

Abstract
Objectives
To compare skeletal and dentoalveolar changes of miniscrew-assisted rapid palatal expansion (MARPE) according to the length of the miniscrews.
Materials and Methods
This two-arm parallel-randomized controlled trial included 32 adult patients aged 19–35 years who received orthodontic treatment with MARPE. Patients were allocated to two groups, group long (L) and short (S), through block randomization according to the length of the miniscrews installed in MARPE. Cone-beam computed tomography was performed before expansion and after removal of the MARPE; superimposition of the images was conducted. The primary outcome included the amount of bone expansion and the change in the inclination of the anchorage teeth. The secondary outcome included the success rate of midpalatal suture opening and stability of the miniscrews. Blinding was performed during outcome assessment.
Results
The final sample comprised 31 patients. There was no significant difference in patient characteristics between group L (n = 16) and group S (n = 15). The change in the width of the processus zygomaticus (P = .010) and ectocanine (P = .001) was significantly higher in group L. A significantly higher success rate of the posterior miniscrews was seen in group L (P = .024). There was no statistically significant difference in the success rate of suture separation or change in tooth inclination. Notable complications were not reported.
Conclusions
MARPE with longer miniscrews can increase the amount of expansion of the maxillary basal bone and canine alveolar bone. Although it also aided in miniscrew stability, it did not guarantee successful midpalatal suture separation.
Keywords: MARPE, Randomized clinical trial
INTRODUCTION
Successful maxillary skeletal expansion with tooth-bone–borne rapid palatal expansion (RPE) incorporating miniscrews (miniscrew-assisted RPE; MARPE) has been reported in adult patients.1 Recent clinical studies have found significant dentoalveolar and skeletal expansion with long-term stability using MARPE.2,3 MARPE reportedly causes relatively even stress distribution, reduces the stress to the buccal plate of the anchor teeth, and reduces tipping of the teeth compared with conventional or bone-borne RPE.4 Therefore, MARPE could serve as an effective treatment modality in adult patients with transverse maxillary deficiency.2–5
Failure of nonsurgical maxillary expansion is critical, as it can lead to changes in the treatment plan, such as surgical-assisted RPE. The success rate of MARPE in adult patients reportedly ranges from 84.25%–86.96%.1,2 Various MARPE designs are used in orthodontic clinics to overcome individual variation and increase the predictability of nonsurgical orthodontic treatment.1,6–8
The length of the miniscrews installed with MARPE is one of the design factors that can be selected by the clinicians. Longer miniscrews, which can penetrate the bicortical bone (palatal and nasal cortical bone of the maxilla), have been recommended for greater orthopedic effects and parallel expansion at the coronal aspect.7 However, longer miniscrews can damage the nasal floor mucosa or cause discomfort to the patient; thus, the effectiveness should be carefully evaluated. Several finite element analyses (FEA) have been conducted to compare the effect of MARPE based on the length of the miniscrews.9,10 However, FEA cannot accurately reflect the complex craniofacial structure and actual biological responses of the human body.
This prospective randomized clinical trial (RCT) was designed to investigate the skeletal and dentoalveolar effects of MARPE according to the length of the miniscrew in adults using cone-beam computed tomography (CBCT). In addition, the success rates of the opening of the midpalatal suture and the applied miniscrews were evaluated in the study population.
MATERIALS AND METHODS
Trial Design
This was a two-arm, parallel-group RCT with a 1:1 allocation ratio performed at the Department of Orthodontics, Yonsei University Dental Hospital, Seoul, Republic of Korea. Ethical approval was obtained from the Institutional Review Board of Yonsei University Dental Hospital (CRNo: 2-2019-0037). The trial was registered at the Clinical Research Information Service of Republic of Korea (No. KCT0005452). No changes were incorporated in the methods following trial commencement.
Participants, Eligibility, and Settings
The inclusion criteria were patients who had undergone CBCT before orthodontic treatment and were diagnosed with maxillary constriction (maxillomandibular transverse differential index values >19.6 mm11), minimum age of 19 years, without missing teeth, and scheduled for MARPE. The exclusion criteria were previous orthodontic treatment history, presence of periodontal disease or history of craniofacial syndrome or deformities, unable to read and comprehend the informed consent, and refusal of study participation.
