

Abstract
Purpose Identify factors associated with infant mortality by a hierarchical model based on socioeconomic, health care, obstetric and biological determinants in a northeastern Brazilian capital.
Methods Observational, retrospective cohort study based on secondary data of births and deaths of infants of mothers living in the city of Teresina.
Results Based on the distal level of determination of infant mortality, the characteristics that remained statistically significant were maternal age, maternal education and maternal occupation (p < 0.001). In the intermediate level, all variables were statistically significant, particularly the type of pregnancy and delivery (p < 0.001). The gender of the baby was the proximal level feature that had no significant association with the outcome, while the other variables of this level had association (p < 0.001).
Conclusions This study evidenced that, in addition to biological factors, socioeconomic status and maternal and child health care are important to determine infant mortality.
Keywords: infant mortality, risk factors, information systems, health planning
Abstract
Resumo
Objetivo Identificar os fatores associados à mortalidade infantil por modelo hierárquico segundo determinantes socioeconômicos, assistenciais, obstétricos e biológicos em uma capital do Nordeste brasileiro.
Métodos Estudo observacional, de coorte retrospectiva, com base em dados secundários de nascimentos e óbitos de crianças menores de um ano, de mães residentes no município de Teresina (PI).
Resultados Para o nível distal de determinação da mortalidade infantil, as características que se mantiveram estatisticamente significativas foram idade materna, escolaridade materna e ocupação materna, com p < 0,001. No intermediário, todas as variáveis apresentaram significância estatística, com destaque para o tipo de gravidez e de parto, com p < 0,001. O sexo do bebê representou a característica do nível proximal que não obteve associação significativa com o desfecho, enquanto as demais variáveis desse nível estavam associadas, com p < 0,001.
Conclusões Além da determinação da mortalidade infantil pelos fatores biológicos, destacou-se a importância da condição socioeconômica e da assistência à saúde materno-infantil.
Palavras-chave: mortalidade infantil, fatores de risco, sistemas de informação, planejamento em saúde
Introduction
The worldwide concern about infant mortality gained visibility with the publication, in 2000, of the Millennium Development Goals, in which reduction in infant mortality was highlighted as goal number 4, which proposed to reduce by two thirds the mortality rate in children younger than five years old, in the period between 1990 and 2015. Additionally, it represents a critical point to achieve other goals related to welfare, equality and poverty reduction. Brazil is a signatory of these goals.1 2
It is known that in Brazil there is a high level of heterogeneity among the country's regions caused by sharp socioeconomic and cultural differences, in addition to inequality in access to health services. Thus, the investigation of infant mortality and its risk factors at the local level is relevant.3
The study of the risk factors involved in the causal chain of infant mortality is crucial to understand the living conditions of the maternal and child population, to define the priority actions for proper public policies for each situation, and to develop strategies to control and organize the healthcare network.
Because of its sensitivity to the living and health conditions of the population, infant mortality is determined by factors of different dimensions. However, it is not uncommon to find situations in which socioeconomic and health care factors are superficially analyzed due to the presence of biological factors.4
In this sense, strategies with hierarchical data analysis (which takes into account the temporal precedence of these factors, the potential relationship between them and their relevance to determine the outcome) have been used as alternatives to the analyses based only on statistical associations.5 6
This strategy is based on the construction of a conceptual model aiming to establish a hierarchical relationship between the effects of exposure variables on the outcome studied, assuming that its effect on the occurrence of this event can be direct or through other variables.7 8
Data from the official Health Care Information Systems in Brazil, particularly the Mortality Information System (Sistema de Informações sobre Mortalidade, SIM) and Live Birth Information System (Sistema de Informação sobre Nascidos Vivos, SINASC), have been widely used to monitor infant mortality in Brazil. However, their use to carry out epidemiological studies depends on the coverage degree of the event in question, in addition to the completeness, reliability and validity of their data.6 Studies have shown progressive improvement of these systems with an increasing level of coverage and improved quality of their data.7 9 10
The possibility to use linkage or another database relationship methodology is highlighted as an important strategy to improve the quality of the national healthcare information systems, identifying and recovering information that are present in a system and missing or incomplete in another.11
Given the above mentioned, this study aims to identify, through linkage, factors associated with infant mortality using a hierarchical model based on socioeconomic, health care, obstetric and biological determinants, in a northeastern Brazilian capital.
Methods
This is an observational, retrospective cohort study based on secondary data of births and deaths of infants of mothers living in Teresina in 2011.
The study population comprised the number of live births (N = 13,882) of mothers living in Teresina, with delivery occurring in the same capital, in the period from January 1st, 2011, to December 31st, 2011. Also included in this population are the deaths of infants (n = 207) from those live births in the study, comprising the deaths occurred between January 1st, 2011, and December 31st, 2012. The year 2011 was chosen because it represents the most recent period of data availability at the time of collection.
