

Abstract
Background
The mental health and wellbeing of care-experienced children and young people (i.e. foster care, kinship care, residential care) is poorer than non-care-experienced populations. The Care-experienced cHildren and young people’s Interventions to improve Mental health and wEll-being outcomes Systematic review (CHIMES) aimed to synthesise the international evidence base for interventions targeting subjective wellbeing, mental health and suicide amongst care-experienced young people aged ≤ 25 years.
Methods
For the first phase of the review, we constructed an evidence map identifying key clusters and gaps in interventions and evaluations. Studies were identified through 16 electronic databases and 22 health and social care websites, in addition to expert recommendations, citation tracking and screening of relevant systematic reviews. We charted interventions and evaluations with a summary narrative, tables and infographics.
Results
In total, 64 interventions with 124 associated study reports were eligible. The majority of study reports were from the USA (n = 77). Interventions primarily targeted children and young people’s skills and competencies (n = 9 interventions), the parental functioning and practices of carers (n = 26), or a combination of the two (n = 15). While theoretically under-specified, interventions were largely informed by theories of Attachment, Positive Youth Development, and Social Learning Theory. Current evaluations prioritised outcomes (n = 86) and processes (n = 50), with a paucity of study reports including theoretical descriptions (n = 24) or economic evaluations (n = 1). Interventions most frequently targeted outcomes related to mental, behavioural or neurodevelopmental disorders, notably total social, emotional and behavioural problems (n = 48 interventions) and externalising problem behaviours (n = 26). There were a limited number of interventions targeting subjective wellbeing or suicide-related outcomes.
Conclusions
Future intervention development might focus on structural-level intervention theories and components, and target outcomes related to subjective wellbeing and suicide. In accordance with current methodological guidance for intervention development and evaluation, research needs to integrate theoretical, outcome, process and economic evaluation in order to strengthen the evidence base.
Systematic review registration
PROSPERO CRD42020177478.
Keyword: Systematic review, Scoping review, Mental health, Wellbeing, Foster care, Residential care, Children, Adolescents
Background
Children and young people with experience of living in care represent a diverse population, with significant international variation in nomenclature and classification [1]. They can be defined as individuals who have had statutory involvement, whereby parental rights have been transferred to another adult. In some countries, such as the UK, there are specific mechanisms to support care entry, such as the issuing of Special Guardianship Orders [2]. Care can include a range of placement types, such as formal kinship care, foster care and residential care [3]. There are also variations in the identity of care-leavers, who are largely defined by their ongoing rights to statutory provision. For example in Germany, young people from a range of care placements are entitled to legal assistance until 21 years old while in England they are entitled to certain services up to 25 [3]. Globally, the estimation of children and young people in care has been challenging, with most recent efforts to establish the prevalence of individuals in institutional care reporting a range from 3.18 million to 9.42 million, depending on the methods and data sources employed [4].
While not a clearly defined population, evidence reports that care-experienced individuals generally have poorer mental health and wellbeing, and higher rates of suicide attempts, compared to non-care-experienced groups [5–9]. Individuals with a history of care have excess mortality in adulthood, attributable to non-natural causes of self-harm, accidents, and other mental health and behavioural risk [10]. Mental health problems incur substantial health and social care costs, largely due to the associated risk of placement instability and breakdown [11–13], which is concerning given increased financial pressures on social care systems [14].
There has been significant development in international intervention research to target reported issues. A number of literature and systematic reviews have synthesised the evidence base for social and healthcare approaches [15–25], with recent National Institute for Health and Care Excellence (NICE) reviews and associated guideline recommendations endorsing implementation of interventions centred on mentoring, positive parenting practices and system change to facilitate more efficient implementation [26].
Despite their contributions, there are two key limitations associated with extant syntheses, relating to both scope and methodology. The first limitation is a focus on a limited range of countries [26]; specific diagnosable conditions (e.g. depression) [20, 21]; discrete population subgroups (e.g. foster care) [17, 20, 27]; or single intervention packages (e.g. Treatment Foster Care) [27, 28]. Where reviews are inclusive of diverse outcomes, populations and intervention types, they tend to take an aggregative approach when presenting syntheses. Notably, there is limited differentiation between the evidence for interventions that operate in different parts of the social system.
This differentiation is imperative, as there is suggestion that interventions can be ineffective due to an over-reliance on individual-level approaches that are minimally disruptive [29], and there is a need to understand the evidence for structural interventions to guide the development of system-level approaches moving forward. Equally, with the advance of complex systems thinking perspectives in intervention research, there is increased recognition that an intervention’s functioning is dependent on its interaction with proximal and distal system characteristics [30–34]. As such, interventions operating in different parts of the system may be subject to different contextual influences and implementation challenges. We need to disentangle these complex interactions to inform effective intervention delivery in future.
There are a number of organising frameworks to help locate interventions in different parts of the social system, including the socio-ecological model, with versions originating from child development and public health research [35, 36]. There are broadly five domains of factors that influence outcomes, and which may be targeted for intervention [35]. These are as follows: intrapersonal, which is an individual’s knowledge, attitude and behaviour; interpersonal, which is an individual’s relationships and social network systems, including family and friendship networks; organisational, which is the formal and informal rules, ethos and characteristics of social institutions; community, which is the relationship between organisations and networks; and policy, which includes local, regional and national laws and policies.
The second limitation with existing reviews is that they tend to restrict syntheses to outcome evaluations, with scant attention paid to interventions’ programme theory, the context of evaluation, the process of implementation, acceptability or cost-effectiveness. Even recent comprehensive NICE reviews [26], which do include a range of evidence types, do not provide a clear overview of programme theories or the contextual factors that give rise to reported barriers and facilitators to intervention functioning.
Integration of these different evidence types is important in understanding how interventions operate and generate effects within their delivery context, and their potential transportability to other health and social care systems. This integrated approach to evaluation, which draws on a range of evidence, is recommended by a range of methodological guidance on intervention development, adaptation and evaluation [37–40]. As such, an evidence map and review that systematically charts the range of interventions targeting the mental health of care-experienced children and young people, in addition to the types of evidence currently generated, is important in identifying where there may be limitations in current intervention research and where it needs to be further strengthened [41].
The Care-experienced cHildren and young people’s Interventions to improve Mental health and wEll-being outcomes Sytematic review (CHIMES) was a complex systems informed, multi-method review that aimed to synthesise international evidence on programme theory, process evaluation, outcome evaluation, equity harms, and economic evaluation [42]. For the first phase, reported presently, we constructed a map of interventions and associated evaluations to chart key evidence gaps and clusters. It addressed the following review questions:
What are the targeted socio-ecological domains, theories and outcomes addressed in mental health and wellbeing interventions for care-experienced children and young people?
What are the types of evidence generated as part of intervention evaluations?
In charting the available evidence on interventions and types of evidence, the map informed the scope and feasibility of the second phase of the systematic review. For example, the map identified sufficient randomised controlled trials to conduct meta-analysis for relevant outcomes. The second review phase involved method-level syntheses for outcome evaluations, process evaluations, equity harms and economic evaluations. These were then integrated into an overarching review-level synthesis, where data from one synthesis (e.g. process evaluation) supported explanation of another synthesis (e.g. outcome evaluation) [43]. The third and final phase of the review entailed stakeholder consultation to reflect on the synthesis and prioritise interventions for future development and/or adaptation, evaluation and implementation.
Methodology
We generated an evidence map, drawing on systematic mapping guidance [44]. Evidence maps have some conceptual overlap with scoping reviews, but with clearer emphasis on stakeholder involvement in the early stages of the research process, a systematic search strategy, and the visual presentation of data [41]. As there is no standardised methodology for the reporting of evidence maps, we describe the process with reference to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Extension for Scoping Reviews (PRISMA-ScR) [45]. The review is registered with the PROSPERO registry of systematic reviews (reference number CRD42020177478).