Consecutive patients indicated for maxillary expansion using MARPE were recruited from September 2019 to November 2021. Of the 36 patients examined, 32 patients fulfilled the selection criteria and agreed to participate in this study.
Interventions
All patients were treated with the MARPE, a modified Hyrax-type expander (Hyrax II; Dentaurum, Ispringen, Germany) that connected to the palate at the para-midsagittal area with four miniscrews (diameter, 1.5 mm; self-drilled type; BMK, Biomaterials Korea, Seoul, Republic of Korea; Figure 1A). After written informed consent was obtained from the patients, they were randomized into two groups (16 patients each): group S: anterior miniscrews of 8-mm length, posterior 6 mm; group L: anterior 13 mm, posterior 11 mm (Figure 1B,C). Following cementation of the MARPE, four miniscrews were inserted perpendicular to the center of the hooks under infiltration anesthesia. The heads of the miniscrews were subsequently attached to the hooks with core resin (Light-Core, BISCO Dental, Schaumburg, Ill).
Figure 1.
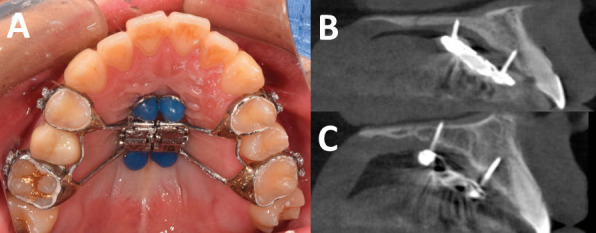
Clinical application of MARPE. (A) Intraoral view. (B, C) Sagittal view in CBCT images. (B) Group S. (C) Group L.
For both groups, 0.2 mm activation of the MARPE per day was performed. After 2 weeks of activation, periapical radiography of the maxillary anterior teeth was performed to evaluate the opening of the midpalatal suture (Figure 2A). In the case of successful suture separation, the expander was activated until the palatal cusps of the maxillary first molar contacted the buccal cusp tips of the mandibular first molar. All expanders were maintained for 3 months following active expansion and then removed. On the day of appliance removal, the resin adhesion between the MARPE's hook and miniscrew was carefully removed, and the stability of the miniscrews was evaluated (Figure 2B). The miniscrews were finally removed after CBCT scan.
Figure 2.
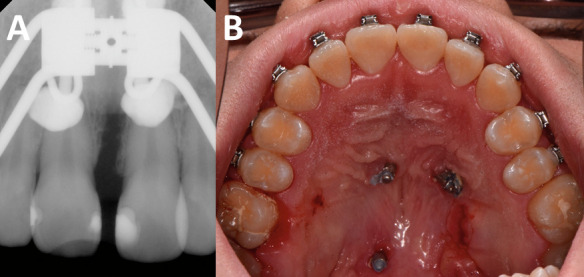
Evaluation of the success of midpalatal suture opening and miniscrews. (A) Periapical radiograph following 2 weeks of expansion. (B) Occlusal view of the miniscrews alone on the day of MARPE removal.
CBCT Imaging and Three-Dimensional Reconstruction
CBCT (Alphard VEGA; ASAHI Roentgen IND, Kyoto, Japan) was set at 80 kV, 5.0 mA, 17 seconds scanning time, 154 × 154-mm field of view, and 0.3-mm voxel size (CBCT panoramic mode, low-dose exposure). CBCT was performed before treatment (T1) and immediately after removal of the MARPE (T2).
The CBCT images were imported as Digital Imaging and Communications in Medicine (DICOM) files. Using the fusion module in the OnDemand3D software (Cybermed, Seoul, Republic of Korea), two CBCT volumes were superimposed using the intensity of the gray levels for each voxel in the anterior cranial base.12
Twelve landmarks were traced according to a previous report, and each landmark was assigned its own coordinates13 (Table 1, Figure 3). The distance between the right and left corresponding landmarks was measured. To compare the change in the inclination of the anchor teeth before and after expansion with MARPE, 4 landmarks were additionally traced on both sides (Figure 4).
Table 1.