The study was performed in Teresina, capital of the state of Piauí, located in the Northeast of Brazil. The city has a population of 814,230 inhabitants, and 94.27% of them live in urban areas, according to the 2010 census of the Brazilian Institute of Geography and Statistics.12 Currently, it ranks 8th among the capitals in the northeastern states in relation to the Gross Domestic Product. Services focused on health care are meeting the demands in the countryside of the states of Piauí, Maranhão, Pará, Amapá, the North of Tocantins and the West of Ceará.13 As shown in Table 1, in order to meet the highly complex demands in child health care in Teresina, there are 35 beds in the Neonatal Intensive Care Unit (Maternidade Municipal Professor Wall Ferraz e Maternidade Dona Evangelina Rosa, Teresina, Brazil), 27 of which are for patients assisted by the Brazilian Unified Health Care System (Sistema Único de Saúde, SUS); and 29 beds in the Pediatric ICU (Hospital de Urgência de Teresina and Hospital Infantil Lucídio Portela, Teresina, Brazil), with 22 of them for SUS patients.14
Table 1. List of beds intended for the maternal and child population in Teresina, Piauí, Brazil.
| Description | Existing | SUS | Non-SUS |
|---|---|---|---|
| Neonatology | 23 | 23 | 0 |
| Neonatal Intermediate Unit | 15 | 5 | 10 |
| Neonatal Intermediate Care Unit | 53 | 23 | 30 |
| Neonatal Intensive Care Unit | 35 | 27 | 8 |
| Clinical Pediatrics | 341 | 279 | 62 |
| Surgical Pediatrics | 18 | 10 | 8 |
| Pediatric Intermediate Care Unit | 2 | 2 | 0 |
| Pediatric Intensive Care Unit | 29 | 22 | 7 |
| Clinical Obstetrics | 77 | 67 | 10 |
| Surgical Obstetrics | 252 | 206 | 46 |
Abbreviation: SUS, Brazilian Unified Health Care System.
Source: Brasil (2014).14
Data collection was performed from January to April, 2014. The Health Information Center of the Municipal Health Foundation in Teresina provided the report with the digital files from the SIM and SINASC databases with a list of live births in 2011 of mothers living in the city of Teresina; additionally, a list of deaths of infants and stillbirths for the years 2011 and 2012 of mothers living in Teresina was also provided.
Then, data collection was performed among the original death certificates (DCs) for the years of 2011 and 2012. This step was taken to find potential deaths that, perhaps, were not included in the digital system SIM. Stillbirths in 2011 were searched to identify potential death misclassification.
Ten original DCs were not found in this file, and copies of these originals were requested from the health care facilities where the deaths occurred, so they could be restored and filed. For the Statements of Live Births (SLBs) not found in the system, active searches by date of birth were performed at the health care facilities where the deaths occurred.
Determinist linkage was performed through the variable “SLB number” filled in the DC. Deaths not matching their SLB deterministically were paired in a probabilistic manner using the variables “mother's name,” “date of birth of the newborn” and “gender of the newborn”. All pairs were reviewed to minimize the presence of bias. Information contained in SINASC were considered gold standard in the case of disagreement or missing information in SIM.
Categorization of independent variables (Table 2) was performed for a hierarchical analysis according to the theoretical model for determination of infant mortality based on a hierarchical relationship (temporal and causal) between them, at three levels of determinants: distal, intermediate and proximal (Fig. 1). The dependent variable or outcome corresponded to the occurrence of infant death.
Table 2. Categorization of variables, Teresina, Piauí, Brazil.
| Variable | Categories | Categorization |
|---|---|---|
| Mother race | White Non-white |
White Brown, black, yellow |
| Mother marital status | With partner No partner |
Married, stable relationship Single, widow, legally separated |
| Mother age | 10–19 years 20–34 years ≥ 35 years |
10–19 years 20–34 years Higher and equal to 35 years |
| Mother education | Low Intermediate High |
Adjustment between mother's age and education expected for each age group |
| Mother occupation | With remuneration No remuneration |
With remuneration No remuneration |
| Hospital type | SUS Non-SUS |
SUS Non-SUS |
| Parity | First time Multiparous |
No live birth or still birth in previous pregnancies With one or more live births or still births from previous pregnancies |
| Pregnancy type | Single Multiple |
Single Double, triple or more |
| Delivery type | Vaginal Cesarean |
Vaginal Cesarean |
| Prenatal | Did not perform Inappropriate Appropriate |
Correspondence between the number of prenatal visits and gestational age |
| Gender | Female Male |
Female Male |
| Gestational age | Preterm Term Post-term |
Less than or equal to 36 weeks of pregnancy 37–41 weeks of pregnancy Greater than or equal to 42 weeks of pregnancy |
| Weight | Low weight Normal |
Less than or equal to 2499 g Greater than or equal to 2500 g |
| Apgar 1st min | 0–3 4–6 7–10 |
Severe asphyxia Moderate asphyxia No asphyxia |
| Apgar 5th min | 0–3 4–6 7–10 |
Severe asphyxia Moderate asphyxia No asphyxia |
| Congenital malformation | Yes No |
Presence of congenital malformation Absence of congenital malformation |
Abbreviations: SUS, Brazilian Unified Health Care System; min, minute.
Source: Santos et al.11
Fig. 1.
