

This cross-sectional study examines the association of ambient temperature with the prevalence of intimate partner violence among partnered women, aged 15 to 49 years, in low- and middle-income countries in South Asia and also projects the association of future climate warming with intimate partner violence.
Key Points
Question
What is the association of ambient temperature with the prevalence of intimate partner violence (IPV) among partnered women in 3 low- and middle-income countries in South Asia (India, Nepal, and Pakistan)?
Findings
This cross-sectional study of 194 871 ever-partnered women aged 15 to 49 years from 3 South Asian countries found an increase in IPV prevalence with higher annual mean temperature, with a 1 °C increase in the annual mean temperature associated with a 4.5% increase in IPV prevalence. By the end of the 21st century, the prevalence of IPV was estimated to increase substantially as temperatures increase, particularly under an unlimited carbon emissions scenario.
Meaning
The findings of this study suggest a need for sustainable climate change mitigation and adaptation strategies, along with public health programs, to address the issue of IPV in climate-sensitive regions.
Abstract
Importance
Intimate partner violence (IPV), including physical, sexual, and emotional violence, constitutes a critical public health problem, particularly in low- and middle-income countries. While climate change could escalate violent events, data quantifying its possible association with IPV are scant.
Objective
To evaluate the association of ambient temperature with the prevalence of IPV among partnered women in low- and middle-income countries in South Asia, and to estimate the association of future climate warming with IPV.
Design, Setting, and Participants
This cross-sectional study used data from the Demographic and Health Survey and included 194 871 ever-partnered women aged 15 to 49 years from 3 South Asian countries (India, Nepal, and Pakistan). The study applied the mixed-effect multivariable logistic regression model to investigate the association of ambient temperature with IPV prevalence. The study further modeled the change in IPV prevalence under various future climate change scenarios. The data included in the analyses were collected from October 1, 2010, to April 30, 2018, and the current analyses were performed from January 2, 2022, to July 11, 2022.
Exposure
Annual ambient temperature exposure for each woman, estimated based on an atmospheric reanalysis model of the global climate.
Main Outcomes and Measures
The prevalence of IPV and its types (physical, sexual, and emotional violence) were assessed based on self-reported questionnaires from October 1, 2010, to April 30, 2018, and the changes in the prevalence with climate changes were estimated through the 2090s.
Results
The study included 194 871 ever-partnered women aged 15 to 49 years (mean [SD] age, 35.4 [7.6] years; overall IPV prevalence, 27.0%) from 3 South Asian countries. The prevalence of physical violence was highest (23.0%), followed by emotional (12.5%), and sexual violence (9.5%). The annual temperature ranges were mostly between 20 °C and 30 °C. A significant association was found between high ambient temperature and the prevalence of IPV against women, with each 1 °C increase in the annual mean temperature associated with a mean increase in IPV prevalence of 4.49% (95% CI, 4.20%-4.78%). According to the study’s projections under the unlimited emissions scenarios (SSPs [shared socioeconomic pathways], as defined by the Intergovernmental Panel on Climate Change] 5-8.5), IPV prevalence would increase by 21.0% by the end of the 21st century, while it would only moderately increase under increasingly stricter scenarios (SSP2-4.5 [9.8%] and SSP1-2.6 [5.8%]). In addition, the projected increases in the prevalence of physical (28.3%) and sexual (26.1%) violence were greater than that of emotional violence (8.9%). In the 2090s, India was estimated to experience the highest IPV prevalence increase (23.5%) among the 3 countries, compared with Nepal (14.8%) and Pakistan (5.9%).
Conclusions and Relevance
This cross-sectional, multicountry study provides ample epidemiological evidence to support that high ambient temperature may be associated with the risk of IPV against women. These findings highlight the vulnerabilities and inequalities of women experiencing IPV in low- and middle-income countries in the context of global climate warming.
Introduction
Intimate partner violence (IPV) is a critical public health issue that threatens women’s human rights and undermines the achievement of the United Nations Sustainable Development Goals.1,2 Estimates3,4 suggest that up to 30% of ever-partnered women have experienced either physical or sexual violence or both, in their lifetime, with notably higher incidences in low- and middle-income countries (LMICs). Intimate partner violence can lead to multiple severe health consequences for women, including mental health problems, physical injury, adverse birth outcomes, and even death.5,6 Interrelated risk factors, which can interact in complex ways with legal, economic, and cultural systems, are contributing factors to IPV.
Climate factors have been suggested as possible contributors to violence. The heat-aggression hypothesis proposes that hot temperatures increase violent behaviors through various biological and psychological processes,7 such as triggering angry feelings, aggressive thoughts, and physiological arousal,8 or modifying daily activities to create more social interaction situations.9 Additionally, proximity to the equator is associated with a quicker life pace, and lower focus on self-control, which may lead to greater aggressiveness.10 Mounting evidence11,12 linking ambient temperature and violence supports that heat exposure has the potential to increase the risk of IPV. However, few studies have quantitatively explored the role of ambient temperature in IPV risk.
Climate change has been increasingly portrayed as the greatest public health threat to human society in the 21st century. Growing evidence11,13,14 suggests that climate change has strong causal influences on various types of violence. Climate change may limit agricultural productivity and economic development, inducing family financial crises and violent events.15,16 Also, hot weather events can aggravate certain mental disorders (eg, anxiety, schizophrenia), and increase people’s aggressive tendencies.17 Therefore, it could be reasonably hypothesized that further climate change may exacerbate the burden of IPV. However, to our knowledge, no previous studies have quantified such possible associations.
Given the higher prevalence of IPV in South Asia compared with that at the global level, and the region’s history of more frequent and intense heat waves in the last 30 years,3,18 this study was designed to evaluate the association of ambient temperature with the prevalence of IPV and its types (physical, sexual, and emotional violence) among partnered women. Additionally, the study aimed to project the association of future warming with IPV prevalence under different climate scenarios in South Asia.
Methods
Data Sources
This cross-sectional study used data from the Demographic and Health Surveys (DHS)19 that were georeferenced and available for domestic violence in 3 LMICs in South Asia (India, Nepal, and Pakistan) from 2000 to 2018. The DHS were routinely conducted (3- to 5-year intervals) in more than 90 LMICs worldwide, collecting health and sociodemographic information at the household level (details of the surveys and variables are given in the eAppendix in Supplement 1).
Data on domestic violence were derived from the DHS module of questionnaires about IPV, including physical, sexual, and emotional violence. With the respondents’ consent, all ever-partnered women aged 15 to 49 years were interviewed by trained fieldwork staff about their experience of IPV in the past 12 months. The interview questions are given in the eAppendix in Supplement 1, and the data inclusion and exclusion processes are summarized in eFigure 1 in Supplement 1. This analysis included 4 DHS from the 3 South Asian countries (eTable 1 in Supplement 1). The publicly available population data used in this study have been reviewed and approved by the Institutional Review Board of ICF International Inc. Written consent was obtained from the participants. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross-sectional studies.