Definition of Landmarks Used in This Study
| Landmark |
Description |
| Alare (1,2)a | The most inferolateral point of the nasal aperture in a transverse plane |
| Processus zygomaticus (3,4) | The most inferolateral point of the processus zygomaticus |
| Ectocanine (5,6) | The most inferolateral point on the alveolar ridge opposite the center of the maxillary canine |
| Ectomolare (7,8) | The most inferolateral point on the alveolar ridge opposite the center of the maxillary first molar |
| Furcation (9,10) | Furcation of maxillary first molar's root |
| Central fossa (11,12) | Central fossa of maxillary first molar's crown |
| RMcusp | Cusp tip of the right first molar's mesiobuccal cusp |
| RMapex | Apical third of the right first molar's mesiobuccal root |
| LMcusp | Cusp tip of the left first molar's mesiobuccal cusp |
| LMapex | Apical third of the left first molar's mesiobuccal root |
| RPcusp | Cusp tip of the right first premolar's buccal cusp |
| RPapex | Apical third of the right first premolar's buccal root |
| LPcusp | Cusp tip of the left first premolar's buccal cusp |
| LPapex | Apical third of the left first premolar's buccal root |
The number in the description indicates the number of the landmarks presented in Figure 3.
Figure 3.

Skeletal and dentoalveolar landmarks and coordinate system for linear measurements. See Table 1.
Figure 4.
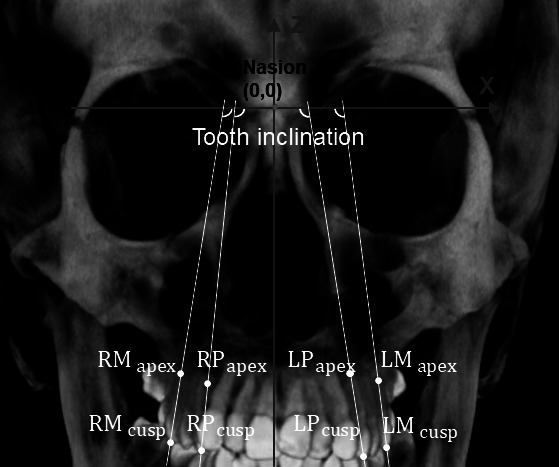
Dental landmarks and coordinate system for angular measurements. See Table 1.
Outcomes
Skeletal and dentoalveolar changes (6 linear measurements and 4 angular measurements) following expansion with MARPE were considered as the primary outcomes (Table 2). The success rate of the midpalatal suture separation and the stability of the miniscrews at the time of the MARPE removal were considered secondary outcomes. There were no changes in the outcome evaluation following trial commencement.
Table 2.
Definition of Parameters Measured in This Studya
| Parameter |
Description |
| Skeletal linear measurements | |
| Interalare width | Linear distance (mm) between the left and right alare (1–2b) |
| Interprocessus zygomaticus width | Linear distance (mm) between the left and right processus zygomaticus (3–4) |
| Dentoalveolar linear measurements | |
| Interectocanine width | Linear distance (mm) between the left and right ectocanine (5–6) |
| Interectomolare width | Linear distance (mm) between the left and right ectomolare (7–8) |
| Interfurcation width | Linear distance (mm) between the left and right furcation of upper first molar (9–10) |
| Intercentral fossa width | Linear distance (mm) between the left and right central fossa of upper first molar (11–12) |
| Dental angular measurements | |
| Right first molar | Inclination (°) of upper right first molar |
| Right first premolar | Inclination (°) of upper right first premolar |
| Left first molar | Inclination (°) of upper left first molar |
| Left first premolar | Inclination (°) of upper left first premolar |
Sample Size Calculation
A power analysis using G*Power (version 3.1.9.4; Franz Faul, Universitat Kiel, Germany) was used to determine the sample size required for the study. Based on the preliminary study,2 a minimum total sample size of 24 (12 for each group) was required with a significance level of 0.05, power of 90%, and effect size of 0.25 for detecting differences in the skeletal and dentoalveolar changes over time within each group. At least 16 patients were included in each group, an addition of 30%, to ensure power of the study in case of any dropouts.
Interim Analyses and Termination Guidelines
No interim analyses were performed, and no termination guidelines were established.
Randomization
A randomization sequence was created using Microsoft Excel 2016 (Microsoft, Redmond, Wash) with a 1:1 allocation using random block sizes of 4 by an independent doctor (Dr Choi). Allocation concealment was achieved with sequentially numbered, opaque, sealed envelopes containing the treatment allocation cards prepared before the trial. The clinical manager (Dr Cha) was responsible for opening the next envelope in sequence and implementing the randomization process.