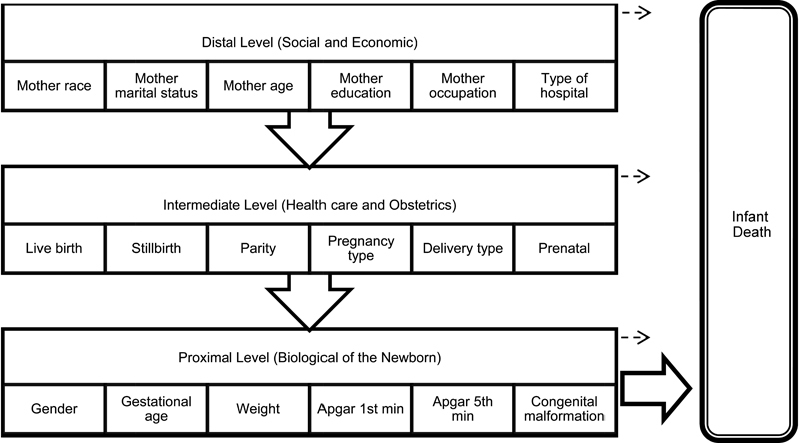
Conceptual hierarchical model for the factors associated with infant mortality, Teresina, Piauí, Brazil. Source: Santos et al (2014).11
The variable “maternal education” was adjusted according to the mother's age in: low, intermediate and high, in order for it to be compatible with the expected education for each age group. According to a study by Sampaio and Nespoli,15 to provide appropriate old: years of school ratio, a 9-year old student should have at least 1 year of education completed, a 10-year-old with at least 2 years of study completed and so on.15
Based on this premise, the category “low” was considered for all ages as those with no years of education; for mothers aged 17–19 years, those with 1 to 3 years of education; and for mothers aged 20 years or more, those with 1 to 7 years of education. For the category “intermediate,” the following was included: mothers aged 13–16 years who had 1 to 3 years of education; mothers aged 17–19 years who had 4 to 7 years of education; and mothers aged 20 years or more who had 8 to 11 years of education. The category “high” comprised mothers aged 9–12 years who had at least 1 year of education; mothers aged 13–16 years, with at least 4 years of education; mothers aged 17–19 years, with at least 8 years of education; and mothers aged 20 years or more who had at least 12 years of education.
The variable “prenatal care” was obtained from the correspondence between the number of prenatal visits and the gestational age, and categorized according to the recommendations of the Brazilian Ministry of Health as: “not performed”, “inappropriate” and “appropriate”. The first prenatal visit should start early in the first trimester, and should be regular, with visits performed monthly until the 28th week; every other week between the 28th and 36th week; and weekly between the 36th and 41st weeks.16
The category “not performed” comprised mothers who did not have any prenatal visit. In the “inappropriate” category were included newborns with gestational age of 28–36 weeks and 1 to 3 prenatal visits, and those with gestational age of 37 weeks or higher and 1 to 6 visits. The category “appropriate” comprised newborns with gestational age of 27 weeks or older and at least 1 visit performed, those with 28–36 weeks of gestational age with at least 4 visits, and those with a gestational age of 37 weeks or older with at least 7 visits performed.
The variable “congenital malformation” was defined by the presence or absence of malformation recorded on SINASC, along with the analysis of the underlying cause of death recorded on SIM. Some birth defects are not diagnosed at birth and, therefore, do not appear on the SINASC, and sometimes can be identified as one of the underlying causes of death recorded on SIM.17
To organize, tabulate the data, list the database searched and format results, the software Microsoft Excel for Windows® was used with double data entry to reduce the presence of bias. Statistical analyses were performed using the SPSS 20.0 software (Statistical Package for the Social Sciences Inc., Chicago, USA).
It is emphasized that the open variables were re-categorized in order to become closed and make feasible the statistical analysis. To explain the effect “set of independent variables” on infant mortality, Multivariate Logistic Regression (MLR) was used, adjusted by the Enter method with the hierarchical input of variables (Fig. 1).18
The multicollinearity test required for MLR was performed by the Variance Inflation Factor (VIF), taking as cut-off point for the diagnosis of multicollinearity one VIF above four; however, the test did not detect multicollinearity between the variables studied. Hosmer and Lemeshow19 test was used as a quality measure of MLR adjustment.
In the final model, a 5% level of significance was used for analysis, and the variables were considered significant with a p-value ≤ 0.05 (p = Wald test), and 95% confidence interval (CI95%). The association measurement used was Odds Ratio adjusted (ORadj), and a reference category was set (ORadj equal to 1) to the lower risk for occurrence of the outcome.20
The project was registered at Plataforma Brasil under the CAAE (Certificado de Apresenta¸ão para Aprecia¸ão Ética) number 21832513.0.0000.5214, and forwarded to the Institutional Review Board at the Federal University of Piauí to analyze the ethical aspects of the study, in accordance with the regulatory guidelines and standards for human research of the Brazilian National Health Council Resolution No. 466, dated December 12, 2012.21 The study was approved under the opinion letter No. 514.075.
Results
For the distal level for determination of infant mortality, the characteristics that remained statistically significant after applying the hierarchical MLR model were maternal age, maternal education and maternal occupation (p < 0.001) (Table 3). Mothers aged 20–34 years (ORadj = 5.11; CI95% 3.80–6.46) had the strongest association with infant mortality, followed by teenage mothers, who had a higher chance of death (2.82 times compared with mothers aged 35 years or more). The results for maternal education were unexpected, since mothers with low education were the group with stronger association with the outcome (ORadj = 1.85; CI95% 1.43–2.32), as well as the high education group, whose association was 1.28 times stronger when compared with the group with intermediate education. Similar to the variable “maternal education,” mothers who work for a living had an association with infant death 2.03 times stronger when compared with those who don't.
