

Abstract
We provide incidences (cases/10 million persons) in the Netherlands during 2009–2019 for pathogens listed as potential bioterrorism agents. We included pathogens from the highest categories of the European Medicines Agency or the US Centers for Disease Control and Prevention. Notifiable diseases and recently published data were used to calculate the average annual incidence. Coxiella burnetii had the highest incidence because of a Q fever epidemic during 2007–2010. Incidence then decreased to 10.8 cases/. Pathogens with an incidence >1 were Brucella spp. (2.5 cases), Francisella tularensis (1.3 cases), and Burkholderia pseudomallei (1.1 cases). Pathogens with an incidence <1 were hemorrhagic fever viruses (0.3 cases), Clostridium botulinum (0.2 cases), and Bacillus anthracis (0.1 cases). Variola major and Yersinia pestis were absent. The generally low incidences make it unlikely that ill-meaning persons can isolate these pathogens from natural sources in the Netherlands. However, the pathogens are stored in laboratories, underscoring the need for biosecurity measures.
Keywords: epidemiology, pathogens, bacteria, viruses, diseases, biosecurity, potential bioterrorism agents, bioterrorism and preparedness, the Netherlands
An act of bioterrorism could affect public health and will cause substantial societal disruption. Although the risk for bioterrorism is considered to be low, an incident involving a limited number of persons, or even a hoax, may result in panic in the general public, and a larger attack might have major consequences up to total disruption of society (1). Despite the low probability, the risk for bioterrorism remains and should not be neglected. The continued interest of terrorists in bioweapons and toxins is illustrated by the 2018 foiled plot of a ricin attack by an extremist from Tunisia in Cologne, Germany (2) and a ricin letter sent in 2020 to the President of the United States (3). The continued risk for bioweapons was addressed during the Munich Security Conference in 2018 by the Dutch Minister of Defense (4). Furthermore, the US government designates biologic weapons as a persistent threat in their 2022 National Biodefense Strategy (5).
The pathogens listed as potential bioterrorism agents originate from nature and, although rare, can be encountered either as causing autochthonous or travel-related disease. The aim of this study was to provide an overview of the incidences of these pathogens, exemplified by the Netherlands, to maintain awareness for biosafety at laboratories, and to underscore the relevance of material accountability and the need for biosecurity measures to prevent unauthorized access to the actual pathogens and related knowledge, to reduce the risk for bioterrorism.
There are many pathogens that could potentially be used as bioweapons based on characteristics such as route of transmission, pathogenicity, infectious dose, stability in the environment, and other factors (6). It is essential to reduce the risk for misuse and deliberate release by controlling and restricting the development, production, stockpiling, or other ways of acquiring biologic and toxin weapons or their means of delivery. Several lists have been compiled to guide measures to mitigate the risks regarding these pathogens (Table 1).
Table 1. Overview of lists related to biosafety and the deliberate release of pathogens*.
| Organization | List | Purpose | Reference |
|---|---|---|---|
| Australia Group |
Handbook volume II |
Nonproliferation |
(7) |
| Biosecurity office, RIVM |
Combined list of biologic agents |
Comparison of lists relevant for the Netherlands |
(8) |
| CDC | Biosafety in Microbiological and Biomedical Laboratories | Biosafety | (9) |
| Bioterrorism Agents/Diseases | Bioterrorism preparedness | (10,11) | |
| Classification of Diseases, Functioning, and Disability | Natural environment protection (GMO regulations) | (12) | |
|
|
Federal Select Agent Program |
State biosecurity legislation |
(13) |
| EMA | Biologic and Chemical Threats | Bioterrorism preparedness | (14) |
|
|
Guidance document on use of medicinal products for the treatment and prophylaxis of biologic agents that might be used as weapons of bioterrorism |
Civilian or military medical guidelines for biowarfare/bioterrorism |
(15) |
| European Union | Biologic agents directive 2000/54/EC | Biosafety | (16) |
|
|
Regulation 2017/2268 dual-use items |
Nonproliferation |
(17) |
| German Federal Ministry of the Interior |
War Weapons Control Act |
Nonproliferation |
(18,19) |
| NATO |
Handbook on the Medical Aspects of NBC Defensive Operations |
Civilian or military medical guidelines for biowarfare/bioterrorism |
(20) |
| USAMRIID | Medical Management of Biologic Casualties Handbook | Civilian or military medical guidelines for biowarfare/bioterrorism | (21) |
*EMA classification of biologic threats adapted from EMA. The encephalitis viruses are Eastern equine encephalitis, Western equine encephalitis, and Venezuelan equine encephalitis. Other hemorrhagic fever viruses, for which no treatment existed: Marburg virus, Ebola virus, yellow fever virus, hantavirus, and tick-borne encephalitis virus. However, for Ebola virus disease, treatment options now exist. CDC, US Centers for Disease Control and Prevention; EMA, European Medical Agency; NATO, North Atlantic Treaty Organization; NBC, nuclear, biological, chemical; RIVM, National Institute for Public Health and the Environment, the Netherlands; USAMRIID, US Army Medical Research Institute of Infectious Diseases.
Only 2 of the lists are directly devoted to bioterrorism: the US Centers for Disease Control and Prevention (CDC) Bioterrorism Agents/Diseases and the European Medicines Agency (EMA). A prioritization and selection of the potential bioterrorism agents was made by CDC 2 decades ago, which resulted in the Bioterrorism Agents/Diseases classification (10). This classification is based on public health experience, as well as Cold War era military experiments, in which potential bioterrorism agents were evaluated for public health impact, dissemination possibilities, public perception, and the need for special preparation (11). The EMA restructured the CDC list, creating the Biologic and Chemical Threats list, of which the biologic agents are provided (Table 2) (12). The 3 categories are created from a medical point of view and accompanied by treatment guidelines (15).