Stakeholder consultation
We integrated a comprehensive programme of stakeholder involvement throughout the CHIMES review. Regarding the evidence map, we consulted with three key groups of stakeholders at the outset to refine and confirm the focus and scope of the review. These groups were as follows: (1) CASCADE Voices (young people’s research advisory group with care-experienced individuals up to the age of 25 years); (2) The Fostering Network in Wales Young Person Forum (group of care-experienced young people who provide advice and guidance to the charity on their programmes of work); and (3) All Wales Fostering Team Managers Forum (group of Local Authority and independent foster care providers). The central priorities of these groups were to focus on wellbeing and suicide-related outcomes, and to map interventions according to a socio-ecological schema. This latter priority related to stakeholders’ perception of a lack of structural interventions at the organisational and policy level, and a need to establish if this is a significant evidence gap and how it might be addressed moving forward.
Eligibility criteria
The inclusion parameters for the review were defined according to the Population, Intervention, Comparator, Outcome and Study Design (PICOS) framework:
Types of participants
Intervention participants could be care-experienced children and young people ( 25 years old), or their proximal relationships, organisations and communities. Care could include in-home care and out-of-home care (foster care; residential care; and formal kinship care), and could be current or previous (e.g. care-leaver). The amount of time in care was not restricted. The following populations were excluded: general population; children and young people classified as being in need but not placed in care (e.g. having a Children in Need (CiN) plan or Child Protection plan); children and young people at the edge of care; care without statutory involvement; adoption; or unaccompanied asylum seekers and refugees.
Intervention
We defined interventions as an attempt to disrupt existing practices in any part of the social system (e.g. healthcare, social care, education, youth justice). They could operate across the following socio-ecological domains: intrapersonal; interpersonal; organisational; community; and policy. They could be mono-component or multi-component. There were no a priori criteria for implementation (i.e. delivery setting, delivery mode, delivery agent). Pharmacological interventions were excluded.
Comparator
For outcomes evaluations, a comparator had to be specified and could include: treatment as usual; other active treatment; or no specified treatment.
Outcomes
Interventions had to target one of three domains of primary outcomes: subjective wellbeing (in addition to life satisfaction and quality of life); mental, behavioural or neurodevelopmental disorders as specified by the International Classification of Disease (ICD)-11; and suicide-related outcomes (self-harm; suicidal ideation; suicide). Measurement could be dichotomous, categorical or continuous. Outcomes had to be obtained for the child or young person, but could be ascertained through clinical assessment, self-report or report by another informant. Excluded primary outcomes included substance misuse and eating disorders, which have some conceptual overlap with the eligible outcomes, but are large literatures that could form the basis of separate reviews. We mapped all secondary outcomes included in eligible study reports (e.g. physical wellbeing).
Study design
Different study designs were eligible according to the research question targeted. Study reports could describe an intervention’s programme theory; outcome evaluation (Randomised Contolled Trial (RCT) or non-randomised design); process evaluation that reported on context, implementation and/or acceptability (qualitative and quantitative design); and economic evaluation (cost-minimisation; cost-effectiveness; cost utility; or cost–benefit analysis).
Information sources and search strategy
We identified study reports from sixteen electronic bibliographic databases: Applied Social Sciences Index and Abstracts (ASSIA); British Education Index; Child Development & Adolescent Studies; CINAHL; Embase; Education Resources Information Center (ERIC); Cochrane Central Register of Controlled Trials; Cochrane Database of Systematic Reviews; Health Management Information Consortium (HMIC); International Bibliography of the Social Sciences; Medline; PsycINFO; Scopus; Social Policy & Practice; Sociological Abstracts; and Web of Science. We identified additional peer-reviewed studies and grey literature through searching websites of 22 relevant social and health care organisations. Searches were conducted May–June 2020 and updated April–May 2022. We contacted 32 subject experts and 17 third sector organisations for recommendations, particularly regarding grey literature and in progress studies. We screened relevant systematic reviews and conducted forward and backward citation tracking with included study reports. The search strategy was developed in Ovid Medline and adapted to the functionality of each platform (Supplement A). Searches were undertaken from 1990 to coincide with the ratification of the United Nations Convention on the Rights of the Child [46]. Study reports were restricted to higher-resource countries. They were not restricted by language.
Data selection
We uploaded retrieved citations to the Evidence for Policy and Practice Information and Coordinating (EPPI) Centre’s review software EPPI Reviewer version 4.0 for storage and management. Study titles were screened by one reviewer to identify clearly irrelevant retrievals, with irrelevant reports checked by a second reviewer. Title and abstracts were screened independently and in duplicate by two reviewers. Where there was a conflict on exclusion, the study report progressed to the next stage of screening. Full texts were screened independently and in duplicate with conflicts resolved through discussion or recourse to a third reviewer. An inclusion criteria proforma guided selection, which was tested and calibrated with a subset of retrievals. The same inclusion criteria were applied to study reports from databases and grey literature. Study quality or publication process (e.g. peer review) was not part of the inclusion criteria and was assessed as part of quality appraisal.
Data extraction
We coded eligible study reports for the evidence map according to country; publication date; intervention type; target population; intervention name; intervention characteristics; programme theory; evidence type; study design; and intervention outcome domains. Intervention characteristics were further coded in accordance with the Template for Intervention Description and Replication (TIDieR) Checklist for Intervention Development [47]. To support description of interventions, we extracted programme theory with a tool used in a previous systematic review [48]. Extraction domains were as follows: method or process for developing the theory; name of theory; discipline of theory; socio-ecological domain of theory; and description of theory.
Evidence map
Scoping review and systematic mapping methods supported the mapping of the evidence base [44, 49]. Following the coding of study reports, we constructed numerical and narrative summaries of intervention and evidence clusters and gaps, with accompanying infographics. For details on intervention characteristics, we produced a narrative summary and table describing the features according to extractable domains of the TIDieR framework. For interventions reporting on programme theory, we narratively summarised these according to the socio-ecological domains in which they operated and produced a summary table. For evidence types, we constructed a narrative summary and table.
Results
Study characteristics
A total of 15,068 unique study reports were identified. Of these, 888 were screened at full text, with 64 interventions being included that linked to 124 study reports (Fig. 1) [50–173].
Fig. 1.

PRISMA flow diagram
Study reports were published between 1994 and 2022. Interventions were from twelve countries: USA (n = 77); UK (n = 22); Netherlands (n = 6); Belgium (n = 3); Australia (n = 3); Portugal (n = 3); Canada (n = 2); Ireland (n = 2); Israel (n = 2); Germany (n = 1); Spain (n = 1); Sweden (n = 1); and both the USA and UK (n = 1).
Intervention types
We classified interventions according to the socio-ecological domain or domains targeted (Fig. 2). As indicated, this was due to our assumption that interventions will interact with context differentially if they target different parts of the social system. The classification of interventions by socio-ecological domain was informed by information about the causes being targeted and the reported theoretical basis. Where the theory was not specified, we also drew upon reported information on the target population (e.g. individuals in a relationship with the care-experienced child) and delivery setting (e.g. a social care organisation). While interventions within each group had a shared target set of causes and theories, there was diversity in terms of activities. An overview of intervention characteristics is presented in Table 1.
Fig. 2.

Intervention type by socio-ecological domain
Table 1.
