

Abstract
Objective
To assess the impact of delayed invitation on screen-detected and interval colorectal cancers (CRC) within a faecal immunochemical testing (FIT)-based CRC screening programme.
Design
All individuals that participated in 2017 and 2018 with a negative FIT and were eligible for CRC screening in 2019 and 2020 were included using individual-level data. Multivariable logistic regression analyses were used to assess the association between either the different time periods (ie, ‘before’, ‘during’ and ‘after’ the first COVID-19 wave) or the invitation interval on screen-detected and interval CRCs.
Results
Positive predictive value for advanced neoplasia (AN) was slightly lower during (OR=0.91) and after (OR=0.95) the first COVID-19 wave, but no significant difference was observed for the different invitation intervals. Out of all individuals that previously tested negative, 84 (0.004%) had an interval CRC beyond the 24 months since their last invitation. The time period of invitation as well as the extended invitation interval was not associated with detection rates for AN and interval CRC rate.
Conclusion
The impact of the first COVID-19 wave on screening yield was modest. A very small proportion of the FIT negatives had an interval CRC possibly due to an extended interval, which potentially could have been prevented if they had received the invitation earlier. Nonetheless, no increase in interval CRC rate was observed, indicating that an extended invitation interval up to 30 months had no negative impact on the performance of the CRC screening programme and a modest extension of the invitation interval seems an appropriate intervention.
Keywords: COVID-19, COLORECTAL CANCER SCREENING
WHAT IS ALREADY KNOWN ON THIS TOPIC
Most cancer screenings were suspended during COVID-19, resulting in an absolute reduction in cancer yield when comparing invitation year 2020 to the preceding invitation year 2019. Modelling studies showed, however, that a short extension (ie, <3 months) will have a minimal impact of the long-term benefits of screening.
WHAT THIS STUDY ADDS
The impact of the first COVID-19 wave on screening yield was modest. An extended invitation interval of up to 30 months had no negative impact on the positive predictive value for advanced neoplasia or interval cancer rate as the entire screening process was only postponed for a few months and individuals caught up their missed invitation.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study showed that in case of future disruption of healthcare or programmes resulting in restricted colonoscopy capacity a modest extension of the invitation interval up to 30 months seems an appropriate intervention.
Introduction
Worldwide, many cancer screening programmes have been impacted by the COVID-19 pandemic. Many countries were forced to temporarily suspend their screening programme to lower the burden of non-emergency healthcare.1–5 In the Netherlands, the biennial faecal immunochemical testing (FIT)-based colorectal cancer (CRC) screening programme was completely suspended for 2 months during the first COVID-19 wave in 2020.
Many reports have shown that the COVID-19 pandemic resulted in a decrease in CRC detection mainly due to a decrease in screen-detected CRCs as a result of the suspension of screening.1–3 6 7 This was also reflected in the CRC incidence rate in the Netherlands, showing a decrease during the first COVID-19 wave.8 9 After the restart of the screening programme, however, a stabilisation and even a small increase in CRC incidence rate were observed by the end of 2020.
The restart screening strategy in the Dutch CRC screening programme was a well-considered decision, informed by long-term predications of microsimulation model. Three scenarios were modelled to determine the optimal restart screening strategy in the Netherlands: (1) omit screening in certain age groups, (2) increase the FIT cut-off and (3) extend the invitation interval. This latter modelled strategy turned out to be the best option in terms of balancing the reduction in colonoscopy capacity with maintaining the benefits of the programme.2 In line with the outcomes of this modelling study, the Dutch Minister of Health decided to extend the invitation interval from 24 months up to a maximum of 30 months to anticipate on the disruption of screening to avoid non-emergency healthcare.
It is important to evaluate whether the decision to extend the invitation interval actually resulted in a moderate reduction in screening yield. Moreover, it is unknown whether this extended invitation interval negatively impacts the yield of CRC screening or results in an increase in number of interval CRCs. Therefore, this study assessed the impact of the first COVID-19 wave as well as the associated extended invitation interval on screen-detected CRCs and interval CRCs within the Dutch CRC screening programme.