Table 2. European Medicines Agency classification of biologic threats.
| Category I agents: major infectious diseases for which treatment exists | Category II agents: other bacterial infections for which treatment exists | Category III agents: biologic agents for which currently no specific treatment can be recommended |
|---|---|---|
| Bacillus anthracis, Yersinia pestis, Francisella tularensis, Variola major, hemorrhagic fever viruses, botulinum toxin (Clostridium botulinum), Brucella spp., Coxiella burnetii, Burkholderia mallei, Burkholderia pseudomallei | Chlamydia psittaci, Rickettsia prowazekii, Mycobacterium tuberculosis, Shigella spp., Salmonella spp., Vibrio cholerae | Enterohemorrhagic Escherichia coli, Cryptosporidium, encephalitis viruses,* Nipah virus, other hemorrhagic fever viruses,† Clostridium perfringens epsilon toxin, Staphylococcal enterotoxin B, ricin |
*Encephalitis viruses include Eastern equine encephalitis, Western equine encephalitis, and Venezuelan equine encephalitis. †Other hemorrhagic fever viruses, for which no treatment existed: Marburg virus, Ebola virus, yellow fever virus, hantavirus, and tick-borne encephalitis virus. However, for Ebola virus disease, treatment options now exist.
Materials and Methods
Selection of Potential Bioterrorism Agents
This study includes the pathogens that are categorized in the highest risk category by either EMA (Table 2) or CDC. The CDC category A contains the classic potential bioterrorism agents: Bacillus anthracis, Yersinia pestis, Francisella tularensis, Clostridium botulinum toxin, and hemorrhagic fever viruses (10). EMA category I includes the same pathogens, expanded by Brucella spp., Burkholderia mallei and Burkholderia pseudomallei, and Coxiella burnetii (14).
Nationally Notifiable Diseases and EMA Major Biologic Threats
Many potential bioterrorism agents are notifiable diseases in the Netherlands because of their infectiousness and virulence. Notifications of these diseases are collected at the National Institute for Public Health and the Environment (RIVM), and data are made publicly available (22). Not all potential bioterrorism agents from the highest categories are notifiable diseases in the Netherlands. Biologic threats that are not notifiable are B. mallei and B. pseudomallei, the causative agents of glanders and melioidosis, respectively. An overview of melioidosis cases in the Netherlands was recently published by Birnie et al. (23). Furthermore, Rijks et al. recently published the incidence of F. tularensis in the Netherlands (24). These data were added to the overview of the major biologic threats.
Observation Period
The observation period was set from 2009 through 2019. January 2009 was selected as the starting point because in 2008 the Netherlands implemented the Public Health Act, on which the current selection of nationally notifiable diseases and notification criteria are based (25). December 2019 was selected as the endpoint because measures taken to combat the SARS-CoV-2 pandemic in 2020 and 2021, including limiting international travel, mitigated the incidence of many other infectious diseases. Because the aim of this study was to provide an overview of the standard incidence, we excluded those years.
Calculating Average Annual Incidences Per 10 Million Persons
To enable international comparison, we calculated the average annual incidences per 10 million persons. During the observation period, the population of the Netherlands increased from 16.5 million in 2009 to 17.3 million in 2019 (26). We calculated average incidence per year and, subsequently, the average annual incidence.
Results
We compiled absolute numbers of cases and annual incidence for each organism (Table 3; Figure). Detailed descriptions of cases and incidence for individual pathogens follow.
Table 3. Epidemiology of pathogens listed as highest category potential bioterrorism agents, the Netherlands, 2009–2019*.
| Pathogen | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | Average annual incidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bacillus anthracis | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0.1 |
| Brucella spp. | 4 | 6 | 1 | 2 | 5 | 2 | 9 | 4 | 2 | 5 | 7 | 2.5 |
| Burkholderia mallei | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0.0 |
| Burkholderia pseudomallei | 0 | 2 | 0 | 5 | 2 | 1 | 1 | 1 | 5 | 2 | NA | 1.1 |
| Clostridium botulinum | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0.2 |
| Coxiella burnetii | 2,424 | 411 | 77 | 63 | 20 | 26 | 20 | 14 | 22 | 18 | 18 | 171.2 (10.8)† |
| Francisella tularensis | 1 | 0 | 1 | 0 | 1 | 3 | 1 | 9 | 2 | 2 | 4 | 1.3 |
| Variola major | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0.0 |
| Yersinia pestis | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0.0 |
| Hemorrhagic fever viruses | 0 | 0 | 0 | 0 | 0 | 1‡ | 0 | 0 | 1§ | 2§ | 2¶ | 0.3 |
*Incidence is given as cases/10 million persons. NA, not available. †Incidence is shown in parentheses for postoutbreak years of 2015–2019, which is more representative. ‡Ebola fever virus. §Yellow fever virus. ¶Lassa fever virus.
Figure.
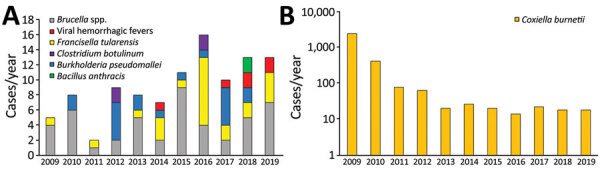
Infections with pathogens listed as potential bioterrorism agents in the Netherlands, 2009−2019. A) Absolute numbers for most pathogens. No cases of infection with Burkholderia mallei, variola major virus (smallpox), or Yersinia pestis were reported. B) Coxiella burnetii is shown on a logarithmic scale to accommodate the high incidence during the Q fever epidemic of 2007‒2010. Complete data are shown in Table 2.
B. anthracis
The incidence of B. anthracis ranged from 0 to 2 cases/year during 2009–2019 in the Netherlands. This finding results in an average annual incidence for B. anthracis of 0.1 cases/10 million persons. Two cases of the cutaneous form of anthrax occurred in 2018. One patient was a returning traveler from Tanzania who had no possible source of infection. The second patient had a travel history to Turkey and possibly got infected during the slaughtering of sheep or preparation of meat. No anthrax spores have thus far been detected in hoax letters in the Netherlands (27).
