

Abstract
Evidence-based clinical guidelines ensure best practice protocols are available in health care. There is a widespread use of human papillomavirus deoxyribonucleic acid (HPV-DNA) tests in Brazil, regardless of the lack of official guidelines. On behalf of the Brazilian Association for the Lower Genital Tract Pathology and Colposcopy (ABPTGIC, in the Portuguese acronym), a team of reviewers searched for published evidence and developed a set of recommendations for the use of HPV-DNA tests in cervical cancer screening in Brazil. The product of this process was debated and consensus was sought by the participants. One concern of the authors was the inclusion of these tests in the assessment of women with cytologic atypia and women treated for cervical intraepithelial neoplasia (CIN). Testing for HPV is recommended in an organized screening scenario to identify women with precursor lesions or asymptomatic cervical cancer older than 30 years of age, and it can be performed every 5 years. It also has value after the cytology showing atypical squamous cells of undetermined significance (ASC-US) or low-grade squamous intraepithelial lesions (LSILs) as a triage test for colposcopy, in the investigation of other cytological alterations when no abnormal findings are observed at colposcopy, seeking to exclude disease, or, further, after treatment of high-grade cervical intraepithelial neoplasia, to rule out residual disease.
Keywords: screening, cervical neoplasms, DNA-HPV probes, cervical intraepithelial neoplasia, cytology
Resumo
O uso de diretrizes clínicas baseadas em evidências visa assegurar as melhores práticas na área de cuidado à saúde. O uso de testes de ácido desoxirribonucleico de papilomavírus humano (DNA-HPV) vem crescendo e se disseminando sem que existam recomendações de uso no cenário brasileiro. Em nome da Associação Brasileira de Patologia do Trato Genital Inferior e Colposcopia (ABPTGIC), grupos de revisores pesquisaram evidências e formularam recomendações para o uso dos testes de DNA-HPV no rastreamento do câncer do colo do útero, no seguimento de mulheres com atipias citológicas, e após tratamento de neoplasia intraepitelial cervical (NIC). O produto desse processo foi debatido e foi buscado consenso entre participantes. Os testes de DNA-HPV são recomendados num cenário de rastreamento organizado para identificação de mulheres portadoras de lesões precursoras ou câncer assintomático com mais de 30 anos e podem ser realizados a cada 5 anos. Também têm valor após a citologia mostrando células escamosas atípicas de significado indeterminado (ASC-US) ou lesão intraepitelial escamosa de baixo grau (LSIL) como teste de triagem para colposcopia, na investigação de outras alterações citológicas quando não são observados achados anormais à colposcopia, buscando excluir doença, ou, ainda, no seguimento após tratamento das neoplasias intraepiteliais de alto grau, para exclusão de doença residual.
Palavras-chave: rastreamento, neoplasias do colo do útero, sondas de DNA de HPV, neoplasia intraepitelial cervical, citologia
Introduction
The present article is a result of the review and update process of the Brazilian Guidelines for Cervical Cancer Screening,1 published in 2016. Human papillomavirus deoxyribonucleic acid (HPV-DNA) tests had already been widely used in Brazil for years, without specific national guidelines, and these recommendations aimed to fill this gap.
Thus, the workgroup that revised and updated the current Brazilian guidelines prepared the present document on behalf of the Brazilian Association for the Lower Genital Tract Pathology and Colposcopy (ABPTGIC, in the Portuguese acronym). This document does not represent the position of the Brazilian Ministry of Health on the use of DNA-HPV detection tests, and it should be emphasized that this text does not replace the existing recommendations, which are based on technologies widely recognized and available to the Brazilian population.
The aim of these recommendations is to guide practitioners working in scenarios in where the test is available, so they can use it according to the best practice and in the light of the best evidence.
The process of building these recommendations was described in the Brazilian Guidelines for Cervical Cancer Screening - 2nd edition, revised, expanded and updated.1
Technical Considerations
By “HPV-DNA test,” we mean any test for the detection of oncogenic HPV-DNA in biological specimens obtained by a cervical smear or brushing. The detection of non-oncogenic HPV types is not clinically relevant in this setting.
Generally, the use of HPV-DNA tests in cervical cancer screening is beneficial because it is more sensitive, identifying more women with precursor lesions and cancer than the conventional Pap smear. On the other hand, because of its lower specificity, more women may be unnecessarily referred for colposcopy, which leads to an increase in costs and unwanted morbidity.
One advantage of HPV-DNA tests following an abnormal Pap smear is their high negative predictive value. When oncogenic HPV-DNA is undetectable, the occurrence of precursor lesions or cervical cancer is very unlikely.