Blinding
Double blinding was not possible since the operator (Dr Choi) and patients were aware of the length of the miniscrew that was being installed. However, blinding was performed during outcome evaluation.
Error Study
A single examiner (Dr Cha) performed all measurements and repeated them in 30% of the sample following a 30-day interval. The intraexaminer error was assessed using intraclass correlation coefficients.14
Statistical Analysis
All statistical analyses were performed using IBM SPSS software for Windows, version 21.0 (IBM Korea, Seoul, Republic of Korea). Kolmogorov-Smirnov tests were used to verify the normal distribution of the variables. Descriptive statistics, such as the mean and standard deviation, were used to describe the distribution of each variable in the study. Differences in patient characteristics between the groups were analyzed using the χ2, Mann-Whitney U, and independent t-tests. Repeated-measures analysis of variance was used to compare the postexpansion angular and linear changes in each group and between the two groups over time. The success rates of the suture opening and miniscrew were analyzed using the Fisher's exact test.
RESULTS
Participant Flow
Thirty-two healthy adult patients were included in the trial. Only one participant in group S dropped out owing to refusal to undergo CBCT due to pregnancy. Finally, the data of 31 patients (19 males, 12 females) were analyzed in this study. Figure 5 shows the CONSORT flow diagram of the patient allocation and dropout.
Figure 5.
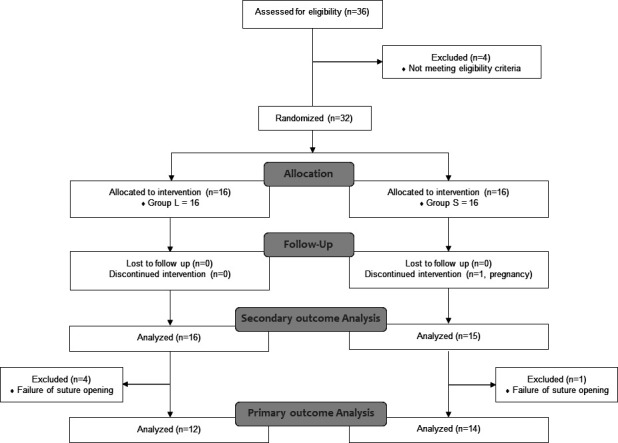
Flow diagram according to CONSORT.
Baseline Data
Baseline characteristics were similar in both groups (Table 3).
Table 3.
Patient Characteristics (N = 31)a
| Variable |
Group L (n = 16) |
Group S (n = 15) |
P Value |
| Age, y | |||
| Range | 19 to 35 | 19 to 30 | |
| Mean (SD) | 23.6 (4.4) | 22.3 (2.6) | .57b |
| Sex, n (%) | .89c | ||
| Female | 6 (37.5) | 6 (40.0) | |
| Male | 10 (62.5) | 9 (60.0) | |
| ANB, ° | |||
| Range | −6.0 to 3.7 | −7.0 to 6.9 | |
| Mean (SD) | −0.6 (3.0) | 0.8 (4.5) | .40b |
| Transverse differential index,11 mm | |||
| Range | 20.3 to 30.9 | 21.9 to 32.7 | |
| Mean (SD) | 25.7 (4.4) | 25.8 (3.9) | .98d |
| Turn, n | |||
| Range | 25 to 40 | 24 to 35 | |
| Mean (SD) | 30.4 (4.2) | 29.9 (3.5) | .72d |
| Duration, mo | |||
| Range | 4.3 to 10 | 4.1 to 7.9 | |
| Mean (SD) | 6.1 (1.6) | 5.6 (1.3) | .45b |
SD, standard deviation; turn, activation number of miniscrew-assisted rapid palatal expansion (MARPE); duration, duration between initial activation and removal of the MARPE appliance (T1–T2).
P value was calculated using Mann-Whitney U-test.
P value was calculated using chi-square test.
P value was calculated using independent t-test.