Brucella spp.
Brucellosis occurred only as an imported disease in the Netherlands (1‒9 cases/year). The average annual incidence during 2009–2019 of Brucella spp. was 2.5 cases/10 million persons.
B. mallei
Glanders is not a notifiable disease in the Netherlands; therefore, no data are available on B. mallei cases. However, no B. mallei has been detected in patient samples or cultured isolates received by RIVM for confirmation of rare or highly virulent pathogens, and no cases were otherwise reported during 2009–2019 (RIVM, unpub. data). Furthermore, no scientific publications were identified describing cases of glanders in the Netherlands.
B. pseudomallei
Melioidosis is also not a notifiable disease in the Netherlands. However, Birnie et al. identified 33 returning travelers who had this disease over the past 25 years (23). During 2009–2019, the average annual incidence was 1.1 cases/10 million persons (range 0‒5 total cases/year) in the Netherlands.
C. botulinum Toxin
The incidence of botulism ranged from 0 to 2 cases/year, resulting in an average annual incidence of 0.2 cases/10 million persons. In 2012, two unrelated cases of infant botulism were reported, 1 possibly related to honey consumption and 1 that did not have a suspected source (28). In 2016, two additional case-patients were given diagnoses of autochthonously acquired botulism in the Netherlands. The first case-patient was a young man from eastern Europe who had no confirmed exposure. The second case-patient had suspected foodborne botulism, possibly related to the use of glass jars for home preservation of food, which is associated with botulism (29).
C. burnetii
During 2007‒2010, an epidemic of Q fever occurred in the Netherlands that was related to goat farming and had a peak of 2,424 cases in 2009. This epidemic was the largest recorded outbreak globally (30). Since then, preventative measures have been taken, and the annual incidence has decreased to preoutbreak levels. For the total 2009–2019 period, the average annual incidence of C. burnetii was 171.2 cases/10 million persons. However, during the last 5 years of the study period (2015–2019), the average incidence was 10.8 cases/10 million persons (14 to 26 cases/year).
F. tularensis
For decades, F. tularensis cases did not occur in the Netherlands. However, sporadic imported cases were seen, such as a single imported case from Finland in 2009 (31). However, in 2011, an autochthonous case of F. tularensis was detected for the first time since 1953. The disease became a notifiable disease in 2016, and an overview of all 26 autochthonous cases from 2011–2021 has been published (24). A total of 21 autochthonous cases were reported during 2011–2019. There were 2 imported cases in 2019 (RIVM, unpub. data), resulting in 24 cases during 2009–2019 (range 0‒9 total cases/year). The annual average incidence of F. tularensis was 1.3 cases/10 million persons. Those cases were all F. tularensis subspecies holarctica (type B), which is the type from Europe and rarely associated with severe disease. The more severe pathogenic F. tularensis subspecies tularensis (type A) from North America has not been found in the Netherlands (24).
Hemorrhagic Fever Viruses
In 2014, a military peacekeeper from Nigeria who was given a diagnosis of Ebola was transferred to the Netherlands as part of an international agreement during the West Africa Ebola epidemic. The patient was given treatment at the Major Incident Hospital of the University Medical Centre of Utrecht and fully recovered from Ebola (32,33).
In 2017, yellow fever was diagnosed in a woman returning from Suriname at the University Medical Centre Groningen; she survived (34). In 2018, two cases of yellow fever were imported to the Netherlands. One case was in a woman returning from Brazil, who recovered (35). The second case was in a man returning from the Gambia‒Senegal region. He was admitted to the Amsterdam Medical Centre and referred to the Erasmus Medical Centre because of liver failure and for transplantation (36).
In 2019, Lassa fever was diagnosed in 2 repatriated physicians from Sierra Leone; 1 died (37). This finding resulted in an average annual incidence for hemorrhagic fever viruses of 0.3 cases/10 million persons.
Variola Major Virus and Y. pestis
No cases of infection with variola major virus (smallpox) or Y. pestis occurred during 2009–2019 in the Netherlands.
Discussion
Pathogens from EMA category II and category III are excluded from this study because those pathogens are considered to pose lower risks from an intentional release perspective. The EMA modified the CDC list from both a bioterrorism risk, as well as from a medical point of view, accompanied by a treatment guideline. EMA category I does not include Marburg and Ebola viruses because no treatment was available for infection with these viruses when the classification was made. Currently, at least for Zaire Ebola virus at least, treatment options are available (38). Because these filoviruses are included in CDC Category A, they are included in this study.
This example indicates that the EMA classification might require updating. Furthermore, it could be argued that the European Centre for Disease Prevention and Control is a more logical institution to maintain the list of potential bioterrorism agents for the European Union.
The most common pathogen found in the Netherlands was C. burnetii, a zoonotic, gram-negative bacterium whose reservoirs are mainly goats, sheep, and other herbivores. Q fever is associated with intensive goat farming and is endemic to the Netherlands, which is the second-largest exporter of agricultural products in the world (30). During parturition, many spore-like bacteria are released, which remain viable in the environment for months. This pathogen is highly infectious; inhalation of as few as 10 aerosolized organisms can cause disease. Disease ranges from asymptomatic or mild to severe forms, such as pneumonia or endocarditis. Some patients show development of Q fever fatigue syndrome (5). The incidence was much higher than average during the 2007–2010 epidemic. Afterward, the incidence decreased to ≈10 cases/10 million persons/year. Doxycycline is the first-choice treatment because of obligate intracellular growth of C. burnetii (15,39).