Methods
In summary, from February 2013 to August 2014, almost 40 experts got together to update the previously published recommendations2 based on the best available evidence. Among these experts were prominent gynecologists with known experience in the subject, as well as representatives of institutions involved in cervical cancer screening and the follow-up of abnormal screening tests, who share the authorship of this paper. The remaining participants of the revision and consensus process are listed in the Acknowledgments. The review leaders were selected by a panel of specialists leaded by the ABPTGIC. Each review leader invited other specialists from other parts of the country, considering their work in the specific area of interest. Each review group reviewed one main topic, searching for the best evidence in original articles or secondary information sources, submitting their summary and updated recommendations to the whole group. The result of the work of each group was discussed in videoconferences and, at the end of this process, the final text was discussed in a special meeting in Rio de Janeiro.
The following text presents, in each topic, evidence that supports the use of the HPV-DNA tests in each individual scenario. The evidence from the literature was classified as high, moderate or low, according to the risk of bias (Table 1).
Table 1. Level of certainty.
| Certainty Level* | Description |
|---|---|
| High | The available evidence usually includes consistent results from well-designed and well-conducted studies among the representative populations to which they apply. These studies assess the effects of the preventive practice on health outcomes. This conclusion is therefore unlikely to be strongly affected by the results of future studies. |
| Moderate | The available evidence is sufficient to establish the effects of the preventive practice on health outcomes, but confidence is limited by factors such as: • The number, size or quality of the individual studies • Inconsistency in the findings across individual studies • Limited generalizability of the findings to the routine practice • Lack of consistency in the chain of evidence As more information becomes available, the magnitude or direction of the observed effect may change, and this change may be large enough to alter the conclusion. |
| Low | The available evidence is insufficient to assess effects on health outcomes. The evidence is insufficient because of: • The limited number or size of the studies • Important flaws in the studies' designs or methods • Inconsistency in the findings across individual studies • Gaps in the chain of evidence • Findings not generalizable to the routine practice • Lack of information on important health outcomes More information can allow estimates of the effects on health outcomes. |
The United States Preventive Services Task Force (USPSTF) attributes a level of certainty based on the general nature of the evidence available to assess the net benefit of a preventive practice.3
The summary of evidences is followed by specific recommendations that resulted in the experts' consensus. Each recommendation is followed by a capital letter in parentheses, meaning its strength, based on the degree of certainty from the best scientific evidence and judgment of the participants (Table 2). In Table 3 we list the most relevant recommendations.
Table 2. Strength of recommendation.
| Grade | Definition* | Recommendations for practice |
|---|---|---|
| A | The practice is recommended. There is high certainty that the net benefit is substantial. | Offer or provide the practice. |
| B | The practice is recommended. There is high certainty that the net benefit is moderate or there is moderate certainty that the net benefit is moderate to substantial. | Offer or provide the practice. |
| C | The practice is not routinely recommended. There may be considerations that support the practice at an individual level. There is at least moderate certainty that the net benefit is small. | Offer or provide this service for selected patients depending on individual circumstances. |
| D | The practice is not recommended. There is moderate or high certainty that the practice has no net benefit, or that the damages outweigh the benefits. | Discourage the use of this practice. |
| I | The current evidence is insufficient to assess the balance between its benefits and harms. The evidence is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined. | Read the introductory text containing evidence obtained in the literature review that supports this recommendation. If the practice is offered, the patients should understand that there is uncertainty in the balance between benefits and harms. |
The United States Preventive Services Task Force (USPSTF) defines certainty as the “likelihood that the USPSTF's assessment of the net benefit of a preventive practice is correct.” The net benefit is defined as the benefit minus the practice injury when implemented in a general population.2
Table 3. Most relevant recommendations for the use of the HPV-DNA test in cervical cancer screening and after an abnormal cytology.
| The HPV-DNA test can be the primary screening method as an alternative to cytology in women aged 30 years or older. When negative, the test should be repeated every 5 years. |
| When the HPV-DNA test is positive for oncogenic HPV, triage with cytology is recommended. If genotyping is available and if it is positive for HPV types 16 or 18, the woman may be referred for colposcopy. |
| Women aged 30 years or older with ASC-US can perform the HPV-DNA test as an alternative to a new cytology after 6 months. |
| Women 30 years of age or older with LSIL can perform the HPV-DNA test to select those who should be referred for colposcopy. |
| In women with ASC-H or HSIL and normal colposcopy, a negative HPV-DNA test will virtually rule out precursor lesions or invasive disease. |
| In women with AGC or AIS and normal colposcopy, a negative HPV-DNA test means a low probability of cervical disease, demanding investigation of the endometrium and other pelvic organs. |
| The HPV-DNA test may be used at follow-up after the treatment of CIN II/III and AIS to exclude residual or recurrent lesions, and it is recommended between 6 and 12 months after the treatment. |
Abbreviations: ASC-H, atypical squamous cells, cannot exclude high-grade squamous intraepithelial lesion; ASC-US, atypical squamous cells of undetermined significance; AGC, atypical glandular cells; AIS, adenocarcinoma in situ; CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus; HPV-DNA, human papillomavirus deoxyribonucleic acid; HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion.