Description of intervention characteristics (N = 64) [174]
| Intervention | Socio-ecological domain | Country | Participant group; Participant age |
Intervention duration | Delivery agent and setting | Intervention components |
|---|---|---|---|---|---|---|
| Acceptance and Commitment Therapy (ACT) [155] | Intrapersonal; Interpersonal | Sweden |
Children: Residential care Age: 16–18 years |
6 weeks |
Treatment assistants Residential care placement |
Group-based psychoeducational curriculum (2-h sessions) that include experiential exercises, role play and illustrations |
| Animal Associated Psychotherapy (AAP) [158] | Intrapersonal; Interpersonal | Spain |
Children: Residential care Age: Mean 15.17 years |
12 weeks |
Psychiatrists; Child psychologist Caserio (farm) |
Individual and small group sessions (32 sessions) over 2-day visits to a farm. Sessions involve spending time with dogs, horses and other farm animals |
| Attachment and Behavioural Catch-up (ABC) [143] | Interpersonal | USA |
Children: Foster care Age: 0–5 years Adults: Foster carers |
10 weeks |
Child psychologist; Psychiatric nurse; Social worker Foster care placement |
Manualised parenting programme and coaching sessions. Sessions video-taped to tailor content to specific needs of each carer-child dyad. Monthly family support group |
| Behavioural modification training; psychodynamic treatment; structured community living; adventurous learning [163] | Intrapersonal; Interpersonal | Netherlands |
Children: Residential care Age: Mean 14.9 years |
Not specified | Not specified for all interventions | Four models of treatment: behavioural management by online care workers; psychodynamic treatment; structured boundaries and relationships; and adventurous learning that models self-supportive, adaptive behaviours |
| Care placement type [150, 153, 157, 159] | Policy | Netherlands; USA |
Children: Foster care; Kinship care; Residential care Age: < 18 years |
Not specified |
Foster carers; Kinship carers; Residential carers Care placement |
Comparison of different types of care placement |
| Child Adult Relationship Enhancement [135, 167] | Interpersonal | USA |
Children: Foster care Age: 3–12 years Adults: Foster carers |
Not specified |
CARE trainer Not specified |
Trauma-informed parenting training (2 × 3 h) |
| Child and Adolescent Mental Health Services (CAMHS) [80] | Community | UK | Children: Foster care; Residential care | Not specified |
Local authority staff; Mental health workers; Psychologists; Psychiatrists Community mental health services |
Development of a single referral pathway to improve access and effective engagement with children and young people, through joint professional forums, partnership working and training |
| Child-Directed Interaction Training (CDIT) [138] | Interpersonal | USA |
Children: Kinship care Age: 2–7 years old Adults: Kinship carers |
4 weeks |
Graduate students Neighbourhood resource centre |
Group-based coaching of carers (twice weekly) |
| Children and Residential Experiences (CARE) [73, 151] | Organisational | USA |
Children: Residential care Age: 7–18 years Adults: Residential carers; Social care/health care professionals |
3 years |
Care Consultants; CARE Implementation Team (CIT) Residential care setting |
Consultation, training and technical assistance to residential placements to create a therapeutic environment through policies and practices |
| Cognitive and Affective Bibliotherapy [123] | Intrapersonal | Israel |
Children: Residential care Age: 6–15 years |
Not specified |
Trained bibliotherapists Residential care placement |
Eight small group sessions (45 min) to explore eight texts. Discussion of the texts serves as a departure point for discussing emotions |
| Cognitively-Based Compassion Training (CBCT) [96] | Intrapersonal | USA |
Children: Foster care Age:13–17 years |
6 weeks | Not specified | Cognitive training programme (1 h twice per week) |
| Computer game [74] | Intrapersonal | UK |
Children: Residential care Age: 12–17 years |
6–18 months |
Social worker Online |
Online game (6 × 1-h sessions) including SIMS Life Stories (or ‘electronic dolls house’) and emotional regulation skills coaching by a social worker |
| Connect-KP [117] | Interpersonal | Australia |
Children: Kinship care Age: 8–16 years Adults: Kinship carers |
9 weeks |
Psychologists; Clinical psychologists; Social workers Community settings |
Support group sessions (weekly) to develop trauma-informed parenting and explore challenges of kinship care |
| Dojo: Biofeedback videogame [97] | Intrapersonal | Netherlands |
Children: Residential care Age: Mean 13.67 |
4 weeks |
Researcher; Research assistant Online |
Online game (30-min sessions twice weekly) with tutorials and emotion-evoking mini-games. Tutorials teach CBT relaxation techniques and positive thinking |
| Early Intervention Foster Care (EIFC) [56] | Intrapersonal; Interpersonal | USA |
Children: Foster care Age: < 6 years Adults: Biological parents; Foster carers |
6–9 months |
Clinician; Foster carer; Psychiatrist; Psychologist Care placement; School; Day care; Telephone |
Before receiving a child, foster carers complete intensive training. After placement, carers are given support thorough daily contact with foster carer consultant, weekly support group meeting and 24-h on call crisis intervention. Children receive services from behavioural specialist and weekly therapeutic playgroup sessions |
| Enhanced Foster Care Treatment [152] | Interpersonal | USA |
Children: Foster care Age: 14–18 years Adults: Foster carers |
Not specified |
Not specified Foster care placement |
Increased financial resource for foster carers and access to educational support |
| Equine-Facilitated Psychotherapy (EFP) [50] | Intrapersonal; Interpersonal | Israel |
Children: Residential care Age: 14–18 years |
7 months |
Treatment facility staff Treatment facility |
Psychotherapy with horses (50 min sessions weekly) to provide a healing experience and develop interpersonal adaptation skills |
| Evolve Behaviour Support Services (EBSS) [107] | Interpersonal; Organisational; Community | Australia |
Children: Out-of-home care; Adults: Biological families; Out-of-home carers; Social care/health care professionals |
Not specified |
Child Safety Officers; Clinicians Not specified |
Holistic and flexible positive behaviour support for children and young people with disabilities, including: child-focused therapy; carer education and training; and environmental strategies. Collaborative working with a range of stakeholders to ensure coordinated, integrated and targeted service delivery |
| Family Finding [110, 146, 154] | Interpersonal | USA |
Children: Foster care Age: 6–17 years Adults: Biological parents; Other family members |
40 days |
Independent professional; Child’s case worker Not specified |
Approach for searching for, discovering and engaging actual and fictive kin to support attachment and permanency needs |
| Family Minds [120] | Interpersonal | USA | Adults: Foster carers | 6 weeks |
Study author Online |
Group-based curricula (3 classes of 3 h each) to increase carers’ reflective functioning and mentalisation skills |
| Foster carer and foster children group-based intervention [142] | Interpersonal | USA |
Children: Foster care Age: Mean 11.54 years Adults: Foster carers |
12 months | Trained foster carers; Graduate students; Undergraduate students | Group-based programme (6 sessions, twice weekly over 3 weeks), with one group for girls and one for foster carers. Follow-up training and support provided (2 h once per week) on individual basis for girls and group basis for carers for subsequent school year |
| Foster carer training [136] | Interpersonal | UK |
Children: Foster care Age: 5–16 years Adults: Foster carers |
1 week |
Social workers Not specified |
Training sessions (6 h per day for 3 days) including didactive material, group material and homework tasks to improve carers communication and attachment |
| Foster carer training [61] | Interpersonal | UK | Adults: Foster carers | 3 days |
Clinical psychologist Not specified |
Pre-training materials and in-person group training on managing challenging behaviour, with follow-up to discuss progress |
| Foster parent training [67, 68] | Interpersonal | Belgium | Adults: Foster carers | 10 weeks |
Trained specialist foster carers Foster care placement |
Weekly home visits to deliver a curriculum that includes psychoeducation, practice of emotions and communication skills. Homework tasks of daily 10-min play activity. Group sessions to provide peer support |
| Fostering Changes [88, 137] | Interpersonal | UK |
Adults: Biological parents; Foster carers |
12 weeks |
Trained facilitators Not specified |
Group-based training (3 h weekly) with support group to reinforce learning |
| Fostering Connections [92, 156] | Interpersonal | Ireland | Adults: Foster carers | 6 weeks |
Trainer practitioners Community setting |
Trauma-informed psychoeducational programme (3.5 h weekly). Content includes experiential exercises, videos, role play, discussion and at home exercises. Carers receive a toolkit and homework book |