Since 2011, F. tularensis subspecies holarctica has been endemic to the Netherlands. This pathogen has a terrestrial lifecycle associated with animals around water and mud. This pathogen is considered a potential bioweapon because it can be aerosolized and is highly infectious; a single bacterium can cause disease (40). It can enter through the skin, conjunctiva, oral, or lungs. The disease ranges from ulcers to potentially fatal pneumonia (24). Determination of the subspecies is essential; identifying F. tularensis subspecies tularensis in a patient in the Netherlands who had no history of travel to North America would be a trigger to further investigate the likelihood of a deliberate release. Because of the facultative intracellular nature of this pathogen, suitable antimicrobial drugs for treatment are gentamicin, doxycycline, and ciprofloxacin (41).
Brucella spp., in contrast to F. tularensis, are not endemic to the Netherlands and are encountered only as imported cases. B. melitensis and B. abortus can be found in different animal species (sheep, goats, cattle); B. suis is found in pigs and B. canis in dogs. Recently, a case of B. canis was reported in a dog breeder in the Netherlands (42). Brucella spp. are considered potential bioweapons and constitute a well-established cause of laboratory infections (43). The bacteria can be aerosolized and have a low infectious dose, ranging from 10 to 100 microorganisms (44). Disease ranges from mild disease to osteomyelitis and endocarditis. Brucellosis is treated with doxycycline plus gentamicin or rifampin or streptomycin (29,45).
Another travel-related pathogen is B. pseudomallei, found in soil of (sub-)tropical regions and considered a potential bioweapon because of the high mortality rate and possibility of aerosol formation (46). Empirical antimicrobial drug treatment regimens for pneumonia based on cefuroxime or ceftriaxone are not effective against this pathogen (47). Suitable antimicrobial drugs are ceftazidime or meropenem (48).
Hemorrhagic fever virus cases are sporadically imported to the Netherlands but can cause considerable safety concerns for health care providers. In Europe in general, imported cases of viral hemorrhagic fevers are relatively rare. For example, within the EuroTravNet sentinel surveillance network reporting on >100,000 cases of imported infectious diseases within its realm in the 20-year period from 1998 to 2018, just 44 cases of viral hemorrhagic fevers were recorded (49). For hemorrhagic fever viruses, antiviral treatment options are limited, other than supportive therapeutic measures. For Ebola, treatment options are available (38).
C. botulinum is a spore-forming, anaerobic, gram-positive, rod-shaped bacterium that can be ubiquitously found in the soil and agricultural products. Botulinum toxin in one of the most potent neurotoxins; it results in paralysis (50). Detection of botulinum toxin, alongside C. botulinum DNA, can be indicative of foodborne botulism, either unintentionally or as an unsophisticated attempt at bioterrorism. If toxins are found without C. botulinum or its DNA, especially if deployed by aerosolization, this finding would indicate deliberate release and technical sophistication (51). Treatment consist of botulism antitoxin only for wound botulism. Additional antimicrobial drug treatment is indicated, and suitable options are (benzyl-)penicillin or metronidazole (52,53).
The reservoir of B. anthracis is soil, and infection can occur through infected animals, ingestion of uncooked meat, or aerosols. B. anthracis has become increasingly rare because introduction of laws mandating the destruction of animal carcasses in 1942; only 9 cases have been reported in the Netherlands since 1976 (27). The low incidence in 2009–2019 is consistent with the incidence predating this period. However, anthrax spores in soil remain a potential risk. In 2013, B. anthracis DNA was detected in a so-called white pit near the city of Nijmegen; those old cattle graves, covered in quicklime, remain a potential source of anthrax (54). In addition, most natural cases are cutaneous or gastrointestinal anthrax, and only a small portion are pulmonary forms of anthrax. Bioterrorism would probably involve release of aerosolized spores; therefore, pulmonary anthrax is more indicative of intentional release. First-choice antimicrobial drugs are ciprofloxacin or doxycycline. Because of the high mortality rate for inhalation anthrax, treatment with multiple antimicrobial drugs is advised. Spores can have a long incubation time. Therefore, prolonged treatment is required. Furthermore, antitoxins and vaccines are available (15,55).
B. mallei is a potential bioterrorism agent that is not endemic to the Netherlands. Glanders is a disease primarily found in horses and was eradicated from the European Union by strict control measures. Infection can occur by contact with infected animals through mucous membrane or skin; clinical manifestations range from localized disease to sepsis (56). Similar to the case for B. pseudomallei, empirical antimicrobial drug treatment may not be effective for this pathogen; suitable antimicrobial drugs are ceftazidime or meropenem (48).
As expected, no cases of variola major infection were reported in 2009–2019 from the Netherlands. Variola major virus is highly infectious, and the infectious dose is 1 virus particle (57). It is also highly virulent, starting with an exanthema, which can progress to hemorrhagic lesions, and has a mortality rate <30%. The World Health Organization declared global eradication in 1980 because of a large-scale vaccination operation (58). The last smallpox epidemic in the Netherlands occurred in 1951 in the city of Tilburg, during which 51 infections occurred, resulting in 2 deaths (59). However, variola major stocks remain in 2 reference laboratories, designated by the World Health Organization: 1 in the United States at the CDC and 1 in Russia at the State Research Center of Virology and Biotechnology VECTOR. Although those laboratories have strict security measures, a release from the laboratory, either accidental or deliberate, is not unthinkable. Novel antiviral drugs are being developed (60,61). Furthermore, there are concerns about the possibility of resurrecting the virus by using synthetic biology (62). Finally, fragments of smallpox virus are believed to be present in the thawing Arctic permafrost. This possibility could pose additional, unknown risks (63).
Recently, a major outbreak of mpox (formerly known as monkeypox) was reported in most Western countries (64,65). Exceptions excluded, those cases typically were not characterized by a travel history to disease-endemic regions and resulted from local transmission, mainly in the men who have sex with men community (66). Mpox is not listed a potential bioterrorism agent by EMA or CDC. It is yet unclear whether this virus, originally a zoonosis from the family Poxviridae and related to variola virus, might be used as a biologic threat. A vaccine is available and proven to be effective to prevent mpox cases (67).