Number of Patients Analyzed for Each Outcome, Estimation, and Precision and Subgroup Analyses
Group L comprised 16 patients (10 males, 6 females) with a mean age of 23.6 years (standard deviation [SD], 4.4 years), and group S comprised 15 patients (9 males, 6 females) with a mean age of 22.3 years (SD, 2.6 years). Failure of the midpalatal suture to split was observed in 4 of 16 and 1 of 15 patients of groups L and S, respectively. These patients were separately classified into the expansion failure group and excluded from the statistical data set of the primary outcome. All patients in whom the midpalatal suture succeeded in opening were appropriately analyzed in their original assigned groups. No patients were lost to follow-up.
Intraexaminer reliability was considered very good since the intraclass correlation coefficient ranged from 0.894 to 0.999.15
Considering the within-group changes, all linear measurements showed statistically significant increases during the T1-T2 period (time P < .001; Table 4). Only the interprocessus zygomaticus and interectocanine width changes showed statistically significant differences between the groups over time (time × group P = .010 and .001; Table 4).
Table 4.
Skeletal and Dentoalveolar Measurements (Outcome Variable) According to Group (Predictor Variable) in Different Periodsa
|
P Value |
||||||
| Outcome Variable |
T1 |
T2 |
T2–T1 Difference |
Timeb |
Groupb |
Time × Groupb |
| Skeletal linear measurements, mm (SD) | ||||||
| Interalare width | ||||||
| Group L | 16.35 (5.47) | 19.35 (5.60) | 3.00 (0.59) | <.001* | .904 | .270 |
| Group S | 16.83 (6.64) | 19.43 (6.10) | 2.59 (1.13) | <.001* | ||
| Interprocessus zygomaticus width | ||||||
| Group L | 64.85 (3.20) | 68.03 (3.20) | 3.18 (0.88) | <.001* | .773 | .010* |
| Group S | 65.83 (4.92) | 68.02 (4.90) | 2.18 (0.91) | <.001* | ||
| Dentoalveolar linear measurements, mm (SD) | ||||||
| Interectocanine width | ||||||
| Group L | 35.77 (2.62) | 39.47 (2.60) | 3.70 (0.81) | <.001* | .466 | .001* |
| Group S | 35.59 (3.26) | 37.96 (3.05) | 2.38 (0.97) | <.001* | ||
| Interectomolare width | ||||||
| Group L | 57.89 (3.20) | 62.05 (3.11) | 4.16 (0.94) | <.001* | .956 | .435 |
| Group S | 58.02 (3.83) | 61.78 (3.43) | 3.76 (1.48) | <.001* | ||
| Interfurcation width | ||||||
| Group L | 45.78 (2.59) | 50.63 (2.52) | 4.85 (0.78) | <.001* | .760 | .525 |
| Group S | 45.52 (3.55) | 50.14 (3.31) | 4.62 (1.02) | <.001* | ||
| Intercentral fossa width | ||||||
| Group L | 46.71 (3.46) | 52.94 (3.77) | 6.22 (1.42) | <.001* | .930 | .744 |
| Group S | 46.48 (3.34) | 52.53 (3.80) | 6.05 (1.01) | <.001* | ||
| Dental angular measurements, ° (SD) | ||||||
| Right first molar | ||||||
| Group L | 97.06 (5.06) | 97.36 (5.99) | 0.30 (2.81) | .717 | .999 | .090 |
| Group S | 96.05 (4.72) | 98.38 (5.18) | 2.33 (3.00) | .012* | ||
| Right first premolar | ||||||
| Group L | 95.28 (3.96) | 97.03 (3.66) | 1.75 (2.26) | .021* | .462 | .687 |
| Group S | 96.61 (4.71) | 97.94 (3.60) | 1.33 (2.85) | .103 | ||
| Left first molar | ||||||
| Group L | 95.54 (5.12) | 97.53 (4.42) | 1.99 (3.51) | .075 | .820 | .354 |
| Group S | 95.61 (5.05) | 96.58 (5.25) | 0.97 (1.88) | .075 | ||
| Left first premolar | ||||||
| Group L | 94.94 (4.10) | 97.28 (4.63) | 2.33 (2.59) | .154 | .278 | .649 |
| Group S | 97.33 (4.63) | 98.84 (5.96) | 1.52 (3.67) | .145 | ||
Data are presented as mean (standard deviation).
By repeated-measures analysis of variances.
P < .05.