HPV-DNA Test Use in Cervical Cancer Screening
The occurrence of false-negative and unsatisfactory cytology tests prompted the development of new technologies that improve screening quality.4 In addition, the evidence of a causal relationship between oncogenic HPV infection and cervical cancer and its precursor lesions led to the development of HPV-DNA detection techniques to prevent and identify these lesions.5
There is currently scientific evidence supporting HPV-DNA tests as the primary screening method for women aged 30 years or older. Screening for HPV-DNA has a high sensitivity, and anticipates the diagnosis of cervical intraepithelial neoplasia (CIN) II and III even when the screening is performed in a 5-year interval. This technique is better than regular cervical cytology in the diagnosis of glandular lesions (adenocarcinoma) (evidence level: high).6 Staff training is fast, laboratory results are reproducible, and it qualifies for self-sample HPV-DNA-based screening (evidence level: high).7
The main limitation of HPV-DNA-based tests is their low specificity (positive results when there is no lesion – a common finding in women under 30 years of age) (evidence level: high).8 To avoid an excessive number of women unnecessarily referred to colposcopy because they were screened with a positive HPV result, triage methods are necessary. One option is the cytology triage of HPV-DNA-positive cases, referring only women who tested positive for HPV-DNA and whose cytology test was abnormal (evidence level: high).9 This strategy has proven to be more sensitive and to have the same specificity as cytology alone in a Swedish randomized clinical trial, which was part of the national population-based screening program (evidence level: high).10
Screening for HPV-DNA has a greater operational advantage if performed using a sample that would also allow a cytology triage, and this is the case of the liquid medium. Therefore, if the HPV-DNA test is positive, the cytology test can be performed in the same sample, and a new sample collection is not necessary, thus saving time and resources.
Human papillomavirus types 16 and 18 (genotyping) in women with a positive HPV-DNA test and a negative cytology have shown favorable results for the selection of women with a higher probability of having CIN II or higher type (CIN II +). Prospective studies with a large number of women support the immediate referral of patients with positive HPV-DNA types 16 and 18 to colposcopy, regardless of the use of cytology as triage (evidence level: high).11 12 13
In summary, screening with HPV-DNA-based tests may be advantageous in women aged 30 years or older, followed by a triage with cytology, provided that only those with cytological atypia are referred for colposcopy. This is true for an organized screening scenario, that is, one in which there is a control of who should be screened at the recommended time intervals. There are only a few municipalities with organized cervical cancer screening programs in Brazil. There is no suitable control of the women who carry out their screening or how often they do it. Thus, there are no tools to ensure that the interval between screening tests will be effectively widened with the adoption of an HPV-DNA test, nor that women missed by this screening program will be identified. Furthermore, in most Brazilian municipalities, the cost-effectiveness improvement of HPV-DNA testing is not warranted. Given this background, the use of this technology in each and every municipality of Brazil can only be recommended once their screening program is organized and operational.
Recommendations
Testing based on HPV-DNA as an alternative to cytology in cervical cancer screening should be performed every 5 years in women aged 30 years or older, and may be extended up to when the patients are 64 years of age (B). Testing for HPV-DNA is unacceptable before the age of 30 (D). When an HPV-DNA test is positive for oncogenic types, a cytology exam should be performed, preferably using the same sample, since no further sampling would be necessary. Therefore, the recommended medium for HPV-DNA test collection is the same as for liquid-based cytology (B).
If an HPV-DNA test is positive for oncogenic types and the cytology shows any atypia (ASC-US or worse), the woman should be referred for colposcopy (A). Instead, if the cytology is negative, the woman should repeat the HPV-DNA test after 12 months (A). If the HPV-DNA result remains positive for oncogenic types, the woman should be referred for colposcopy (A). If the sample is negative for oncogenic HPV on the first or second sampling opportunity after a negative cytology, a new cytology exam must be performed after three years (A). If HPV-DNA genotyping is available and is positive for HPV types 16 or 18, the woman should be directly referred for colposcopy, bypassing the cytology test (A). If an HPV-DNA test (with or without genotyping) is negative, it should be repeated in 5 years (A). Any therapeutic procedure performed because of a positive HPV-DNA test is unacceptable (D). Women between the ages of 25 and 29 should keep performing cytology tests (A). Women aged 65 years or older who tested negative for HPV-DNA may discontinue screening (B). Fig. 1 summarizes the recommendations for the use of HPV-DNA tests in cervical cancer screening.
Fig. 1.
