

Abstract
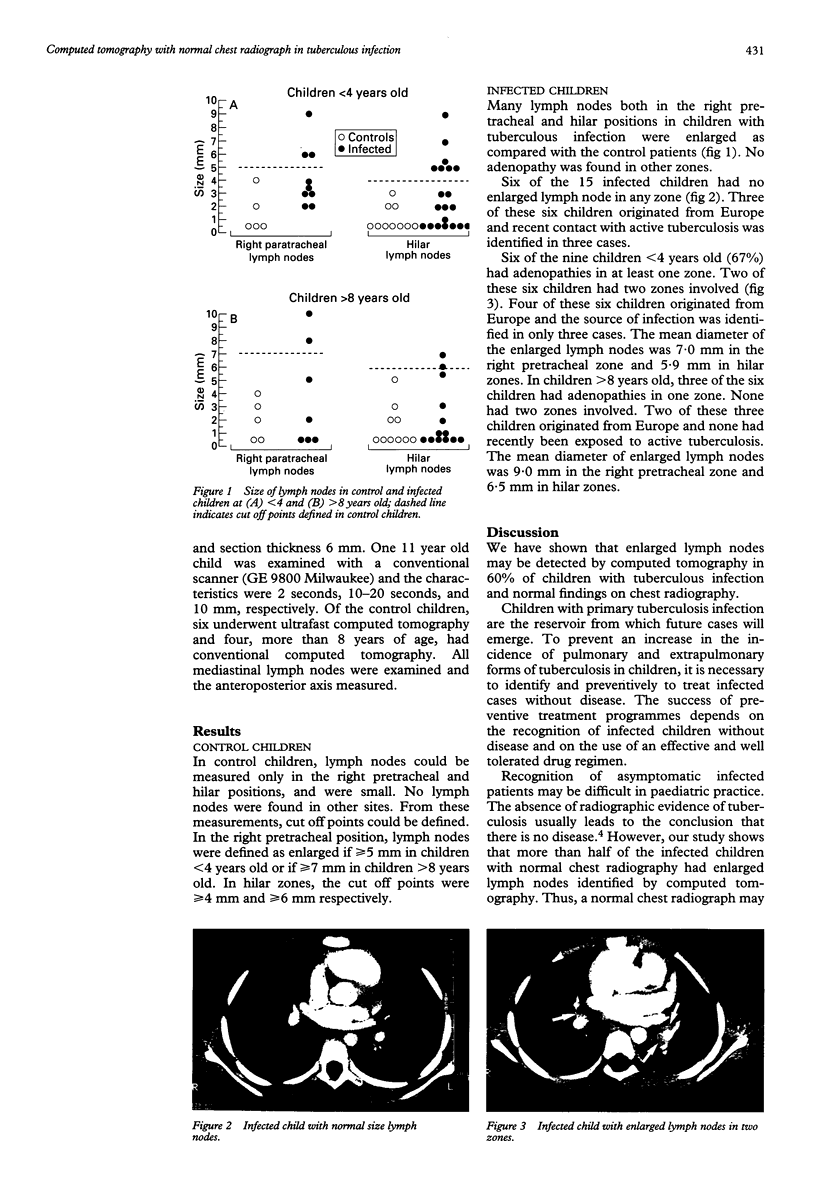
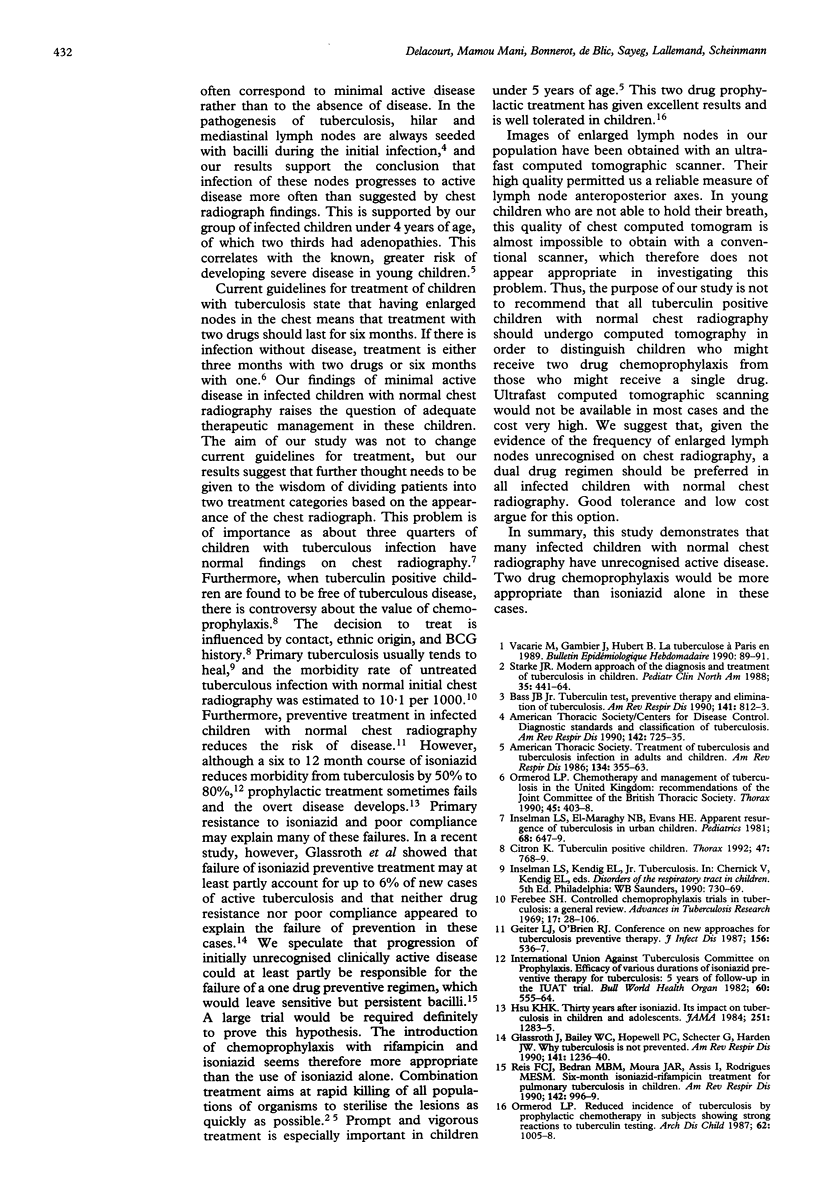
Children with primary tuberculosis infection without disease must be identified and treated preventively to avoid an increase in the incidence of tuberculosis in children. However, the recognition of infected cases without disease is often difficult. In particular, minimal active disease may be present in many cases but unrecognised on chest radiography. Computed tomography was therefore performed in 15 children with tuberculous infection and a normal chest radiograph to measure the size of their mediastinal lymph nodes. Ten control children without tuberculosis were also evaluated. When compared with controls it was found that nine of 15 (60%) infected children had enlarged lymph nodes. Adenopathies were more frequent in infected children less than 4 years old than in those over 8 years old. The demonstration of unrecognised active disease in many infected children raises the question of the adequate treatment for these children. It is proposed that a two drug regimen would be more appropriate than isoniazid alone in these cases.
Full text
PDF
Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bass J. B., Jr Tuberculin test, preventive therapy, and elimination of tuberculosis. Am Rev Respir Dis. 1990 Apr;141(4 Pt 1):812–813. doi: 10.1164/ajrccm/141.4_Pt_1.812. [DOI] [PubMed] [Google Scholar]
- Chemotherapy and management of tuberculosis in the United Kingdom: recommendations of the Joint Tuberculosis Committee of the British Thoracic Society. Thorax. 1990 May;45(5):403–408. doi: 10.1136/thx.45.5.403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Citron K. Tuberculin positive children. Thorax. 