| Fostering Healthy Futures (FHF) [64–66, 69, 70, 101, 144] | Intrapersonal; Interpersonal | USA |
Children: Out-of-home care Age: 9–11 years |
30 weeks |
Facilitators; Masters-level social workers Not specified |
Group-based manualised curricula (1.5 h weekly) and one-to-one mentoring to model positive social relationships |
| Fostering Individualised Assistance programme (FIAP) [125] | Intrapersonal; Organisational; Community | USA |
Children: Foster care Age: 7–15 years Adults: Biological parents; Foster carers; Social care/health care professionals |
Not specified |
FIAP family specialists Foster care placement; Community settings; School |
Specialist acts as a family-centred, clinical case manager and home-based counsellor. Provide strength-based assessment, life domain planning, clinical case management, and tailoring of services |
| Glasgow Infant Family Team (GIFT); London Infant Family Team (LIFT); New Orleans Model [103, 175] | Interpersonal; Organisational; Community | UK |
Children: Foster care; Kinship care Age: 0–5 years Adults: Biological parents; Foster carers; Kinship carers; Social care/health care professionals |
12 weeks |
Psychiatrists; Psychologists; Social workers; Family liaison workers Not specified |
Referrals made to multi-disciplinary team who engage in series of interviews, observations and questionnaires to assess family functioning (biological family) and parental mental health to make placement decision. Social work team meets with family (2 h per meeting for eight meetings) over 3 months |
| Head, Heart, Hands [93] | Interpersonal; Organisational | UK | Adults: Foster carers; Social care / health care professionals | Not specified |
Social pedagogues Foster care system |
One-day taster session, 2-day orientation course, 8-day core course and follow-on group to support introduction of social pedagogic learning |
| Head Start [131] | Community | USA |
Children: In and out-of-home care Age: 3–4 years Adults: In and out-of-home carers |
12 months |
Community service providers Community services |
Wraparound community services and support, including early learning in vocabulary and early literacy, maths skills, and behavioural and emotional problems |
| HealthRHYTHMS [124] | Intrapersonal; Interpersonal | USA |
Children: Residential care Age: 12–18 |
6 weeks |
Trained facilitator; Counsellor Not specified |
Group sessions (1 h weekly) including self-expression with a drum, before progressing to verbal and written communication. Combined with tactile conditioning, where young people have a crystal to heighten emotional awareness |
| Herts and Mind: Mentalization-Based Therapy [94] | Interpersonal | UK |
Children: Foster care Age: 5–11 years Adults: Foster carers |
12 weeks |
CAMHS Targeted Team Not specified |
Short manualised treatment including a combination of psychoeducation about attachment and mentalising in children with histories of maltreatment; consultations with professionals; and relational work |
| Incredible Years [60, 82, 84, 87, 98] | Interpersonal | Portugal; UK; USA |
Children: Foster care; Kinship care; Residential care Age: 2–12 years Adults: Biological parents; Foster carers; Kinship carers; Residential carers |
12–18 weeks |
Experienced foster carers; Social workers Care placement; Community settings |
Parenting group (2–2.5 h sessions). One-to one home visit programme to reinforce skills learnt during sessions |
| Individual therapy and rehabilitative strategies [160] | Intrapersonal | USA | Children: Foster care | Not specified. Data availability for 3 years |
Counsellors and therapeutic specialists Foster care placement; Therapeutic setting |
Individual therapy: Varying types of therapy with mental health provider offering at home sessions 2–5 times per week Therapeutic behavioural services: Treatment services between a child and mental health provider 2–5 times per week |
| Intensive Permanence Systems (IPS) [86] | Interpersonal; Organisational | USA |
Children: Foster care Adults: ‘Supportive connections’ |
24 months |
IPS experienced staff Not specified |
Family search and engagement strategies to create a supportive network for youth to help on the path to permanency |
| kContact [169] | Interpersonal | Australia |
Children: Foster care Age: 0–14 years Adults: Biological parents |
9 months |
Caseworkers Telephone |
Four phases of support for biological parents to plan for, reflection upon and review goals for contact with child |
|
Keeping Foster and Kinship Parents Supported and Trained(KEEP) |
Interpersonal; Organisational; Community | USA |
Children: Foster care; Kinship care Age:4–16 years Adults: Foster carers; Kinship carers; Social care/health care professionals |
16 weeks |
Trained facilitators Care placement; Community settings |
Parenting group (90 min weekly), home practice activities and weekly check in phone calls. Different community implementation models to integrate into child welfare system |
| Kids in Transition to Schools (KITS) [148] | Intrapersonal; Interpersonal | USA |
Children: In and out-of-home care Age: 4–6 years |
7 weeks |
Not specified Care placement; School |
Therapeutic playgroups (2 h, twice weekly) to learn and practice the social and self-regulatory requirements of school |
| Kundalini Yoga [105] | Intrapersonal | UK |
Children: Residential care Age: Mean 14.78 years Adults: Residential staff |
20 weeks |
Not specified Residential care placement |
Yoga classes (44–60-min sessions) teaching posture, breathing and meditation |
| Life Story [85] | Intrapersonal; Interpersonal | USA |
Children: Foster care Age: 7–15 years |
7 months |
Teachers; Child welfare professionals; Counsellors Foster care placement |
Meeting once per week to construct a culturally sensitive narrative of personal experience, where the professional challenges assumptions about substance use |
| Mentoring intervention for teenage pregnancy [59] | Interpersonal | UK |
Children: In and out-of-home care Age: 5–16 years |
1 year |
Peer mentors Range of settings |
Peer mentoring sessions with trained peers. Engaged in a range of activities, and communication via email, face-to-face, telephone and text |
| Mindfulness [89] | Intrapersonal | USA |
Children: Foster care; Kinship care Age: 14–21 years |
10 weeks |
Psychologist; Research Assistant Health clinic |
Mindfulness curriculum (2-h sessions) with guest speakers, crafts, yoga, music and socialising |
|
Multidimensional Treatment Foster Care (MTFC); Multidimensional Treatment Foster Care-Adolescents (MTFC-A); Multidimensional Treatment Foster Care-Pre-schoolers (MTFC-P) |
Interpersonal; Organisational; Community; | Netherlands; UK; USA |
Children: Foster care; Kinship care; Residential care Age: 3–17 years Adults: Foster carers; Social care/health care professionals |
Approx. 2 years |
Foster carers; Clinicians; Therapists; Programme supervisors; Skills workers; Education workers Care placement; Community settings |
Specialist, supported foster carers with expertise in behaviour management. Range of wraparound services, including clinical and educational provision. Different community implementation models to integrate into child welfare system |
| Nonviolent Resistance (NVR) Training [145] | Interpersonal | Belgium |
Children: Foster care Age: Mean 11.6 years Adults: Foster carers |
10 weeks |
Foster care workers Foster care placement |
Training programme (75 min sessions per week) with telephone support between every two sessions, a workbook, handout and DVD, |
| Opportunities Box [164] | Intrapersonal | Portugal |
Children: Foster care Age: 14–17 years |
6 weeks |
Psychologist Not specified |
Sessions (90 min) on career ability, adaptability and decision-making |
| Outpatient mental health services [147] | Community | USA | Children: Foster care | Not specified |
Outpatient mental health service providers Outpatient mental health services |
Access and availability to outpatient mental health services, including drug and alcohol clinics, community health centres, crisis centres and private professional treatment |
| Parent–Child Interaction Therapy (PCIT) [77, 134, 165, 172] | Interpersonal | USA |
Children: Foster care Age: 2–7 years Adults: Biological parents; Foster carers |
14 weeks |
Clinician; PCIT graduate student Outpatient setting; Telephone |
Parent management training (2/3 full days and weekly phone consultation) with two stages: Child-Directed interaction (CDI) to promote parent–child bonding; and Parent-Directed Interaction (PDI) to enhance parent management |
|
Parent Management Training (PMT); Parent Management Training Oregon Model (PMTO) |
Interpersonal | Netherlands; USA |
Children: Foster care; Kinship care Age: 3–16 years Adults: Biological parents; Foster carers; Kinship carers |
16 weeks |
Trained facilitators Community setting; Care placement |
Group programme (90 min 1–2 time weekly) and home visit supervision in behaviour management. Combined with home practice assignments |
| Pathways Home [54] | Interpersonal | USA |
Children: Foster care Age: 5–12 years Adults: Biological parents |
32 weeks |
Trained consultants Not specified |
Parenting curriculum to prevent reunification failure by supporting development of a safe and nurturing environment. Booster sessions to fine-tune skills |