No cases of Y. pestis were found in the observation period. This finding was expected because the last human case of plague in the Netherlands was recorded in 1929 (68). However, Y. pestis continues to be endemic to animal reservoirs around the world and still causes epidemics, such as during 2017 in Madagascar (69). This infection can occur in a bubonic or pneumonic form. Infection can because of the bite of an infected flea by aerosols for pneumonic plague. The mortality rate for plague is 5%–15% if adequately treated and 50%‒90% if untreated (70). A recent update found ciprofloxacin to be a first-choice treatment (71).
Most pathogens in the top risk categories only occur sporadically in the Netherlands, restricting access by ill-meaning persons. However, some of the pathogens are present in clinical microbiology laboratories. Therefore, those pathogens must have proper systems in place that cover the key areas of biosecurity to minimize the risk for misuse, such as a policy on personnel and information security, material accountability, and physical security, as well as biosecurity awareness. Several assessment tools exist to assess the level of biosecurity implementation within an organization, such as the RIVM self-scan toolkit (72) and the more extended vulnerability scan (73), which provide questions, scenarios, and best practices built around the key areas of biosecurity.
Restrictive access to those pathogens is much less the case for biologic toxins such as ricin and abrin, which can be extracted from the seeds of the castor bean and the rosary pea plant, respectively; both are obtainable more easily than the bacteria or viruses described. The continued interest in biologic toxins is illustrated by a ricin attack prevented in 2018 in Cologne, Germany (2). Preventing this type of event requires the attention of law enforcement, customs agencies, and healthcare professionals.
Preparedness for an act of bioterrorism requires cross-sectoral collaboration, involving public health, law enforcement, and intelligence. The ability to detect and confirm individual cases of disease, in and of itself, is not proof of preparedness for a biologic attack or unusual unintentional outbreak. A high index of suspicion, clinical astuteness, and rapid epidemiologic and laboratory investigations by a robust, standing public infrastructure are required. The determination whether a pathogen was intentionally released ultimately rests with law enforcement agencies.
Despite the assumed low probability of an attack with biologic agents, it is essential to maintain (inter-)national preparedness. As noted, in 2018 in Cologne, Germany, an attempt to use ricin in an attack was prevented (2). This incident demonstrated the persistent interest for the use of biologic agents by perpetrators. Therefore, hospitals and medical microbiology laboratories should have up-to-date protocols on how to respond to biothreat agents. Methods that describe how to screen for biologic agents in suspected objects, such as powder letters, are included in the Dutch Chemical, Biologic, Radiological and Nuclear protocols (74).
The SARS-CoV-2 pandemic shows the potential of societal disruption caused by infectious diseases. For a resilient society, it is essential to maintain and improve the preparedness to not only natural events but also with the intentional release of biologic agents. This preparedness should be integrated in the well-established Chemical, Biologic, Radiological and Nuclear framework and through national and international cooperation.
Biography
Dr. Broertjies is a physician and resident in clinical microbiology at the Amsterdam University Medical Centers, Amsterdam the Netherlands. His primary research interests are biosafety, biosecurity, bioterrorism preparedness, and clinical microbiology.
Footnotes
Suggested citation for this article: Broertjes J, Franz E, Friesema IHM, Jansen H-J, Reubsaet FAG, Rutjes SA, et al. Epidemiology of pathogens listed as potential bioterrorism agents, the Netherlands, 2009‒2019. Emerg Infect Dis. 2023 Jul [date cited]. https://doi.org/10.3201/eid2907.221769
References
- 1.Jansen HJ, Breeveld FJ, Stijnis C, Grobusch MP. Biological warfare, bioterrorism, and biocrime. Clin Microbiol Infect. 2014;20:488–96. 10.1111/1469-0691.12699 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.The June 2018. Cologne ricin plot: a new threshold in Jihadi biol terror. Combating Terrorism Center at West Point [cited 2021 Feb 3]. https://ctc.westpoint.edu/june-2018-cologne-ricin-plot-new-threshold-jihadi-bio-terror
- 3.Woman suspected of sending letter containing ricin to Trump arrested. CNN. September 21, 2020. [cited 2021 Dec 27]. https://edition.cnn.com/2020/09/20/politics/poison-ricin-addressed-trump-arrest/index.html
- 4.Bijleveld A. Toespraak Minister Ank Bijleveld Munich Security Conference (Engels). Toespraak Defensie.nl, 2018. [cited 2021 Feb 3]. https://www.defensie.nl/downloads/toespraken/2018/02/17/toespraak-minister-munich-security-conference
- 5.Fact Sheet. Biden-Harris administration releases Strategy to strengthen health security and prepare for biothreats, 2022. The White House [cited 2022 Nov 7]. https://www.whitehouse.gov/briefing-room/statements-releases/2022/10/18/fact-sheet-biden-harris-administration-releases-strategy-to-strengthen-health-security-and-prepare-for-biothreats
