness, number sense, etc.) at the onset of formal and informal learning activities is important. For example, early maltreatment experiences have resulted in impaired syntax knowledge (Sylvestre & Mérette, 2010), decoding abilities (Mills et al., 2011), and vocabulary knowledge (Hong et al., 2018) that may explain problems with reading comprehension and achievement (Fantuzzo et al., 2014; Maclean et al., 2016; Widom, 2014). By incorporating these psychologies of subject matter, it becomes helpful for teachers to assess students’ baseline knowledge and understand how adversity may have specifically impacted specific subject matter areas that might inform where learning supports can be provided as preventive measures.
As active learners, students’ self-regulated learning processes (i.e., forethought and planning, performance and monitoring, and reaction and reflection on performance phases) allow them to systematically orient toward, and subsequently achieve, learning-related goals (Schunk & Zimmerman, 2003; Zimmerman, 2008; Zimmerman & Schunk, 2011). However, the neurophysiological impact of early adversity may prove to be problematic for such proactive and dynamic processes. For example, competing goals between emotional security (Davies & Martin, 2013) and task completion within the forethought and planning phase may result in different reactive patterns of emotional responding (Panlilio et al., 2020) in the performance and monitoring phase that impact planning (Kavanaugh & Holler, 2015) and motivation to achieve (Vondra et al., 1990). Given the dynamic nature of self-regulated learning, such problems in the forethought phase may lead to problems in the performance and monitoring phase. For example, pursuit of emotional security goals in lieu of achievement goals, coupled with smaller error-related negativity patterns due to early adversity, may result in selective attention that is not conducive to learning (Loman et al., 2013). Specifically, as an adaptive response to early adversity, students may orient toward perceived threat and exhibit difficulty in recognizing error and shifting attention (Pollak, 2015; Pollak et al., 2005). This response may give rise to problems with increased stress reactivity (Blair, 2010; Blair & Ursache, 2011), selection of appropriate learning-related and/or emotion regulation-related strategies (Jones Harden et al., 2016), metacognitive monitoring of strategy effectiveness toward goal attainment (Daly et al., 2017; Ferrara & Panlilio, 2020), and persistence and engagement necessary for task completion (Mullins & Panlilio, 2021), highlighting the need for socioemotional learning. Unfortunately, attribution of academic performance at the reaction and reflection phase may preclude constructive reflection on the selection of context-dependent strategies that were appropriate for adaptive responding in the context of adversity but inappropriate in the context of classroom-based learning. Inaccurate reflections on task-related performance may undergird the reasons for increased avoidance of school and absenteeism (Zorc et al., 2013), decreased likelihood of graduation (Stone, 2007), or decreased likelihood of pursuing post-secondary education (Courtney et al., 2011). Taken together, the different psychologies of subject matter, the complexities of self-regulated learning processes, and the impact of adversity make trauma-informed teaching inherently challenging and complicated.
Accounting for the complexity of adversity within classroom instruction
As outlined above, understanding the impact of adversity on student learning is a complicated endeavor and one in which the simplicity of ACEs becomes appealing. Specifically, conceptualizing adverse events as categories and equating higher scores with “worse” outcomes gives the illusion of a clearly defined problem that can be easily remedied by attending a professional development workshop on trauma-informed practice. However, such a proposition cannot be further from the truth as experiences of early adversity are quite complex, with an even more complicated set of consequences on the development and learning of children. If not careful, such a false belief about translating ACEs knowledge into classroom pedagogy may follow a similar trajectory of propagation as the learning-styles hypothesis (i.e., alignment of instruction method to student “learning style” such as visual learner vs. verbal learner), which persists in practice despite little evidence to support its effectiveness (Nancekivell et al., 2020; Pashler et al., 2008; Rogowsky et al., 2020). There is, therefore, a need to apply SoL within trauma-informed instruction akin to what was done to debunk the folklore of learning-styles hypothesis (Mayer, 2018; Pashler et al., 2008). This application means that adversity should be reframed not as a singular categorical event, but rather as an amalgam of experiences that often result in organized patterns of responses that children developed as adaptive or functional.
Addressing the consequences of adversity in the classroom entails reframing our understanding of trauma and adversity as ill-defined problem structures, defined as problems that have conflicting assumptions, evidence, and opinions that may lead to multiple solutions (Kitchener, 1983; Schraw et al., 1995). Teachers who attend trauma-informed professional development trainings may have learned strategies within a contrived or controlled context that rarely address a problem structure generally found in the real world (Mayer & Wittrock, 2006). Even the most effective problem solving that is typically associated with expertise in a specific domain of knowledge (e.g., pedagogical expertise in math education) may not necessarily transfer to a new and unfamiliar domain (e.g., trauma-informed instruction), particularly if that domain includes a nonroutine, ill-defined problem structure such as adversity.
Akin to students’ self-regulated learning processes, there are important processes needed to address ill-defined problem structures. According to Mayer and Wittrock (2006), cognitive processes in problem solving include representation (i.e., building a problem space that includes the initial state, the goal state, and subsequent intervention states), planning (i.e., devising a method for solving a problem), monitoring (i.e., evaluating the appropriateness and effectiveness of a strategy), executing (i.e., carrying out the planned strategy), and self-regulating (i.e., the instigating, modifying, or sustaining activities toward goal attainment). Problem solving processes are further reliant on several structures of knowledge that include factual knowledge, conceptual knowledge (e.g., cause-effect relationships), procedural knowledge, strategic knowledge (e.g., general methods or strategies), and metacognitive knowledge (i.e., awareness and control of one’s own cognitive processes that includes beliefs about one’s abilities). It is particularly important to note that when the knowledge structures related to adversity are considered within the context of trauma-informed education, it is expected that such cognitive processes be iterative and dynamic in how teachers select instruction strategies in response to the students’ learning processes and a teacher’s own reflection.
From a SoL perspective, these processes also assume that teachers are themselves active learners in their interactions with students, not just in their participation with professional development, but also in learning generally about their students’ histories. Because SoL focuses on underlying learning processes, it is expected to increase teachers’ reflection on learning that in turn, generates instructional change that can improve student achievement (Desimone, 2009). Such an approach can foster reflexive teaching practices that could potentially help move classroom instruction away from scripted responses to one that is more adaptive in the development of expertise (De Arment et al., 2013).
3.2: Facilitating Better Trauma-Informed Education by Moving Away from ACEs
As aforementioned, research on the effectiveness of “trauma-informed education practices” have typically been conducted on a small scale and should be considered preliminary evidence for such practices, rather than the type of confidence in research gained via extensive randomized trials (Thomas et al., 2019). In other words, though potentially promising, there is not yet an evidence base for what constitutes effective trauma-informed approaches in the educational context (Maynard et al., 2019). For schools and educators interested in integrating adversity/trauma-informed perspectives now, we provide specific ideas to incorporate for screening, teaching practices, school-wide practices, and professional development; yet note that further research is needed to validate these practices.