| Promoting First Relationships [139] | Interpersonal | USA |
Children: Foster care Age: 10–24 months Adults: Biological parents |
10 weeks |
Community mental health agencies Biological parent home |
Brief manualised sessions (60–75 min weekly) with video feedback, worksheets and handouts |
| Psychosocial rehabilitation [166] | Intrapersonal; Interpersonal | USA |
Children: Foster care Age: 3–18 years |
12–24 months |
Children’s psychosocial rehabilitation specialists Foster care placement |
Home support offering individualised family-focused and child-centred treatment (4–8 h per week), in addition to specialist support to relevant adults (2 h per week) |
| Sanctuary Model [162] | Intrapersonal | USA |
Children: Residential care Age: 12–20 years |
12 weeks |
Residential care staff Residential care placement |
Psychoeducational curriculum. Technical assistance from residential care staff. Twice daily community meetings |
| Solution Focused Parenting Group (SFPG) [102] | Interpersonal | Canada |
Children: Foster care Adults: Foster carers |
6 weeks |
Facilitator Not specified |
Parenting group (90 min weekly) focusing on identifying parenting solutions, homework to practice skills, and feedback |
| SuppOrting Looked after children In Decreasing Drugs, and alcohol (SOLID) [72, 108, 109] | Intrapersonal; Interpersonal | UK |
Children: Foster care; Kinship care; Residential care Age: 12–20 years |
35 days |
Motivational interviewing practitioner; Counsellor Care placement |
Two behaviour change interventions: Motivational enhancement therapy: Client-centred counselling (6 sessions) with problem feedback component to reflect on impact of drug and alcohol use Social behaviour and network therapy: Behavioural and cognitive strategies to help build social networks that are supportive of positive behaviour change in relation to problem substance use and goal attainment |
| TAKE CHARGE [113] | Intrapersonal; Interpersonal | USA |
Children: Foster care Age: 14–17 years |
12 months |
Coaches; Peers; Foster care alumni Not specified |
Coaching (50 h) in self-determination and goal achievement. Three mentoring sessions with intervention peers and foster care alumni |
| Teach Your Children Well (TYCW) [133] | Intrapersonal; Interpersonal | Canada |
Children: Foster care Age: Not specified |
30 weeks |
Researchers; Foster carers Foster care placement |
Individual tutoring (3-h sessions) including tutoring in reading, reading aloud to foster carer or other adult, and self-paced supervised maths instruction |
| Therapeutic Mentoring [171] | Interpersonal | USA |
Children: Foster care Age:6–15 years |
6–9 months |
Clinician Not specified |
Therapeutic mentoring relationship (4–5 h, weekly) involving pre-planned activities within the mentor–mentee relationship |
| Trauma-Focused Cognitive Behavioural Therapy (TF-CBT) and evidence-based engagement strategies [83, 112] | Intrapersonal; Interpersonal | USA |
Children: Foster care Age:6–15 years Adults: Foster carers; Kinship carers |
Not specified |
Clinician; Counsellors; Social workers Not specified for TF-CBT; Telephone and foster care placement for engagement strategies |
Sessions (12–20 sessions) with child, carer and child-carer, focusing on parenting, psychoeducation and trauma. Supplementary engagement component, with contact between clinician and family via telephone, in person or both to address participation barriers |
| Trauma Systems Therapy (TST) [115] | Community | USA |
Children: In and out-of-home care Age: Mean 11.98 years Adults: Social care/health care professionals |
3 years | Not specified | Social care system-wide trauma-informed model of clinical provision and service coordination. Informs decision-making for treatment, training for staff, and system culture |
| Treatment Foster Care (TFC); Treatment Foster Care (TFC) for Older Youth; Together Facing the Challenge (TFTC) [55, 57, 63, 91, 95, 127, 176] | Interpersonal; Organisational; Community | USA |
Children: Foster care Age: < 18 years Adults: Foster carers; Social care/health care professionals |
Approx. 12 months |
Key staff; Life coach; Psychiatric nurse Care placement; Clinician settings; Community settings |
Parenting programme (approx. 2.5 h weekly) including role play and didactic instruction. Range of wraparound services that includes psychiatric support, life skills development, life coaching in education and employment |
| Triple P for Foster Carers (TPFC) [111] | Interpersonal | Germany | Children: Foster care Adults: Foster carers | 5 weeks |
Triple P facilitators Community settings |
Manualised parenting group (2.5 h weekly), two 20-min telephone consultations and a closure session |
| Wave by Wave [168] | Intrapersonal; Interpersonal | Portugal |
Children: Residential care Age: 10–16 years |
6 months |
Psychologists; Surf instructors Carcavelos beach, Portugal |
Psychoeducation activities and surf classes (3 h weekly sessions) |
| Youth-Initiated Mentoring (YIM) Relationships [99] | Interpersonal | USA |
Children: Foster care Age: 16–25 years |
12 months |
Mentor from social services, school, church, family or former foster carer Not specified |
Youth nominated mentor meets with young person (1 per month) to provide informational, companionship, emotional, appraisal and instrumental support |
The majority of interventions (n = 26) targeted the interpersonal domain. They primarily focused on the skills, knowledge and confidence of foster and kinship carers through training curricula and professional-delivered support. A small number of interventions promoted children and young people’s positive relationships with biological families, largely with the aim of facilitating reunification [54, 139, 169]. Elsewhere interventions provided opportunities to build relationships with peers [59, 142], trained mentors [99], clinicians [171] and wider social networks [72]. Where details on duration of delivery was specified, most interventions were delivered for 1 to 6 months (n = 17). Seven were delivered between 7 and 12 months.
Nine interventions targeted the intrapersonal domain, directly supporting care-experienced children and young people. Approaches included delivery of Cognitive and Affective Bibliotherapy [123], Cognitively-Based Compassion Training (CBCT) [96], Cognitive Behavioural Therapy (CBT) [74, 97] and mindfulness and yoga practices [89, 105]. These were delivered through a range of online and virtual modalities, including online tutorials and computer games [74, 97]. Where specified, interventions were primarily delivered over the course of 1 to 6 months, with only one intervention being delivered for a longer duration than 6 months [74].
A further fifteen interventions operated across the intrapersonal and interpersonal domains, combining both relationship-based components with skill and competency training for children and young people. For example, Fostering Healthy Futures (FHF) provided group-based curricula and mentoring by a trainee social worker [66]. Group-based activities could include creative or leisure tasks, such as drumming [124] or surfing [168]. For some of these interventions, relationships were fostered through animal-facilitated psychotherapy [158], specifically equine therapy [50]. Five interventions were delivered between 1 and 6 months, seven were delivered between 7 and 12 months and one was delivered between 13 and 24 months.
A further eight interventions primarily included intrapersonal and interpersonal targeting activities, but had a range of organisational- and community-based support to reinforce change mechanisms, support linkage to other interventions and optimise delivery. This included Keeping Foster and Kinship Parents Supported and Trained (KEEP) [53, 62, 71, 79, 81, 106, 140, 141, 149, 161], Multidimensional Treatment Foster Care (MTFC) [51–53, 58, 76, 78, 90, 128, 129] and Treatment Foster Care (TFC) [55, 57, 63, 91, 95, 119, 127, 176]. This group of interventions were delivered up to 6 months (n = 2), 7–12 months (n = 1), 13–24 months (n = 2), or delivery duration was not specified (n = 3).
There were a limited number of structural-level interventions: one had a focus on organisational culture and ethos [73, 151]; four considered the availability of community mental health and wellbeing provision [80, 115, 131, 147]; and one policy-level approach targeted the re-prioritisation and funding of placement types [150, 153, 157, 159]. Generally, the delivery duration of these interventions were not specified, although one was delivered for 12 months [131] and two for 3 years [73, 115, 151].
Programme theories
A subset of 13 interventions, with 24 study reports, included a clearly articulated programme theory (Table 2). These mapped onto three dimensions of programme theory: theories of change that explain the causal mechanisms through which an intervention is intended to bring about change; theories of implementation, which prescribe how an intervention will operationalise proposed change mechanisms; and context theories, which consider how system features interact with and are modified by the change mechanisms [177, 178].
Table 2.