Historical Meteorological Parameters, Population, and Economic Data
In this study, the historical meteorological parameters were obtained from the ERA5 (the fifth-generation ECMWF [European Centre for Medium-Range Weather Forecasts] atmospheric reanalysis of the global climate).20 Land variables, including 2m temperature (temperature of air at 2 m above the surface of land) and total precipitation, with latitude-longitude grids at 0.25° × 0.25° (28 km × 28 km) resolution and time frequency over 1 hour were provided in the database. We calculated the daily mean temperature and daily cumulative precipitation from January 1, 2009, to December 31, 2018, and matched the data to the geocoded addresses of clusters where the women’s households were located. A cluster is defined in the DHS as a group of adjacent households, which serves as the primary sampling unit for field work efficiency in the 2-stage cluster sampling procedure. Finally, daily-level parameters were aggregated into annual mean (for temperatures) or annual cumulative (for precipitations) over the year prior to the interview day. Although data were collected from October 1, 2000, to April 30, 2018, only surveys from October 1, 2010, on were analyzed because data on IPV experience in the past year were not collected before then. The current analyses were performed from January 2, 2022, to July 11, 2022.
The population of reproductive women aged 15 to 49 years was derived from WorldPop21 at a resolution of 1 km and was aggregated into city and country levels. The gross domestic product (GDP) per capita with a resolution of 30 arc seconds was obtained from a gridded global data set for GDP.22
Future Meteorological Parameters and Population Data
The predicted daily mean temperature series under different climate scenarios were obtained from the Coupled Model Intercomparison Project sixth phase.23 We extracted daily mean temperature series from 10 global climate model data sets for the baseline (January 1, 1985-December 31, 2014) and future (January 1, 2015-December 31, 2099) periods under scenarios (shared socioeconomic pathways [SSPs]) as defined by the Intergovernmental Panel on Climate Change.23 The SSPs correspond to the increasing trajectories of atmospheric greenhouse gas (GHG) concentrations and characterize a range of warming in global climate from mild to extreme.23 For this study we used 3 SSPs, categorized as strict (SSP1-2.6; lowest projected change), medium (SSP2-4.5), and unrestricted (SSP5-8.5; highest projected change) GHG emissions,23 with SSP5-8.5 implying unlimited energy consumption, GHG emissions, and population growth. The process of converting gridded temperature to the city level and detailed information of the future population are given in the eAppendix in Supplement 1.
Statistical Analysis
Temperature-IPV Association
We applied a multivariable mixed-effects logistic regression model to quantitatively assess the association of annual mean temperature with the prevalence of IPV and its 3 types (physical, sexual, and emotional) in the past 12 months under a linear association assumption. The associations were adjusted by sociodemographic factors (residence type, woman’s and partner’s age, and marital status), socioeconomic status (woman’s and partner’s educational levels, floor material, roof material, household wealth status), and cluster-level (population density, GDP per capita, and annual cumulative precipitation) variables. To further account for location-specific factors and better isolate the temperature effect, we included a random-effect term of cluster in the main model. The association was presented as a percentage change of IPV prevalence and its 95% CI per a 1 °C increment in the annual mean temperature. We also checked the linearity of temperature-IPV association by comparing the linear and nonlinear models. Detailed information for covariates, effect estimation, and linear assumption testing are provided in the eAppendix in Supplement 1.
We conducted several stratified analyses to explore how the association of annual temperatures with IPV prevalence differed by region, wealth level, floor material, roof material, marital status, ages of the women and their partners, and educational level. To examine the robustness of the associations, we performed several sensitivity analyses, including the use of varied model covariates, mean temperature during the hottest 3 consecutive months as the exposure, and future population change in the projection. Details of stratified analyses and sensitivity analyses are described in the eAppendix in Supplement 1.
Projection of Changes in IPV Prevalence Associated with Climate Warming
Assuming a linear association between annual temperatures and IPV prevalence, we calculated the excess cases of IPV associated with nonoptimum temperature in each city as follows:
| Excess Casesci = Popci × Rateco × ERCco × ΔT, |
where Excess casesci indicates the IPV cases in relation to the annual temperature increase at the city level, Popci is the city population size of women aged 15 to 49 years at baseline, Rateco means the baseline IPV prevalence in the corresponding country, ERCco denotes the percentage change of IPV prevalence along with change in annual temperature increment in the specific country, and ΔT represents the change in future temperature compared with the baseline period (1985-2014). We aggregated the gridded population and projected temperature series at the city level. Finally, we calculated the percentage change of IPV prevalence associated with future climate warming for each country as follows:
| ΔPrevalencecs% = [Excess Casesco / (Popco × Prevalenceco)] × 100%, |
where Excess Casescs denotes the projected excess IPV cases associated with the annual temperature increase in each country under various emission scenarios, Popco represents the country-specific population size of women aged 15 to 49 years aggregated by gridded population data, and Prevalenceco means IPV prevalence for each country at baseline. To quantify the uncertainty in estimating the exposure-response (E-R) association and temperature variability for each climate model, we calculated the empirical 95% CIs through 1000 Monte Carlo simulations.24,25 We further added the gridded future population of women aged 15 to 49 years in the projection of IPV prevalence.
We performed all statistical analyses in R, version 4.0.5 (R Foundation for Statistical Computing). The packages lme4 and hyfo were applied to fit the mixed-effects logistic regression model and conduct bias-correction processes, respectively. A 2-tailed P < .05 indicated statistical significance.
Results
Descriptive Data
The analysis included 194 871 ever-partnered women aged 15 to 49 years (mean [SD] age, 35.4 [7.6] years; overall IPV prevalence, 27.0%) from 3 South Asian countries from 2010 to 2018. The prevalence of physical violence was highest (23.0%), followed by emotional (12.5%) and sexual (9.5%) violence (eTable 2 in Supplement 1). Women who experienced IPV (n = 52 567) had significantly different characteristics from those who had not experienced it (n = 142 304) (eTable 3 in Supplement 1). For example, the proportion of women living in rural areas was significantly higher among those who experienced IPV (74.6%) compared to those without this experience (69.6%). There is a higher proportion of women without education among those (55.0%) who experienced IPV compared with women without this experience (43.8%). In Pakistan, India, and Nepal, 31.9%, 27.6%, and 17.7%, respectively, of women reported IPV experience within the past 12 months (from 2010 to 2018). Most of the studied clusters in South Asia had an annual mean temperature of more than 25 °C (Figure 1A), and the annual temperature ranges were mostly between 20 °C and 30 °C (Figure 1B). During 2011 to 2018, women in India were exposed to higher mean (SD) annual temperatures (23.7 [6.2] °C) than women in Pakistan (14.2 [11.9] °C) and Nepal (9.7 [11.8] °C) (eTable 4 in Supplement 1). The Spearman correlations between individual and household variables are given in eTable 5 in Supplement 1.
Figure 1. Annual Mean Temperatures for the Studied Clusters in South Asia, 2010-2018.