Screening
We advise against the use of the 10-question ACEs survey in schools (see section 1.6). Furthermore, even with appropriate measurement, it is not clear whether we will be able to know how, when, and with whom to intervene (Finkelhor, 2018; Finkelhor et al., 2015). There are evidence-based interventions outside of the classroom for some early adversity experiences (e.g., sexual abuse; Saywitz et al., 2000), though access to them is limited (Finkelhor, 2018), and the role of a teacher in implementation is not clear. Additionally, individual responses to adversity differ and so too may the support a given child may require. In other words, for individual screening to be beneficial, we would need to know how the measurement maps on to effective action for those students. Until we know how to personalize interventions based on reports to such measures, individual screening may not be ethical as it could result in the “soft bigotry of low expectations” (Bush, 2000). Multiple studies have found that when teachers have lower expectations of their students (Rosenthal & Jacobson, 1968), and even implicit bias as a result of a student’s background (e.g., race, gender; Gershenson et al., 2016), those students do not perform as well in school (Nelson, 2015). Importantly, experimental research provides causal evidence of the effect of teacher expectations on student performance. In a landmark study by Rosenthal and Jacobson (1968), teachers were given a list of students expected to make the most gains in a school year and those same students did in fact make the most gains. However, the names provided to the teachers were not selected based on aptitude, but rather placed on the list at random. We raise this concern as information given to teachers about a child’s ACE score or other adversity, while on the surface may allow for increased insight and empathy to this child, also has the risk of undermining the types of high expectations and opportunities for growth that foster student learning. Specifically, if teachers’ expectations of a student are lower, even implicitly so, as a result of seeing an elevated adversity score, there is a chance it could result in worse academic outcomes for that student.
One way in which teacher expectations meet student outcomes is via encouragement, and specifically how that encouragement does or does not encourage a growth mindset (e.g., “Great effort! You tried your best” compared to “The point isn’t to get it all right away. The point is to grow your understanding step by step. What can you try next?”; Dweck, 2015, p. 3). Though both provide students with encouragement, only the latter reflects the student’s potential for growth in a specific task or subject. One’s beliefs about their own abilities (e.g., how good they are in math) and expectancies for their success (e.g., how successful they would be at learning something new in math), which are in part fostered by socialization influences like statements from teachers reflecting a growth mindset, influence achievement (Wigfield & Eccles, 2000). In a longitudinal study on fifth through twelfth graders, students’ beliefs about their math abilities and their expectations for their success were found to be strong predictors of their grades in school, even more so than the previous grades they received (Eccles & Wigfield, 1995; Wigfield & Eccles, 2000).
While we caution against adversity screening using the ACEs survey with the aim of individual intervention in the classroom, we concur with others (e.g., Finkelhor, 2018) that teachers should continue to meet their mandatory reporter responsibilities of observing and reporting suspected maltreatment among students. Furthermore, teacher identification of mental health and behavioral problems, especially early in development, can play an important role for young students and for students who have experienced early adversity (Tabone et al., 2020).
Rather than the use of the ACEs survey for individual students, group-level screening may be helpful to anchor teachers, especially those new to a school or grade level, to knowledge about the range of experiences that their students face, past and present. For schools interested in group-level screening, one alternative assessment to the ACEs questionnaire is the Juvenile Victimization Questionnaire (Finkelhor et al., 2011). It assesses a wider range of adversities than the ACEs survey, including forms of both threat and deprivation, and includes forms of adversity that are particularly relevant to school contexts (e.g., assault or serious victimization by peers). This measure has been used in national tracking surveys and epidemiological studies on the prevalence of childhood adversity and victimization so there are national norms that can be used to interpret the scores as a function of age and sex (Finkelhor et al., 2005). There are many versions of the measure, but the screener (Hamby et al., 2011) requires an estimated 10–15 minutes to complete, making this more feasible for school contexts relative to longer instruments. On the Screener Sum Version of the Juvenile Victimization Questionnaire, respondents select yes/no from a list of questions, and then an item level, module, or aggregate score can be produced based on the victimization endorsements (Finkelhor et al., 2011; Hamby et al., 2011). We propose that de-identified module and aggregate scores may be appropriate for use and informative to teachers and administrators, though note that, as with the ACE scores, a score from this measure is not ideal for guiding individualized intervention at this time. Additionally, youth report survey screening options are often only appropriate for administration to an age range that does not reach students in their first years of school (e.g., the Juvenile Victim Questionnaire youth report measure is listed for ages 8–17; Finkelhor et al., 2011; Hamby et al., 2011) though other reporter versions such as the Juvenile Victimization Questionnaire caregiver report do not have the same age restrictions.
School-Wide Approach
Group-level screening may also be well-suited for a universal classroom-wide or school-wide approach within multi-tiered systems of support (MTSS). MTSS is a framework aimed at meeting the needs of all students that includes a continuum of services and supports in which there are three tiers implemented at a classroom-wide or school-wide level, the first of which is geared towards all students and the second and third increase in services based on student needs (Rossen & Cowan, 2013). MTSS has been suggested in the context of trauma-informed education to provide some structure to schools looking to integrate an adversity perspective (Berger, 2019; Chafouleas et al., 2016) given that current evidence-based trauma-informed education practices are limited (Maynard et al., 2019). In trauma-informed education, an example of a school-wide MTSS includes tier-1 initiatives that all students can benefit from, such as schoolwide bullying or violence prevention efforts, and tier-2 and tier-3 supports that entail more intensive and individualized interventions for those in need (Rossen & Cowan, 2013). Some tier-1 initiatives, such as school-based victimization prevention programs (Ttofi & Farrington, 2011), could potentially play a role in the prevention of some early adversity experiences, though more research is necessary to establish if that is the case (Finkelhor, 2018). Group-level screening could make teachers aware of the general realities their students face and illustrate the importance of these tier-1 interventions. Then, schools could capitalize on current MTSS procedures, so that as teachers identify potential mental health and behavioral problems, more qualified personnel, such as school counselors or special education teachers with mental health training (Hunter et al., 2021) could develop more intensive learning interventions as needed. A common proposal in discussions of adversity screening is referral to behavioral health practitioners or social workers, who then have knowledge about various treatment and referral options, though again the effectiveness of referrals varies based on the availability of treatments (Finkelhor, 2018), and tier-1 interventions that benefit all students, and perhaps especially those who have experienced early adversity, may be the best place for schools to start.