Overview of intervention programme theory (N = 13 interventions)
| Socio-ecological domain of theory | Intervention | Description of theory | Specified theories |
|---|---|---|---|
| Intrapersonal | Equine-facilitated Psychotherapy [50] | Physical and mental development: Horse’s rhythm and riding linked with the mental and physical developmental process | None |
| Interpersonal | Therapeutic alliance: Relationship with horse provides healing experience. Important for building trust with ‘other’ and establishing interpersonal skills | Therapeutic alliance | |
| Intrapersonal | Fostering Healthy Futures [64–66, 69, 70] |
Positive Youth Development: Need to develop prosocial, behavioural and emotional skills Resilience theory: Promote adaptive functioning to increase resiliency |
Attachment; Positive Youth Development; Resilience; Social Learning Theory |
| Interpersonal |
Attachment: Challenging relationship histories can reduce mentoring responsiveness Positive Youth Development: Need to develop prosocial relationships as a template for future relationships Resilience theory: Promotes adaptive functioning Social Learning Theory: Importance of modelling to develop prosocial relationships |
||
| Intrapersonal |
SuppOrting Looked after children In Decreasing Drugs, and alcohol (SOLID) [72] |
Motivational interviewing: Behavioural and cognitive strategies to support change and remove ambivalence towards substance use | Motivational interviewing |
| Interpersonal | Social network support: Important in supporting young people to deal with problem behaviours and attain goals | None | |
| Interpersonal | Early Intervention Foster Care (EIFC) [56] | Delayed maturation: Challenges of children due to delayed maturation. Intervention provides optimal environment to facilitate developmental progress | None |
| Interpersonal | Foster carer training [61] | Behavioural management skills: Parent management training informed by a constructive rather than pathological approach to operant conditioning, which theorises that behaviour can be learned through a system of reward and punishment | Operant conditioning |
| Interpersonal | Foster parent training [67, 68] |
Attachment Theory: Care-experienced young people develop mistrust and insecurity because of absent biological caregiver Social Learning Theory: Background context theory referenced but not explained |
Attachment; Social Learning Theory |
| Interpersonal | Incredible Years [60] | Social Learning Theory: Requirement to alter negative parenting behaviours (e.g. shouting or physical behaviours) modelled to children | Social Learning Theory |
| Interpersonal | Mentoring intervention for teenage pregnancy [59] |
Attachment: Need for positive and responsive attachments between the child and caregiver (or mentor and mentee) Social Learning Theory: Behaviours learned through the modelling and observation of others |
Attachment; Social Learning Theory |
| Interpersonal | Pathways Home [54] | Encouragement-based parenting: Need to develop parenting practices based on encouragement | None |
| Interpersonal | Keeping Foster Carers Trained and Supported (KEEP) [53, 62, 71] | Social Learning Theory: Background context theory referenced but not explained | Social Learning Theory |
| Organisational/ Community | Generic System Change: Cascading dissemination model to support local system capacity | ||
| Interpersonal |
Multidimensional Treatment Foster Care (MTFC) |
Coercion theory: Need to prevent negative and coercive interactions between child and their carer and/or peers Resilience: Focus on positive, asset-based development Social Learning Theory/Positive Youth Development: Background context theory referenced but not explained Trauma-focused cognitive behavioural therapy: Carers need to understand and respond to causes of trauma |
Coercion Theory; Resilience; Social Learning Theory; Positive Youth Development; Trauma- focused Cognitive Behavioural Therapy |
| Organisational/ Community | Generic system change: Rolling cohort model that commences with learning from small-scale implementation and then applied to wider system | None | |
| Interpersonal |
Treatment Foster Care (TFC) [57, 63] / Together Facing the Challenge (TFTC) [55] |
Role enactment: Encourages carer affiliation with role of parent to support adherence with delivery Trauma-focused Cognitive Behavioural Therapy: Carers need to understand and respond to causes of trauma Therapeutic alliance: Relationships between the treatment parent and child is therapeutic and the therapeutic relationship provides an environment for positive change Ecological Context Model: Intervention nested within larger supra-system of influence that impacts effectiveness: foster carer skills and parenting; contact with biological parents; and relationship with peer group |
Trauma-focused Cognitive Behavioural Therapy; Therapeutic Alliance; Ecological Context Model |
| Organisational/ Community | Ecological Context Model: Intervention nested within larger supra-system: lack of educational resources, integration and continuity; delivery agency structure and professionals; funding and access to social services; and young people’s integration into community | ||
| Organisational | Children and Residential Experiences (CARE) [73] | Generic system change: Need to transform organisational ethos and culture to create alignment with attachment / relationship-based approach | Attachment; Ainsworth Maternal Sensitivity |
Theories of change targeted different socio-ecological domains. Three interventions focused on intrapersonal theories [50, 64–66, 69, 70, 72]. Key theoretical approaches within this domain linked to Positive Youth Development [179] and resilience, emphasising the need for young people’s adaptive functioning and self-development so that they can enter prosocial relationships [64, 66, 69].
The majority of interventions foregrounded interpersonal theories of change (n = 12), which mapped onto three sets of causal mechanisms. First was to build a therapeutic environment that could be supportive of positive development and prosocial relationships [50, 56, 63]. Second was to develop parent and carers skills, knowledge and confidence, primarily through parenting curricula [51–58, 60–62, 67, 68]. Theories included Bowlby’s attachment theory [180], Social Learning Theory [181], Positive Youth Development [179] and resilience, which together emphasise the significance of positive attachments that provide opportunities for learning prosocial behaviours observationally through modelling and replication. Some interventions also re-orientated parenting practices according to coercion and operant conditioning, which encourage effective management of negative behaviour through positive reinforcement and non-harsh disciplinary methods [51, 52, 61]. Third, was to develop mentoring relationships [59, 64–66, 69, 101]. These also operated through attachment theory, Social Learning Theory [181] and Positive Youth Development [179].
One intervention included a theory that operated within the organisational domain [73]. The focus was on the transformation of organisational culture within the social care system to ensure its conduciveness with an attachment-based and trauma-informed ethos.
There was more limited inclusion of implementation and context theories. Two interventions operating across the interpersonal, organisation and community domains, focused on optimising delivery in a range of contexts [53, 58, 62, 73]. This included testing a ‘train the trainer’ approach and a structured scale-up model, where the learning from early implementation informed later delivery. We termed these implementation theories as ‘general system change’. One intervention included a context theory, mapping the wider system factors that could inhibit the functioning of an intervention’s parenting curricula. The study report termed this an ‘ecological context model’ [57].
Intervention outcomes
We mapped intervention outcomes according to the a priori outcomes specified by the review (Fig. 3). Outcomes were either theorised (e.g. study reports with theoretical descriptions) or empirically assessed (e.g. study reports with outcome evaluations).
Fig. 3.
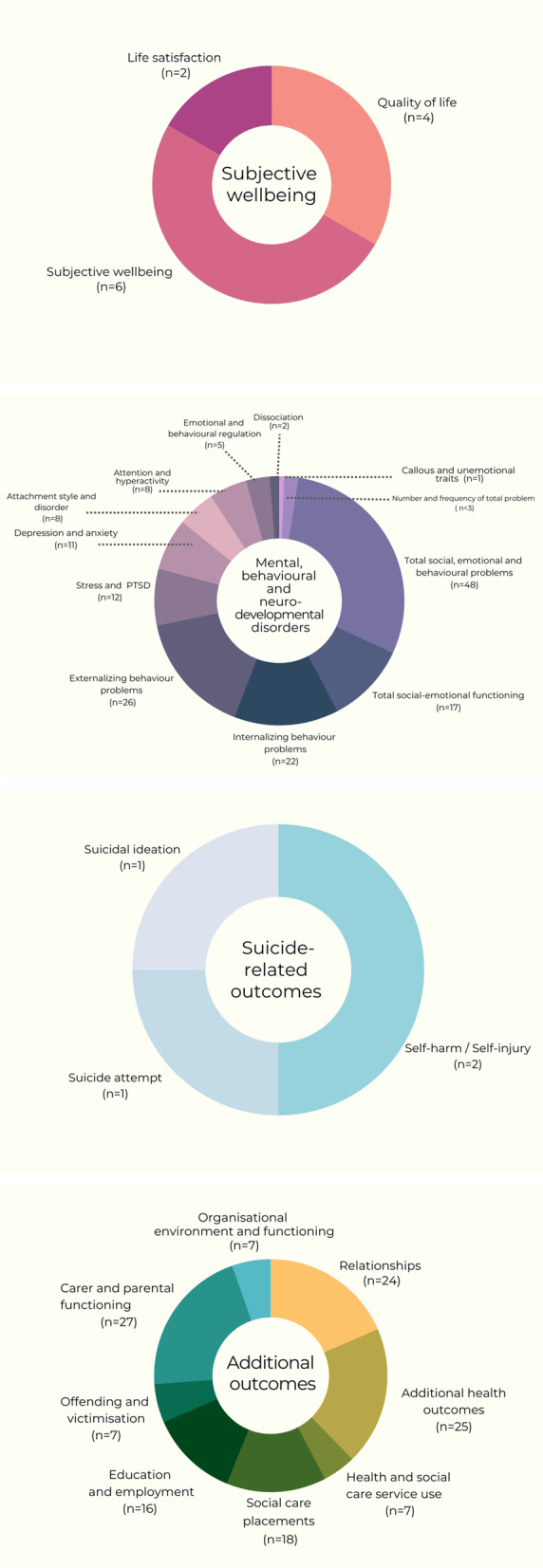
Intervention primary and additional outcome domains
Most interventions targeted mental, behavioural and neurodevelopmental disorders. Within this domain, interventions most frequently assessed outcome measurements of total social, emotional and behavioural problems (n = 48); socio-emotional functioning difficulties (n = 17); internalising problem behaviours (n = 22); and externalising problem behaviours (n = 26). There was a paucity of interventions that targeted subjective wellbeing (n = 11). Only four interventions targeted suicide-related outcomes, including suicidal ideation [124], self-harm [96, 151] and suicide attempt [59].