Table 3. Hierarchical logistic regression of factors associated with infant mortality, Teresina, Piauí, Brazil.
| Variables | Live Births | Deaths | ORadj (CI95%) | p* |
|---|---|---|---|---|
| Mother Race | ||||
| White | 2,054 | 41 | 1 | 0.139 |
| Non-white | 9,418 | 161 | 1.20 (0.89 - 1.51) | |
| Mother Marital Status | ||||
| With Partner | 10,122 | 146 | 1 | 0.266 |
| No Partner | 3,480 | 61 | 1.97 (0.86 - 3.17) | |
| Mother Age | ||||
| 10–19 Years | 2,210 | 49 | 2.82 (1.69 - 3.20) | < 0.001 |
| 20–34 Years | 10,293 | 144 | 5.11 (3.80 - 6.46) | |
| ≥ 35 Years | 1,379 | 14 | 1 | |
| Mother Education | ||||
| Low | 2,618 | 48 | 1.85 (1.43 - 2.32) | < 0.001 |
| Intermediate | 6,566 | 91 | 1 | |
| High | 4,344 | 65 | 1.28 (1.10 - 1.47) | |
| Mother Occupation | ||||
| With Remuneration | 4,451 | 64 | 2.03 (1.48 - 2.44) | < 0.001 |
| No Remuneration | 9,125 | 143 | 1 | |
| Hospital Type | ||||
| SUS | 10,499 | 188 | 1 | 0.512 |
| Non-SUS | 3,368 | 19 | 1.87 (0.72 - 3.43) | |
| Parity | ||||
| First-time | 4,750 | 98 | 1.43 (1.14 - 1.70) | 0.009 |
| Multiparous | 6,082 | 109 | 1 | |
| Pregnancy Type | ||||
| Single | 13,437 | 192 | 1 | < 0.001 |
| Multiple | 324 | 15 | 2.87 (2.00 - 3.78) | |
| Delivery Type | ||||
| Vaginal | 5,782 | 118 | 1.84 (1.26 - 2.45) | < 0.001 |
| Cesarean | 8,058 | 89 | 1 | |
| Prenatal | ||||
| Did not perform | 669 | 9 | 1.28 (1.11 - 1.51) | 0.038 |
| Inappropriate | 4,797 | 66 | 1.12 (1.02 - 1.24) | |
| Appropriate | 7,024 | 99 | 1 | |
| Gender | ||||
| Female | 6,742 | 92 | 1 | 0.322 |
| Male | 7,135 | 114 | 1.15 (0.78 - 1.46) | |
| Gestational Age | ||||
| Preterm | 1,462 | 133 | 13.88 (7.95 - 20.08) | < 0.001 |
| Term | 10,493 | 64 | 1 | |
| Post-term | 767 | 5 | 1.08 (1.01 -1.16) | |
| Weight | ||||
| Low Weight | 1,298 | 141 | 12.3 (8.76 - 16.14) | < 0.001 |
| Normal | 12,584 | 66 | 1 | |
| Apgar 1st Minute | ||||
| 0–3 | 180 | 56 | 23.12 (17.90 - 28.41) | < 0.001 |
| 4–6 | 671 | 50 | 11.36 (7.15 - 14.97) | |
| 7–10 | 12,743 | 82 | 1 | |
| Apgar 5th Minute | ||||
| 0–3 | 58 | 19 | 21.80 (16.47 - 27.31) | < 0.001 |
| 4–6 | 71 | 26 | 23.65 (17.89 - 30.59) | |
| 7–10 | 13,468 | 143 | 1 | |
| Congenital Malformation | ||||
| Yes | 98 | 58 | 42.33 (30.11 - 54.48) | < 0.001 |
| No | 12,498 | 112 | 1 | |
Abbreviations: CI95%, 95% confidence interval; ORadj, Odds Ratio adjusted; SUS, Brazilian Unified Health Care System.
Source: Santos et al. (2014).11
Note: *p = Wald test; Hosmer and Lemeshow test (p = 0.896); Live Birth (N = 13882); Deaths (n = 207).
At the intermediate level, all variables were statistically significant, particularly the type of pregnancy and type of delivery (p-value < 0.001). The first-time mothers (ORadj = 1.43; CI95% 1.14–1.70), who had multiple pregnancies (ORadj = 2.87; CI95% 2.00–3.78) and vaginal delivery (ORadj = 1.84; CI95% 1.26–2.45) had a higher risk of infant death compared with multiparous, single pregnancy and caesarean section respectively. With regard to prenatal care, mothers who did not have (ORadj = 1.28; CI95% 1.11–1.51) or had inappropriate prenatal care were more associated with the study outcome when compared with those with appropriate prenatal care.
The baby's gender was a determinant factor at proximal level that did not have significant association with infant death. The other variables of this level had an association with a p-value < 0.001. Babies born preterm had a 13.88-time increase in the risk of death compared with those born at term. Also, a stronger association with the outcome studied was observed on those born post-term (ORadj = 1.08; CI95% 1.01–1.16) when compared with those born at term. The low birth weight represented a greater chance of infant mortality (12.3 times [CI95% 8.76–16.14] than those who were born weighing 2,500 g or more. For the Apgar score at 1st minute and 5th minute, the group scoring 7 to 10 had the lowest chance of death if compared with the others. Newborns identified with congenital malformation were more associated (ORadj = 42.33; CI95% 30.11–54.48) with death before completing the first year of life compared with those who have not been identified with congenital malformation.