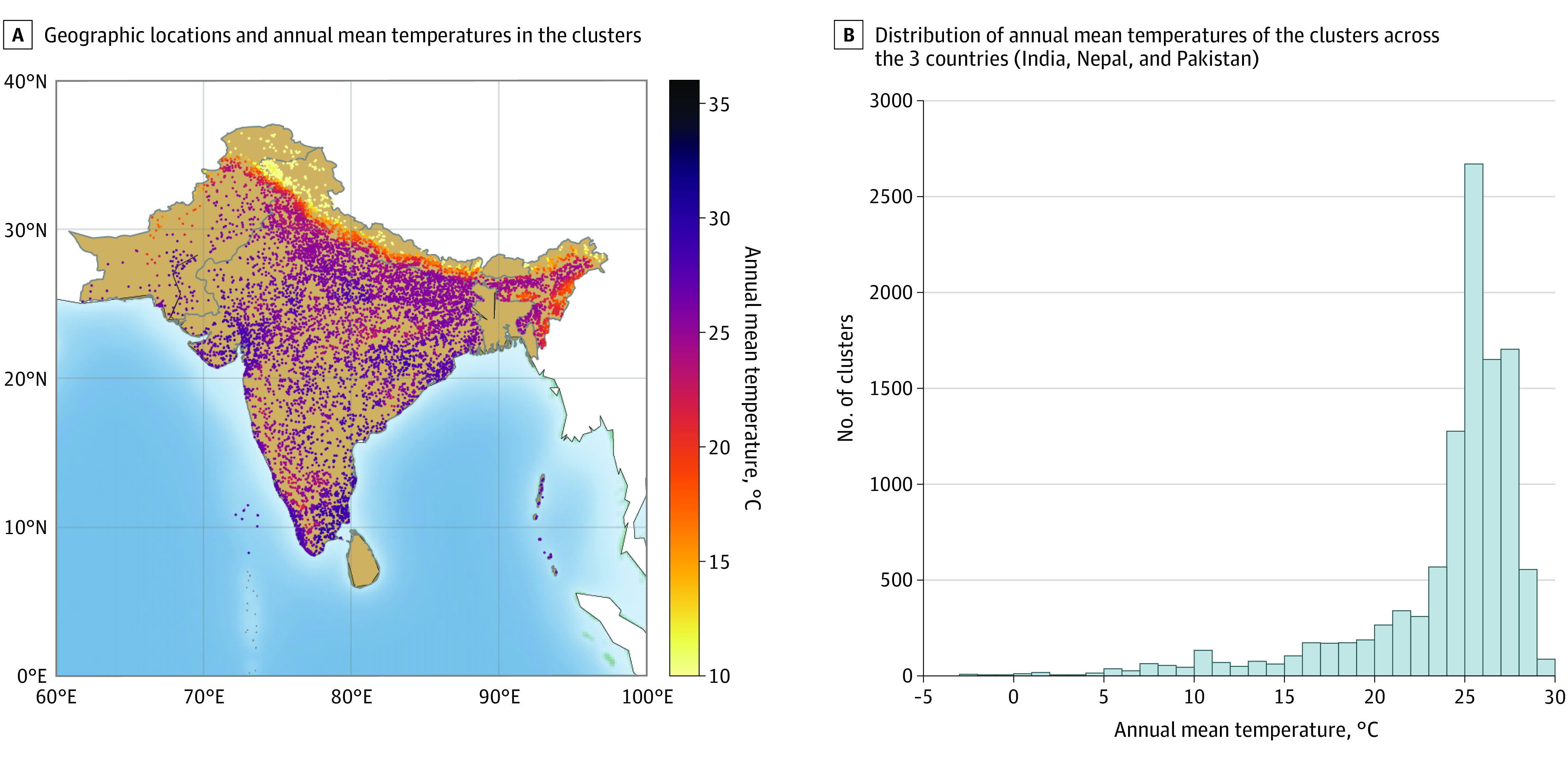
Clusters refer to groups of adjacent households, which serve as the primary sampling unit for field work efficiency in a 2-stage cluster sampling procedure in Demographic and Health Surveys.
Associations of Historical Temperature With IPV
For all 3 countries together, each 1 °C increase in the annual mean temperature was associated with a mean increase in the prevalence of IPV of 4.49% (95% CI, 4.20%-4.78%) (Figure 2). Furthermore, a greater increase in the prevalence of physical violence (mean increase, 6.55%; 95% CI, 6.21%-6.90%) and sexual violence (mean increase, 6.21%; 95% CI, 5.69%-6.74%) was observed compared with emotional violence (mean increase, 1.39%; 95% CI, 1.04%-1.73%) for every 1 °C increase. The percentages of physical and sexual violence were higher in India than in Nepal and Pakistan (Figure 2).
Figure 2. Percentage Change in Intimate Partner Violence (IPV) Prevalence per 1 °C Increase in Annual Mean Temperature in 3 South Asian Countries.

Error bars represent 95% CIs.
We flexibly plotted the E-R curves for the associations between annual temperature and IPV prevalence. The odds of IPV prevalence increased consistently with higher temperatures over most temperature ranges (eFigure 2 in Supplement 1). The overall shape of the E-R curves for total IPV and the 3 subtypes was approximately linear according to an F test (eTable 6 in Supplement 1), although there was a plateau for the association for a specific IPV type or a specific country at high temperatures.
In stratified analyses, we found significant associations between temperature and IPV among women living in rural (mean increase, 4.54%; 95% CI, 4.21%-4.88%) vs urban (mean increase, 3.68%; 95% CI, 3.07%-4.29%) areas, in households with middle wealth level and lower (mean increase, 5.09%; 95% CI, 4.66%-5.53%) vs high wealth level (mean increase, 3.38%; 95% CI, 2.99%-3.78%), and in houses with an unfinished floor (mean increase, 5.30%; 95% CI, 4.88%-5.73%) or roof (mean increase, 4.95%; 95% CI, 4.62%-5.28%) (Figure 3). Furthermore, women or their partners below the mean age or with primary education levels and lower may have higher odds of IPV prevalence in association with high temperature. The temperature-IPV associations were robust in all sensitivity analyses, as shown in eTable 7 and the results of the sensitivity analysis in the eAppendix in Supplement 1. Compared with the main model estimate using the annual mean temperature, the analysis found an association between the mean temperature in the hottest 3 months and IPV prevalence (odds ratio, 1.06; 95% CI, 1.05-1.06). However, the model fit was slightly worse than in the main analysis, except for emotional violence in Nepal (eTable 8 in Supplement 1).
Figure 3. Effect Estimates for the Association Between Annual Mean Temperatures and Intimate Partner Violence (IPV) Prevalence in Various Subgroups.

Low wealth level refers to the wealth level of the poorer or poorest individuals; high wealth level refers to individuals with middle wealth level or higher; not finished refers to natural, rudimentary, or other materials; not married refers to individuals living with a partner, widowed, divorced, or separated; young or old refers to women or their partner under and over the mean age; low educational level refers to individuals with primary education or lower; and high educational level refers to secondary education or higher. Error bars represent 95% CIs.
Spatial and Temporal Trends In Future Temperature Changes
eFigure 3 in Supplement 1 depicts the changes in the modeled ambient temperatures during the projection period (2015-2099) compared with those in the baseline period (1985-2014) under 3 emission scenarios. After the 2050s, larger increases in the annual temperature were estimated under the unlimited emission scenario (SSP5-8.5), while the increasing trends would be moderate under the stricter scenario (SSP2-4.5) and leveled off under the strictest emission scenario (SSP1-2.6). Almost all cities (the second-level administrative area in a country) exhibited a consistent increasing trend, with the most significant increase in the Himalayas region. Specifically, temperatures in South Asia were estimated to increase by 1.3 °C (95% CI, 1.1 °C-1.5 °C), 2.4 °C (95% CI, 2.2 °C-2.7 °C), and 4.7 °C (95% CI, 4.2 °C-5.4 °C) under the SSP1-2.6, SSP2-4.5, and SSP5-8.5 scenarios, respectively, by the 2090s (eTable 9 in Supplement 1).
