

A 37-year-old male patient presented with subacute paraparesis, urinary incontinence, and a sensory level of T8. An analysis of the cerebrospinal fluid revealed lymphocytic pleocytosis (5 white blood cells/mm 3 ), low levels of glucose (25 mg/dL), increased levels of protein (713 mg/dL), high levels of lactic acid (4.7 mmol/L), and positive cryptococcal antigen. A magnetic resonance imaging (MRI) scan showed hydrocephalus ( Figure 1 ), myelopathy ( Figure 2 ), and adhesive arachnoiditis ( Figure 3 ). Meningeal biopsy showed round cells suggestive of cryptococcosis ( Figure 4 ), without species differentiation in the culture samples. Cryptococcus may exhibit unique clinical manifestations, such as gelatinous pseudocysts in the basal ganglia, cerebral cryptococcomas, leptomeningitis, cranial neuropathies, adhesive arachnoiditis, and obstructive hydrocephalus. 1 2 3 4 5
Figure 1.
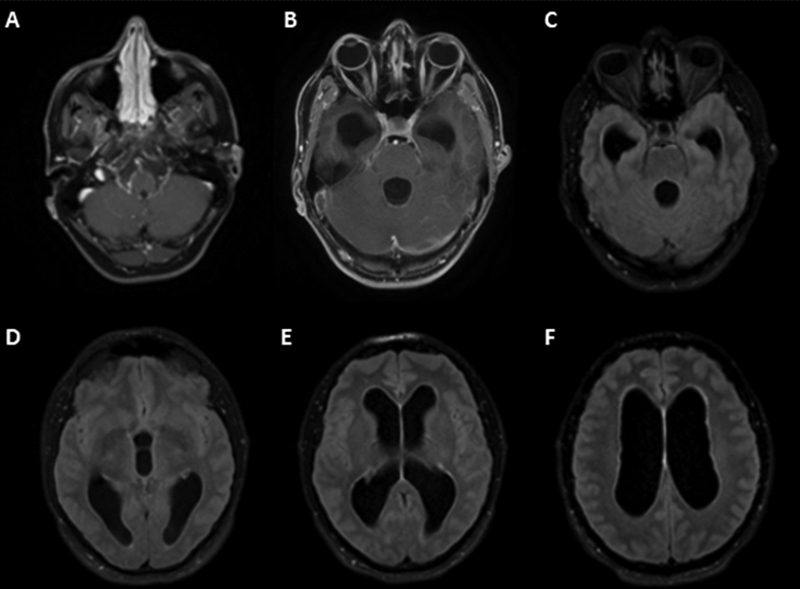
( A,B ) Axial contrast-enhanced T1-weighted magnetic resonance imaging (MRI) scan revealing leptomeningeal enhancement at the base of the brain in the posterior fossa; ( C–F ) axial fluid-attenuated inversion recovery (FLAIR) MRI showing hydrocephalus throughout the ventricular system, without significant transudation of the cerebrospinal fluid.
Figure 2.
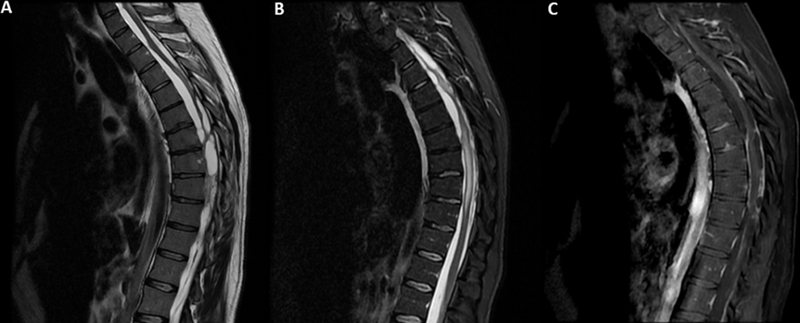
( A ) Sagittal T2-weighted MRI showing septations in the subarachnoid space around the spinal cord; ( B ) sagittal short-tau inversion recovery (STIR) MRI showing hyperintensity and distortion in the spinal cord; ( C ) sagittal contrast-enhanced T1-weighted MRI revealing leptomeningeal enhancement around the entire spinal canal.
Figure 3.