Teaching Practices and Professional Development
Though it is possible to implement tailored or individualized approaches for responding to specific needs in students, at present there is little guidance regarding how specifically educational practices should be tailored based on the adversity profile of a student. Instead, we recommend teachers adopt an open and accepting stance honoring the possibility that adversity may be affecting behaviors that are interfering with a student’s progress.
For professional development, rather than rooting trauma-informed education practices in the ACEs study, we recommend sharing the definitions and terms outlined in this paper to foster a broader view of adversity. Additionally, professional development sessions could include reflection by educators on adversity that encourages them to begin to question their own pedagogical practices. From a SoL perspective, teacher reflection can bring about instructional change that can improve student achievement (Desimone, 2009). Some teachers describe how engaging in reflection about the realities their students are facing and how their practices could be especially helpful for students who have experienced early adversity has helped them build more supportive classrooms (Koslouski & Stark, 2021). Ideally, this reflection could be guided by some adversity-informed reflective prompts for teachers, though until such are developed and studied reflection with less structure may still be helpful. Emphasizing the importance of teacher–student relationships may promote resilience through supportive relationships with adults (Gartland et al., 2019). Additionally, encouraging teachers to engage in continued learning about how adversity may influence learning, classroom behaviors, and peer relationships could be beneficial because, as aforementioned, a broader understanding of adversity could improve translation from research to classroom practice.
As aforementioned, we also encourage the continued use of tier-1 trauma-informed education practices that will be beneficial for providing supportive classrooms. For example, regular use of socioemotional learning practices in the classroom is beneficial to all students (Schonert-Reichl, 2017), and may be especially beneficial for students who have disproportionately experienced early adversity (Scott et al., 2021). These practices are aimed at developing a range of skills including those that aid in maintaining positive relationships and recognizing and managing emotions (Ragozzino et al., 2003). Examples of socioemotional learning practices include incorporating mindfulness exercises (e.g., a mental whole-body scan while noting current feelings and sensations; see Black & Fernando, 2014) and teacher modeling of emotion-regulation (e.g., “When people start talking about other things while I’m still giving directions, it feels frustrating for me and I have to take a breath. Afterward, I tell myself to try again”; George Lucas Educational Foundation, 2019). Teachers’ socioemotional competence and well-being are important for the implementation of supportive classroom practices, including socioemotional learning and building supportive teacher–student relationships (Jennings & Greenberg, 2009), and could be impacted if students share their past or present adverse experiences with them (Hydon et al., 2015). It is critical that teachers receive support in fostering their own well-being as they build classrooms that meet the needs of their students (Hydon et al., 2015).
Conclusion
Experiences of adversity are common among children, and more severe exposures are associated with poorer outcomes in academic contexts. Thus, many well-meaning teachers and administrators have advocated for screening to assess adversity exposure in the students they serve. We list recommendations in Table 2. However, the, the ACEs screening, which is the most commonly used method for this purpose, is not only unlikely to meet goals regarding matching up children to specific supports, it also has the potential to harm. There is not yet evidence that knowledge of adversity exposure leads to personalized trauma-informed interventions within schools, and it is plausible there may never be given that individuals vary in the manner in which even the same forms of adversity may affect functioning in the educational context. Furthermore, in addition to the ACEs survey being limited in measurement, even more comprehensive and accurate screening could have the unintended effect of negatively biasing teachers regarding students with histories of more adversity (e.g., the “soft bigotry of low expectations”). Rather than tailoring educational practices to specific children based on their “traumatic” experiences, we instead recommend educators focus their efforts on building supportive classrooms geared towards all students, with the understanding that early adversity can influence heterogeneous trajectories in student development and behavior. In addition, further research on educational practices, including the use of a shared language for describing and defining adversity-related experiences, are the concrete steps needed to better support a goal of adversity-informed education.
Table 2.
TRAUMA-INFORMED EDUCATION RECOMMENDATIONS
| SCREENING | - We do not recommend screening for adversity for individual intervention until there is a way of personalizing those interventions. Rather, group screening may make teachers aware of the realities the students at their school face, generally |
| SCHOOL-WIDE APPROACH | - Multi-tiered systems of support within schools could allow qualified personnel to provide additional support to individual students as necessary |
| TEACHING PRACTICES | - Given the lack of personalized interventions steps available, we recommend teachers adopt an open and accepting stance honoring the possibility of adversity affecting behavior rather than attempt individualized intervention for those who have experienced early adversity - We also encourage teachers to incorporate tier-1 support practices for all students, such as the integration of socioemotional learning (e.g., mindfulness exercises and emotion-regulation modeling) and the continued prioritization of teacher-student relationships |
| PROFESSIONAL DEVELOPMENT | - Rather than rooting trauma-informed education practices in the ACEs study, we recommend sharing the definitions and terms outlined in this paper - We also recommend teachers engage in continued reflection about adversity and their classroom practices, in line with a SoL perspective |
TRAUMA-INFORMED EDUCATION RECOMMENDATIONS
Acknowledgements:
We are grateful for comments on an earlier version of this draft from Dr. Katie McLaughlin.
Funding:
Dr. Humphreys was supported in part by the National Science Foundation (2042285) and by the National Institutes of Mental Health (R01MH129634).
Footnotes
Conflict of interest disclosure: The authors declare no conflicts of interest.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Elementary and Secondary Education Act of 1965, 20 U.S.C § 7801 (1965). https://uscode.house.gov/view.xhtml?req=(title:20%20section:7801%20edition:prelim).