Discussion
Among the distal level factors related to the socioeconomic aspects of the mothers, the characteristics that remained statistically significant were maternal age, education and occupation.
Mothers with advanced age had a weaker association with infant death compared with other age groups in the cohort studied. This finding is different from what was reported in a study performed in two cohorts (2000–2001 and 2007–2008) of babies born in the city of Londrina (capital of the State of Paraná), which found that the pregnancies of women over 34 years old were more likely to lead to infant death when compared with the pregnancies of women aged between 20 and 34 years for both periods analyzed, reflecting the increased proportion of Brazilian mothers with over 34 years old and possibly representing the biological disadvantages of pregnancies in mothers with older age.6
On the other hand, women who decide to get pregnant later can usually be also those with higher education and socioeconomic level, stable marital status, as well as have a planned pregnancy with greater attention to prenatal visits, factors that could explain the finding of this study in relation to this variable.
The pregnancies of teenage mothers were almost three times more likely to lead to infant death when compared with the pregnancies of those older than 34 years. In the cohort of live births in Londrina, for the periods of 2000–2001 and 2007–2008, teenage pregnancy was respectively 2.70 and 1.59 times more likely to lead to death in infants when compared with the pregnancies of mothers aged 20–34 years.6
The association between teenage mothers and infant mortality can be discussed from a social and a biological standpoint. One of the outcomes of poor socioeconomic status for the adolescent and her family is the teenage pregnancy, a situation that precedes and creates difficulties to have access to health care services, as well as adverse perinatal outcomes, which demonstrate the need to strengthen the family planning activities recommended by primary health care.7
The immaturity of the female reproductive system and the continued growth and development of the teenager during pregnancy are examples of biological predisposing factors for adverse perinatal outcomes, such as intrauterine growth restriction, prematurity and low birth weight.6
Mothers with low and high education were more associated with infant mortality than mothers with intermediate education in this study.
In a research conducted in five Brazilian cities from every region of the country, low education had statistical significance only for Belém, the capital of the state of Pará, northern Brazil. Similarly, in Passo Fundo, a city on the South region, lower education had significant association with deaths in infants.1 7
For the two cohorts studied in Londrina, education was associated with the outcome, but with different behavior between the two periods. In the older cohort, the group with low education had a higher chance of infant death; however, in the most recent cohort, low education was a protective factor for infant mortality.6 Importantly, in the latter study, education was categorized similarly to the present study, adjusting the years of study to the maternal age, unlike the others, in which education was provided only by the amount of years of study completed, regardless of the mother's age.
Analyses associating groups of mothers with fewer years of education with an increased risk of infant death assume that mothers with higher education are those belonging to higher social classes, who have fewer children and greater access to knowledge about child care and appropriate prenatal care, factors that would increase the protection against the outcome.1 7
A reduction in Infant Mortality Rate (IMR) is observed among mothers with low education, and an increase or stabilization of this rate is observed among mothers with higher education, which are usually older, more likely to have a cesarean delivery, and have a higher ratio of premature births and low birth weight. This scenario depicts the changes in the health care, social and reproductive characteristics of Brazilian women in recent years.6
The offspring of mothers who work for a living were significantly associated with infant mortality, which was two times higher than those of stay-at-home mothers. Few studies were found reporting this association. However, in a study conducted in Salvador (the capital of the northeastern state of Bahia), maternal occupation took part in the multivariate analysis, reaching statistical significance, with lower probability of infant death among the offspring of self-employed professionals and mid-level technicians when compared with the offspring of housewives, students and house maids. Additionally, the chance of death for the infants of house maids was higher than among the infants of housewives and students.22
In this context, the authors attributed the less likelihood found in women with paid work to their better social and economic conditions. In contrast, house maids were analyzed as a separate group due to their poor working conditions that not always follow the labor laws. Despite receiving payment, their working hours keep them from receiving the appropriate prenatal care, and the limited time available for them to stay at home affects the quality of their maternal care.
Nevertheless, the continuous improvement in the house maids' working conditions are evident and guaranteed by current labor laws in Brazil, at a time when many other jobs for Brazilian women also offer poor working conditions. Thus, this study was performed employing only two strata for this category: with and without remuneration. As a result, women with paid work were two times more likely to face infant death, which could have been attributed to the stress of modern life, where women work double shifts, at work and at home, a factor that could contribute to adverse perinatal outcomes.
Infant mortality was higher among those born in hospitals that are not part of the SUS network when compared with deliveries occurred in hospitals that are part of this network in Teresina, but they were not statistically significant. This contrasts with the study performed in Salvador, which showed significant association between the birth in public hospitals and the death of infants, suggesting the existence of deficiencies in the care of newborns at risk in the population assisted by public health care facilities.22
In 2011, it was observed that the vast majority of live births of women living in Teresina reported by SINASC occurred in facilities integrating SUS network; however, the number of births in the private network, which counts with only 8 beds for neonatal intensive care, is also high in Teresina, while in the public facilities that integrate the SUS network there are 27 beds for this purpose, which is also seen as low considering the demand.14
Although Teresina is considered a reference in health care services for the other municipalities and even neighboring states, there is insufficient amount of high complexity beds for the pediatric care both in the public and private sectors, particularly for the neonatal period, a main component of IMR in this city.