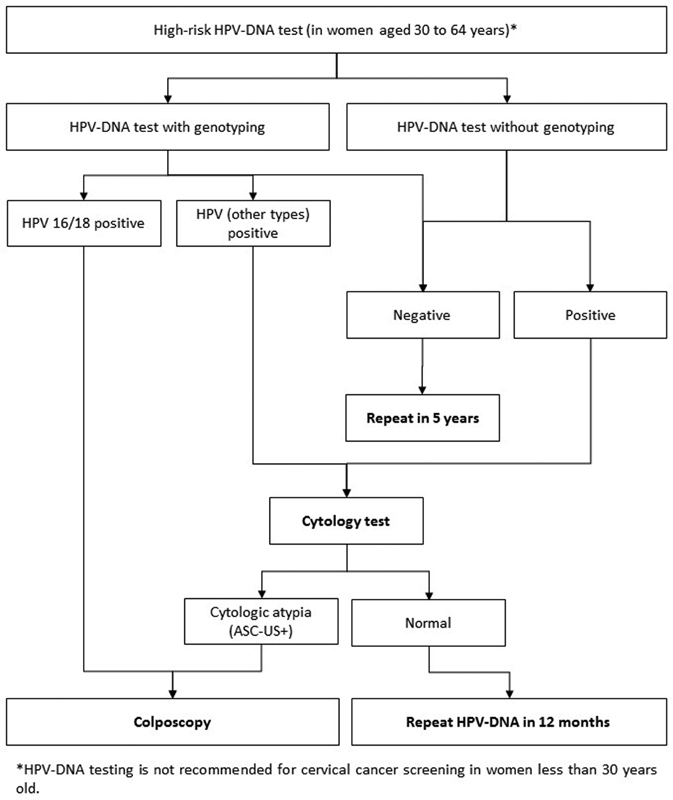
Recommendations for HPV-DNA testing in cervical cancer screening in women aged 30 to 64 years.*
Use of HPV-DNA Tests in the Follow-up of Women with Abnormal Cytology Results
Atypical Squamous Cells
Atypical Squamous Cells of Undetermined Significance (ASC-US), Possibly Non-neoplastic
The cytology diagnosis of atypical squamous cells of undetermined significance (ASC-US) does not mean, in most cases, the presence of a precursor lesion or cancer. However, identifying which women with this diagnosis are more likely to have one of these lesions has led to several screening recommendations for colposcopy referral.
As mentioned in the Brazilian Guidelines for Cervical Cancer Screening,1 there is a similarity among management recommendations for woman with ASC-US in France,14 the United Kingdom,15 and Australia and New Zealand.16 In these countries, a repeat cytology test is recommended after 6 to 12 months. The American Society for Colposcopy and Cervical Pathology (ASCCP) states that using the oncogenic HPV-DNA test for women aged over 25 with ASC-US cytology is preferable to cytology. This same guideline states that this test is acceptable in 21- to 24-year-old women with ASC-US, but repeat cytology is preferable in this age range.17 The guidelines published in Korea18 and Argentina19 follow ASCCP recommendations and endorse the use of oncogenic HPV-DNA testing in women with ASC-US cytology.
Recommendations
Women with ASC-US cytology can perform the HPV-DNA test alternatively to a new cytology test within 6 months. If the test is positive for oncogenic types, the woman should be referred for colposcopy (A).
The HPV-DNA test can also be used to outline the follow-up of women with ASC-US cytology aged 30 years or older after a negative colposcopy. If the test is positive, the woman should be followed in the primary care unit in the same way as the others. She should undergo a new cytology test every 6 months (for women aged 30 years or more) or annually (for younger women) (I) until 2 consecutive negative test results are achieved, then she should return to triennial cytological screening, unless a different cytology result occurs (A). If the HPV-DNA test is negative for oncogenic types, this woman may return to triennial screening (A).
Atypical Squamous Cells, Cannot Exclude High Squamous Grade Intraepithelial Lesion (ASC-H)
Differently from the diagnosis of ASC-US, in the presence of atypical squamous cells, cannot exclude high squamous grade intraepithelial lesion (ASC-H), the probability of a precursor lesion or cancer is significantly higher. Of all current recommendations, the most favored is referral to colposcopy.
However, in many cases, colposcopy cannot ensure there is no lesion, and a negative oncogenic HPV-DNA test virtually ensures its absence (evidence level: moderate).20
Recommendations
When available, the HPV-DNA test may also be used in women with an ASC-H cytology who have a type-III transformation zone (TZ) and no abnormal colposcopy findings (B). If there is no oncogenic HPV, this woman may return to triennial cytology screening (I). If there are abnormal findings, this woman should continue to undergo the investigation of the endocervical canal as recommended by the Brazilian Guidelines for Cervical Cancer Screening (I). If the presence of a precursor or invasive lesion is not proven, the HPV-DNA test may also be used at the follow-up. In this case, it should be performed within 6 months of the initial cytology test (A). If there is no oncogenic HPV, this woman can go back to triennial screening (A). If oncogenic HPV is present, this woman should be referred for colposcopy to ensure there are no precursor lesions (I).
