

Abstract
Introduction:
Lipomas are most common soft-tissue tumors but rarely are found to be symptomatic. <1% of lipomas are found in hand. Subfascial lipomas can cause pressure symptoms. Carpal tunnel syndrome (CTS) can be idiopathic or secondary to any space-occupying lesion. Triggering usually occurs due to inflammation/thickening of A1 pulley. Most have reported a lipoma in distal forearm or near median nerve, leading to triggering of index or middle finger and carpal tunnel symptoms. All the cases reported had either an intramuscular lipoma in flexor digitorum superficialis (FDS) tendon slip of index or middle finger, with or without accessory belly of FDS muscle or a neurofibrolipoma of the median nerve. In our case, the lipoma was under palmer fascia, in flexor digitorum profundus (FDP) tendon sheath of fourth finger causing triggering of the ring finger and CTS symptoms in flexion of the ring finger. Hence, this is a first report of this kind in the literature.
Case Report:
We hereby report a one of its kind case in which a 40-year-old Asian male patient had triggering of the ring finger with associated intermittent CTS symptoms, on making a fist, secondary to space-occupying lesion in palm, which was diagnosed by ultrasound as lipoma in FDP tendon of the ring finger in palm. This lipoma was surgically removed by AO ulnar palmer approach and carpal tunnel was decompressed. Histopathology report confirmed the lump to be fibrolipoma. The patient had complete relief of symptoms postoperatively. At 2 years follow-up, there was no recurrence.
Keywords: Fibrolipoma, triggering, carpal tunnel syndrome, ulnar palmar approach of AO, case report
Learning Point of the Article:
A high index of suspicion, meticulous history taking, clinical examination when patient comes with trigger finger and unilateral intermittent CTS symptoms is of paramount importance to rule out secondary CTS due to a space occupying lesion.
Introduction
Lipoma is the most common benign soft-tissue tumor [1]. When such lipoma develops on the palmer aspect of wrist near carpal tunnel, it leads to compression of median nerve in carpal tunnel. Such patients complain of triggering of index or middle finger and tingling, numbness, and paresthesia with or without weakness of radial three and half fingers. There are few case reports in the literature which reports triggering of index or middle finger at wrist secondary to a lipoma. These lipomas were usually found to be intramuscular lipoma of flexor digitorum superficialis (FDS) muscle with or without accessory belly of FDS muscle.
We hereby report a rare case where a patient came with complaints of triggering of the right ring finger with intermittent tingling numbness in the right three and half fingers, clinically diagnosed as carpal tunnel syndrome (CTS) secondary to a lipoma of flexor digitorum profundus (FDP) tendon of the ring finger in palm. Such a case has not been reported in the English literature.
The work has been reported in line with the SCARE criteria [2].
Case Report
A 36-year-old man, clerk by occupation, came to orthopedic outpatient depart in B.K.L. Walawalkar rural medical college and hospital Dervan in May 2019 with complaints of difficulty in performing right (dominant hand) ringer finger movements for the past 3–4 months. Formation of fist was associated with a clunk in palm and, pain and heaviness in radial side of hand, that is, the thumb, index, middle finger, and ring finger. Opening of fist relieved all the symptoms. He had no history of trauma and no comorbidities. On clinical examination, there was triggering of the right ring finger at palm. No obvious swelling was noted. There was no wasting of thenar eminence. In extension on deep palpation, a firm swelling was palpable in palm along the ring finger which moved proximally along the flexor tendon of ring finger and disappeared on flexing the ring finger. In this position, the patient developed pain and heaviness along the radial three fingers. Tinel’s sign was positive only in this position. Phalen’s test was negative. Transillumination test was negative. In X-ray, no abnormality was noted. Ultrasound showed a well-defined hypoechoic partially compressible focal oval lesion, measuring 19 × 8 mm in size with no vascularity inside, and arising from FDP of the right ring finger, located just distal to palmer aponeurosis. This swelling moved longitudinally along the FDP of ring finger during flexion and extension of ring finger. Median nerve was normal. These findings were suggestive of lipoma/giant cell tumor of FDP tendon of ring finger.
After counseling, pre-operative investigations and pre-anesthetic check-up patient was posted for excision of the lump. Regional block was given and tourniquet used. An ulnar palmar approach of AO was chosen for this surgery as it facilitated easy exposure of FDP tendon of ring finger as well as distally same could be used to do carpal tunnel release (Figs. 1, 2, 3, 4).