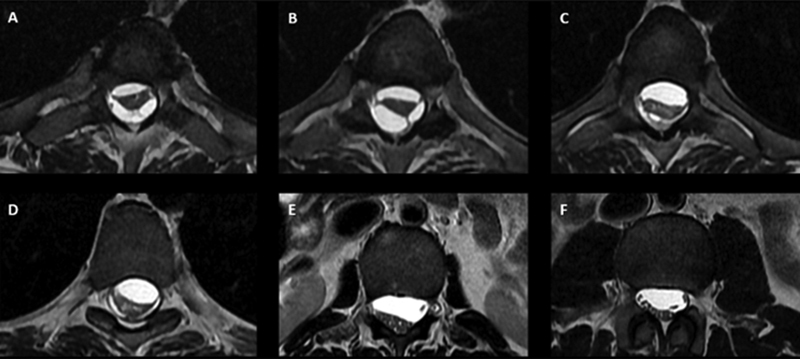
( A–D ): Axial T2-weighted MRI showing adhesive arachnoiditis and septations distorting the spinal cord at the level of the thoracic spinal cord; ( E,F ) axial T2-weighted MRI showing adhesive arachnoiditis and septations distorting the spinal cord at the level of the lumbosacral spinal cord.
Figure 4.
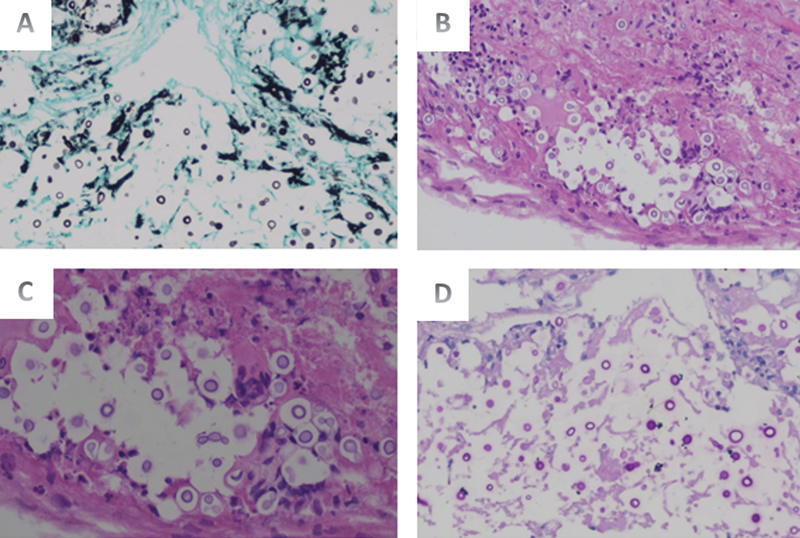
Encapsulated, spherical-to-oval yeast cells (5–10 μm in diameter) with narrow-based budding and polysaccharide capsules. The yeast cells vary in size, and the organisms can be capsule-deficient. ( A ) Grocott methenamine silver (GMS), smallest increase (×20); yeast cells tested positive for GMS; ( B ) hematoxylin and eosin staining, the smallest increase (×20); ( C ) periodic acid Schiff–diastase (PAS‒D), highest magnification (×40); yeast cells tested positive for PAS‒D staining; ( D ) PAS‒D, smallest increase (×20).
Acknowledgments
We would like to thank the Neurosurgery Service at Hospital de Clínicas (HC), Universidade Federal do Paraná (UFPR), Curitiba, Brazil), which provided assistance in the meningeal biopsy of the patient.
Conflict of Interest The authors have no conflict of interest to declare.
Authors' Contributions
All authors contributed to the conception and design of the study. AEAF: performed material preparation, data collection and analysis, and wrote the first draft of the manuscript, and all authors commented on previous versions and read and approved the final manuscript.
References
- 1.Maziarz E K, Perfect J R. Cryptococcosis. Infect Dis Clin North Am. 2016;30(01):179–206. doi: 10.1016/j.idc.2015.10.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Eshwara V K, Garg R, Chandrashekhar G S, Shaw T, Mukhopadhyay C. Fatal Cryptococcus gattii meningitis with negative cryptococcal antigen test in a HIV-non-infected patient . Indian J Med Microbiol. 2018;36(03):439–440. doi: 10.4103/ijmm.IJMM_18_164. [DOI] [PubMed] [Google Scholar]
- 3.Grosse P, Tintelnot K, Söllner O, Schmitz B. Encephalomyelitis due to Cryptococcus neoformans var gattii presenting as spinal tumour: case report and review of the literature. J Neurol Neurosurg Psychiatry. 2001;70(01):113–116. doi: 10.1136/jnnp.70.1.113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Agrawal A, Agrawal A, Agrawal C, Rohtagi A. An unusual spinal arachnoiditis. Clin Neurol Neurosurg. 2006;108(08):775–779. doi: 10.1016/j.clineuro.2005.09.007. [DOI] [PubMed] [Google Scholar]
- 5.Panackal A A, Komori M, Kosa P. Spinal arachnoiditis as a complication of cryptococcal meningoencephalitis in non-HIV previously healthy adults. Clin Infect Dis. 2017;64(03):275–283. doi: 10.1093/cid/ciw739. [DOI] [PMC free article] [PubMed] [Google Scholar]