In both groups, four anchor teeth showed increased buccal inclination (with a large standard deviation), which was statistically significant only for the right first molar in group S and the right first premolar in group L (Table 4). There was no statistically significant difference when comparing the change in the inclination of each anchor tooth between the groups over time (Table 4).
The overall success rate of suture opening was 83.9% (26 of 31); the success rates of groups L and S were 75% and 93.3%, respectively; which was not significantly different (Table 5). The anterior miniscrews showed high success rates regardless of the group (Table 5). For posterior miniscrews, group L showed a high success rate of 96.9%, whereas group S showed a relatively low success rate of 76.7%, showing a statistically significant difference (P = .024; Table 5).
Table 5.
Success Rate of Suture Opening and of the Miniscrewsa
|
|
Group L |
Group S |
P Value |
| Suture opening, n (%) | |||
| Success | 12 (75.0) | 14 (93.3) | .33 |
| Failure | 4 (25.0) | 1 (6.7) | |
| Miniscrew, n (%) | |||
| Anterior | |||
| Success | 31 (96.9) | 29 (96.7) | >.99 |
| Failure | 1 (3.1) | 1 (3.3) | |
| Posterior | |||
| Success | 31 (96.9) | 23 (76.7) | .024* |
| Failure | 1 (3.1) | 7 (23.3) | |
Success of the miniscrew was evaluated for both right and left sides. P values were calculated using Fisher's exact test.
P < .05.
Complications
No notable complications, such as moderate to severe pain, gingival recession, bone dehiscence, and so forth, were observed in the participants of this study. Since the interval between CBCT scans was relatively short, the CBCT panoramic mode, a small field of view CBCT with low-dose exposure, was taken.16 The participants in this study did not show any abnormal signs except for a slight thickening of the mucous membrane as the miniscrew penetrated the nasal floor when viewing the CBCT after removal of MARPE.
DISCUSSION
In this study, expansion was assessed by the positional changes of previously reported anatomical landmarks.13,17 However, some landmarks (anterior nasal spine, point A, prosthion) were excluded because they are hard to measure on the CBCT images since the midpalatal suture was ossified at T2. Both groups showed significant transverse expansion between T1 and T2 (Table 4). In addition, the amount of expansion decreased from the upper first molar to the alare resulting in a pyramidal expansion pattern in the coronal aspect.6,17,18 In group L, the expansion amount was generally large; however, only the interprocessus zygomaticus and interectocanine width changes were statistically significant compared with group S. Skeletal expansion at the maxillary basal bone level (interprocessus zygomaticus width change; Table 4) accounted for 36% and 51% of total screw expansion (turn number × 0.2 mm; Table 3) in groups S and L, respectively, similar to previous studies.17,19 Therefore, in this study, MARPE expansion with longer miniscrews led to higher skeletal expansion in patients in whom the suture opening was successful. There was no significant difference in interectomolare width change between the two groups, but the interectocanine width in group L was expanded by about 1.3 mm more than in group S and was statistically significant. The use of MARPE with longer miniscrews can be beneficial to the expansion of the canine alveolar bone. It can help increase the intercanine width or improve V-shaped arches. Since the upper first molars were firmly fixed as anchor teeth to the MARPE, no significant difference was observed in the amount of change in intermolar width between the two groups at the furcation or crown level.
Radiologic midpalatal suture opening was observed in 83.9% of the patients, which is relatively low compared with previous studies.9,20 In this study, the higher mean and upper limit of the patient's age (mean, 23.0 years; range, 19–35 years) could have resulted in the lower success rate.21 Groups L and S showed a success rate of 75.0% and 93.3%, which was not statistically significantly different. According to previous FEA, the stress distribution of the maxilla by MARPE was not affected by the miniscrew length, and the group with short miniscrews showed the greatest overall stress in the paramedian area, which could be more effective in the midpalatal suture split.10 Therefore, MARPE with longer miniscrews does not guarantee successful midpalatal suture opening.22
The high success rate of the anterior miniscrews suggests that the anterior portion of the palatal bone is a predictable region for miniscrew stability regardless of the length of the miniscrew in MARPE.23 The success rates of the posterior miniscrews were statistically significantly different (Table 5). In group L, an increase in bone contact and bicortical engagement (Figure 1C) due to the use of longer miniscrews appears to increase the stability of the miniscrews.9 Therefore, long posterior miniscrews (more than 6 mm) should be considered for miniscrew stability.