We inductively classified additional outcomes measured by evaluations. These were primarily child-level outcomes: relationships; additional health outcomes; health and social care service use; social care placements; education and employment; and offending and victimisation.
We classified fourteen study reports, linked to eight interventions, that considered potential equity harms in relation to intervention outcomes [54, 65, 69–71, 101, 122, 126, 130, 133, 140, 142, 170, 182]. Reported equity harms focused on children and young people’s personal characteristics (age; gender; ethnicity; baseline mental health status) and personal relationships (exposure to maltreatment; placement type; quality of relationship with caregiver; number of caregivers). Parent and carer-related equity harms were linked to personal characteristics (age; ethnicity; baseline mental health status; and drug and alcohol use) and personal relationships (relationship status).
Evidence types
We categorised study reports according to the type of evidence reported (Fig. 4). The evidence type linked to each intervention is further presented in Table 3. Twenty-four study reports described a programme theory [50–73]. Fifty process evaluations provided data on context, implementation and acceptability. Of these, we defined 27 as conceptually and/or empirically ‘thin’, whereby they provided limited description of intervention implementation and acceptability [60, 68, 77–79, 81, 82, 84, 85, 87, 89, 91, 94, 96–98, 101, 102, 106, 111–115, 117, 118, 183]. Meanwhile, 23 were considered conceptually and/or empirically ‘rich’, presenting detailed data and analysis of contextual characteristics that might structure intervention functioning through their influence on implementation and acceptability [72, 74, 80, 83, 86, 93, 95, 99, 100, 103–105, 107–110, 116, 119, 175, 182, 184–186]. This set of rich process evaluations had theoretical generalisability beyond the immediate evaluation context.
Fig. 4.

Cumulative rate of report and evidence type
Table 3.
Overview of intervention evidence types
| Intervention | Country | Theory | Process | Outcome | |
|---|---|---|---|---|---|
| RCT | Non-randomised | ||||
| Acceptance and Commitment Therapy (ACT) | Sweden | Livheim, Tengström, et al. (2020) [155] | |||
| Animal Associated Psychotherapy (AAP) | Spain | Muela, Balluerka, et al. (2017) [158] | |||
| Attachment and Behavioural Catch-up (ABC) | USA |
Dozier, Peloso, et al. (2006) [126]; Sprang (2009) [143] |
|||
| Behavioural modification training; psychodynamic treatment; structured community living; adventurous learning | Netherlands | Scholte, Van der Ploeg, et al. (2006) [163] | |||
| Care placement type | Netherlands; USA |
Hayduk (2017) [150]; Leloux-Opmeer, Kuiper, et al. (2018) [153]; McCrae, Lee, et al. (2010) [157]; Portwood, Boyd, et al. (2018) [159] |
|||
| Child Adult Relationship Enhancement | USA | Messer, Greiner, et al. (2018) [135] | Wood, Dougherty, et al. (2019) [167] | ||
| Child and Adolescent Mental Health Services (CAMHS) | UK | Callaghan, Young, et al. (2003) [80] | |||
| Child-Directed Interaction Training (CDIT) | USA | N’Zi, Stevens, et al. (2016) [138] | |||
| Children and Residential Experiences (CARE) | USA | Izzo (2020) [73] |
Izzo, Smith, et al. (2016) [151] Izzo (2020) [73] |
||
| Cognitive and Affective Bibliotherapy | Israel |
Betzalel, Schechtman (2010) [123] |
|||
| Cognitively-Based Compassion Training (CBCT) | USA | Reddy, Negi, et al. (2013) [96] | Reddy, Negi, et al. (2013) [96] | ||
| Computer game | UK | Aventin, Houston, et al. (2014) [74] | |||
| Connect-KP | Australia |
Pasalich, Moretti, et al. (2021) [117] |
Pasalich, Moretti, et al. (2021) [117] |
||
| Dojo: Biofeedback videogame | Netherlands | Schuurmans, Nijhof, et al. (2018) [97] | Schuurmans, Nijhof, et al. (2018) [97] | ||
| Early Intervention Foster Care (EIFC) | USA | Fisher, Ellis, et al. (1999) [56] | |||
| Enhanced Foster Care Treatment | USA | Kessler, Pecora, et al. (2008) [152] | |||
| Equine-Facilitated Psychotherapy (EFP) | Israel | Bachi, Terkel, et al. (2012) [50] | Bachi, Terkel, et al. (2012) [50] | ||
| Evolve Behaviour Support Services (EBSS) | Australia | Ziviani, Darlington, et al. (2013) [107] | |||
| Family Finding | USA | Shklarski (2020) [110] | Vandivere, Malm, et al. (2017) [146] | Leon, Saucedo, et al. (2016) [154] | |
| Family Minds | USA |
Adkins, Reisz, et al (2021) [120] |
|||
| Foster carer and foster children group-based intervention | USA | Smith, Leve, et al. (2011) [142] | |||
| Foster carer training | UK | Minnis, Pelosi, et al. (2001) [136] | |||
| Foster carer training | UK | Pithouse, Hill-Tout, et al. (2002) [61] | Pithouse, Hill-Tout, et al. (2002) [61] | ||
| Foster parent training | Belgium |
Van-Holen, Vanschoonlandt, et al. (2016) [67]; Vanschoonlandt, Vanderfaeillie, et al. (2012) [68] |
Vanschoonlandt, Vanderfaeillie, et al. (2012) [68] | Van-Holen, Vanschoonlandt, et al. (2016) [67] | Vanschoonlandt, Vanderfaeillie, et al. (2012) [68] |
| Fostering Changes | UK | Briskman, Castle, et al. (2012) [88] |
Briskman, Castle, et al. (2012) [88]; Moody, Coulman, et al. (2020) [137] |
||
| Fostering Connections | Ireland | Lotty, Bantry-White, et al. (2020) [92] | Lotty, Dunn, et al. (2020) [156] | ||
| Fostering Healthy Futures (FHF) | USA |
Taussig, Culhane, et al. (2007) [66]; Taussig, Culhane, et al. (2013) [65]; Taussig, Weiler, et al. (2015) [64]; Weiler, Taussig (2019) [70]; Weiler, Lee (2021) [69] |
Taussig, Weiler, et al. (2019) [101] |
Taussig, Culhane (2010) [144]; Taussig, Culhane, et al. (2013) [65]; Taussig, Weiler, et al. (2019) [101]; Weiler, Taussig (2019) [70]; Weiler, Lee (2021) [69] |
|
| Fostering Individualised Assistance programme (FIAP) | USA | Clark, Prange, et al. (1994) [125] | |||
| Glasgow Infant Family Team (GIFT); London Infant Family Team (LIFT); New Orleans Model | UK |
Baginsky (2017) [175]; Turner-Halliday, Watson, et al. (2016) [104]; Turner-Halliday, Kainth, et al. (2017) [103] |
|||
| Head, Heart, Hands | UK | McDermid, Trivedi, et al. (2021) [93] | |||