Figure 1.

Marking of AO ulnar palmer approach.
Figure 2.

Deep fascia cut between ulnar artery and nerve on ulnar side and flexor digitorum superficialis tendons on radial side.
Figure 3.

Lipoma brought into surgical field by flexing ring finger and pulling FDP tendon of ring finger proximally with a curved hemostat inserted underneath the tendon.
Figure 4.
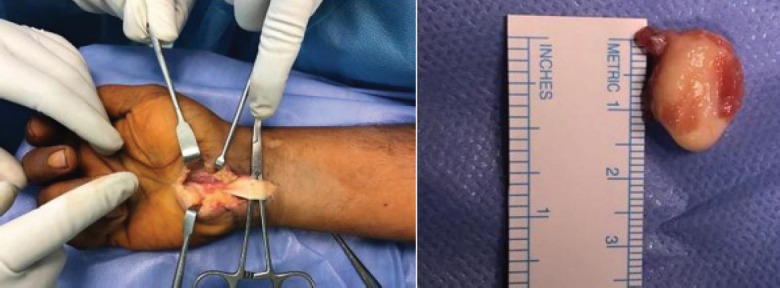
After excision of the lipoma. Complete excision of the lump measuring 1.5 cm × 1 cm × 1 cm with its capsule intact was done carefully.
The ring finger was again flexed and extended alternately to confirm that there is no triggering. Transverse carpal ligament was released to achieve complete decompression of the carpal tunnel. Once satisfied with the decompression tourniquet was deflated. Wash was given and closure done in layers. Dressing was done and crepe bandage was applied from distal to proximal forearm. The lump was sent for histopathologic study. The patient was given elevation in immediate post-operative period.
The patient was discharged same day with advice to actively do movements of all fingers regularly. Oral antibiotics, anti-inflammatory, and analgesics for pain relief were given in post-operative period for 3 days according to our institutions protocol. Physiotherapy was started immediately. He was noted to have satisfactory range of motion. Sutures were removed in out-patient department on day 14 post surgery. The patient had full painless range of motion of all fingers and so was allowed to perform all activities with no restrictions.
Histopathology report showed mixture of mature adipocytes and fibro collagenous tissue with thick collagen bundles seen infiltrating the muscle tissue at periphery confirmed the lump to be a fibrolipoma (Fig. 5).
Figure 5.
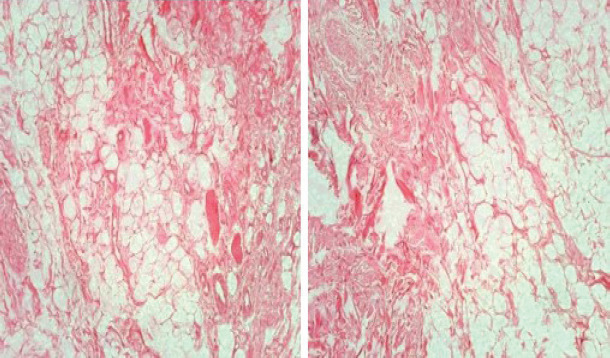
Histology slides showing abundant mature adipocytes with interspersed fibrous bands s/o fibrolipoma.
At 2 years follow-up, the patient was clinically and radiologically assessed (Fig. 6). He was completely asymptomatic and performing all his activities without any discomfort or limitations of wrist or fingers. There was no triggering and USG confirmed no recurrence of fibrolipoma.
Figure 6.

At 2 years follow-up clinical picture of operative hand.
Discussion
Lipoma is known to be the most common soft-tissue tumor [1]. Jalan D reported a giant lipoma causing external compression of median nerve and causing CTS [3]. Our case consists of triggering of the right ring finger with intermittent tingling numbness in the right three and half fingers secondary to histologically proven fibrolipoma in palm in FDP tendon of ring finger. All cases of CTS secondary to lipoma had lipoma in FDS tendon of index or middle finger or accessory muscle belly of FDS or lipoma in carpal tunnel near or arising from median nerve, that is, neurofibrolipoma. There is no case report of fibrolipoma, leading to CTS, nor any report of fibrolipoma of FDP tendon of ring finger in palm causing triggering, nor is there a report of using an AO ulnar palmar approach for carpal tunnel release.