- 6.Cieslak TJ, Kortepeter MG, Wojtyk RJ, Jansen HJ, Reyes RA, Smith JO; NATO Biological Medical Advisory Panel. Beyond the dirty dozen: a proposed methodology for assessing future bioweapon threats. Mil Med. 2018;183:e59–65. 10.1093/milmed/usx004 [DOI] [PubMed] [Google Scholar]
- 7.Australia Group Handbook. Volume II: biological weapons-related common control lists. 2021. [cited 2023 May 11]. https://www.dfat.gov.au/publications/minisite/theaustraliagroupnet/site/en/controllisthandbooks.html
- 8.Bureau of Biosecurity. Combined list of biological agents. 2012. [cited 2022 May 23]. https://www.bureaubiosecurity.nl/en/biological-agents/combined-list-of-biological-agents
- 9.Centers for Disease Control and Prevention. Biosafety in microbiological and biomedical laboratories (BMBL), 6th ed. CDC Laboratory Portal. 2020. [cited 2022 Sep 8].https://www.cdc.gov/labs/BMBL.html
- 10.Centers for Disease Control and Prevention. Bioterrorism agents/diseases. 2000. [cited 2021 Oct 17]. https://emergency.cdc.gov/agent/agentlist-category.asp
- 11.Rotz LD, Khan AS, Lillibridge SR, Ostroff SM, Hughes JM. Public health assessment of potential biological terrorism agents. Emerg Infect Dis. 2002;8:225–30. 10.3201/eid0802.010164 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Centers for Disease Control and Prevention. Classification of diseases, functioning, and disability. 2020. [cited 2022 Sep 6]. https://www.cdc.gov/nchs/icd/index.htm
- 13.Centers for Disease Control and Prevention. Federal Select Agent Program. 2017. [cited 2022 Sep 8]. https://www.selectagents.gov/
- 14.European Medicines Agency. Biological and chemical threats, 2002. [cited 2021 Oct 17]. https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/biological-chemical-threats
- 15.European Medicines Agency/Committee for Medicinal Products for Human Use. Guidance document on use of medicinal products for the treatment and prophylaxis of biological agents that might be used as weapons of bioterrorism, 2014. [cited 2021 Oct 17]. https://www.ema.europa.eu/en/documents/regulatory-procedural-guideline/european-medicines-agency/committee-proprietary-medicinal-products-guidance-document-use-medicinal-products-treatment_en.pdf
- 16.European Union. Biological agents directive 2000/54/EC. 2000. [cited 2023 May 11]. https://eur-lex.europa.eu/legal-content/EN/ALL/?uri=CELEX%3A32000L0054
- 17.Regulation of the European Union. 2017/2268 dual-use items. 2017 [cited 2021 Dec 21]. https://eur-lex.europa.eu/legal-content/NL/TXT/?uri=CELEX%3A32017R2268
- 18.German Federal Ministry of the Interior. War Weapons Control Act German Law Archive. 2002. [cited 2023 May 11]. https://germanlawarchive.iuscomp.org/?p=741
- 19.Annex: war weaponslList (Kriegswaffenliste, KWL). German Law Archive. [cited 2022 Oct 12]. Available from: https://germanlawarchive.iuscomp.org/?p=743
- 20.NATO. NATO Handbook on the medical aspects of NBC defensive operations. FAS.org. 1996. [cited 2022 Sep 8]. https://apps.dtic.mil/sti/citations/ADA434662
- 21.USAMRIID. USAMRIID’s medical management of biological casualties handbook. 2020. [cited 2022 Sep 9]. http://www.usamriid.army.mil
- 22.National Institute for Public Health and the Environment (RIVM). Overview notifications [in Dutch]. 2022. [cited 2021 Dec 1]. https://www.rivm.nl/meldingsplicht-infectieziekten/overzicht-meldingen
- 23.Birnie E, Savelkoel J, Reubsaet F, Roelofs JJTH, Soetekouw R, Kolkman S, et al. ; Dutch Melioidosis Study Group. Melioidosis in travelers: An analysis of Dutch melioidosis registry data 1985-2018. Travel Med Infect Dis. 2019;32:101461. 10.1016/j.tmaid.2019.07.017 [DOI] [PubMed] [Google Scholar]
- 24.Rijks JM, Tulen AD, Notermans DW, Reubsaet FAG, de Vries MC, Koene MGJ, et al. Tularemia transmission to humans, the Netherlands, 2011‒2021. Emerg Infect Dis. 2022;28:883–5. 10.3201/eid2804.211913 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Netherlands Central Government. Public Health Act [in Dutch]. 2008. [cited 2023 May 10]. https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---ilo_aids/documents/legaldocument/wcms_127977.pdf
- 26.Central Government. Population counter [in Dutch]. 2022. [cited 2022 May 23]. https://www.cbs.nl/nl-nl/visualisaties/dashboard-bevolking/bevolkingsteller
- 27.National Institute for Public Health and the Environment (RIVM). State of zoonosis [in Dutch]. 2018. [cited 2023 May 10]. https://www.rivm.nl/en/news/prevention-essential-thema-state-of-zoonotic-diseases-2018
- 28.National Institute for Public Health and the Environment (RIVM). State of zoonosis, 2012. [in Dutch]. 2013 [cited 2022 May 23]. https://www.rivm.nl/publicaties/staat-van-zoonosen-2012
- 29.National Institute for Public Health and the Environment (RIVM). State of zoonosis, 2016. [in Dutch]. 2017 [cited 2013 May 11]. https://www.rivm.nl/bibliotheek/rapporten/2017-0029.pdf
- 30.Schneeberger PM, Wintenberger C, van der Hoek W, Stahl JP. Q fever in the Netherlands - 2007-2010: what we learned from the largest outbreak ever. Med Mal Infect. 2014;44:339–53. 10.1016/j.medmal.2014.02.006 [DOI] [PubMed] [Google Scholar]
- 31.Limper M, Roest HI, van Gorp EC. [A patient with a fever and an eschar caused by tularemia] [in Dutch]. Ned Tijdschr Geneeskd. 2009;153:B84. [PubMed] [Google Scholar]