In postmenopausal women with an ASC-H cytology test, the HPV-DNA test may also be used, avoiding topical estrogens before a new colposcopy, as indicated in the Brazilian Guidelines (I). If there is no oncogenic HPV, this woman may return to triennial cytological screening (I). If positive for oncogenic HPV, she should be followed as recommended in the Brazilian Guidelines for Cervical Cancer Screening: continuation of the investigation, preferably with estrogen preparation (I).
Atypical Glandular Cells (AGC)
Atypical Glandular Cells of Undetermined Significance, Possibly Non-neoplastic or Atypical Glandular Cells in Which High-grade Intraepithelial Lesions Cannot Be Ruled Out
Atypical glandular cells are another challenge. The prevalence of precursor lesions and invasive disease in women with this cytological diagnosis is higher than in women with ASC-US. In addition, most glandular lesions are in the endocervical canal, which is often a colposcopic challenge, with less specific colposcopic findings than those of squamous lesions.
Considering the limitations of cytology and colposcopy in such situations, the HPV-DNA test may provide additional information to the investigation. The presence of oncogenic HPV-DNA also showed association with invasive or precursor glandular disease (evidence level: high).21 The probability that an intraepithelial lesion may reach 40% when oncogenic HPV types are present, compared with 4% when absent, points to a possible use of this test in the investigation of these women (evidence level: high).22
Recommendations
In women with an AGC cytology, and in situations in which the colposcopy cannot ensure the absence of glandular disease, a negative oncogenic HPV-DNA test will virtually rule out precursor or malignant disease of the cervix (A).
Low-grade Squamous Intraepithelial Lesion (LSIL)
This cytology result implies a low probability of cancer or a precursor lesion. In order to identify women at a greater risk of developing these diseases and to define the need to refer them for colposcopy, the use of HPV-DNA tests was proposed. In this situation, HPV-DNA tests have a significantly higher sensitivity, but significantly lower specificity, when compared with repeat cytology (evidence level: high).23 The low specificity of HPV-DNA tests is due to the high HPV prevalence in women with LSIL (76.9%) (evidence level: high),24 which would imply the referral of most women for colposcopy, compromising the cost-effectiveness strategy. However, a positive HPV-DNA test is determined by the prevalence of HPV infection, which in turn is age-dependent. More recent studies have shown that several HPV-DNA tests have increased specificity with increasing age, in addition to high sensitivity, for the detection of CIN II + in women with LSIL (evidence level: high).25 26 Scientific evidence suggests that HPV-DNA tests may be useful for the triage of older women with LSIL. However, because of the lack of stratified data, we don't have enough evidence to recommend the best moment to use it in this situation (evidence level: high).27
A meta-analysis of studies on the performance of HPV-DNA test as a triage for the colposcopy of women with LSIL cytology published in 2013 concluded that these tests may have a greater ability to detect cases of NIC II +. However, their use should be weighed against the costs of the testing and the colposcopy, in addition to the adherence to follow-up. Furthermore, they point out that DNA-HPV tests are certainly useless in young women with LSIL, that more studies are needed to define their usefulness in the triage of older women (in the US it is recommended for postmenopausal women), and that higher cut-off points might be used to consider the test positive (evidence level: high).22
In the follow-up after colposcopy, if there are no abnormal findings, or when the result is compatible with CIN I or a less severe type, the sensitivity of the biannual cytology control and the 12-month HPV-DNA test for CIN II+ detection was similar (89% and 92% respectively). However, the referral rates for new colposcopy were different (64% for cytology and 55% for HPV-DNA), pointing to a higher cost-effectiveness of the HPV-DNA test (evidence level: high).26
Recommendations
Where HPV-DNA testing is available, it may be used in women with LSIL cytology who are aged 30 years or older for referral for colposcopy. If the HPV-DNA test is negative for oncogenic types, the woman should return to triennial cytology screening (I). If the HPV-DNA test is positive for oncogenic types, the woman should be referred for colposcopy (I). In addition, after the first colposcopy, in the follow-up of the women with no abnormal findings or after the histology diagnosis of CIN I, a 12-month HPV-DNA test may be used (A) as an option. When oncogenic types are present, the follow-up should be continued as aforementioned (A). Negative cases should go back to the triennial cytology screening routine (A).
High-grade Squamous Intraepithelial Lesion (HSIL)
The use of HPV-DNA tests is of no value for the colposcopy referral of women after this cytology result. However, in view of the high prevalence of oncogenic HPV types in precursor lesions (evidence level: high),20 it can be useful in situations in which the colposcopy cannot rule out disease.
Recommendations
In cases of high-grade squamous intraepithelial lesion (HSIL) cytology, the HPV-DNA test, when available, may be used only if there are normal or low-grade colposcopy findings. If no oncogenic types are present, precursor or invasive disease is virtually excluded, and the woman can return to triennial cytology screening (A).
Adenocarcinoma in situ (AIS) and Invasive Adenocarcinoma
These cytology results are a challenge for colposcopy. These lesions are usually located inside the endocervical canal and are not easily recognized, even by experts. Occasionally, the disease may come from the endometrium or other pelvic organs.