Methods
Dutch CRC screening programme
CRC screening was implemented in the Netherlands in 2014.10 The target population consist of men and women aged 55–75 years. All eligible individuals are invited biennially. The primary screening modality is the FIT, with a positivity threshold of 47 µg haemoglobin per gram (Hb/g) faeces. If the FIT result is positive, individuals are referred for intake for follow-up colonoscopy. Location and date of the intake for colonoscopy is determined on date of first available slots and second on travel distance to intake location. If the FIT result is negative, individuals receive a new invitation after 24 months. Individuals with relevant findings at colonoscopy will be treated and go into surveillance in compliance with Dutch guidelines. Individuals without relevant findings at the colonoscopy will return to the CRC screening programme in 10 years.
First COVID-19 wave in the Netherlands
COVID-19 in the Netherlands and its impact on the CRC incidence has been previously described.9 In short, on 27 February 2020, the first COVID-19 case was confirmed, with a rapid increase in new COVID-19 cases in the subsequent weeks. This placed a tremendous strain on the healthcare system in the Netherlands. In a response, the National Institute for Public Health and the Environment announced to stop inviting individuals for CRC screening from 16 March 2020. At that time, individuals already invited were still able to return their FIT or those tested FIT positive could still undergo colonoscopy. By the end of March, individuals were asked to stop returning their FIT. In the second half of May 2020, the screening invitations were gradually resumed, starting with reinviting the backlog prioritising those that already received an invitation and thereafter those eligible for subsequent screening rounds (ie, second, third, fourth rounds). From 1 June 2020 onwards, invitations were sent to the total target population again, although at that time still at lower rates than before the first COVID-19 wave. Figure 1 shows the numbers of invitations sent per month for 2019, 2020 and first half of 2021.
Figure 1.

Number of screening invitations per month by calendar years 2019, 2020 and first half of 2021.
Study population
Participants eligible and originally scheduled for second or third invitation round of FIT screening in 2019 and 2020 were included in this study. Fourth round invitees were excluded because they were only invited in 2020, making a comparison with invitees of 2019 (ie, prior to COVID-19) impossible. Individuals were only eligible to be included in this study if they participated and had a negative FIT in the previous invitation round. Allowing for adequate follow-up time for all individuals, study participants were included in the study if invited for CRC screening before 1 July 2021. For interval CRC data, all CRCs detected in the period after the previous negative FIT in 2017 and 2018 but before the new invitation for the subsequent screening round in 2019 and 2020 were included. As there is a slight delay in the default linkage between the national screening information system (ScreenIT) and Netherlands Cancer Registry (NCR), study participants were included in the analysis for interval CRC if they were invited before 1 January 2021.
Database and definitions
Database
All data on the key performance indicators of the Dutch CRC screening programme were retrieved from ScreenIT using data until 31 October 2021. Data on interval CRCs were retrieved from NCR, the Dutch national cancer registry in which all cancer data are captured. All participants with a negative FIT in the screening database were linked with the NCR to identify whether there was a CRC clinically detected before the next invitation.
Key performance indicators
Our key performance indicators of interest were the following:
Invitation interval: number of days between invitation date of the previous screening round (2017 or 2018) and invitation date of the current screening round (2019, 2020 or 2021).
Screening interval: number of days between date of FIT analysis in the previous screening round (2017 or 2018) and date of FIT analysis in the current screening round (2019, 2020 or 2021).
Person-years: number of days between date of invitation in the previous screening round (2017 or 2018) and either the data of invitation in the current screening round (2019, 2020 or 2021) or, in case of an interval CRC, the incidence date of the CRC.
FIT participation rate: number of individuals returning their FIT divided by the number of individuals invited.
Participation rate of follow-up colonoscopy: number of individuals undergoing colonoscopy divided by the number of individuals with a positive FIT.
FIT positivity rate: number of individuals with a positive FIT divided by the number of individuals that returned an assessable FIT.
Positive predictive value (PPV) for CRC or advanced neoplasia (AN): number of individuals with CRC or AN detected divided by the number of individuals undergoing colonoscopy.
Detection rate for CRC or AN: number of individuals with CRC or AN detected divided by the number of individuals that returned their FIT.
Interval CRC rate: number of individuals with CRC diagnosed after a negative FIT per 10 000 individuals with a negative FIT and per 10 000 person-years. ANs are considered relevant findings within the Dutch CRC screening programme and consist of CRCs and advanced adenomas (AA). Screen-detected CRCs were defined as CRCs detected within 6 months after a positive FIT. An AA was defined as any adenoma with histology showing ≥25% villous component or adenoma with high-grade dysplasia or with size ≥10 mm. Interval CRC is defined as CRC diagnosed after a previous negative FIT and before invitation to the next screening round. Individuals were only eligible to be included in this study if they had a negative FIT in the previous screening round in 2017 or 2018 and were invited in 2019, 2020 or 2021. As a result, data of interval CRCs were complete for all study participants.