Obstetrical history was significantly associated with the outcome, and it was more likely to lead to infant death for first-time mothers. Other studies have reported the association between multiparous women and infant mortality, linking the high parity to the low socioeconomic level of the family as a determinant of mortality in infants.23 On the other hand, mothers coming from higher social classes have a current tendency to have fewer children, which may also be related to their paid work and high education, a finding consistent with the current study.
Multiple pregnancies had a higher chance of leading to infant death compared with single pregnancies, with statistical significance. The same finding was reported in the analysis conducted in Londrina in two different periods, in which both had a high probability of death in infants born of multiple pregnancies.6 Some studies excluded this variable from their analyses; however, we chose to keep this subgroup of live births, controlling its effect in the multivariate analysis.
Births of twins are related to an increased rate of adverse perinatal outcomes, such as premature birth and low birth weight. This emphasizes the importance of special care for women with this risk profile in Teresina.
The type of delivery performed presented statistical significance in this study, showing that infants born vaginally have a stronger association with infant mortality when compared with those born by caesarean section. A study conducted in nine municipalities of the western region of the state of Paraná, and another performed in the city of Londrina, in the same state, found that caesarean section is a protective factor against infant mortality.6 24
An analysis performed on newborns with high risk in a neonatal ICU in northeastern Brazil found that cesarean section increases maternal and newborn morbidity and mortality, substantially increasing the cost of health care when compared with vaginal delivery. However, operative delivery in high-risk pregnancies is considered an important procedure to reduce perinatal risks, increasing the newborn's chance of survival.25
Failure to attend the visits or inadequacy of prenatal monitoring showed up as determinant of infant mortality in Teresina. Importantly, this variable was achieved by adjusting the number of prenatal visits performed according to gestational age at delivery, following a model recommended by the Brazilian Ministry of Health.16 Reclassification was required since this study included extremely premature infants and births that occurred after42 weeks of pregnancy, which, therefore, had unequal opportunities to attend the visits.
Several studies have found a significant association between inappropriate prenatal care and infant death in the cities of Belém, Recife, Porto Alegre, Salvador and Maracanaú. In the cities of Guarulhos and Goiânia, prenatal care did not show statistical significance as a determinant for infant mortality.7 22 23 These analyses took into account only the number of prenatal visits, not associating them with the duration of the pregnancy.
Unlike the study performed in Londrina, which associated prenatal care with gestational age for the cohorts of 2000–2001 and 2007–2008, showing significant association only for the earliest period, the cohort of 2007–2008 did not show that prenatal care determines death in infants.6 The authors attributed this loss of statistical significance to improvements in the social policies and primary health care in the city, with the expansion of primary care through the Family Health Strategy Program, which contributed to an increased coverage and improved prenatal care, and favored the decentralization of primary health care services through the capture, follow-up and referral of pregnant women to other levels of care.
In Brazil, the coverage and average number of prenatal visits seem to be increasing. However, in the current studies on infant mortality using the LBIS database, the assessment of quality in prenatal care is not available. In this context, there is evidence that the poor quality of the service is a more serious problem than simply performing fewer visits.26
Male infants had a stronger association with infant mortality in this study, but it was not statistically significant. Being of the female gender has shown to be a protective factor in some studies that attribute the early lung maturation in females during the neonatal period with a consequent decrease in the incidence of neonatal respiratory problems, resulting in a greater number of hospital days in the first year of life in males.6 24 The loss of effect of this variable in the current context in Teresina may result from the expansion of perinatal care, with the hierarchical organization and regionalization of health care services and the greater access to neonatal technologies, such as intensive care and use of corticosteroids and surfactant in preterm infants.
The length of the gestation showed a strong association between preterm birth and infant mortality, as well as births occurring after 41 weeks, to a lesser extent, but yet significant.
Several authors found a higher likelihood of infant death with premature births, which was statistically significant in several cities in Brazil, of all regions in diverse periods.6 7 22 23 24 27 Preterm birth can be not only triggered by biological factors, but also by several social factors, with the change in women's lifestyle in recent decades, with an increased use of alcohol and tobacco, social stress, occupational stress and poor diet.
On the other hand, two studies performed in the state of Rio Grande do Sul, in the cities of Porto Alegre and Passo Fundo, found no significant association between prematurity and infant mortality, which may be related to the level of social and economic development, as well as greater access to human and technological resources for child health care in that region.1 7
A study performed on trends in infant mortality in Porto Alegre found that the considerable decline in the IMR in that city is a phenomenon that may reflect the process of poverty reduction. In 2009 Porto Alegre had the lowest poverty rate among the six main metropolitan regions in Brazil. This demonstrates that Porto Alegre is ahead in the demographic and epidemiological transition phenomenon, reducing the neonatal mortality rate, post-natal mortality rate and the number of live births.28
Post-term infants also showed significant association with the outcome under study. The Brazilian Ministry of Health has established that between the 36th and 41st weeks of pregnancy prenatal visits should occur weekly. This increased frequency of visits in late pregnancy aims to assess the perinatal risk and clinical and obstetric complications, which are more common in this trimester. Placental function reaches its fullness around the 36th week, declining thereafter. Senile placenta has calcifications and other changes that are responsible for decreased nutrition and oxygen supply to the fetus and, therefore, is associated with increased perinatal morbidity and mortality.16 This shows the importance that should be given to these births. Few studies on risk factors associated with infant mortality refer to those prolonged pregnancies.