As a result, there usually are no abnormal findings at the colposcopy, and that requires an excisional diagnostic procedure, as well as investigation of the endometrium and other pelvic organs in women aged 35 years or older, or below that age if there is any abnormal bleeding.1
A negative oncogenic HPV-DNA test may be useful in identifying women at a higher risk of having endometrial disease, especially those over 50 years of age (evidence level: moderate).28
Recommendations
Where available, HPV testing may be used in the initial investigation of women with a cytology result of adenocarcinoma in situ (AIS) or invasive adenocarcinoma. If negative, this will mean a lower probability of having cervical disease, and that will endorse the evaluation of the endometrium as well as of other pelvic organs in women aged 35 years or older and in those with abnormal bleeding under 35 years of age (I).
Use of the HPV-DNA Test in the Follow-up of Women Treated for Cervical Cancer Precursor Lesions
After Treatment of CIN II/III
Long-term follow-up studies indicate that women treated for CIN II/III are at a higher risk of developing cervical cancer for at least 10 years, and perhaps up to 20 years after treatment, when compared with the general population (evidence level: high).29
The ideal follow-up for the detection of residual or recurrent disease appears to be cytology associated with colposcopy, but current data suggests that the HPV-DNA test identifies disease earlier, with greater sensitivity and specificity, than the cytology follow-up (evidence level: moderate).30
Several studies have reported the elimination or persistence of HPV infections after the treatment of high-grade squamous intraepithelial cervical lesions. These reports vary, and they sometimes show conflicting results. One study reported that out of 49 women treated with large loop excision of the transformation zone (LLETZ), only 6 (12.2%) persisted with viral infection 3 months after the treatment (evidence level: moderate).28 Another study identified that at 31 months of follow-up after a high-grade lesion treatment, the HPV-DNA test was still positive in 19.6% of the patients, and no longer detectable in 80.4% of the women (evidence level: moderate).31 Another study showed that 94% of women with a positive HPV-DNA test before treatment had cleared the infection in 12 months (evidence level: moderate).32
Brazilian studies showed that most patients undergoing excisional treatment for high-grade lesions were negative for HPV-DNA six months after the procedure (evidence level: moderate).33
Recommendations
The HPV-DNA test may be used for follow-up after NIC II/III treatment to exclude residual or recurrent lesions. In this case, it should be performed between 6 and 12 months after the treatment (A). If cleared from oncogenic types, the woman may return to triennial cytological screening (A).
After Treatment of Adenocarcinoma in situ
The HPV-DNA test can also be useful after a conservative treatment for AIS (when the uterus is maintained) because, if negative, it indicates that the patients have a lower risk of persistence and relapse (evidence level: moderate).34
Recommendations
The HPV-DNA test may be used at follow-up after a conservative AIS treatment (when the uterus is maintained) to exclude residual or recurrent lesion. In this case, it should be performed 6 to 12 months after the treatment (A). If the oncogenic HPV-DNA test is negative, the woman may return to triennial cytological screening (A).
Acknowledgments
The authors would like to thank the following collaborators, who took part in the reviewer groups: Adalberto Xavier Ferro Filho, Adriana Campaner, Andréa Cytryn, Angela Rosa Imperio Meyrelles, Dulcimary Dias Bitencourt, Edison Natal Fedrizzi, Etelvino de Souza Trindade, Evandro Russo, Filomena Aste, Gulnar Azevedo e Silva, Gutemberg Almeida, José Eluf Neto, José Humberto Fregnani, Juliana Monteiro, Letícia Katz, Lise P. Cury, Manoel Afonso Gonçalves, Marcia Terra Cardial, Maria José de Camargo, Maricy Tacla, Marise Moreira, Nathalie Raibolt, Neila Speck, Newton Carvalho, Paulo Sérgio Viero Naud, Renato Bravo, Rosane Figueiredo Alves, Susana Aidé, Tania Lago e Wanuzia Miranda Moreira.
Footnotes
Conflicts of Interest The authors have none to declare.