The Projected Changes in IPV Prevalence Associated With Climate Warming
As shown in Figure 4, IPV prevalence was estimated to increase more at higher altitudes under climate warming scenarios in the 2090s compared with that in the baseline period. The spatial distributions for the prevalence changes were similar in the 3 climate scenarios, but the magnitude varied, with the largest changes under the SSP5-8.5 scenario. As shown in Figure 5, the IPV prevalence would increase by 21.0% (95% CI, 19.4%-22.6%) by the 2090s under SSP5-8.5, while the increases would be smaller under SSP2-4.5 (9.8%; 95% CI, 9.0%-10.5%), and SSP1-2.6 (5.8%; 95% CI, 5.3%-6.2%). The projected change in IPV prevalence would also vary by country, with the largest change in India (23.5%; 95% CI, 22.0%-24.9%), followed by Nepal (14.8%; 95% CI, 8.7%-20.8%) and Pakistan (5.9%; 95% CI, 3.5%-8.2%). (eTable 10 in Supplement 1).
Figure 4. Spatial Distributions of City-Level Percentage Changes in Intimate Partner Violence (IPV) Prevalence Associated With Climate Warming From the Baseline Period (1985-2014) in South Asia Under Different Climate Scenarios.
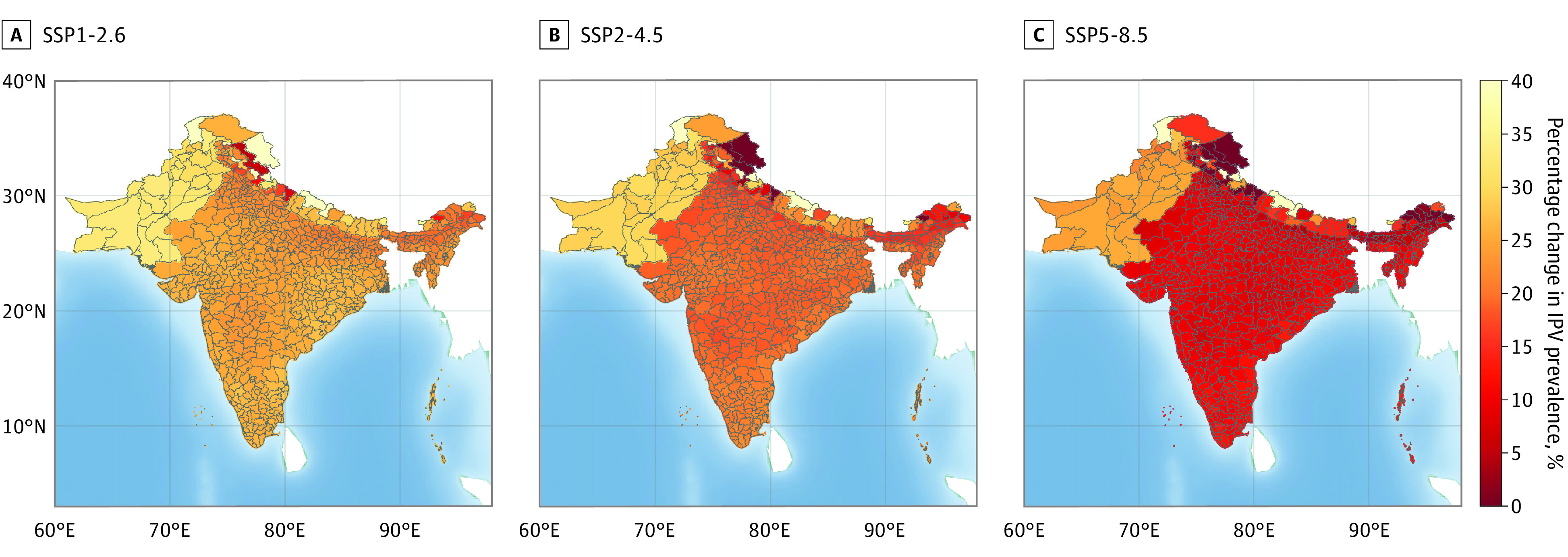
The SSPs (shared socioeconomic pathways), as defined by the Intergovernmental Panel on Climate Change, correspond to the increasing trajectories of atmospheric greenhouse gas (GHG) concentrations and characterize a range of warming in global climate from mild to extreme; for this study, 3 SSPs were used, categorized as strict (SSP1-2.6; lowest projected change), medium (SSP2-4.5), and unrestricted (SSP5-8.5; highest projected change) GHG emissions.
Figure 5. Estimated Percentage Changes in Prevalence of Intimate Partner Violence (IPV) and its Types (Physical, Sexual, and Emotional) Associated With Climate Warming From the Baseline Period (1985-2014) in 3 South Asian Countries Under Different Climate Scenarios.
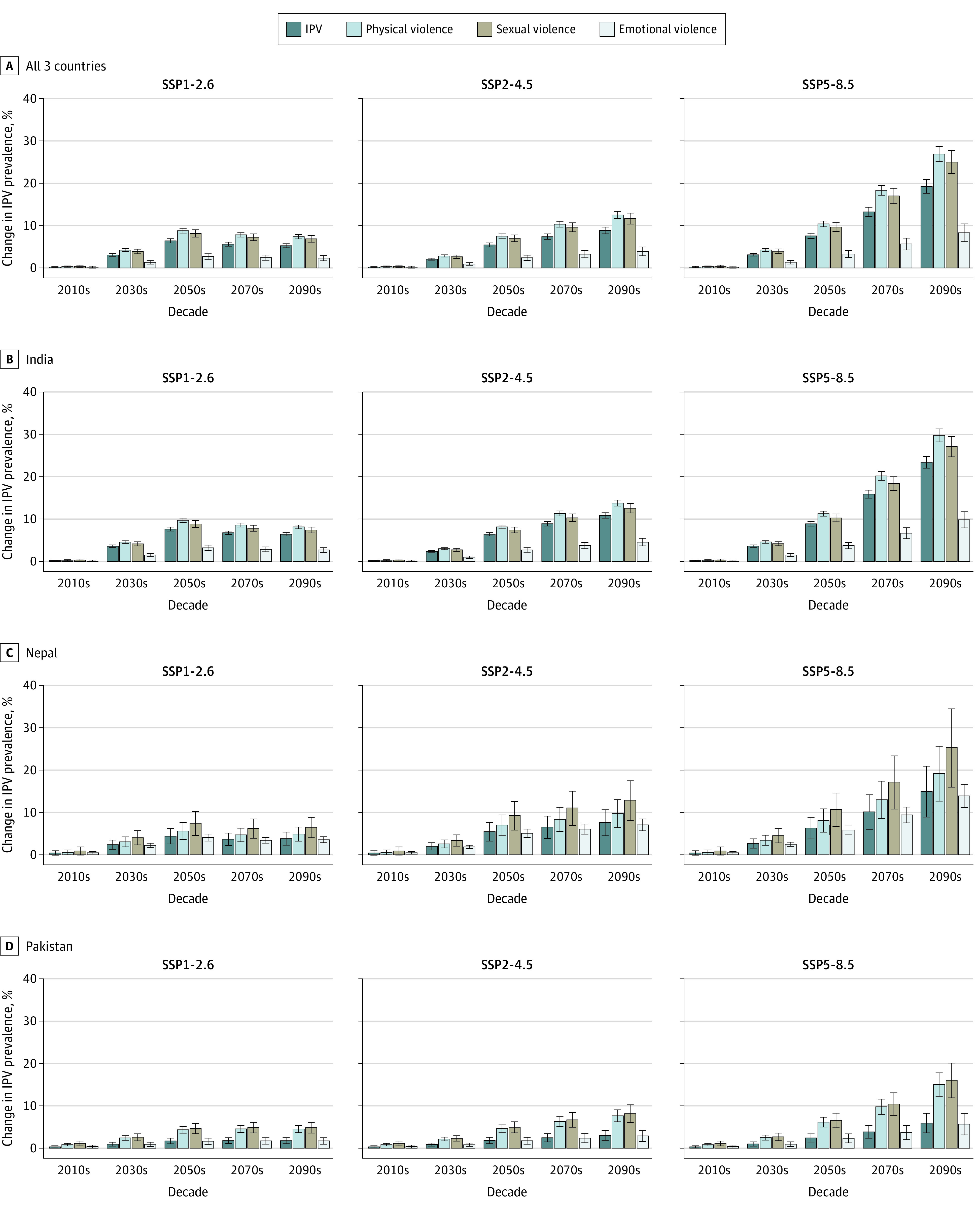
The SSPs (shared socioeconomic pathways), as defined by the Intergovernmental Panel on Climate Change, correspond to the increasing trajectories of atmospheric greenhouse gas (GHG) concentrations and characterize a range of warming in global climate from mild to extreme; for this study, 3 SSPs were used, categorized as strict (SSP1-2.6; lowest projected change), medium (SSP2-4.5), and unrestricted (SSP5-8.5; highest projected change) GHG emissions. Whiskers represent 95% empirical CIs.