Time points of invitation and invitation interval
In the first analysis we assessed the impact of the different time points of sending the invitation on the key performance indicators. We defined the three different time points as follows: (1) period ‘before’ the first COVID-19 wave consisting of all invitations sent from January 2019 until January 2020; (2) period ‘during’ the first COVID-19 wave consisting of all invitations sent from February 2020 until June 2020; and (3) period ‘after’ the first COVID-19 wave consisting of all invitations sent from July 2020 until June 2021. In the second analysis, we assessed the impact of the invitation interval on the key performance indicators, regardless in which time period they were invited. For the invitation interval the following categories were defined: ≤24–25 months, 25–26 months, 26–27 months, 27–28 months, 28–29 months and >29 months. Because the scheduled dates of invitation for first round invitees were unknown, delay in invitation could not be determined for this group.
Statistical analyses
Χ2 test was used to determine differences between moment of invitation for study population demographics, with p values <0.05 considered statistically significant. Multivariable logistic regression analyses were used to assess the association between either the different time periods or the invitation interval on PPV, detection rates and interval CRC, adjusted for the well-known confounding factors age, sex and invitation round. For each key performance indicator two models were constructed; a base model including the key performance indicator and confounding variables and an alternative model including an additional variable time period or invitation interval. Likelihood ratio test was used to test whether the alternative model better fitted the data than the base model. The alternative model was considered significantly better with p values <0.05.
Results
Between 1 January 2019 and 1 July 2021, a total of 3 035 847 individuals were invited to participate in FIT-based screening in the Netherlands; 742 751 first round invitees and 2 293 096 subsequent round invitees (table 1). In this study, only outcomes of subsequent screening round are presented.
Table 1.
Demographics of the study population before, during and after the first COVID-19 wave
| Total | Before | During | After | |||||
| Subsequent invitation round | ||||||||
| n | % | n | % | n | % | n | % | |
| Total | 2 293 096 | 100.0 | 1 289 655 | 56.2 | 239 538 | 10.4 | 763 903 | 33.3 |
| Men | 1 078 429 | 47.0 | 608 365 | 47.2 | 111 866 | 46.7 | 358 198 | 46.9 |
| Women | 1 214 667 | 53.0 | 681 290 | 52.8 | 127 672 | 53.3 | 405 705 | 53.1 |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |||||
| Age in years | 65.2 (5.3) | 66.6 (5.1) | 64.6 (6.1) | 63.0 (4.7) | ||||
| Invitation interval in days | 761.5 (46.2) | 734.8 (9.9) | 759.3 (39.0) | 807.2 (49.8) | ||||
| Screening interval in days | 762.0 (58.9) | 734.3 (36.4) | 772.5 (62.5) | 805.6 (61.2) | ||||
Impact timing of invitation on key performance indicators
Mean age was higher before the COVID-19 wave with 66.6 (SD 5.1) years, and lower with 64.6 (SD 6.1) years and 63.0 (SD 4.7) years during and after, respectively (p<0.001; table 1). Mean invitation interval differed for the different time periods: 735 (SD 9.9) days before, 759 (SD 39.0) days during and 807 (SD 49.8) days after the COVID-19 wave (p<0.001). A similar pattern was observed for the mean screening intervals, with also the longest interval after the COVID-19 wave.
A total of 2 106 978 (91.9%) individuals participated by returning their FIT. FIT participation rate differed for the three time periods, with a similar trend in participation rate observed for the follow-up colonoscopy (online supplemental table 1). In total, 84 340 (4.0%) individuals tested FIT positive in the subsequent invitation rounds, without significant differences between the three time periods.
gutjnl-2022-328559supp001.pdf (209.5KB, pdf)
During follow-up colonoscopy, 3622 (4.9%) CRCs and 21 152 (28.7%) AAs were diagnosed. PPVs for CRC and AN, as well as the detection rates for CRC and AN, were significantly lower during and after, with ORs ranging from 0.91 to 0.97 (table 2A). FIT interval CRC rate was not significantly different for the three time periods; 3.9 per 10 000 person-years before, 3.4 per 10 000 person-years during and 2.6 per 10 000 person-years after the first COVID-19 wave (table 3).
Table 2.