- Alicke MD, & Weigel SH (2021). The reasonable person standard: Psychological and legal perspectives. Annual Review of Law and Social Science, 17(1), 123–138. 10.1146/annurev-lawsocsci-111620-020400 [DOI] [Google Scholar]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (Fifth Edition). American Psychiatric Association. 10.1176/appi.books.9780890425596 [DOI] [Google Scholar]
- Anda RF, Dong M, Brown DW, Felitti VJ, Giles WH, Perry GS, Valerie EJ, & Dube SR (2009). The relationship of adverse childhood experiences to a history of premature death of family members. BMC Public Health, 9(1), 106. 10.1186/1471-2458-9-106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anda RF, Felitti VJ, Bremner JD, Walker JD, Whitfield Ch., Perry BD, Dube SR, & Giles WH (2006). The enduring effects of abuse and related adverse experiences in childhood: A convergence of evidence from neurobiology and epidemiology. European Archives of Psychiatry and Clinical Neuroscience, 256(3), 174–186. 10.1007/s00406-005-0624-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anda RF, Porter LE, & Brown DW (2020). Inside the adverse childhood experience score: Strengths, limitations, and misapplications. American Journal of Preventive Medicine, 59(2), 293–295. 10.1016/j.amepre.2020.01.009 [DOI] [PubMed] [Google Scholar]
- Baldwin JR, Caspi A, Meehan AJ, Ambler A, Arseneault L, Fisher HL, Harrington H, Matthews T, Odgers CL, Poulton R, Ramrakha S, Moffitt TE, & Danese A (2021). Population vs individual prediction of poor health From results of adverse childhood experiences screening. JAMA Pediatrics, 175(4), 385. 10.1001/jamapediatrics.2020.5602 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baldwin JR, & Degli Esposti M (2021). Triangulating evidence on the role of perceived versus objective experiences of childhood adversity in psychopathology. JCPP Advances, 1(1). 10.1111/jcv2.12010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baldwin JR, Reuben A, Newbury JB, & Danese A (2019). Agreement between prospective and retrospective measures of childhood maltreatment: A systematic review and meta-analysis. JAMA Psychiatry, 76(6), 584. 10.1001/jamapsychiatry.2019.0097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berger E (2019). Multi-tiered approaches to trauma-informed care in schools: A systematic review. School Mental Health, 11(4), 650–664. 10.1007/s12310-019-09326-0 [DOI] [Google Scholar]
- Berger E, & Martin K (2021). Embedding trauma-informed practice within the education sector. Journal of Community & Applied Social Psychology, 31(2), 223–227. 10.1002/casp.2494 [DOI] [Google Scholar]
- Bernard DL, Calhoun CD, Banks DE, Halliday CA, Hughes-Halbert C, & Danielson CK (2021). Making the “C-ACE” for a culturally-informed adverse childhood experiences framework to understand the pervasive mental health impact of racism on black youth. Journal of Child & Adolescent Trauma, 14(2), 233–247. 10.1007/s40653-020-00319-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernstein DP, Fink L, Handelsman L, Foote J, Lovejoy M, Wenzel K, Sapareto E, & Ruggiero J (1994). Initial reliability and validity of a new retrospective measure of child abuse and neglect. American Journal of Psychiatry, 151(8), 1132–1136. 10.1176/ajp.151.8.1132 [DOI] [PubMed] [Google Scholar]
- Black DS, & Fernando R (2014). Mindfulness training and classroom behavior among lower-income and ethnic minority elementary school children. Journal of Child and Family Studies, 23(7), 1242–1246. 10.1007/s10826-013-9784-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blair C (2010). Stress and the development of self-regulation in context: Stress and the development of self-regulation. Child Development Perspectives, 4(3), 181–188. 10.1111/j.1750-8606.2010.00145.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blair C, & Ursache A (2011). A bidirectional theory of executive functions and self-regulation. In Vohs K & Baumeister R (Eds.), Handbook of self-regulation (pp. 300–320). Guilford Press. [Google Scholar]
- Bransford J, National Research Council (U.S.), & National Research Council (U.S.) (Eds.). (2000). How people learn: Brain, mind, experience, and school (Expanded ed). National Academy Press. [Google Scholar]
- Briggs EC, Amaya-Jackson L, Putnam KT, & Putnam FW (2021). All adverse childhood experiences are not equal: The contribution of synergy to adverse childhood experience scores. American Psychologist, 76(2), 243–252. 10.1037/amp0000768 [DOI] [PubMed] [Google Scholar]
- Bronfenbrenner U (1996). The ecology of human development: Experiments by nature and design. Harvard University Press. [Google Scholar]
- Brown MN (2021). Building trauma informed teachers: A constructivist grounded theory study of remote primary school teachers’ experiences with children living with the effects of complex childhood trauma [PhD, Queensland University of Technology]. 10.5204/thesis.eprints.213045 [DOI] [Google Scholar]
- Bush G (2000, July 10). OnPolitics. https://www.washingtonpost.com/wp-srv/onpolitics/elections/bushtext071000.htm
- Chafouleas SM, Johnson AH, Overstreet S, & Santos NM (2016). Toward a blueprint for trauma-informed service delivery in schools. School Mental Health, 8(1), 144–162. 10.1007/s12310-015-9166-8 [DOI] [Google Scholar]
- Chaudry A, & Wimer C (2016). Poverty is not just an indicator: The relationship between income, poverty, and child well-being. Academic Pediatrics, 16(3), S23–S29. 10.1016/j.acap.2015.12.010 [DOI] [PubMed] [Google Scholar]
- Corbin TJ, Purtle J, Rich LJ, Rich JA, Adams EJ, Yee G, & Bloom SL (2013). The Prevalence of trauma and childhood adversity in an urban, hospital-based violence intervention program. Journal of Health Care for the Poor and Underserved, 24(3), 1021–1030. 10.1353/hpu.2013.0120 [DOI] [PubMed] [Google Scholar]
- Courtney M, Brown A, Katz C, Love K, & Klodnick V (2011). Midwest Evaluation of the Adult Functioning of Former Foster Youth: Outcomes at Age 26. https://www.chapinhall.org/wp-content/uploads/Midwest-Eval-Outcomes-at-Age-26.pdf
- Cronholm PF, Forke CM, Wade R, Bair-Merritt MH, Davis M, Harkins-Schwarz M, Pachter LM, & Fein JA (2015). Adverse childhood experiences: Expanding the concept of adversity. American Journal of Preventive Medicine, 49(3), 354–361. 10.1016/j.amepre.2015.02.001 [DOI] [PubMed] [Google Scholar]