Low birth weight had a strong and statistically significant association with infant death, consistent with the vast majority of studies addressing this topic.1 6 7 22 23 24 27
The risk factors described in the literature that have a greater association with infant mortality are low birth weight and prematurity, and they should not be studied as isolated risk factors, but rather associated with the biological and socioeconomic characteristics of the mother, which are also considered determinants for death in infants.24
The Apgar score at the 1st and 5th minutes is a simple and helpful indicator used to measure the vitality of the live birth and to assess responses to resuscitation maneuvers, and it is an important risk indicator for perinatal morbidity and mortality.6 7
The findings of the study show that the lowest scores in this index, both at the 1st and 5th minutes, are risk factors in the final model for determination of infant mortality, as shown by other recent studies.1 6 7 23 27
These results suggest the need for appropriate and sustained support measures to ensure greater survival of newborns with an Apgar score below 7 in the 1st and 5th minutes of life.23
The presence of congenital malformations was shown to be a determinant strongly associated with infant mortality, as reported by studies conducted in the cities of Belém, Recife, Porto Alegre, Goiânia and Foz do Iguaçu.7 27
In places where there is a decreased infant mortality from preventable causes and an improvement in the quality of prenatal care, congenital anomalies become the leading cause of infant mortality. A few teratogens affecting the Brazilian population have been described, such as rubella and acute toxoplasmosis among the infectious diseases in pregnancy, drugs such as thalidomide, radiation therapy and chemotherapy, when their use cannot be prevented during pregnancy, and genetic factors. It is also known that pregnant women aged over 40 years are more likely to have malformed children when compared with younger age groups.29
Providing proper prenatal care to identify potential teratogenic risks is another potential goal to be met, by making available an examination system capable to identify potential teratogenic risk agents, and more complex and specific tests, when early identification of birth defects is required. Another factor that could reduce mortality due to congenital malformations is structuring the service network to detect/provide clinical genetic counseling for the SUS, in addition to primary care in the identification of families at risk, performing preventive diagnosis and preventing the birth of malformed children.30
In conclusion, it was evidenced that, in addition to biological factors in determining infant mortality, socioeconomic status and proper healthcare for the pregnant women and newborns are also important, since they are factors that can be changed with public policies, through an increased investment and qualification of health care professionals for prenatal care, childbirth and the neonatal period at local level.
Acknowledgments
SLD Santos worked in the study concept and design, data analysis and interpretation, writing and critical review of the article. LB Santos and V Campelo worked on writing and critical review of the article. ARV da Silva worked in the study conception and design, writing and critical review of the article.
References
- 1.Geib L TC Fréu C M Brandão M Nunes M L [Social and biological determinants of infant mortality in population cohort in the city of Passo Fundo, Rio Grande do Sul State] Cien Saude Colet 2010152363–370. Portuguese [DOI] [PubMed] [Google Scholar]
- 2.Shetty A K. Global maternal, newborn, and child health: successes, challenges, and opportunities. Pediatr Clin North Am. 2016;63(1):1–18. doi: 10.1016/j.pcl.2015.08.001. [DOI] [PubMed] [Google Scholar]
- 3.Batista Filho M Cruz R SBLC [Child health around the world and in Brazil] Rev Bras Saude Mater Infant 2015154451–454. Portuguese [Google Scholar]
- 4.Lisboa L Abreu D MX Lana A MQ França E B [Infant mortality: leading avoidable causes in the central region of Minas Gerais, Brazil, 1999–2011] Epidemiol Serv Saúde. 2015244711–720. Portuguese [Google Scholar]
- 5.Lima Sd Carvalho M L Vasconcelos A GG [Proposal for a hierarchical framework applied to investigation of risk factors for neonatal mortality] Cad Saude Publica 20082481910–1916. Portuguese [DOI] [PubMed] [Google Scholar]
- 6.Santos H G, Andrade S M, Silva A MR, Carvalho W O, Mesas A E. Risk factors for infant mortality in a municipality in southern Brazil: a comparison of two cohorts using hierarchical analysis. Cad Saude Publica. 2012;28(10):1915–1926. doi: 10.1590/s0102-311x2012001000010. [DOI] [PubMed] [Google Scholar]
- 7.Maia L TS Souza W V Mendes AdaC [Differences in risk factors for infant mortality in five Brazilian cities: a case-control study based on the Mortality Information System and Information System on Live Births] Cad Saude Publica 201228112163–2176. Portuguese [DOI] [PubMed] [Google Scholar]