Multivariable logistic regression analyses for impact of (A) the invitation time period or (B) invitation interval on the detection of AN and interval CRC in the subsequent invitation round
| PPV for CRC | PPV for AN† | Detection rate for CRC | Detection rate for AN† | |||||||||||||
| % | OR | 95% CI | % | OR | 95% CI | % | OR | 95% CI | % | OR | 95% CI | |||||
| A. Invitation period | ||||||||||||||||
| Before | 5.3 | Ref | 34.7 | Ref* | 0.19 | Ref | 1.25 | Ref | ||||||||
| During | 4.6 | 0.91 | 0.81 | 1.1.03 | 31.8 | 0.91 | 0.86 | 0.96 | 0.16 | 0.90 | 0.80 | 1.01 | 1.09 | 0.92 | 0.88 | 0.96 |
| After | 4.2 | 0.91 | 0.84 | 0.99 | 32.0 | 0.95 | 0.92 | 0.98 | 0.14 | 0.92 | 0.85 | 0.99 | 1.07 | 0.97 | 0.94 | 1.00 |
| B. Invitation interval (months) | ||||||||||||||||
| ≤24–25 | 5.1 | Ref | 33.9 | Ref | 0.18 | Ref | 1.20 | Ref | ||||||||
| 25–26 | 4.7 | 1.02 | 0.89 | 1.17 | 32.9 | 1.02 | 0.96 | 1.09 | 0.16 | 1.04 | 0.92 | 1.19 | 1.11 | 0.78 | 0.75 | 1.09 |
| 26–27 | 4.6 | 1.01 | 0.89 | 1.14 | 31.9 | 1.01 | 0.96 | 1.07 | 0.15 | 1.02 | 0.91 | 1.15 | 1.07 | 1.04 | 0.99 | 1.07 |
| 27–28 | 3.9 | 0.89 | 0.77 | 1.02 | 31.3 | 0.98 | 0.92 | 1.04 | 0.13 | 0.93 | 0.81 | 1.07 | 1.06 | 1.02 | 0.98 | 1.08 |
| 28–29 | 4.1 | 0.89 | 0.74 | 1.08 | 33.4 | 1.05 | 0.97 | 1.14 | 0.14 | 0.94 | 0.78 | 1.13 | 1.15 | 1.02 | 0.97 | 1.16 |
| >29 | 4.3 | 0.92 | 0.72 | 1.17 | 32.8 | 1.04 | 0.94 | 1.15 | 0.28 | 0.94 | 0.74 | 1.19 | 2.16 | 1.09 | 1.02 | 1.13 |
All ORs are adjusted for confounding variables age, sex and invitation round.
*Ref indicates that the alternative model (including the time period) better fitted the data. All ORs are presented for the alternative model including time period, regardless if it improved the model.
†AN is the combination of colorectal cancer and advanced neoplasia.
AN, advanced neoplasia; CRC, colorectal cancer; PPV, positive predictive value.
Table 3.
Multivariable logistic regression analyses for impact of the invitation time period on interval cancer rate
| Period | n | Interval CRC per 10 000 negative FITs | Interval CRC per 10 000 person-years | OR | 95% CI |
| Before | 1006 | 7.8 | 3.9 | Ref* | |
| During | 167 | 7.0 | 3.4 | 1.04 | 0.88–1.23 |
| After | 391 | 5.7 | 2.6 | 1.07 | 0.94–1.22 |
All ORs are adjusted for confounding variables age, sex and invitation round.
*Ref indicates that the alternative model (including the time period) better fitted the data. All ORs are presented for the alternative model including time period, regardless if it improved the model.
CRC, colorectal cancer; FIT, faecal immunochemical testing.
Impact of extended invitation interval on key performance indicators
The extension of the invitation interval resulted in an average extension of 72.4 days, with the longest invitation interval of 807.2 (SD 49.8) days in the period after COVID-19 wave and the shortest invitation interval of 734.8 (SD 9.9) days before the COVID-19 wave (table 1). The majority of the individuals were invited within 24–25 months (68.3%), with only a small proportion of the target population having an invitation interval beyond 29 months (2.3%; figure 2). Participants with the longest invitation interval (>29 months) were more likely to return their FIT than those with the standard invitation interval (24–25 months) (OR=1.15; 95% CI 1.11–1.19; online supplemental table 2). The positivity rate differed significantly by length of the invitation interval, but without an upward trend, with ORs varying from 1.01 to 1.05. The participation rate to follow-up colonoscopy was not significantly different for the different invitation intervals.