Figure 5 shows the prevalence of each type of IPV in South Asia was estimated to significantly increase in the 2090s compared with that in the baseline period, except for the emotional violence prevalence in Pakistan (with nearly no change). We estimated larger increases of prevalence of physical violence (28.3%, 95% CI, 26.6%-30.1%) and sexual violence (26.1%, 95% CI, 23.4%-28.8%) than emotional violence (8.9%; 95% CI, 6.8%-11.0%) (eTable 11 in Supplement 1). India is estimated to experience a larger increase in the prevalence of physical and sexual violence (29.8%; 95% CI, 28.3%-31.4% and 27.2%; 95% CI, 24.7%-29.6%, respectively) associated with climate warming than both Pakistan (14.9%; 95% CI, 12.0%-17.7% and 15.9%; 95% CI, 11.6%-20.1%, respectively) and Nepal (18.9%; 95% CI, 12.4%-25.4% and 25.0%; 95% CI, 15.6%-34.1%, respectively).
When gridded future population of women aged 15 to 49 years was included in the projection of IPV prevalence, the percentage increase in IPV prevalence associated with climate change was not significantly different compared with the projection under the assumption of no population change (eFigure 4, eFigure 6, eTable 12, and eTable 13 in Supplement 1), although the trend of excess IPV cases differed (eFigure 5 and eFigure 7 in Supplement 1).
Discussion
This cross-sectional study, using data from a multicountry survey in South Asia, found increases in IPV prevalence associated with higher annual mean temperature between 2010 and 2018. We also estimated significant increases in IPV prevalence associated with increasing temperatures by the 2090s, particularly under the unlimited emissions scenario (SSP5-8.5). To our knowledge, our investigation provides the first evidence on the association of ambient temperature with IPV prevalence from a multicountry perspective, as well as on the projections of future IPV prevalence associated with climate change.
The associations between high temperature and IPV in this study coincide with the broader findings of the associations of high temperatures with violence. In Kenya, women who experienced severe weather events, such as heat waves, had 60% higher odds of reporting IPV.26 Similarly, a heat wave in Madrid was associated with a 40% increase in the risk of intimate partner femicides.27 Moreover, high temperature was associated with multiple manifestations of violence such as intentional homicide, collective violence, and even regional conflicts.11,13,28 Global data29 suggested that the risks of interpersonal violence and intergroup conflicts increased by 2.3% and 13.2%, respectively, with a standard deviation increase in local temperature. Collectively, these findings support our findings on the increased risks of IPV associated with heat exposure.
Our results are theoretically reasonable and supported by the heat-aggression hypothesis, which suggests that global warming is likely to increase violent behaviors through both direct and indirect pathways.7 Acute heat exposure was associated with increased adrenaline production, which could heighten physiological arousal and activate high aggression under certain conditions (eg, provocation).30,31,32 Extreme heat could also directly activate the brain areas associated with thermoregulation and emotion regulation.33 In addition, heat-related events may contribute to a range of adverse mental health outcomes, including anxiety, acute stress disorder, and posttraumatic stress disorder,34 which potentially increase IPV risk. On the other hand, high ambient temperature could decrease agricultural production and labor efficiency, consequently exacerbating household economic circumstances and further aggravating the issue of IPV.16,35 Finally, more frequent and intense extreme weather events, such as heat waves, may cause substantial damage to infrastructure and social orders, creating a deteriorating living environment that increases life stressors, weakens law enforcement, and worsens gender inequality.36,37
Our stratified analyses found higher heat-associated IPV prevalence among women with partners who were younger or had a lower educational level or lower income. To address these vulnerabilities, governments may need to offer greater access to education and vocational training for both partners and improve economic stability by reducing financial stress.38 These measures would be helpful in reducing incidents of domestic violence. Additionally, mental health services are also necessary for younger partners with less social experience and higher psychological pressure, particularly during hot seasons. These services can contribute to decreasing IPV prevalence and help both survivors and perpetrators of IPV to cope with the challenges of a changing climate.5
The projected changes in IPV prevalence associated with climate warming were associated with different emissions scenarios. The SSP5-8.5 scenario, characterized by unlimited energy consumption, GHG emissions, and population growth, would result in a dramatic increase in IPV prevalence. Our projections were generally consistent with previous estimations of violence associated with future climate warming. For instance, armed conflict incidence in Africa was projected to increase by 54% in Africa by 2030 under the representative concentration pathways (RCPs) 8.5 scenario (highest greenhouse gas concentration scenarios).39 Individuals who have experienced domestic violence are more likely to exhibit depressive symptoms or comorbidity with posttraumatic stress disorder and have a higher risk of engaging in self-harm.40 A study41 projected a 1.4% increase in suicide rates in the United States and 2.3% in Mexico by 2050 under the RCP8.5 scenario. Our projections enrich the knowledge of how high temperature in the future may be associated with human violence and add further impetus to implement more rigorous policies in mitigating future climate warming and reducing IPV.