- 8.Soares E S Menezes G MS [Factors associated with neonatal mortality: situation analysis at the local level] Epidemiol Serv Saúde. 201019151–60. Portuguese [Google Scholar]
- 9.Mendes A CG Lima M M Sá D A Oliveira L CS Maia L TS [The use of the interrelation of data bases to improve information on child mortality in municipalities in the Brazilian State of Pernambuco] Rev Bras Saude Mater Infant 2012123243–249. Portuguese [Google Scholar]
- 10.Oliveira M M, Andrade S SCA, Dimech G S. et al. Evaluation of the National Information System on Live Births in Brazil, 2006–2010. Epidemiol Serv Saúde. 2015;24(4):629–640. [Google Scholar]
- 11.Santos S LD Vilarouca da Silva A R Campelo V Rodrigues F T Ribeiro J F [Use of the linkage method to identify the risk factors associated with infant mortality: an integrative review of the literature] Cien Saude Colet 20141972095–2104. Portuguese [DOI] [PubMed] [Google Scholar]
- 12.Instituto Brasileiro de Geografia e Estatística [Internet] Censo 2010 2010 [citado 2013 Jun 15]. Disponível em: http://www.censo2010.ibge.gov.br
- 13.Teresina . Teresina: Prefeitura Municipal; 2016. Prefeitura Municipal. Plano municipal de saneamento básico 2016. [Google Scholar]
- 14.Brasil Ministério da Saúde. Datasus. Informações de Saúde [Internet]. Cadastro Nacional de Estabelecimentos de Saúde Brasília (DF)Ministério da Saúde; 2014. [citado 2014 Jun 5]. Disponível em: http://cnes.datasus.gov.br/ [Google Scholar]
- 15.Sampaio C EM Nespoli V Índice de Adequação Idade-Anos de Escolaridade Estatística Rev Bras Estud Pedagogicos 200485(209/210/211):137–142. [Google Scholar]
- 16.Brasil . Brasília (DF): Editora do Ministério da Saúde; 2013. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Atenção ao pré-natal de baixo risco. [Google Scholar]
- 17.São Paulo . São Paulo: Secretaria Municipal da Saúde; 2012. Prefeitura Municipal. Secretaria Municipal da Saúde. Coordenação de Epidemiologia e Informação. Declaração de Nascido Vivo - Manual de anomalias congênitas. 2a ed. [Google Scholar]
- 18.Abreu M NS, Siqueira A L, Caiaffa W T. [Ordinal logistic regression in epidemiological studies] Rev Saude Publica. 2009;43(1):183–194. doi: 10.1590/s0034-89102009000100025. [DOI] [PubMed] [Google Scholar]
- 19.Hosmer D W, Lemeshow S. New York: John Wiley & Sons; 2000. Applied logistic regression. 2nd ed. [Google Scholar]
- 20.Lee H Y. Goodness-of-fit tests for a proportional odds model. J Korean Data Inf Sci Soc. 2013;24(6):1465–1475. [Google Scholar]
- 21.Brasil Ministério da Saúde. Conselho Nacional de Saúde. Resolução n. 466, de 12 de dezembro de 2012 Diário Oficial da República Federativa do Brasil, Poder Executivo, Brasília (DF) 2013 jun 13;Sec.1:59
- 22.Nascimento E MR Costa MdaC Mota E LA Paim J S [Investigation of risk factors for infant mortality by linking health databases] Cad Saude Publica 200824112593–2602. Portuguese [DOI] [PubMed] [Google Scholar]
- 23.Silva C F Leite A JM Almeida N MGS Gondim R C [Risk factors for infant mortality in a city of northeastern Brazil: linkage between live birth and infant death databases – 2000 to 2002] Rev Bras Epidemiol 20069169–80. Portuguese [Google Scholar]
- 24.Mombelli M A Sass A Molena C AF Téston E F Marcon S S [Risk factors for child mortality in towns of Paraná State (South Brazil), from 1997 to 2008] Rev Paul Pediatr. 2012302187–194. Portuguese [Google Scholar]
- 25.Silva C F Leite A JM Almeida N MGS Leon A CMP Olofin I; Rede Norte-Nordeste de Saúde Perinatal. [Factors associated with neonatal death in high-risk infants: a multicenter study in High-Risk Neonatal Units in Northeast Brazil] Cad Saude Publica 2014302355–368. Portuguese [DOI] [PubMed] [Google Scholar]
- 26.Kassar S B, Melo A MC, Coutinho S B, Lima M C, Lira P IC. Determinants of neonatal death with emphasis on health care during pregnancy, childbirth and reproductive history. J Pediatr (Rio J) 2013;89(3):269–277. doi: 10.1016/j.jped.2012.11.005. [DOI] [PubMed] [Google Scholar]
- 27.Doldan R V, Costa J SD, Nunes M F. Associated factors and infant mortality in the municipality of Foz do Iguaçu, state of Paraná, Brazil – a case control study. Epidemiol Serv Saúde. 2011;20(4):491–498. [Google Scholar]
- 28.Hernandez A R Silva C H Agranonik M Quadros F M Goldani M Z [Analysis of infant mortality trends and risk factors in Porto Alegre, Rio Grande do Sul State, Brazil, 1996-2008] Cad Saude Publica 201127112188–2196. Portuguese [DOI] [PubMed] [Google Scholar]
- 29.Jobim R Aerts D [Avoidable infant mortality and associated factors in Porto Alegre, Southern Brazil, 2000-2003] Cad Saude Publica 2008241179–187. Portuguese [DOI] [PubMed] [Google Scholar]
- 30.Gomes M RR, Costa J SD. Infant mortality and congenital abnormalities in the Municipality of Pelotas, State of Rio Grande do Sul, Brazil: ecologic study in the period 1996–2008. Epidemiol Serv Saúde. 2012;21(1):119–128. [Google Scholar]