- 32.Haverkort JJ, Minderhoud AL, Wind JD, Leenen LP, Hoepelman AI, Ellerbroek PM. Hospital preparations for viral hemorrhagic fever patients and experience gained from admission of an Ebola patient. Emerg Infect Dis. 2016;22:184–91. 10.3201/eid2202.151393 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Deutsche Welle. UN peacekeeper flown to Netherlands for Ebola treatment. 2014. [cited 2021 Dec 1]. https://www.dw.com/en/un-peacekeeper-flown-to-netherlands-for-ebola-treatment/a-18114228
- 34.Wouthuyzen-Bakker M, Knoester M, van den Berg AP, GeurtsvanKessel CH, Koopmans MP, Van Leer-Buter C, et al. Yellow fever in a traveller returning from Suriname to the Netherlands, March 2017. Euro Surveill. 2017;22:30488. 10.2807/1560-7917.ES.2017.22.11.30488 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Phan MVT, Mendonca Melo M, van Nood E, Aron G, Kreeft-Voermans JJC, Koopmans MPG, et al. Shedding of yellow fever virus from an imported case in the Netherlands after travel to Brazil. Open Forum Infect Dis. 2020;7:a020. 10.1093/ofid/ofaa020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Phan MV, Murad SD, van der Eijk AA, Metselaar HJ, Hartog H, Harinck F, et al. Genomic sequence of yellow fever virus from a Dutch traveller returning from the Gambia-Senegal region, the Netherlands, November 2018. Euro Surveill. 2019;24:1. 10.2807/1560-7917.ES.2019.24.4.1800684 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Overbosch F, de Boer M, Veldkamp KE, Ellerbroek P, Bleeker-Rovers CP, Goorhuis B, et al. Lassa fever response team of The Netherlands. Public health response to two imported, epidemiologically related cases of Lassa fever in the Netherlands (ex Sierra Leone), November 2019. Euro Surveill. 2020;25:6–10. 10.2807/1560-7917.ES.2020.25.15.2000265 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Mulangu S, Dodd LE, Davey RT Jr, Tshiani Mbaya O, Proschan M, Mukadi D, et al. ; PALM Writing Group; PALM Consortium Study Team. PALM Consortium Study Team. A randomized, controlled trial of Ebola virus disease therapeutics. N Engl J Med. 2019;381:2293–303. 10.1056/NEJMoa1910993 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Eldin C, Mélenotte C, Mediannikov O, Ghigo E, Million M, Edouard S, et al. From Q fever to Coxiella burnetii infection: a paradigm change. Clin Microbiol Rev. 2017;30:115–90. 10.1128/CMR.00045-16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Jones RM, Nicas M, Hubbard A, Sylvester MD, Reingold A. The infectious dose of Francisella tularensis (tularemia). Appl Biosaf. 2005;10:227–39. 10.1177/153567600501000405 [DOI] [Google Scholar]
- 41.Centers for Disease Control and Prevention. Tularemia: diagnosis and treatment. [cited 2023 Apr 2]. https://www.cdc.gov/tularemia/diagnosistreatment/index.html
- 42.Kolwijck E, Lutgens SPM, Visser VXN, van Apeldoorn MJ, Graham H, Koets AP, et al. First case of human Brucella canis infection in the Netherlands. Clin Infect Dis. 2022;75:2250–2. 10.1093/cid/ciac425 [DOI] [PubMed] [Google Scholar]
- 43.Traxler RM, Lehman MW, Bosserman EA, Guerra MA, Smith TL. A literature review of laboratory-acquired brucellosis. J Clin Microbiol. 2013;51:3055–62. 10.1128/JCM.00135-13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Centers for Disease Control and Prevention. Brucellosis reference guide: exposures, testing, and prevention. 2017. [cited 2022 Sep 15]. https://www.cdc.gov/brucellosis/pdf/brucellosi-reference-guide.pdf
- 45.Centers for Disease Control and Prevention. Treatment. Brucellosis. 2012. [cited 2023 Apr 2]. https://www.cdc.gov/brucellosis/treatment
- 46.Inglis TJ, Sagripanti JL. Environmental factors that affect the survival and persistence of Burkholderia pseudomallei. Appl Environ Microbiol. 2006;72:6865–75. 10.1128/AEM.01036-06 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Wiersinga WJ, van der Poll T, White NJ, Day NP, Peacock SJ. Melioidosis: insights into the pathogenicity of Burkholderia pseudomallei. Nat Rev Microbiol. 2006;4:272–82. 10.1038/nrmicro1385 [DOI] [PubMed] [Google Scholar]
- 48.Tapia D, Sanchez-Villamil JI, Torres AG. Emerging role of biologics for the treatment of melioidosis and glanders. Expert Opin Biol Ther. 2019;19:1319–32. 10.1080/14712598.2019.1677602 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Grobusch MP, Weld L, Goorhuis A, Hamer DH, Schunk M, Jordan S, et al. ; for EuroTravNet. Travel-related infections presenting in Europe: A 20-year analysis of EuroTravNet surveillance data. Lancet Reg Health Eur. 2020;1:100001. 10.1016/j.lanepe.2020.100001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Clostridium, Bacteroides, and other anaerobes. In: Ryan KJ. Sherris Medical Microbiology, 7th ed. New York: McGraw Hill Medical [cited 2022 Oct 11]. https://accessmedicine.mhmedical.com/content.aspx?bookid=2268§ionid=176086328
- 51.Lutwick LI, Lutwick SM. Beyond anthrax: the weaponization of infectious diseases. New York: Humana Press; 2009. [Google Scholar]
- 52.Swaan CM, van Ouwerkerk IM, Roest HJ. Cluster of botulism among Dutch tourists in Turkey, June 2008. Euro Surveill. 2010;15:19532. 10.2807/ese.15.14.19532-en [DOI] [PubMed] [Google Scholar]