References
- 1.Ministério da Saúde. Instituto Nacional de Câncer José Alencar Gomes da Silva. Coordenação de Prevenção. Diretrizes Brasileiras para o Rastreamento do Câncer do Colo do Útero. 2ª ed Rio de Janeiro, RJ: INCA; 2016 [Google Scholar]
- 2.Ministério da Saúde. Instituto Nacional de Câncer José Alencar Gomes da Silva. Diretrizes Brasileiras para o Rastreamento do Câncer do Colo do Útero Rio de Janeiro, RJ: INCA; 2011 [Google Scholar]
- 3.US Preventive Services Task Force. Grade Definitions 2013. https://www.uspreventiveservicestaskforce.org/Page/Name/grade-definitions. Accessed Dec 19, 2016
- 4.Basu P, Mittal S, Bhadra Vale D, Chami Kharaji Y.Secondary prevention of cervical cancer Best Pract Res Clin Obstet Gynaecol 20184773–85.. Doi: 10.1016/j.bpobgyn.2017.08.012 [DOI] [PubMed] [Google Scholar]
- 5.Schiffman M, Doorbar J, Wentzensen Net al. Carcinogenic human papillomavirus infection Nat Rev Dis Primers 2016216086. Doi: 10.1038/nrdp.2016.86 [DOI] [PubMed] [Google Scholar]
- 6.Ronco G, Giorgi-Rossi P, Carozzi Fet al. Efficacy of human papillomavirus testing for the detection of invasive cervical cancers and cervical intraepithelial neoplasia: a randomised controlled trial Lancet Oncol 20101103249–257.. Doi: 10.1016/S1470-2045(09)70360-2 [DOI] [PubMed] [Google Scholar]
- 7.Arbyn M, Verdoodt F, Snijders P JFet al. Accuracy of human papillomavirus testing on self-collected versus clinician-collected samples: a meta-analysis Lancet Oncol 20141502172–183.. Doi: 10.1016/S1470-2045(13)70570-9 [DOI] [PubMed] [Google Scholar]
- 8.Koliopoulos G, Nyaga V N, Santesso Net al. Cytology versus HPV testing for cervical cancer screening in the general population Cochrane Database Syst Rev 20178CD008587. Doi: 10.1002/14651858.CD008587.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Muwonge R, Wesley R S, Nene B Met al. Evaluation of cytology and visual triage of human papillomavirus-positive women in cervical cancer prevention in India Int J Cancer 2014134122902–2909.. Doi: 10.1002/ijc.28627 [DOI] [PubMed] [Google Scholar]
- 10.Naucler P, Ryd W, Törnberg Set al. Human papillomavirus and Papanicolaou tests to screen for cervical cancer N Engl J Med 2007357161589–1597.. Doi: 10.1056/NEJMoa073204 [DOI] [PubMed] [Google Scholar]
- 11.Khan M J, Castle P E, Lorincz A Tet al. The elevated 10-year risk of cervical precancer and cancer in women with human papillomavirus (HPV) type 16 or 18 and the possible utility of type-specific HPV testing in clinical practice J Natl Cancer Inst 200597141072–1079.. Doi: 10.1093/jnci/dji187 [DOI] [PubMed] [Google Scholar]
- 12.Thomsen L T, Frederiksen K, Munk C, Junge J, Iftner T, Kjaer S K.Long-term risk of cervical intraepithelial neoplasia grade 3 or worse according to high-risk human papillomavirus genotype and semi-quantitative viral load among 33,288 women with normal cervical cytology Int J Cancer 201513701193–203.. Doi: 10.1002/ijc.29374 [DOI] [PubMed] [Google Scholar]
- 13.Wright T C, Stoler M H, Behrens C M, Sharma A, Zhang G, Wright T L.Primary cervical cancer screening with human papillomavirus: end of study results from the ATHENA study using HPV as the first-line screening test Gynecol Oncol 201513602189–197.. Doi: 10.1016/j.ygyno.2014.11.076 [DOI] [PubMed] [Google Scholar]
- 14.Management of a Patient with an Abnormal Cervical Smear: 2002 Update. http://www.has-sante.fr/portail/upload/docs/application/pdf/Frottis_anglais.pdf. Accessed Dec 19, 2016
- 15.Screening C.Programme and Colposcopy Management. 2016 https://www.gov.uk/government/publications/cervical-screening-programme-and-colposcopy-management. Accessed Dec 19, 2016
- 16.Ministry of Health. National Cervical Screening Programme. Guidelines for Cervical Screening in New Zealand: Incorporating the Management of Women with Abnormal Cervical Smears. 2008 https://www.health.govt.nz/system/files/documents/publications/cervical-screening-guidelines-aug08.pdf. Accessed Dec 19, 2016
- 17.Massad L S, Einstein M H, Huh W Ket al. 2012 updated consensus guidelines for the management of abnormal cervical cancer screening tests and cancer precursors Obstet Gynecol 201312104829–846.. Doi: 10.1097/AOG.0b013e3182883a34 [DOI] [PubMed] [Google Scholar]
- 18.Lee J K, Hong J H, Kang Set al. Practice guidelines for the early detection of cervical cancer in Korea: Korean Society of Gynecologic Oncology and the Korean Society for Cytopathology 2012 edition J Gynecol Oncol 20132402186–203.. Doi: 10.3802/jgo.2013.24.2.186 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Arrossi S, Paul L, Thouyaret L.Prevención del Cáncer Cervicouterino. Buenos Aires: Instituto Nacional del Cáncer; 2015 http://www.msal.gob.ar/images/stories/bes/graficos/0000000017cnt-manual_recomendaciones_tamizaje_2015_baja.pdf. Accessed Dec 19, 2016