1992 Oct;47(10):768–769. doi: 10.1136/thx.47.10.768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geiter L. J., O'Brien R. J. From the Centers for Disease Control. Conference on new approaches for tuberculosis preventive therapy. J Infect Dis. 1987 Sep;156(3):536–537. doi: 10.1093/infdis/156.3.536. [DOI] [PubMed] [Google Scholar]
- Glassroth J., Bailey W. C., Hopewell P. C., Schecter G., Harden J. W. Why tuberculosis is not prevented. Am Rev Respir Dis. 1990 May;141(5 Pt 1):1236–1240. doi: 10.1164/ajrccm/141.5_Pt_1.1236. [DOI] [PubMed] [Google Scholar]
- Hsu K. H. Thirty years after isoniazid. Its impact on tuberculosis in children and adolescents. JAMA. 1984 Mar 9;251(10):1283–1285. doi: 10.1001/jama.251.10.1283. [DOI] [PubMed] [Google Scholar]
- Inselman L. S., El-Maraghy N. B., Evans H. E. Apparent resurgence of tuberculosis in urban children. Pediatrics. 1981 Nov;68(5):647–649. [PubMed] [Google Scholar]
- Ormerod L. P. Reduced incidence of tuberculosis by prophylactic chemotherapy in subjects showing strong reactions to tuberculin testing. Arch Dis Child. 1987 Oct;62(10):1005–1008. doi: 10.1136/adc.62.10.1005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reis F. J., Bedran M. B., Moura J. A., Assis I., Rodrigues M. E. Six-month isoniazid-rifampin treatment for pulmonary tuberculosis in children. Am Rev Respir Dis. 1990 Nov;142(5):996–999. doi: 10.1164/ajrccm/142.5.996. [DOI] [PubMed] [Google Scholar]
- Starke J. R. Modern approach to the diagnosis and treatment of tuberculosis in children. Pediatr Clin North Am. 1988 Jun;35(3):441–464. doi: 10.1016/s0031-3955(16)36465-3. [DOI] [PubMed] [Google Scholar]