This study suggests that India may suffer a much higher burden of IPV associated with climate warming than Nepal and Pakistan. The heterogeneity may be attributed to India’s higher annual temperatures compared with those of Nepal and Pakistan. Moreover, heat waves in India are becoming more frequent and severe than in other South Asian countries, which could aggravate the issue of IPV in the region.18 The high baseline prevalence of IPV and other social factors may also contribute to the vulnerability of Indian women to the effects of climate warming. India has a high prevalence of IPV among ever-partnered women (32.8%) and acceptability of marital violence compared with other regions of the world.42,43 Thus, the Indian government should adopt more stringent policies to reduce anthropogenic GHG emissions and address the issue of IPV. Existing laws and policies that protect women’s rights need to be reinforced, and sufficient resources should be allocated to promote education and healthy associations to foster positive and healthy partner relationships in schools and communities to adapt to the rapidly changing climate.
Limitations
This study has several limitations. First, the temperature-IPV associations were estimated using a cross-sectional design. Although this design was most commonly adopted in epidemiological studies of IPV due to the limitation of data collection, compilation, and sharing, any causal associations could not be inferred.44,45 Second, self-reported outcomes are subject to memory biases, but we assume a weak association with ambient temperature, which would not significantly confound the results. Third, historical meteorological data were derived from atmospheric reanalysis products rather than observations, but previous studies46 showed that this kind of association can be minimal. Reanalysis data have been proven to be a valid alternative source of exposure variables in epidemiological analyses, particularly in assessing temperature-associated risks.47 Fourth, projections of future changes in IPV prevalence associated with climate warming were based on the assumption of no changes in E-R associations, socioeconomic status, or climatic adaptation, and further research is needed to define their associations with the projections. Fifth, the DHS data set applied in this study included data from only 3 South Asian countries, and thus the results could not be easily extrapolated to other regions. Additional potential sources of bias are detailed in the eAppendix in Supplement 1.
Conclusion
In this cross-sectional study in 3 countries in South Asia, high ambient temperatures were associated with an increased prevalence of IPV against women. These findings highlight the additional vulnerabilities and inequalities faced by women experiencing IPV in LMICs during climate changes. The projected increase in IPV prevalence, particularly under the unlimited emissions scenario, highlights the necessity for sustainable climate change mitigation and adaptation strategies, as well as public health programs, to address the IPV issue in climate-sensitive regions or subgroups.
eAppendix
eFigure 1. Diagram of Data Preparations
eTable 1. List of DHS Survey Included in the Analysis.
eTable 2. Summary Characteristics for the Study Population and Those Suffering From Intimate Partner Violence (IPV) in Different Types
eTable 3. Summary Characteristics for the Samples in Original Database and the Samples Included in Final Analysis
eTable 4. Summary Statistics for Annual-Mean Temperatures and IPV Prevalence in Different Types During 2011-2017 in 3 South Asian Countries
eTable 5. Spearman Correlation Coefficient of Individual and Household Variables
eFigure 2. Exposure-Response Curves for the Associations Between Annual Temperature and Prevalence of IPV in South Asia, Classified by IPV Types and Countries
eTable 6. Summary of P value for F Test to Examine Linearity of the E-R Curves
eTable 7. Odds Ratios (95% Confidence Intervals) of IPV Prevalence per 1 °C Increment in Annual Temperature in Models of Sensitivity Analyses
eTable 8. R2 of Models Using Annual Temperature and Average Temperature of the Hottest 3 Consecutive Months in the Past Year in Sensitivity Analyses
eFigure 3. Projected Changes in Annual Mean Temperature From the Baseline Period (1985-2014) Under Different Climate Scenarios in 3 South Asian Countries
eTable 9. Summary Statistics of the Projected Annual Temperature Under the SSP1-2.6, SSP2-4.5 and SSP5-8.5 Scenarios in the 2010s, 2030s, 2050s, 2070s and 2090s
eTable 10. Projected Percentage Change of IPV Prevalence Attributable to Climate Warming Comparing Specific Decades to the Baseline Period (1985-2014) in 3 South Asian Countries, by Country, Period, and Climate Change Scenario, Under the Assumption of No Change in Population Size and Structure
eTable 11. Projected Percentage Change of Physical Violence, Sexual Violence and Emotional Violence Prevalence in 3 South Asian Countries From the Baseline Period (1985-2014) Under the SSP1-2.6, SSP2-4.5 and SSP5-8.5 Scenarios in the 2010s, 2030s, 2050s, 2070s and 2090s, Under the Assumption of No Change in Population
eFigure 4. Projected Percentage Changes in IPV Prevalence Attributable to Climate Warming From the baseline Period (1985-2014) in 3 South Asian Countries Under Different Climate Scenarios, Under the Assumption of No Change in Population
eFigure 5. Excess IPV Cases Attributable to Climate Warming From the Baseline Period (1985-2014) in 3 South Asian Countries Under Different Climate Scenarios, Under the Assumption of No Change in Population Size and Structure
eTable 12. Projected Percentage Change of IPV Prevalence Attributable to Climate Warming Comparing Specific Decades to the Baseline Period (1985-2014) in 3 South Asian Countries, by Country, Period, and Climate Change Scenario, Considering Population Changes Based on the Corresponding SSP Assumption
eTable 13. Projected Percentage Change of Physical Violence, Sexual Violence And Emotional Violence Prevalence in 3 South Asian Countries From the Baseline Period (1985-2014) Under the SSP1-2.6, SSP2-4.5 and SSP5-8.5 Scenarios in the 2010s, 2030s, 2050s, 2070s and 2090s, Considering Population Changes Based on the Corresponding SSP Assumption
eFigure 6. Projected Percentage Changes in IPV Prevalence Attributable to Climate Warming From the Baseline Period (1985-2014) in 3 South Asian Countries Under Different Climate Scenarios, Considering Population Changes Based on the Corresponding SSP Assumption
eFigure 7. Excess IPV Cases Attributable to Climate Warming From the Baseline Period (1985-2014) in 3 South Asian Countries Under Different Climate Scenarios, Considering Population Changes Based on the Corresponding SSP Assumption
eReferences
Data Sharing Statement
References
- 1.Anderson S. Intimate partner violence and female property rights. Nat Hum Behav. 2021;5(8):1021-1026. doi: 10.1038/s41562-021-01077-w [DOI] [PubMed] [Google Scholar]
- 2.United Nations Department of Economic and Social Affairs. Sustainable Development Goals 5: achieve gender equality and empower all women and girls. Updated 2022. Accessed May 2023. https://sdgs.un.org/goals/goal5