- Crowley DM, Connell CM, Noll J, Green L, Scott T, & Giray C (2022). Legislating to prevent adverse childhood experiences: Growth and opportunities for evidence-based policymaking and prevention. Prevention Science, 23(2), 181–191. 10.1007/s11121-021-01292-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daly BP, Hildenbrand AK, Turner E, Berkowitz S, & Tarazi RA (2017). Executive functioning among college students with and without history of childhood maltreatment. Journal of Aggression, Maltreatment & Trauma, 26(7), 717–735. 10.1080/10926771.2017.1317685 [DOI] [Google Scholar]
- Danese A, & McEwen BS (2012). Adverse childhood experiences, allostasis, allostatic load, and age-related disease. Physiology & Behavior, 106(1), 29–39. 10.1016/j.physbeh.2011.08.019 [DOI] [PubMed] [Google Scholar]
- Davies PT, & Martin MJ (2013). The reformulation of emotional security theory: The role of children’s social defense in developmental psychopathology. Development and Psychopathology, 25(4pt2), 1435–1454. 10.1017/S0954579413000709 [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Arment ST, Reed E, & Wetzel AP (2013). Promoting adaptive expertise: A conceptual framework for special educator preparation. Teacher Education and Special Education: The Journal of the Teacher Education Division of the Council for Exceptional Children, 36(3), 217–230. 10.1177/0888406413489578 [DOI] [Google Scholar]
- Desimone LM (2009). Improving impact studies of teachers’ professional development: Toward better conceptualizations and measures. Educational Researcher, 38(3), 181–199. 10.3102/0013189X08331140 [DOI] [Google Scholar]
- Diemer MA, Mistry RS, Wadsworth ME, López I, & Reimers F (2013). Best Practices in conceptualizing and measuring social class in psychological research: Social class measurement. Analyses of Social Issues and Public Policy, 13(1), 77–113. 10.1111/asap.12001 [DOI] [Google Scholar]
- Dube SR, Anda RF, Felitti VJ, Chapman DP, Williamson DF, & Giles WH (2001). Childhood abuse, household dysfunction, and the risk of attempted suicide throughout the life span: Findings from the Adverse Childhood Experiences Study. JAMA, 286(24), 3089. 10.1001/jama.286.24.3089 [DOI] [PubMed] [Google Scholar]
- Dunn EC, Soare TW, Raffeld MR, Busso DS, Crawford KM, Davis KA, Fisher VA, Slopen N, Smith ADAC, Tiemeier H, & Susser ES (2018). What life course theoretical models best explain the relationship between exposure to childhood adversity and psychopathology symptoms: Recency, accumulation, or sensitive periods? Psychological Medicine, 48(15), 2562–2572. 10.1017/S0033291718000181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dweck C (2015, September 22). Carol Dweck revisits the ‘growth mindset.’ EducationWeek https://www.edweek.org/leadership/opinion-carol-dweck-revisits-the-growth-mindset/2015/09?print=1 [Google Scholar]
- Eaton S, Cornwell H, Hamilton-Giachritsis C, & Fairchild G (2022). Resilience and young people’s brain structure, function and connectivity: A systematic review. Neuroscience & Biobehavioral Reviews, 132, 936–956. 10.1016/j.neubiorev.2021.11.001 [DOI] [PubMed] [Google Scholar]
- Eccles JS, & Wigfield A (1995). In the mind of the actor: The structure of adolescents’ achievement task values and expectancy-related beliefs. Personality and Social Psychology Bulletin, 21(3), 215–225. 10.1177/0146167295213003 [DOI] [Google Scholar]
- Ellis BJ, & Boyce WT (2008). Biological sensitivity to context. Current Directions in Psychological Science, 17(3), 183–187. 10.1111/j.1467-8721.2008.00571.x [DOI] [Google Scholar]
- Ellis BJ, Figueredo AJ, Brumbach BH, & Schlomer GL (2009). Fundamental dimensions of environmental risk: The impact of harsh versus unpredictable environments on the evolution and development of life history strategies. Human Nature, 20(2), 204–268. 10.1007/s12110-009-9063-7 [DOI] [PubMed] [Google Scholar]
- Ellis BJ, Sheridan MA, Belsky J, & McLaughlin KA (2022). Why and how does early adversity influence development? Toward an integrated model of dimensions of environmental experience. Development and Psychopathology, 34(2), 447–471. 10.1017/S0954579421001838 [DOI] [PubMed] [Google Scholar]
- Fantuzzo JW, LeBoeuf WA, & Rouse HL (2014). An investigation of the relations between school concentrations of student risk factors and student educational well-being. Educational Researcher, 43(1), 25–36. 10.3102/0013189X13512673 [DOI] [Google Scholar]
- Felitti VJ (2019). Origins of the ACE study. American Journal of Preventive Medicine, 56(6), 787–789. 10.1016/j.amepre.2019.02.011 [DOI] [PubMed] [Google Scholar]
- Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, Koss MP, & Marks JS (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. American Journal of Preventive Medicine, 14(4), 245–258. 10.1016/S0749-3797(98)00017-8 [DOI] [PubMed] [Google Scholar]
- Ferrara AM, & Panlilio CC (2020). The role of metacognition in explaining the relationship between early adversity and reading comprehension. Children and Youth Services Review, 112, 104884. 10.1016/j.childyouth.2020.104884 [DOI] [Google Scholar]
- Finkelhor D (2018). Screening for adverse childhood experiences (ACEs): Cautions and suggestions. Child Abuse & Neglect, 85, 174–179. 10.1016/j.chiabu.2017.07.016 [DOI] [PubMed] [Google Scholar]
- Finkelhor D, Hamby SL, Ormrod R, & Turner H (2005). The Juvenile Victimization Questionnaire: Reliability, validity, and national norms. Child Abuse & Neglect, 29(4), 383–412. 10.1016/j.chiabu.2004.11.001 [DOI] [PubMed] [Google Scholar]
- Finkelhor D, Shattuck A, Turner H, & Hamby S (2015). A revised inventory of Adverse Childhood Experiences. Child Abuse & Neglect, 48, 13–21. 10.1016/j.chiabu.2015.07.011 [DOI] [PubMed] [Google Scholar]
- Finkelhor D, Turner H, Hamby S, & Ormrod R (2011). The Juvenile Victimization Questionnaire—2nd Revision (JVQ-R2). [Google Scholar]
- Folkman S, & Lazarus RS (1986). Stress processes and depressive symptomatology. Journal of Abnormal Psychology, 95(2), 107–113. 10.1037/0021-843X.95.2.107 [DOI] [PubMed] [Google Scholar]
- Fondren K, Lawson M, Speidel R, McDonnell CG, & Valentino K (2020). Buffering the effects of childhood trauma within the school setting: A systematic review of trauma-informed and trauma-responsive interventions among trauma-affected youth. Children and Youth Services Review, 109, 104691. 10.1016/j.childyouth.2019.104691 [DOI] [Google Scholar]