Figure 2.

Distribution of individuals by length of invitation interval.
The extended invitation interval had no impact on the diagnostic yield of CRC screening; PPVs for CRC and AN, as well as the detection rates for CRC and AN, were not significantly different for various lengths of the invitation interval (table 4). Figure 3 shows the cumulative interval CRC rate for individuals with and without an extended invitation interval; interval CRC rate (per 10 000 persons with a negative FIT) was not higher for individuals with an extended invitation interval than for individuals with a regular invitation interval. This was confirmed in the logistic regression analysis, which showed that the length of the invitation interval was not significantly associated with interval CRC risk. Of all the interval CRCs, 84 (5.4%) were detected ≥25 months after the previous negative FIT. In other words, 0.004% of all individuals with a negative FIT had an interval CRC beyond the regular invitation interval of 24 months.
Table 4.
Multivariable logistic regression analyses for impact of the invitation interval on interval cancer rate
| Invitation interval (months) |
n | Interval CRC per 10 000 negative FITs | Interval CRC per 10 000 person-years | OR | 95% CI |
| ≤24–25 | 1136 | 7.3 | 3.6 | ||
| 25–26 | 102 | 6.2 | 2.9 | 1.11 | 0.91–1.37 |
| 26–27 | 136 | 6.3 | 2.8 | 1.18 | 0.98–1.41 |
| 27–28 | 104 | 6.6 | 2.9 | 1.24 | 1.01–1.53 |
| 28–29 | 63 | 7.8 | 3.3 | 1.41 | 1.09–1.83 |
| >29 | 23 | 7.3 | 2.9 | 1.31 | 0.86–1.98 |
All ORs are adjusted for confounding variables age, sex and invitation round.
*Indicates that the alternative model (including the time period) better fitted the data. All ORs are presented for the alternative model including time period, regardless if it improved the model.
CRC, colorectal cancer; FIT, faecal immunochemical testing.
Figure 3.
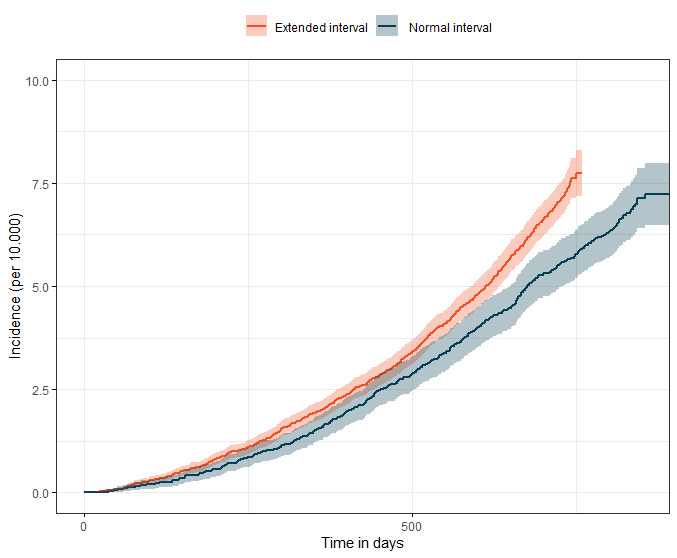
Interval cancer rate over time for individuals with and without extended invitation interval.
Discussion
The first wave of the COVID-19 pandemic resulted in a temporary interruption of the national CRC screening programme in the Netherlands. To clear the backlog, it was decided to extend the invitation interval for a limited time period. This extension of an average 73 days had a minimal impact on the yield of the CRC screening programme. More importantly, despite the extension of the invitation interval up to 30 months, there was no significant increase in the number of interval CRCs.