Fibrolipoma is second most common type of lipoma found after classic lipoma [4]. All types of lipomas have well-defined margins and are encapsulated except liposarcoma which has ill-defined margins and invaginates into surrounding tissue. In our case, it was found to be fibrolipoma type of lipoma. Ozturk M found the growth rate of fibrolipomas is faster than the classic variants and even though fibrolipomas are benign tumors, few cases of conversion to liposarcoma are also reported [5]. This might be a reason why our patient developed symptoms over just 3–4 months duration.
CTS is most common compressive neuropathy in the hand [6]. Most cases of CTS are idiopathic, however when found to be unilateral, space-occupying lesions or narrowing of space due to swelling of tendon sheath, distal radius fracture, volar dislocation of lunate, ganglion, occult calcified mass, tuberculous synovitis, rheumatoid arthritis, non-specific synovitis, gout, etc., should be suspected and ruled out. If these space-occupying lesions are not discovered or misdiagnosed and patient is treated as idiopathic CTS, the patient’s symptoms may not improve by mere transverse carpal ligament release. To rule out space-occupying lesions in patients who exhibit swelling or palpable mass in the volar wrist region during physical examination or patients who exhibit radio-opaque lesion discovered during plain X-ray, further special studies (ultrasonogram, CT, and MRI) should be performed [7, 8].
In the literature, very few cases of CTS secondary to lipoma have been reported until now [9]. Chen found only three out of 779 CTS patients had lipoma which acted like a space-occupying lesion in carpal tunnel and lead to CTS [10]. Ho Jung Kang did not report any cases of lipoma in his 568 CTS cases [11].
Lipomas in palm can be difficult to diagnose due its rare occurrence and thick palmer aponeurosis. Other soft-tissue tumors such as ganglion cysts, giant-cell tumors, myxomas, angiolipomas, and intraneural lipofibromas are to be considered as differential diagnosis [12]. In our case, classical features on ultrasound and its longitudinal gliding movement in relation to movement of the ring finger helped to narrow our differential diagnosis to lipoma or giant cell tumor of tendon sheath. For identification of the specific subtype, that is, fibrolipoma histopathology was done of the excised lump.
As ultrasound ruled out ganglion cyst, myxoma, angiolipoma, and intraneural lipofibroma, we did not feel the need to do any further investigation. USG due to its ability to localize a lesion, determine whether lesion is cystic or solid, ability to show real time vascularity, dynamic study, cheap, and easy availability, of is investigation of choice after routine X-rays to rule out space-occupying lesion in wrist, leading to secondary CTS [13].
Ultrasound being 86.8% sensitive and 95.5 % specific in diagnosing soft-tissue lipomas unless ultrasound findings are not confirmatory further investigations may not be performed [14].
Trigger finger is the most common cause of pain and click in fingers [15]. It is vital to remember that in a trigger finger, A 1 pulley is affected and noted to be tender on palpation. Absence of tenderness at A 1 pulley warrants attention to palm and wrist which can be a cause of triggering of finger like in our case.
We performed open release of transverse carpal ligament after excision of the fibrolipoma. We used an ulnar palmer approach which is suggested by AO trauma for exploration of ulnar structures at wrist and simultaneously release of transverse carpal ligament to achieve median nerve decompression. Patient’s CTS symptoms and triggering of ring finger had disappeared immediately and had not recurred at 2 years follow-up.
Conclusion
Lipoma can occur anywhere in body. Although most of these are asymptomatic a detailed clinical examination and appropriate investigations can help to diagnose such rare instances. Knowledge of different approaches for carpal tunnel release can help in achieving decompression in different situations.
Clinical Message.
A very high index of suspicion and meticulous history taking, clinical examination when patient comes with ring trigger finger and unilateral intermittent CTS symptoms is of paramount importance to rule out secondary CTS due to a space-occupying lesion. For pre-operative planning X-rays, ultrasound and MRI whenever felt necessary are essential for accurate diagnosis, surgical planning, and successful outcome. Whenever excision of lipoma is planned, along with transverse carpal ligament release its better to use extensile open approach and mini open or endoscopic procedures should be avoided. Awareness of different surgical incisions can help by better visibility and easy access to lipoma. Every specimen should be sent for histopathology as histopathology is gold standard for diagnosis.