- 3.Sardinha L, Maheu-Giroux M, Stöckl H, Meyer SR, García-Moreno C. Global, regional, and national prevalence estimates of physical or sexual, or both, intimate partner violence against women in 2018. Lancet. 2022;399(10327):803-813. doi: 10.1016/S0140-6736(21)02664-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Coll CVN, Ewerling F, García-Moreno C, Hellwig F, Barros AJD. Intimate partner violence in 46 low-income and middle-income countries: an appraisal of the most vulnerable groups of women using national health surveys. BMJ Glob Health. 2020;5(1):e002208. doi: 10.1136/bmjgh-2019-002208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ellsberg M, Jansen HA, Heise L, Watts CH, Garcia-Moreno C; WHO Multi-country Study on Women’s Health and Domestic Violence against Women Study Team . Intimate partner violence and women’s physical and mental health in the WHO multi-country study on women’s health and domestic violence: an observational study. Lancet. 2008;371(9619):1165-1172. doi: 10.1016/S0140-6736(08)60522-X [DOI] [PubMed] [Google Scholar]
- 6.Ferdousy EZ, Matin MA. Association between intimate partner violence and child morbidity in South Asia. J Health Popul Nutr. 2015;33:16. doi: 10.1186/s41043-015-0016-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Anderson CA. Temperature and aggression: ubiquitous effects of heat on occurrence of human violence. Psychol Bull. 1989;106(1):74-96. doi: 10.1037/0033-2909.106.1.74 [DOI] [PubMed] [Google Scholar]
- 8.Anderson CA, Bushman BJ. Human aggression. Annu Rev Psychol. 2002;53(1):27-51. doi: 10.1146/annurev.psych.53.100901.135231 [DOI] [PubMed] [Google Scholar]
- 9.Cohn EG. Weather and crime. Br J Criminol. 1990;30(1):51-64. doi: 10.1093/oxfordjournals.bjc.a047980 [DOI] [Google Scholar]
- 10.Van Lange PAM, Rinderu MI, Bushman BJ. Aggression and violence around the world: a model of climate, aggression, and self-control in humans (CLASH). Behav Brain Sci. 2017;40:e75. doi: 10.1017/S0140525X16000406 [DOI] [PubMed] [Google Scholar]
- 11.Levy BS, Sidel VW, Patz JA. Climate change and collective violence. Annu Rev Public Health. 2017;38:241-257. doi: 10.1146/annurev-publhealth-031816-044232 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.O’Loughlin J, Linke AM, Witmer FD. Effects of temperature and precipitation variability on the risk of violence in sub-Saharan Africa, 1980-2012. Proc Natl Acad Sci USA. 2014;111(47):16712-7. doi: 10.1073/pnas.141189911 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Xu R, Xiong X, Abramson MJ, Li S, Guo Y. Ambient temperature and intentional homicide: a multi-city case-crossover study in the US. Environ Int. 2020;143:105992. doi: 10.1016/j.envint.2020.105992 [DOI] [PubMed] [Google Scholar]
- 14.Scheffran J, Brzoska M, Kominek J, Link PM, Schilling J. Climate change and violent conflict. Science. 2012;336(6083):869-871. doi: 10.1126/science.1221339 [DOI] [PubMed] [Google Scholar]
- 15.Dasgupta S, van Maanen N, Gosling SN, Piontek F, Otto C, Schleussner CF. Effects of climate change on combined labour productivity and supply: an empirical, multi-model study. Lancet Planet Health. 2021;5(7):e455-e465. doi: 10.1016/S2542-5196(21)00170-4 [DOI] [PubMed] [Google Scholar]
- 16.Myers SS, Smith MR, Guth S, et al. Climate change and global food systems: potential impacts on food security and undernutrition. Annu Rev Public Health. 2017;38:259-277. doi: 10.1146/annurev-publhealth-031816-044356 [DOI] [PubMed] [Google Scholar]
- 17.Shukla J. Extreme weather events and mental health: tackling the psychosocial challenge. Int Sch Res Notices. 2013;2013:127365. doi: 10.1155/2013/127365 [DOI] [Google Scholar]
- 18.Sharma A, Andhikaputra G, Wang Y-C. Heatwaves in South Asia: characterization, consequences on human health, and adaptation strategies. Atmosphere. 2022;13(5):734. doi: 10.3390/atmos13050734 [DOI] [Google Scholar]
- 19.US Agency for International Development. Demographic and Health Surveys Program. Accessed March 1, 2023. https://www.dhsprogram.com
- 20.Hersbach H, Bell B, Berrisford P, et al. The ERA5 global reanalysis. Q J R Meteorol Soc. 2020;146(730):1999-2049. doi: 10.1002/qj.3803 [DOI] [Google Scholar]
- 21.Pezzulo C, Hornby G, Sorichetta A, et al. Sub-national mapping of population pyramids and dependency ratios in Africa and Asia. Sci Data. 2017;4(170089). doi: 10.1038/sdata.2017.89 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kummu M, Taka M, Guillaume JHA. Gridded global datasets for gross domestic product and human development index over 1990-2015. Sci Data. 2018;5(1):180004. doi: 10.1038/sdata.2018.4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lee JY, Marotzke J, Bala G, et al. Future global climate: scenario-based projections and near-term information. In: Masson-Delmotte V, Zhai P, Pirani A, et al, eds. Climate Change 2021: The Physical Science Basis. Contribution of Working Group I to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change. Cambridge University Press; 2021:553-672. [Google Scholar]
- 24.Gasparrini A, Guo Y, Sera F, et al. Projections of temperature-related excess mortality under climate change scenarios. Lancet Planet Health. 2017;1(9):e360-e367. doi: 10.1016/S2542-5196(17)30156-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Yang J, Zhou M, Ren Z, et al. Projecting heat-related excess mortality under climate change scenarios in China. Nat Commun. 2021;12(1):1039. doi: 10.1038/s41467-021-21305-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Allen EM, Munala L, Henderson JR. Kenyan women bearing the cost of climate change. Int J Environ Res Public Health. 2021;18(23):12697. doi: 10.3390/ijerph182312697 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sanz-Barbero B, Linares C, Vives-Cases C, González JL, López-Ossorio JJ, Díaz J. Heat wave and the risk of intimate partner violence. Sci Total Environ. 2018;644:413-419. doi: 10.1016/j.scitotenv.2018.06.368 [DOI] [PubMed] [Google Scholar]
- 28.O’Loughlin J, Witmer FD, Linke AM, Laing A, Gettelman A, Dudhia J. Climate variability and conflict risk in East Africa, 1990-2009. Proc Natl Acad Sci U S A. 2012;109(45):18344-18349. doi: 10.1073/pnas.1205130109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hsiang SM, Burke M, Miguel E. Quantifying the influence of climate on human conflict. Science. 2013;341(6151):1235367. doi: 10.1126/science.1235367 [DOI] [PubMed] [Google Scholar]
- 30.Simister J, Cooper C. Thermal stress in the USA: effects on violence and on employee behaviour. Stress Health. 2005;21(1):3-15. doi: 10.1002/smi.1029 [DOI] [Google Scholar]
- 31.Comai S, Bertazzo A, Vachon J, et al. Tryptophan via serotonin/kynurenine pathways abnormalities in a large cohort of aggressive inmates: markers for aggression. Prog Neuropsychopharmacol Biol Psychiatry. 2016;70:8-16. doi: 10.1016/j.pnpbp.2016.04.012 [DOI] [PubMed] [Google Scholar]
- 32.Tiihonen J, Halonen P, Tiihonen L, Kautiainen H, Storvik M, Callaway J. The association of ambient temperature and violent crime. Sci Rep. 2017;7(1):6543. doi: 10.1038/s41598-017-06720-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Nakamura K, Nakamura Y, Kataoka N. A hypothalamomedullary network for physiological responses to environmental stresses. Nat Rev Neurosci. 2022;23(1):35-52. doi: 10.1038/s41583-021-00532-x [DOI] [PubMed] [Google Scholar]