- Frankenhuis WE, & Amir D (2022). What is the expected human childhood? Insights from evolutionary anthropology. Development and Psychopathology, 34(2), 473–497. 10.1017/S0954579421001401 [DOI] [PubMed] [Google Scholar]
- Gartland D, Riggs E, Muyeen S, Giallo R, Afifi TO, MacMillan H, Herrman H, Bulford E, & Brown SJ (2019). What factors are associated with resilient outcomes in children exposed to social adversity? A systematic review. BMJ Open, 9(4), e024870. 10.1136/bmjopen-2018-024870 [DOI] [PMC free article] [PubMed] [Google Scholar]
- George Lucas Educational Foundation (Director). (2019, January 14). Teaching self-regulation by modeling. https://www.edutopia.org/video/teaching-self-regulation-modeling
- Gershenson S, Holt SB, & Papageorge NW (2016). Who believes in me? The effect of student–teacher demographic match on teacher expectations. Economics of Education Review, 52, 209–224. 10.1016/j.econedurev.2016.03.002 [DOI] [Google Scholar]
- Greenough WT, Black JE, & Wallace CS (1987). Experience and brain development. Child Development, 58(3), 539. 10.2307/1130197 [DOI] [PubMed] [Google Scholar]
- Guyon-Harris KL, Humphreys KL, & Zeanah CH (2021). Adverse caregiving in early life: The trauma and deprivation distinction in young children. Infant Mental Health Journal, 42(1), 87–95. 10.1002/imhj.21892 [DOI] [PubMed] [Google Scholar]
- Hamby S, Finkelhor D, Turner H, & Kracke K (2011). The Juvenile Victimization Questionnaire toolkit. https://www.unh.edu/ccrc/juvenile-victimization-questionnaire [Google Scholar]
- Herrenkohl TI, Hong S, & Verbrugge B (2019). Trauma-informed programs based in schools: Linking concepts to practices and assessing the evidence. American Journal of Community Psychology, 64(3–4), 373–388. 10.1002/ajcp.12362 [DOI] [PubMed] [Google Scholar]
- Hong S, Rhee TG, & Piescher KN (2018). Longitudinal association of child maltreatment and cognitive functioning: Implications for child development. Child Abuse & Neglect, 84, 64–73. 10.1016/j.chiabu.2018.07.026 [DOI] [PubMed] [Google Scholar]
- Humphreys KL, King LS, Guyon-Harris KL, & Zeanah CH (2022). Caregiver regulation: A modifiable target promoting resilience to early adverse experiences. Psychological Trauma: Theory, Research, Practice, and Policy, 14(S1), S63–S71. 10.1037/tra0001111 [DOI] [PubMed] [Google Scholar]
- Humphreys KL, LeMoult J, Wear JG, Piersiak HA, Lee A, & Gotlib IH (2020). Child maltreatment and depression: A meta-analysis of studies using the Childhood Trauma Questionnaire. Child Abuse & Neglect, 102, 104361. 10.1016/j.chiabu.2020.104361 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hunter W, Taylor Jonte C., Bester M, Nichols S, & Panlilio C (2021). Considerations for incorporating trauma-informed care content within special education teacher preparation and professional development programs. Journal of Special Education Preparation, 1(2), 48–55. 10.33043/JOSEP.1.2.48-55 [DOI] [Google Scholar]
- Hydon S, Wong M, Langley AK, Stein BD, & Kataoka SH (2015). Preventing secondary traumatic stress in educators. Child and Adolescent Psychiatric Clinics of North America, 24(2), 319–333. 10.1016/j.chc.2014.11.003 [DOI] [PubMed] [Google Scholar]
- Jennings PA, & Greenberg MT (2009). The prosocial classroom: Teacher social and emotional competence in relation to student and classroom outcomes. Review of Educational Research, 79(1), 491–525. 10.3102/0034654308325693 [DOI] [Google Scholar]
- Jensen SKG, Berens AE, & Nelson CA (2017). Effects of poverty on interacting biological systems underlying child development. The Lancet Child & Adolescent Health, 1(3), 225–239. 10.1016/S2352-4642(17)30024-X [DOI] [PubMed] [Google Scholar]
- Johnson SB, Riley AW, Granger DA, & Riis J (2013). The science of early life toxic stress for pediatric practice and advocacy. Pediatrics, 131(2), 319–327. 10.1542/peds.2012-0469 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones Harden B, Buhler A, & Parra LJ (2016). Maltreatment in infancy: A developmental perspective on prevention and intervention. Trauma, Violence, & Abuse, 17(4), 366–386. 10.1177/1524838016658878 [DOI] [PubMed] [Google Scholar]
- Karatekin C, & Hill M (2019). Expanding the original definition of adverse childhood experiences (ACEs). Journal of Child & Adolescent Trauma, 12(3), 289–306. 10.1007/s40653-018-0237-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kavanaugh B, & Holler K (2015). Brief report: Neurocognitive functioning in adolescents following childhood maltreatment and evidence for underlying planning & organizational deficits. Child Neuropsychology, 21(6), 840–848. 10.1080/09297049.2014.929101 [DOI] [PubMed] [Google Scholar]
- Kessler RC, McLaughlin KA, Green JG, Gruber MJ, Sampson NA, Zaslavsky AM, Aguilar-Gaxiola S, Alhamzawi AO, Alonso J, Angermeyer M, Benjet C, Bromet E, Chatterji S, de Girolamo G, Demyttenaere K, Fayyad J, Florescu S, Gal G, Gureje O, … Williams DR (2010). Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. British Journal of Psychiatry, 197(5), 378–385. 10.1192/bjp.bp.110.080499 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kitchener KS (1983). Cognition, metacognition, and epistemic cognition. Human Development, 26(4), 222–232. 10.1159/000272885 [DOI] [Google Scholar]
- Koslouski JB, & Stark K (2021). Promoting learning for students experiencing adversity and trauma: The everyday, yet profound, actions of teachers. The Elementary School Journal, 121(3), 430–453. 10.1086/712606 [DOI] [Google Scholar]
- Loman MM, Johnson AE, Westerlund A, Pollak SD, Nelson CA, & Gunnar MR (2013). The effect of early deprivation on executive attention in middle childhood: Early deprivation and executive attention. Journal of Child Psychology and Psychiatry, 54(1), 37–45. 10.1111/j.1469-7610.2012.02602.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maclean MJ, Taylor CL, & O’Donnell M (2016). Pre-existing adversity, level of child protection involvement, and school attendance predict educational outcomes in a longitudinal study. Child Abuse & Neglect, 51, 120–131. 10.1016/j.chiabu.2015.10.026 [DOI] [PubMed] [Google Scholar]
- Maguire-Jack K, Lanier P, & Lombardi B (2020). Investigating racial differences in clusters of adverse childhood experiences. American Journal of Orthopsychiatry, 90(1), 106–114. 10.1037/ort0000405 [DOI] [PubMed] [Google Scholar]