- 20.Bandyopadhyay S, Austin R M, Dabbs D, Zhao C.Adjunctive human papillomavirus DNA testing is a useful option in some clinical settings for disease risk assessment and triage of females with ASC-H Papanicolaou test results Arch Pathol Lab Med 2008132121874–1881.. Doi: 10.1043/1543-2165-132.12.1874 [DOI] [PubMed] [Google Scholar]
- 21.Longatto-Filho A, Erzen M, Branca Met al. Human papillomavirus testing as an optional screening tool in low-resource settings of Latin America: experience from the Latin American Screening study Int J Gynecol Cancer 20061603955–962.. Doi: 10.1111/j.1525-1438.2006.00582.x [DOI] [PubMed] [Google Scholar]
- 22.Zeferino L C, Rabelo-Santos S H, Villa L Let al. Value of HPV-DNA test in women with cytological diagnosis of atypical glandular cells (AGC) Eur J Obstet Gynecol Reprod Biol 201115901160–164.. Doi: 10.1016/j.ejogrb.2011.05.023 [DOI] [PubMed] [Google Scholar]
- 23.Arbyn M, Roelens J, Simoens Cet al. Human papillomavirus testing versus repeat cytology for triage of minor cytological cervical lesions Cochrane Database Syst Rev 201303CD008054. Doi: 10.1002/14651858.CD008054.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Arbyn M, Ronco G, Anttila Aet al. Evidence regarding human papillomavirus testing in secondary prevention of cervical cancer Vaccine 20123005F88–F99.. Doi: 10.1016/j.vaccine.2012.06.095 [DOI] [PubMed] [Google Scholar]
- 25.Corrêa F M, Russomano F B, Oliveira C A.Colposcopic triage methods for detecting cervical intraepithelial neoplasia grade 3 after cytopathological diagnosis of low-grade squamous intraepithelial lesion: a systematic review on diagnostic tests Sao Paulo Med J 20121300144–52.. Doi: 10.1590/S1516-31802012000100008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cuzick J, Thomas Cox J, Zhang Get al. Human papillomavirus testing for triage of women with low-grade squamous intraepithelial lesions Int J Cancer 201313204959–966.. Doi: 10.1002/ijc.27723 [DOI] [PubMed] [Google Scholar]
- 27.Guido R, Schiffman M, Solomon D, Burke L. ASCUS LSIL Triage Study (ALTS) Group. Postcolposcopy management strategies for women referred with low-grade squamous intraepithelial lesions or human papillomavirus DNA-positive atypical squamous cells of undetermined significance: a two-year prospective study Am J Obstet Gynecol 2003188061401–1405.. Doi: 10.1067/mob.2003.456 [DOI] [PubMed] [Google Scholar]
- 28.Castle P E, Fetterman B, Poitras N, Lorey T, Shaber R, Kinney W.Relationship of atypical glandular cell cytology, age and human papillomavirus detection to cervical and endometrial cancer risks Obstet Gynecol 2010115(2 Pt 1):243–248.. Doi: 10.1097/AOG.0b013e3181c799a3 [DOI] [PubMed] [Google Scholar]
- 29.Melnikow J, McGahan C, Sawaya G F, Ehlen T, Coldman A.Cervical intraepithelial neoplasia outcomes after treatment: long-term follow-up from the British Columbia Cohort Study J Natl Cancer Inst 200910110721–728.. Doi: 10.1093/jnci/djp089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kitchener H C, Walker P G, Nelson Let al. HPV testing as an adjunct to cytology in the follow up of women treated for cervical intraepithelial neoplasia BJOG 2008115081001–1007.. Doi: 10.1111/j.1471-0528.2008.01748.x [DOI] [PubMed] [Google Scholar]
- 31.Park J Y, Kim D Y, Kim J H, Kim Y M, Kim Y T, Nam J H.Human papillomavirus test after conization in predicting residual disease in subsequent hysterectomy specimens Obstet Gynecol 20091140187–92.. Doi: 10.1097/AOG.0b013e3181ab6dca [DOI] [PubMed] [Google Scholar]
- 32.Kreimer A R, Schiffman M, Herrero Ret al. Long-term risk of recurrent cervical human papillomavirus infection and precancer and cancer following excisional treatment Int J Cancer 201213101211–218.. Doi: 10.1002/ijc.26349 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Roncaglia M T, Tacla M, Vieira da Motta Eet al. Evaluation of the combination of cytology and hybrid capture to safely predict the high-grade lesion status of patients treated with conization with large loop excision of the transformation zone Acta Cytol 20115505421–425.. Doi: 10.1159/000330808 [DOI] [PubMed] [Google Scholar]
- 34.Lea J S, Shin C H, Sheets E Eet al. Endocervical curettage at conization to predict residual cervical adenocarcinoma in situ Gynecol Oncol 20028701129–132.. Doi: 10.1006/gyno.2002.6791 [DOI] [PubMed] [Google Scholar]