Buccal tipping of the anchor teeth seems inevitable owing to the initial, large expansion force applied to the teeth in tooth-bone–borne MARPE.4 In this study, as expected, buccal tipping of the anchor teeth occurred on average, and the mean value was 1–2°, which was similar to previous reports.3,17,19 There was no difference between the groups; however, this finding should be cautiously interpreted owing to intragroup variability.24
Limitation of the Study
This was a single-center study, and double blinding was not possible due to the clinical limitations. Further studies with long-term follow-up periods are warranted to determine whether the difference in the amount of expansion is also significant following orthodontic treatment and in the maintenance phase.
Generalization
Results from this RCT can be generalized only to young adults who meet the inclusion criteria. The generalization of the results should be limited only to devices similar to the MARPE design used in this study (including the number and length of miniscrews).
CONCLUSIONS
MARPE with longer miniscrews can increase the amount of expansion of the maxillary basal bone and canine alveolar bone.
The use of a long miniscrew for posterior anchorage of MARPE increases the stability of the miniscrew.
MARPE with longer miniscrews does not guarantee midpalatal suture separation success.
REFERENCES
- 1.Lee KJ, Park YC, Park JY, Hwang WS. Miniscrew-assisted nonsurgical palatal expansion before orthognathic surgery for a patient with severe mandibular prognathism. Am J Orthod Dentofacial Orthop . 2010;137:830–839. doi: 10.1016/j.ajodo.2007.10.065. [DOI] [PubMed] [Google Scholar]
- 2.Choi SH, Shi KK, Cha JY, Park YC, Lee KJ. Nonsurgical miniscrew-assisted rapid maxillary expansion results in acceptable stability in young adults. Angle Orthod . 2016;86:713–720. doi: 10.2319/101415-689.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lim HM, Park YC, Lee KJ, Kim KH, Choi YJ. Stability of dental, alveolar, and skeletal changes after miniscrew-assisted rapid palatal expansion. Korean J Orthod . 2017;47:313–322. doi: 10.4041/kjod.2017.47.5.313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Seong EH, Choi SH, Kim HJ, Yu HS, Park YC, Lee KJ. Evaluation of the effects of miniscrew incorporation in palatal expanders for young adults using finite element analysis. Korean J Orthod . 2018;48:81–89. doi: 10.4041/kjod.2018.48.2.81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Copello FM, Marañón-Vásquez GA, Brunetto DP, et al. Is the buccal alveolar bone less affected by mini-implant assisted rapid palatal expansion than by conventional rapid palatal expansion? A systematic review and meta-analysis. Orthod Craniofac Res . 2020;23:237–249. doi: 10.1111/ocr.12374. [DOI] [PubMed] [Google Scholar]
- 6.Lin L, Ahn HW, Kim SJ, Moon SC, Kim SH, Nelson G. Tooth-borne vs bone-borne rapid maxillary expanders in late adolescence. Angle Orthod . 2015;85:253–262. doi: 10.2319/030514-156.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Brunetto DP, Sant'Anna EF, Machado AW, Moon W. Non-surgical treatment of transverse deficiency in adults using microimplant-assisted rapid palatal expansion (MARPE) Dental Press J Orthod . 2017;22:110–125. doi: 10.1590/2177-6709.22.1.110-125.sar. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yoon A, Guilleminault C, Zaghi S, Liu SY. Distraction osteogenesis maxillary expansion (DOME) for adult obstructive sleep apnea patients with narrow maxilla and nasal floor. Sleep Med . 2020;65:172–176. doi: 10.1016/j.sleep.2019.06.002. [DOI] [PubMed] [Google Scholar]