We recommend in every case of CTS and/or trigger finger
X-ray and ultrasound after clinical examination because ultrasound provides a real time evaluation
We recommend an open approach rather than mini open or endoscopic procedure as either of the last two can lead to incomplete excision of space-occupying lesion, which can lead to recurrence in future
We do not recommend electrodiagnostic testing for patient having triad of CTS, triggering, and space-occupying lesion
Clinical examination is of paramount importance for diagnosis and to decide investigations.
Biography

Footnotes
Conflict of Interest: Nil
Source of Support: Nil
Consent: The authors confirm that informed consent was obtained from the patient for publication of this case report
References
- 1.Adoga AA, Nimkur TL, Manasseh AN, Echejoh GO. Buccal soft tissue lipoma in an adult Nigerian:A case report and literature review. J Med Case Rep. 2008;2:382. doi: 10.1186/1752-1947-2-382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Agha RA, Fowler AJ, Saetta A, Barai I, Rajmohan S, Orgill DP, et al. The SCARE statement:Consensus-based surgical case report guidelines. Int J Surg. 2016;34:180–6. doi: 10.1016/j.ijsu.2016.08.014. [DOI] [PubMed] [Google Scholar]
- 3.Jalan D, Garg B, Marimuthu K, Kotwal P. Giant lipoma:An unusual cause of carpal tunnel syndrome. Pan Afr Med J. 2011;9:29. doi: 10.4314/pamj.v9i1.71205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rajeev R, Beena VT, Indu G, Choudhary K, Devu A. Fibrolipoma of floor of the mouth of 20 years of duration. Clin Cancer Investig J. 2014;3:394–7. [Google Scholar]
- 5.Ozturk M, Ila K, Kara A, Iseri M. Fibrolipoma of the nasal septum;report of the first case. J Otolaryngol Head Neck Surg. 2013;42:11. doi: 10.1186/1916-0216-42-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Eversmann WW., Jr . Entrapment and compression neuropathies. In: Green DP, editor. Operative Hand Surgery. Vol. 2. New York: Churchill Livingstone; 1993. pp. 1341–85. [Google Scholar]
- 7.Horch RE, Allmann KH, Laubenberger J, Langer M, Stark GB. Median nerve compression can be detected by magnetic resonance imaging of the carpal tunnel. Neurosurgery. 1997;41:76. doi: 10.1097/00006123-199707000-00016. discussion 82-3. [DOI] [PubMed] [Google Scholar]
- 8.Kamolz LP, Schrögendorfer KF, Rab M, Girsch W, Gruber H, Frey M. The precision of ultrasound imaging and its relevance for carpal tunnel syndrome. Surg Radiol Anat. 2001;23:117–21. doi: 10.1007/s00276-001-0117-8. [DOI] [PubMed] [Google Scholar]
- 9.Hoehn JG, Farber HF. Massive lipoma of the palm. Ann Plast Surg. 1983;11:431–3. doi: 10.1097/00000637-198311000-00012. [DOI] [PubMed] [Google Scholar]
- 10.Chen CH, Wu T, Sun JS, Lin WH, Chen CY. Unusual causes of carpal tunnel syndrome:Space occupying lesions. J Hand Surg Eur Vol. 2012;37:14–9. doi: 10.1177/1753193411414352. [DOI] [PubMed] [Google Scholar]
- 11.Kang HJ, Jung SH, Yoon HK, Hahn SB, Kim SJ. Carpal tunnel syndrome caused by space occupying lesions. Yonsei Med J. 2009;50:257–61. doi: 10.3349/ymj.2009.50.2.257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Stuffer M, Thurner JE. Lipoma of the index digit--a very rare location. Arch Orthop Trauma Surg. 1995;114:239–40. doi: 10.1007/BF00444272. [DOI] [PubMed] [Google Scholar]
- 13.Toprak H, Kiliç E, Serter A, Kocakoç E, Ozgocmen S. Ultrasound and doppler US in evaluation of superficial soft-tissue lesions. J Clin Imaging Sci. 2014;4:12. doi: 10.4103/2156-7514.127965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rahmani G, McCarthy P, Bergin D. The diagnostic accuracy of ultrasonography for soft tissue lipomas:A systematic review. Acta Radiol Open. 2017;6:2058460117716704. doi: 10.1177/2058460117716704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ryzewicz M, Wolf JM. Trigger digits:Principles, management, and complications. J Hand Surg Am. 2006;31:135–46. doi: 10.1016/j.jhsa.2005.10.013. [DOI] [PubMed] [Google Scholar]