- Masten AS (2001). Ordinary magic: Resilience processes in development. American Psychologist, 56(3), 227–238. 10.1037/0003-066X.56.3.227 [DOI] [PubMed] [Google Scholar]
- Mayer RE (2018). Educational psychology’s past and future contributions to the science of learning, science of instruction, and science of assessment. Journal of Educational Psychology, 110(2), 174–179. 10.1037/edu0000195 [DOI] [Google Scholar]
- Mayer RE, & Wittrock MC (2006). Problem solving. In Handbook of educational psychology (pp. 287–303). Lawrence Erlbaum Associates Publishers. [Google Scholar]
- Maynard BR, Farina A, Dell NA, & Kelly MS (2019). Effects of trauma-informed approaches in schools: A systematic review. Campbell Systematic Reviews, 15(1–2). 10.1002/cl2.1018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mcewen B (2002). Sex, stress and the hippocampus: Allostasis, allostatic load and the aging process. Neurobiology of Aging, 23(5), 921–939. 10.1016/S0197-4580(02)00027-1 [DOI] [PubMed] [Google Scholar]
- McKelvey LM, Conners Edge NA, Fitzgerald S, Kraleti S, & Whiteside-Mansell L (2017). Adverse childhood experiences: Screening and health in children from birth to age 5. Families, Systems, & Health, 35(4), 420–429. 10.1037/fsh0000301 [DOI] [PubMed] [Google Scholar]
- McLaughlin KA (2016). Future Directions in childhood adversity and youth psychopathology. Journal of Clinical Child & Adolescent Psychology, 45(3), 361–382. 10.1080/15374416.2015.1110823 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Sheridan MA, Humphreys KL, Belsky J, & Ellis BJ (2021). The value of dimensional models of early experience: Thinking clearly about concepts and categories. Perspectives on Psychological Science, 16(6), 1463–1472. 10.1177/1745691621992346 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLennan JD, MacMillan HL, & Afifi TO (2020). Questioning the use of adverse childhood experiences (ACEs) questionnaires. Child Abuse & Neglect, 101, 104331. 10.1016/j.chiabu.2019.104331 [DOI] [PubMed] [Google Scholar]
- Mills R, Alati R, O’Callaghan M, Najman JM, Williams GM, Bor W, & Strathearn L (2011). Child abuse and neglect and cognitive function at 14 years of age: Findings from a birth cohort. Pediatrics, 127(1), 4–10. 10.1542/peds.2009-3479 [DOI] [PubMed] [Google Scholar]
- Moffitt TE, Caspi A, Taylor A, Kokaua J, Milne BJ, Polanczyk G, & Poulton R (2010). How common are common mental disorders? Evidence that lifetime prevalence rates are doubled by prospective versus retrospective ascertainment. Psychological Medicine, 40(6), 899–909. 10.1017/S0033291709991036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Monroe SM (2008). Modern approaches to conceptualizing and measuring human life stress. Annual Review of Clinical Psychology, 4(1), 33–52. 10.1146/annurev.clinpsy.4.022007.141207 [DOI] [PubMed] [Google Scholar]
- Mullins CA, & Panlilio CC (2021). Exploring the mediating effect of academic engagement on math and reading achievement for students who have experienced maltreatment. Child Abuse & Neglect, 117, 105048. 10.1016/j.chiabu.2021.105048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nancekivell SE, Shah P, & Gelman SA (2020). Maybe they’re born with it, or maybe it’s experience: Toward a deeper understanding of the learning style myth. Journal of Educational Psychology, 112(2), 221–235. 10.1037/edu0000366 [DOI] [Google Scholar]
- National Center for Health Statistics. (1991). Exposure to alcoholism in the family: United States, 1988. U.S. Department of Health and Human Services. [Google Scholar]
- Nelson L (2015, August 19). Racism in the classroom: The “soft bigotry of low expectations” is just regular bigotry. Vox. https://www.vox.com/policy-and-politics/2015/8/19/9178573/teacher-students-race-study [Google Scholar]
- Overstreet S, & Chafouleas SM (2016). Trauma-informed schools: Introduction to the special issue. School Mental Health, 8(1), 1–6. 10.1007/s12310-016-9184-1 [DOI] [Google Scholar]
- Pandell L (2022, January 25). How trauma became the word of the decade. Vox. https://www.vox.com/the-highlight/22876522/trauma-covid-word-origin-mental-health [Google Scholar]
- Panlilio CC, Harring JR, Jones Harden B, Morrison CI, & Drouin Duncan A (2020). Heterogeneity in the dynamic arousal and modulation of fear in young foster children. Children and Youth Services Review, 116, 105199. 10.1016/j.childyouth.2020.105199 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pashler H, McDaniel M, Rohrer D, & Bjork R (2008). Learning styles: Concepts and evidence. Psychological Science in the Public Interest, 9(3), 105–119. 10.1111/j.1539-6053.2009.01038.x [DOI] [PubMed] [Google Scholar]
- Pollak SD (2015). Developmental psychopathology: Recent advances and future challenges. World Psychiatry, 14(3), 262–269. 10.1002/wps.20237 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollak SD, Vardi S, Putzer Bechner AM, & Curtin JJ (2005). Physically abused children’s regulation of attention in eesponse to hostility. Child Development, 76(5), 968–977. 10.1111/j.1467-8624.2005.00890.x [DOI] [PubMed] [Google Scholar]
- Portell M (2019, December 16). Understanding trauma-informed education. Edutopia. https://www.edutopia.org/article/understanding-trauma-informed-education [Google Scholar]
- Purewal SK, Bucci M, Wang LG, Koita K, Marques SS, Oh D, & Harris NB (2016). Screening for adverse childhood experiences (ACEs) in an integrated pediatric care model. Zero to Three, 36(3), 10–16. [Google Scholar]
- Ragozzino K, Resnik H, Utne-O’Brien M, & Weissberg RP (2003). Promoting Academic Achievement through Social and Emotional Learning. Educational Horizons, 81(4), 169–171. [Google Scholar]
- Rogowsky BA, Calhoun BM, & Tallal P (2020). Providing instruction based on students’ learning style preferences does not improve learning. Frontiers in Psychology, 11, 164. 10.3389/fpsyg.2020.00164 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenthal R, & Jacobson L (1968). Pygmalion in the classroom. The Urban Review, 3(1), 16–20. 10.1007/BF02322211 [DOI] [Google Scholar]
- Rossen E, & Cowan K (2013). The role of schools in supporting traumatized students. Prinicipal’s Research Review, 8(6), 1–8. https://education.ucsb.edu/sites/default/files/hosford_clinic/docs/prr_nov13_trauma_sensitive_schools.pdf. [Google Scholar]