The decision to extend the invitation interval up to a maximum of 30 months resulted in an increase in the length of the invitation interval of 72.4 days (2.5 months) after the restart of the programme in June 2020. This implies that on average individuals were invited after 26.5 months, far below the maximum of 30 months. A similar extension of the invitation interval was observed in Flanders, Belgium, with a screening interval of 25.5 months.5
No significantly higher interval CRC rate was observed among the invitees that received an extended invitation interval. Nonetheless, although the rate was not significantly different, a small proportion (~5%) of the interval CRCs were diagnosed beyond the regular invitation interval of 24 months. The number is most likely too small to result in a significant increase in interval CRC rate. These CRCs could potentially have been diagnosed slightly earlier if the invitation interval would have been shorter. The impact, although minimal, of the first COVID-19 wave on the yield of CRC screening was unexpected. We had anticipated on an increase in PPV for AN because of the delay in invitation, potentially leading to progression of the disease. Although a minimally higher positivity rate was observed in the first invitation round, PPV for AN was actually lower in subsequent invitation round during and after the first COVID-19 wave. Thus, slightly more or similar percentages of individuals had a positive FIT but relatively more individuals had a false-positive result (ie, lower specificity). Therefore, we can only hypothesise on the slightly lower PPV in our study; for example, that blood in the stool might be related to other underlying conditions than colorectal neoplasia or polyps.
To our knowledge, no previous study has evaluated the impact of COVID-19 on interval CRCs. The impact of COVID-19 on the yield of CRC screening has been studied.2 9–11 The findings of this current study, however, are in contrast to previously published studies. They all showed a large decrease in the yield of CRC screening. Coma et al 2 showed a 34% reduction in AN detection in Catalonia, Spain.2 Another study from the same region showed that the screen-detected CRCs were less often detected at an early stage in 2020 compared with 2019.10 Lee et al showed a decrease in the absolute number of screening tests (FIT or colonoscopies) performed, leading to a decrease in AN detection in Northern California, USA.11 These findings are all in line with our previous publication, also showing fewer CRC diagnoses most likely related to the suspension of CRC screening in the Netherlands.9 In this study, however, we looked at the impact of COVID-19 from a different angle. We focused on the impact of the delayed invitation interval on the outcomes of CRC screening for individuals that were invited. The yield of CRC screening was calculated for individuals with a positive FIT that actually underwent a colonoscopy. This showed that the impact of COVID-19 with the associated extended invitation interval on the yield of CRC screening is clinically irrelevant for an individual. This is in contrast to other studies that all showed a significant decrease in yield on a population level. The limited impact of the delayed invitation for an individual as observed in our study was the result of relatively short disruption period of 2.5 months, thus conforming to what was hypothesised in the Flanders study; a short extension will have no impact on the yield of cancer screening programmes.5
The strength of our study is the large sample size and the use of high-quality data captured in the national information system used for the cancer screening programmes. Also the default linkage with the national cancer registry enabled us to report on interval CRCs in a timely manner. Another strength is that the findings of this study correspond to the predictions of the prior modelling study used to determine the optimal restart strategy, predicting that such a short extension (ie, <3 months) will have a minimal impact of the long-term benefits of screening.12 13 A limitation of our study is the lack of data on cancer staging, because these data are not available yet for CRCs detected in 2021. Although it is not expected that CRCs have developed into late-stage cancers with an average extension of 2.5 months, this expectation needs to be confirmed in future studies.
The findings of this study are reassuring for all cancer screening programmes worldwide. It underlines the relevance to restart as soon as possible after an unavoidable interruption of the screening programme. Moreover, it shows that widening the invitation interval for the total population enables a larger part of the population to participate in CRC screening while there is restricted colonoscopy capacity. This is relevant for the situation of COVID-19 and is important in case of future disruption of healthcare or programmes resulting in restricted colonoscopy capacity. A modest extension of the invitation interval up to 30 months seems an appropriate intervention.
To conclude, a temporary suspension of the Dutch CRC screening programme resulting in an extension of the invitation interval did not lead to an increase in the interval CRC rate. The entire screening process was only postponed for a few months and individuals caught up their missed invitation. The extension of the invitation interval turned out to be a good decision, as it allowed the screening programme to be resumed quickly, thereby catching up with the delayed invitations.
Footnotes
Correction notice: This article has been corrected since it published Online First. Errors in the result section of the abstract has been corrected as well as typographical errors in table 2.
Contributors: ET-Z was responsible for study coordination and data collection and is guarantor. ET-Z and LdJ were responsible for data analysis and writing the first version of the manuscript. ET-Z, IL-V and LdJ drafted the final manuscript. All authors gave critical revisions on the intellectual content of the manuscript and approved the final manuscript.
Funding: This research was funded by the National Institute for Public Health and the Environment.
Disclaimer: The funder had no role in the data collection, statistical analyses, interpretation of the results and writing the manuscript.