- 34.Clayton S. Climate change and mental health. Curr Environ Health Rep. 2021;8(1):1-6. doi: 10.1007/s40572-020-00303-3 [DOI] [PubMed] [Google Scholar]
- 35.Parsons LA, Shindell D, Tigchelaar M, Zhang Y, Spector JT. Increased labor losses and decreased adaptation potential in a warmer world. Nat Commun. 2021;12(1):7286. doi: 10.1038/s41467-021-27328-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Boyd E, Chaffin BC, Dorkenoo K, et al. Loss and damage from climate change: a new climate justice agenda. One Earth. 2021;4(10):1365-1370. doi: 10.1016/j.oneear.2021.09.015 [DOI] [Google Scholar]
- 37.Thurston AM, Stöckl H, Ranganathan M. Natural hazards, disasters and violence against women and girls: a global mixed-methods systematic review. BMJ Glob Health. 2021;6(4):e004377. doi: 10.1136/bmjgh-2020-004377 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Adams AE, Tolman RM, Bybee D, Sullivan CM, Kennedy AC. The impact of intimate partner violence on low-income women’s economic well-being: the mediating role of job stability. Violence Against Women. 2012;18(12):1345-1367. doi: 10.1177/1077801212474294 [DOI] [PubMed] [Google Scholar]
- 39.Carleton T, Hsiang SM, Burke M. Conflict in a changing climate. Eur Phys J Spec Top. 2016;225(3):489-511. doi: 10.1140/epjst/e2015-50100-5 [DOI] [Google Scholar]
- 40.Pico-Alfonso MA, Garcia-Linares MI, Celda-Navarro N, Blasco-Ros C, Echeburúa E, Martinez M. The impact of physical, psychological, and sexual intimate male partner violence on women’s mental health: depressive symptoms, posttraumatic stress disorder, state anxiety, and suicide. J Womens Health (Larchmt). 2006;15(5):599-611. doi: 10.1089/jwh.2006.15.599 [DOI] [PubMed] [Google Scholar]
- 41.Burke M, González F, Baylis P, et al. Higher temperatures increase suicide rates in the United States and Mexico. Nat Clim Chang. 2018;8(8):723-729. doi: 10.1038/s41558-018-0222-x [DOI] [Google Scholar]
- 42.Garg P, Das M, Goyal LD, Verma M. Trends and correlates of intimate partner violence experienced by ever-married women of India: results from National Family Health Survey round III and IV. BMC Public Health. 2021;21(1):2012. doi: 10.1186/s12889-021-12028-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Ministry of Health and Family Welfare. National Family Health Survey, India. Government of India. Accessed March 1, 2023. http://rchiips.org/nfhs/
- 44.World Health Organization. Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines. 2013. Accessed May 21, 2023. https://apps.who.int/iris/bitstream/handle/10665/85240/9789241548595_eng.pdf [PubMed]
- 45.Wang Y, Fu Y, Ghazi P, et al. Prevalence of intimate partner violence against infertile women in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Glob Health. 2022;10(6):e820-e830. doi: 10.1016/S2214-109X(22)00098-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Yilmaz M. Accuracy assessment of temperature trends from ERA5 and ERA5-Land. Sci Total Environ. 2023;856(Pt 2):159182. doi: 10.1016/j.scitotenv.2022.159182 [DOI] [PubMed] [Google Scholar]
- 47.Mistry MN, Schneider R, Masselot P, et al. ; Multi-Country Multi-City (MCC) Collaborative Research Network . Comparison of weather station and climate reanalysis data for modelling temperature-related mortality. Sci Rep. 2022;12(1):5178. doi: 10.1038/s41598-022-09049-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eAppendix
eFigure 1. Diagram of Data Preparations
eTable 1. List of DHS Survey Included in the Analysis.
eTable 2. Summary Characteristics for the Study Population and Those Suffering From Intimate Partner Violence (IPV) in Different Types
eTable 3. Summary Characteristics for the Samples in Original Database and the Samples Included in Final Analysis
eTable 4. Summary Statistics for Annual-Mean Temperatures and IPV Prevalence in Different Types During 2011-2017 in 3 South Asian Countries
eTable 5. Spearman Correlation Coefficient of Individual and Household Variables
eFigure 2. Exposure-Response Curves for the Associations Between Annual Temperature and Prevalence of IPV in South Asia, Classified by IPV Types and Countries
eTable 6. Summary of P value for F Test to Examine Linearity of the E-R Curves
eTable 7. Odds Ratios (95% Confidence Intervals) of IPV Prevalence per 1 °C Increment in Annual Temperature in Models of Sensitivity Analyses
eTable 8. R2 of Models Using Annual Temperature and Average Temperature of the Hottest 3 Consecutive Months in the Past Year in Sensitivity Analyses
eFigure 3. Projected Changes in Annual Mean Temperature From the Baseline Period (1985-2014) Under Different Climate Scenarios in 3 South Asian Countries
eTable 9. Summary Statistics of the Projected Annual Temperature Under the SSP1-2.6, SSP2-4.5 and SSP5-8.5 Scenarios in the 2010s, 2030s, 2050s, 2070s and 2090s
eTable 10. Projected Percentage Change of IPV Prevalence Attributable to Climate Warming Comparing Specific Decades to the Baseline Period (1985-2014) in 3 South Asian Countries, by Country, Period, and Climate Change Scenario, Under the Assumption of No Change in Population Size and Structure
eTable 11. Projected Percentage Change of Physical Violence, Sexual Violence and Emotional Violence Prevalence in 3 South Asian Countries From the Baseline Period (1985-2014) Under the SSP1-2.6, SSP2-4.5 and SSP5-8.5 Scenarios in the 2010s, 2030s, 2050s, 2070s and 2090s, Under the Assumption of No Change in Population
eFigure 4. Projected Percentage Changes in IPV Prevalence Attributable to Climate Warming From the baseline Period (1985-2014) in 3 South Asian Countries Under Different Climate Scenarios, Under the Assumption of No Change in Population
eFigure 5. Excess IPV Cases Attributable to Climate Warming From the Baseline Period (1985-2014) in 3 South Asian Countries Under Different Climate Scenarios, Under the Assumption of No Change in Population Size and Structure
eTable 12. Projected Percentage Change of IPV Prevalence Attributable to Climate Warming Comparing Specific Decades to the Baseline Period (1985-2014) in 3 South Asian Countries, by Country, Period, and Climate Change Scenario, Considering Population Changes Based on the Corresponding SSP Assumption
eTable 13. Projected Percentage Change of Physical Violence, Sexual Violence And Emotional Violence Prevalence in 3 South Asian Countries From the Baseline Period (1985-2014) Under the SSP1-2.6, SSP2-4.5 and SSP5-8.5 Scenarios in the 2010s, 2030s, 2050s, 2070s and 2090s, Considering Population Changes Based on the Corresponding SSP Assumption
eFigure 6. Projected Percentage Changes in IPV Prevalence Attributable to Climate Warming From the Baseline Period (1985-2014) in 3 South Asian Countries Under Different Climate Scenarios, Considering Population Changes Based on the Corresponding SSP Assumption
eFigure 7. Excess IPV Cases Attributable to Climate Warming From the Baseline Period (1985-2014) in 3 South Asian Countries Under Different Climate Scenarios, Considering Population Changes Based on the Corresponding SSP Assumption
eReferences
Data Sharing Statement