- Saywitz KJ, Mannarino AP, Berliner L, & Cohen JA (2000). Treatment of sexually abused children and adolescents. American Psychologist, 55(9), 1040–1049. 10.1037/0003-066X.55.9.1040 [DOI] [PubMed] [Google Scholar]
- Schonert-Reichl KA (2017). Social and emotional learning and teachers. The Future of Children, 27(1), 137–155. [Google Scholar]
- Schraw G, Dunkle ME, & Bendixen LD (1995). Cognitive processes in well-defined and ill-defined problem solving. Applied Cognitive Psychology, 9(6), 523–538. 10.1002/acp.2350090605 [DOI] [Google Scholar]
- Schunk DH, & Zimmerman BJ (2003). Self-regulation and learning. In Weiner IB (Ed.), Handbook of Psychology (p. wei0704). John Wiley & Sons, Inc. 10.1002/0471264385.wei0704 [DOI] [Google Scholar]
- Scott J, Jaber LS, & Rinaldi CM (2021). Trauma-informed school strategies for SEL and ACE concerns during COVID-19. Education Sciences, 11(12), 796. 10.3390/educsci11120796 [DOI] [Google Scholar]
- Sheridan MA, & McLaughlin KA (2014). Dimensions of early experience and neural development: Deprivation and threat. Trends in Cognitive Sciences, 18(11), 580–585. 10.1016/j.tics.2014.09.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shonkoff JP, & Garner AS (2012). The lifelong effects of early childhood adversity and toxic stress. Pediatrics, 129(1), e232–e246. 10.1542/peds.2011-2663 [DOI] [PubMed] [Google Scholar]
- Smith KE, & Pollak SD (2021). Rethinking concepts and categories for understanding the neurodevelopmental effects of childhood adversity. Perspectives on Psychological Science, 16(1), 67–93. 10.1177/1745691620920725 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Starecheski L (2015, March 2). Take the ACE quiz—And learn what it does and doesn’t mean. NPR. [Google Scholar]
- Stone S (2007). Child maltreatment, out-of-home placement and academic vulnerability: A fifteen-year review of evidence and future directions. Children and Youth Services Review, 29(2), 139–161. 10.1016/j.childyouth.2006.05.001 [DOI] [Google Scholar]
- Straus MA, Gelles RJ, & Asplund LM (1990). Physical violence in American families: Risk factors and adaptations to violence in 8,145 families. Violence and Victims, 5(4), 297–298. 10.1891/0886-6708.5.4.297 [DOI] [Google Scholar]
- Struck S, Stewart-Tufescu A, Asmundson AJN, Asmundson GGJ, & Afifi TO (2021). Adverse childhood experiences (ACEs) research: A bibliometric analysis of publication trends over the first 20 years. Child Abuse & Neglect, 112, 104895. 10.1016/j.chiabu.2020.104895 [DOI] [PubMed] [Google Scholar]
- Sylvestre A, & Mérette C (2010). Language delay in severely neglected children: A cumulative or specific effect of risk factors? Child Abuse & Neglect, 34(6), 414–428. 10.1016/j.chiabu.2009.10.003 [DOI] [PubMed] [Google Scholar]
- Szabo S, Tache Y, & Somogyi A (2012). The legacy of Hans Selye and the origins of stress research: A retrospective 75 years after his landmark brief “Letter” to the editor of Nature. Stress, 15(5), 472–478. 10.3109/10253890.2012.710919 [DOI] [PubMed] [Google Scholar]
- Tabone JK, Rishel CW, Hartnett HP, & Szafran KF (2020). Examining the effectiveness of early intervention to create trauma-informed school environments. Children and Youth Services Review, 113, 104998. 10.1016/j.childyouth.2020.104998 [DOI] [Google Scholar]
- The National Child Traumatic Stress Network. (2017). Creating, supporting, and sustaining trauma-informed schools: A system framework. https://www.nctsn.org/sites/default/files/resources//creating_supporting_sustaining_trauma_informed_schools_a_systems_framework.pdf
- Thomas MS, Crosby S, & Vanderhaar J (2019). Trauma-informed practices in schools across two decades: An interdisciplinary review of research. Review of Research in Education, 43(1), 422–452. 10.3102/0091732X18821123 [DOI] [Google Scholar]
- Trauma-Informed Schools Act of 2019, H.R.4146, 116th Cong. (2019). https://www.congress.gov/bill/116th-congress/house-bill/4146/text?q=%7B%22search%22%3A%5B%22HR+20%22%5D%7D&r=1&s=1
- Ttofi MM, & Farrington DP (2011). Effectiveness of school-based programs to reduce bullying: A systematic and meta-analytic review. Journal of Experimental Criminology, 7(1), 27–56. 10.1007/s11292-010-9109-1 [DOI] [Google Scholar]
- Vondra JI, Barnett D, & Cicchetti D (1990). Self-concept, motivation, and competence among preschoolers from maltreating and comparison families. Child Abuse & Neglect, 14(4), 525–540. 10.1016/0145-2134(90)90101-X [DOI] [PubMed] [Google Scholar]
- Watson P (2019). How to screen for ACEs in an efficient, sensitive, and effective manner. Paediatrics & Child Health, 24(1), 37–38. 10.1093/pch/pxy146 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Widom CS (2014). Longterm consequences of child maltreatment. In Korbin JE & Krugman RD (Eds.), Handbook of child maltreatment (Vol. 2, pp. 225–247). Springer; Netherlands. 10.1007/978-94-007-7208-3_12 [DOI] [Google Scholar]
- Wigfield A, & Eccles JS (2000). Expectancy–value theory of achievement motivation. Contemporary Educational Psychology, 25(1), 68–81. 10.1006/ceps.1999.1015 [DOI] [PubMed] [Google Scholar]
- Wyatt GE (1985). The sexual abuse of Afro-American and White-American women in childhood. Child Abuse & Neglect, 9(4), 507–519. 10.1016/0145-2134(85)90060-2 [DOI] [PubMed] [Google Scholar]
- Zarse EM, Neff MR, Yoder R, Hulvershorn L, Chambers JE, & Chambers RA (2019). The adverse childhood experiences questionnaire: Two decades of research on childhood trauma as a primary cause of adult mental illness, addiction, and medical diseases. Cogent Medicine, 6(1), 1581447. 10.1080/2331205X.2019.1581447 [DOI] [Google Scholar]
- Zimmerman BJ (2008). Investigating self-regulation and motivation: historical background, methodological developments, and future prospects. American Educational Research Journal, 45(1), 166–183. 10.3102/0002831207312909 [DOI] [Google Scholar]
- Zimmerman BJ, & Schunk DH (Eds.). (2011). Handbook of self-regulation of learning and performance. Routledge. [Google Scholar]
- Zorc CS, O’Reilly ALR, Matone M, Long J, Watts CL, & Rubin D (2013). The relationship of placement experience to school absenteeism and changing schools in young, school-aged children in foster care. Children and Youth Services Review, 35(5), 826–833. 10.1016/j.childyouth.2013.02.006 [DOI] [PMC free article] [PubMed] [Google Scholar]