Competing interests: None declared.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review: Not commissioned; internally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
Data may be obtained from a third party and are not publicly available. Researchers had access to the data for the purpose of evaluation of the national colorectal cancer screening programme. The data are owned by Bevolkingsonderzoek Nederland (BVO-NL) and stored in the national screening database (ScreenIT). Researchers interested in accessing and analysing the data may contact the data officer of BVO-NL (wetenschappelijkonderzoek@bevolkingsonderzoeknederland.nl).
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
This study involves human participants and retrospective deidentified data were used. Participants gave informed consent to participate in the study before taking part.
References
- 1. Chiu H-M, Su C-W, Hsu W-F, et al. Mitigating the impact of COVID-19 on colorectal cancer screening: organized service screening perspectives from the Asia-Pacific region. Preventive Medicine 2021;151:106622. 10.1016/j.ypmed.2021.106622 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Coma E, Guiriguet C, Mora N, et al. Impact of the COVID-19 pandemic and related control measures on cancer diagnosis in Catalonia: a time-series analysis of primary care electronic health records covering about five million people. BMJ Open 2021;11:e047567. 10.1136/bmjopen-2020-047567 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Kempf E, Lamé G, Layese R, et al. New cancer cases at the time of sars-cov2 pandemic and related public health policies: a persistent and concerning decrease long after the end of the national lockdown. Eur J Cancer 2021;150:260–7. 10.1016/j.ejca.2021.02.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Battisti F, Falini P, Gorini G, et al. Cancer screening programmes in italy during the COVID-19 pandemic: an update of a nationwide survey on activity volumes and delayed diagnoses. Ann Ist Super Sanita 2022;58:16–24. 10.4415/ANN_22_01_03 [DOI] [PubMed] [Google Scholar]
- 5. Jidkova S, Hoeck S, Kellen E, et al. Flemish population-based cancer screening programs: impact of COVID-19 related shutdown on short-term key performance indicators. BMC Cancer 2022;22:183. 10.1186/s12885-022-09292-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Kortlever TL, de Jonge L, Wisse PHA, et al. The national fit-based colorectal cancer screening program in the netherlands during the covid-19 pandemic. Prev Med 2021;151:106643. 10.1016/j.ypmed.2021.106643 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Impact COVID-19 on cancer-related health services. Available: https://www.canceraustralia.gov.au/the-impact-of-C [Accessed 12 Mar 2022].
- 8. Dinmohamed AG, Visser O, Verhoeven RHA, et al. Fewer cancer diagnoses during the COVID-19 epidemic in the Netherlands. The Lancet Oncology 2020;21:750–1. 10.1016/S1470-2045(20)30265-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Toes-Zoutendijk E, Vink G, Nagtegaal ID, et al. Impact of covid-19 and suspension of colorectal cancer screening on incidence and stage distribution of colorectal cancers in the Netherlands. Eur J Cancer 2022;161:38–43. 10.1016/j.ejca.2021.11.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Vives N, Binefa G, Vidal C, et al. Short-term impact of the covid-19 pandemic on a population-based screening program for colorectal cancer in Catalonia (Spain). Prev Med 2022;155:106929. 10.1016/j.ypmed.2021.106929 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Lee JK, Lam AY, Jensen CD, et al. Impact of the covid-19 pandemic on fecal immunochemical testing, colonoscopy services, and colorectal neoplasia detection in a large United States community-based population. Gastroenterology 2022;163:723–31. 10.1053/j.gastro.2022.05.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. de Jonge L, Worthington J, van Wifferen F, et al. Impact of the covid-19 pandemic on faecal immunochemical test-based colorectal cancer screening programmes in Australia, Canada, and the Netherlands: a comparative modelling study. Lancet Gastroenterol Hepatol 2021;6:304–14. 10.1016/S2468-1253(21)00003-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Kregting L, Kaljouw S, de Jonge L, et al. Effects of cancer screening restart strategies after COVID-19 disruption. Eur J Cancer 2020;138:S16. 10.1016/S0959-8049(20)30561-X [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
gutjnl-2022-328559supp001.pdf (209.5KB, pdf)
Data Availability Statement
Data may be obtained from a third party and are not publicly available. Researchers had access to the data for the purpose of evaluation of the national colorectal cancer screening programme. The data are owned by Bevolkingsonderzoek Nederland (BVO-NL) and stored in the national screening database (ScreenIT). Researchers interested in accessing and analysing the data may contact the data officer of BVO-NL (wetenschappelijkonderzoek@bevolkingsonderzoeknederland.nl).