- 9.Lee RJ, Moon W, Hong C. Effects of monocortical and bicortical mini-implant anchorage on bone-borne palatal expansion using finite element analysis. Am J Orthod Dentofacial Orthop . 2017;151:887–897. doi: 10.1016/j.ajodo.2016.10.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yoon S, Lee DY, Jung SK. Influence of changing various parameters in miniscrew-assisted rapid palatal expansion: a three-dimensional finite element analysis. Korean J Orthod . 2019;49:150–160. doi: 10.4041/kjod.2019.49.3.150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Vanarsdall RL., Jr Transverse dimension and long-term stability. Semin Orthod . 1999;5:171–180. doi: 10.1016/s1073-8746(99)80008-5. [DOI] [PubMed] [Google Scholar]
- 12.Weissheimer A, Menezes LM, Koerich L, Pham J, Cevidanes LH. Fast three-dimensional superimposition of cone beam computed tomography for orthopaedics and orthognathic surgery evaluation. Int J Oral Maxillofac Surg . 2015;44:1188–1196. doi: 10.1016/j.ijom.2015.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Magnusson A, Bjerklin K, Kim H, Nilsson P, Marcusson A. Three-dimensional assessment of transverse skeletal changes after surgically assisted rapid maxillary expansion and orthodontic treatment: a prospective computerized tomography study. Am J Orthod Dentofacial Orthop . 2012;142:825–833. doi: 10.1016/j.ajodo.2012.08.015. [DOI] [PubMed] [Google Scholar]
- 14.Fleiss JL. Analysis of data from multiclinic trials. Control Clin Trials . 1986;7:267–275. doi: 10.1016/0197-2456(86)90034-6. [DOI] [PubMed] [Google Scholar]
- 15.Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med . 2016;15:155–163. doi: 10.1016/j.jcm.2016.02.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Shin HS, Nam KC, Park H, Choi HU, Kim HY, Park CS. Effective doses from panoramic radiography and CBCT (cone beam CT) using dose area product (DAP) in dentistry. Dentomaxillofac Radiol . 2014;43:20130439. doi: 10.1259/dmfr.20130439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Park JJ, Park YC, Lee KJ, Cha JY, Tahk JH, Choi YJ. Skeletal and dentoalveolar changes after miniscrew-assisted rapid palatal expansion in young adults: a cone-beam computed tomography study. Korean J Orthod . 2017;47:77–86. doi: 10.4041/kjod.2017.47.2.77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Song KT, Park JH, Moon W, Chae JM, Kang KH. Three-dimensional changes of the zygomaticomaxillary complex after mini-implant assisted rapid maxillary expansion. Am J Orthod Dentofacial Orthop . 2019;156:653–662. doi: 10.1016/j.ajodo.2018.11.019. [DOI] [PubMed] [Google Scholar]
- 19.Li N, Sun W, Li Q, Dong W, Martin D, Guo J. Skeletal effects of monocortical and bicortical mini-implant anchorage on maxillary expansion using cone-beam computed tomography in young adults. Am J Orthod Dentofacial Orthop . 2020;157:651–661. doi: 10.1016/j.ajodo.2019.05.021. [DOI] [PubMed] [Google Scholar]
- 20.Bazargani F, Lund H, Magnuson A, Ludwig B. Skeletal and dentoalveolar effects using tooth-borne and tooth-bone-borne RME appliances: a randomized controlled trial with 1-year follow-up. Eur J Orthod . 2021;43:245–253. doi: 10.1093/ejo/cjaa040. [DOI] [PubMed] [Google Scholar]
- 21.Shin H, Hwang CJ, Lee KJ, Choi YJ, Han SS, Yu HS. Predictors of midpalatal suture expansion by miniscrew-assisted rapid palatal expansion in young adults: a preliminary study. Korean J Orthod . 2019;49:360–371. doi: 10.4041/kjod.2019.49.6.360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Oliveira CB, Ayub P, Angelieri F, et al. Evaluation of factors related to the success of miniscrew-assisted rapid palatal expansion. Angle Orthod . 2021;91:187–194. doi: 10.2319/051420-436.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Karagkiolidou A, Ludwig B, Pazera P, Gkantidis N, Pandis N, Katsaros C. Survival of palatal miniscrews used for orthodontic appliance anchorage: a retrospective cohort study. Am J Orthod Dentofacial Orthop . 2013;143:767–772. doi: 10.1016/j.ajodo.2013.01.018. [DOI] [PubMed] [Google Scholar]
- 24.Rungcharassaeng K, Caruso JM, Kan JY, Kim J, Taylor G. Factors affecting buccal bone changes of maxillary posterior teeth after rapid maxillary expansion. Am J Orthod Dentofacial Orthop . 2007;132:428.e1–428.e4288. doi: 10.1016/j.ajodo.2007.02.052. [DOI] [PubMed] [Google Scholar]