- 53.Swenson JM, Thornsberry C, McCroskey LM, Hatheway CL, Dowell VR Jr. Susceptibility of Clostridium botulinum to thirteen antimicrobial agents. Antimicrob Agents Chemother. 1980;18:13–9. 10.1128/AAC.18.1.13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Koene MG, De Rosa M, Spierenburg MA, Jacobi A, Roest HI. An old acquaintance, anthrax in the Netherlands [in Dutch]. Tijdschr Diergeneeskd. 2015;140:18–22. [Google Scholar]
- 55.Bower WA, Hendricks K, Pillai S, Guarnizo J, Meaney-Delman D; Centers for Disease Control and Prevention (CDC). Clinical framework and medical countermeasure use during an anthrax mass-casualty incident. MMWR Recomm Rep. 2015;64:1–22. 10.15585/mmwr.rr6404a1 [DOI] [PubMed] [Google Scholar]
- 56.Nguyen HN, Smith ME, Hayoun MA. Glanders and melioidosis, 2021. In: Handbook of Zoonosis. Tampa (FL): Statpearls; 2021. p.149–65 [cited 2012 Oct 11]. https://www.ncbi.nlm.nih.gov/books/NBK448110/ [Google Scholar]
- 57.Nicas M, Hubbard AE, Jones RM, Reingold AL. The infectious dose of variola (smallpox) virus. Appl Biosaf. 2004;9:118–27. 10.1177/153567600400900302 [DOI] [Google Scholar]
- 58.Fenner F, Henderson DA, Arita I. Z Jezek IL. Smallpox and its eradication. Geneva: World Health Organization; 1988. [cited 2022 Feb 16]. https://apps.who.int/iris/handle/10665/39485
- 59.Peeters MF. The smallpox epidemic in Tilburg in 1951 [in Dutch]. Tijdschr voor Infect. 2009. [cited 2023 May 11]. https://www.ariez.nl/wp-content/uploads/2018/08/231-4.pdf
- 60.Grosenbach DW, Honeychurch K, Rose EA, Chinsangaram J, Frimm A, Maiti B, et al. Oral tecovirimat for the treatment of smallpox. N Engl J Med. 2018;379:44–53. 10.1056/NEJMoa1705688 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Chan-Tack K, Harrington P, Bensman T, Choi SY, Donaldson E, O’Rear J, et al. Benefit-risk assessment for brincidofovir for the treatment of smallpox: U.S. Food and Drug Administration’s Evaluation. Antiviral Res. 2021;195:105182. 10.1016/j.antiviral.2021.105182 [DOI] [PubMed] [Google Scholar]
- 62.World Health Organization. The Independent Advisory Group on public health implications of synthetic biology technology related to smallpox. 2015. [cited 2022 Jan 15]. https://www.who.int/publications/i/item/the-independent-advisory-group-on-public-health-implications-of-synthetic-biology-technology-related-to-smallpox
- 63.Miner KR, D’Andrilli J, Mackelprang R, Edwards A, Malaska MJ, Waldrop MP, et al. Emergent biogeochemical risks from Arctic permafrost degradation. Nat Clim Chang. 2021;11:809–19. 10.1038/s41558-021-01162-y [DOI] [Google Scholar]
- 64.Thornhill JP, Barkati S, Walmsley S, Rockstroh J, Antinori A, Harrison LB, et al. ; SHARE-net Clinical Group. Monkeypox virus infection in humans across 16 countries, April‒June 2022. N Engl J Med. 2022;387:679–91. 10.1056/NEJMoa2207323 [DOI] [PubMed] [Google Scholar]
- 65.Angelo KM, Smith T, Camprubí-Ferrer D, Balerdi-Sarasola L, Díaz Menéndez M, Servera-Negre G, et al. ; GeoSentinel Network Collaborators. Epidemiological and clinical characteristics of patients with monkeypox in the GeoSentinel Network: a cross-sectional study. Lancet Infect Dis. 2023;23:196–206. 10.1016/S1473-3099(22)00651-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.van Ewijk CE, Miura F, van Rijckevorsel G, de Vries HJ, Welkers MA, van den Berg OE, et al. Monkeypox outbreak in the Netherlands in 2022: public health response, epidemiological and clinical characteristics of the first 1000 cases and protection of the first-generation smallpox vaccine. Euro Surveill. 2023;28:2200772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Brooks JT, Marks P, Goldstein RH, Walensky RP. Intradermal vaccination for monkeypox: benefits for individual and public health. N Engl J Med. 2022;387:1151–3. 10.1056/NEJMp2211311 [DOI] [PubMed] [Google Scholar]
- 68.Sluiter E. Bubonic plague on board a ship in Rotterdam [in Dutch]. 1929. [cited 2022 Feb 16]. https://www.ntvg.nl/artikelen/builenpest-aan-boord-van-een-schip-te-rotterdam
- 69.Randremanana R, Andrianaivoarimanana V, Nikolay B, Ramasindrazana B, Paireau J, Ten Bosch QA, et al. Epidemiological characteristics of an urban plague epidemic in Madagascar, August-November, 2017: an outbreak report. Lancet Infect Dis. 2019;19:537–45. 10.1016/S1473-3099(18)30730-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Adamovicz JJ, Worsham PL. Plague. In: Swearengen, JR, editor. Biodefense research methodology and animal models, 2nd ed. Boca Raton (FL): CRC; 2022. p. 113‒46. [Google Scholar]
- 71.Nelson CA, Meaney-Delman D, Fleck-Derderian S, Cooley KM, Yu PA, Mead PS; Contributors. Antimicrobial treatment and prophylaxis of plague: recommendations for naturally acquired infections and bioterrorism response. MMWR Recomm Rep. 2021;70:1–27. 10.15585/mmwr.rr7003a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.National Institute for Public Health and the Environment (RIVM). Biosecurity self-scan toolkit. Biosecurity office. 2022. [cited 2023 May 11]. https://www.biosecurityselfscan.nl
- 73.National Institute for Public Health and the Environment (RIVM). Vulnerability scan, Biosecurity office. 2019. [cited 2022 Jul 8]. https://biosecurityvulnerabilityscan.nl
- 74.IFV. Protocol suspicious objects [in Dutch]. 2015. [cited 2022 Jan 11]. https://www.ifv.nl/kennisplein/crises-en-crisisbeheersing/publicaties/protocol-verdachte-objecten-2015