| Head Start | USA | Lipscomb, Pratt, et al. (2013) [131] | |||
| HealthRHYTHMS | USA | Bittman, Dickson, et al. (2009) [124] | |||
| Herts and Mind: Mentalization-Based Therapy | UK | Midgley, Besser, et al. (2019) [94] | Midgley, Besser, et al. (2019) [94] | ||
| Incredible Years | Portugal; UK; USA | Nilsen (2007) [60] |
Conn, Szilagyi, et al. (2018) [82]; Furlong, McLoughlin, et al. (2021) [84]; Hutchings, Bywater (2013) [87]; Nilsen (2007) [60]; Silva, Gaspar, et al. (2016) [98] |
Conn, Szilagyi, et al. (2018) [82]; Linares, Montalto, et al. (2006) [130] |
Furlong, McLoughlin, et al. (2021) [84]; Nilsen (2007) [60] |
| Individual therapy and rehabilitative strategies | USA | Pozo-Breen (2017) [160] | |||
| Intensive Permanence Systems | USA | Hall, Semanchin, et al. (2018) [86] | |||
| kContact | Suomi, Lucas, et al. (2020) [169] | ||||
| Keeping Foster and Kinship Parents Supported and Trained (KEEP) | USA |
Chamberlain, Price, et al. (2008) [71]; Chamberlain, Roberts, et al. (2012) [53]; Price (2009) [62] |
Buchanan, Chamberlain, et al. (2012) [79]; Walsh (2017) [106]; Chamberlain, Price, et al. [81] |
Chamberlain, Price, et al. (2008) [71]; Price, Roesch, et al. (2015) [140]; Price, Roesch, et al. (2019) [141] |
Greeno, Lee, et al. (2016) [149]; Price, Roesch, et al. (2012) [161] |
| Kids in Transition to Schools (KITS) | USA | Bronz (2004) [148] | |||
| Kundalini Yoga | UK | Vallejos, Ball, et al. (2016) [105] | Vallejos, Ball, et al. (2016) [105] | ||
| Life Story | USA | Haight, Black, et al. (2010) [85] | Haight, Black, et al. (2010) [85] | ||
| Mentoring intervention for teenage pregnancy | UK | Mezey, Meyer, et al. (2015) [59] | Mezey, Meyer, et al. (2015) [59] | Mezey, Meyer, et al. (2015) [59] | |
| Mindfulness | USA | Jee, Couderc, et al. (2015) [89] | Jee, Couderc, et al. (2015) [89] | ||
| Multidimensional Treatment Foster Care (MTFC); Multidimensional Treatment Foster Care-Adolescents (MTFC-A); Multidimensional Treatment Foster Care-Pre-schoolers (MTFC-P) | Netherlands; UK; USA |
Chamberlain (2003) [51]; Chamberlain (2006) [52]; Chamberlain, Roberts, et al. (2012) [53]; Leve, Fisher, et al. (2009) [58] |
Biehal, Dixon, et al. (2012) [76]; Brown, Chamberlain, et al. (2014) [78]; Kirton, Thomas (2011) [90] |
Biehal, Dixon, et al. (2012) [76]; Green, Roberts, et al. (2014) [128]; Jonkman, Schuengel, et al. (2017) [129] |
Biehal, Dixon, et al. (2012) [76]; Green, Roberts, et al. (2014) [128] |
| NonViolent Resistance (NVR) Training | Belgium | Van-Holen, Vanderfaeillie, et al. (2018) [145] | |||
| Opportunities Box | Portugal | Silva, Coelho, et al. (2017) [164] | |||
| Outpatient mental health services | USA | Bellamy (2013) [147] | |||
| Parent–Child Interaction Therapy (PCIT) | USA | Blair, Topitzes, et al. (2019) [77] | Mersky, Topitzes, et al. (2016) [134]; Mersky, Topitzes, et al. (2020) [172] | Timmer, Urquiza, et al. (2006) [165] | |
| Parent Management Training (PMT); Parent Management Training Oregon Model (PMTO) | Netherlands; USA |
Leathers, Spielfogel, et al. (2011) [114]; Maaskant, Van Rooj et al. (2016) [118]; Spielfogel, Leathers, et al. (2011) [100] |
Akin, Lang, Yan, et al. (2018) [121]; Akin, Lang, Yan, et al. (2019) [122]; Maaskant, Van Rooj et al. (2016) [118]; Maaskant, Van Rooj, et al. (2017) [132]; Yan & De Luca (2020) [170] |
Leathers, Spielfogel, et al. (2011) [114] | |
| Pathways Home | USA | DeGarmo, Reid, et al. (2013) [54] | DeGarmo, Reid, et al. (2013) [54] | ||
| Promoting First Relationships | USA | Oxford, Marcenko, et al. (2016) [139] | |||
| Psychosocial rehabilitation | USA | Williams, Sherr (2009) [166] | |||
| Sanctuary Model | USA | Rivard, Bloom, et al. (2003) [162] | |||
| Solution Focused Parenting Group (SFPG) | Canada | Triantafillou (2002) [102] | Triantafillou (2002) [102] | ||
| SuppOrting Looked after children In Decreasing Drugs, and alcohol (SOLID) | UK | Alderson, Kaner, et al. (2020) [72] |
Alderson, Kaner, et al. (2020) [72]; Alderson, Kaner, et al. (2020) [108]; Alderson, McGovern, et al. (2021) [109] |
Alderson, Kaner, et al. (2020) [72]; Alderson, Kaner, et al. (2020) [108] | |
| TAKE CHARGE | USA | Geenen, Powers, et al. (2013) [113] | Geenen, Powers, et al. (2013) [113] | ||
| Teach Your Children Well | Canada | Marquis (2014) [133] | |||
| Therapeutic Mentoring | USA | Johnson, Price et al. (2010) [171] | |||
| Trauma-Focused Cognitive Behavioural Therapy (TF-CBT) and evidence-based engagement strategies | USA |
Dorsey, Conover, et al. (2014) [83]; Dorsey, Pullmann, et al. (2014) [112] |
Dorsey, Pullmann, et al. (2014) [112] | ||
| Trauma Systems Therapy (TST) | USA | Murphy, Moore, et al. (2017) [115] | Murphy, Moore, et al. (2017) [115] | ||
| Treatment Foster Care (TFC); Treatment Foster Care (TFC) for Older Youth; Together Facing the Challenge (TFTC) | USA |
Farmer, Lippold (2016) [55]; James, Meezan (2002) [57]; Southerland, Mustillo et al. (2009) [63] |
Lee, Phillips, et al. (2021) [91]; Tullberg, Vaughon, et al. (2019) [176]; McMillen, Narendorf, et al. (2015) [119]; Murray, Culver, et al. (2014) [95] |
Farmer, Burns, et al. (2010) [127] | |
| Triple P for Foster Carers (TPFC) | Germany | Job, Ehrenberg, et al. (2020) [111] | Job, Ehrenberg, et al. (2020) [111] | ||
| Wave by Wave | Portugal | Pereira, Ferreira, et al. (2020) [168] | |||
| Youth-Initiated Mentoring (YIM) Relationships | USA | Spencer, Drew, et al. (2018) [99] | |||
There were 86 outcome evaluations. Of these, 52 were randomised controlled trials (RCTs) and 34 were non-randomised evaluations. The majority of RCTs (n = 43) evaluated interventions (n = 31) that primarily targeted the intrapersonal or interpersonal domains [54, 59, 65, 67, 69, 70, 82, 85, 88, 89, 94, 96, 97, 101, 111–113, 117, 118, 120–124, 126, 130, 132–139, 142–146, 168–170, 172]. Five interventions that operated across the organisational, community and policy domains were evaluated via an RCT (n = 9 study reports) [71, 125, 127–129, 131, 140, 141, 182]. Of interventions evaluated through a non-randomised study, 21 interventions, with 22 study reports, targeted the intrapersonal and interpersonal domains [50, 60, 61, 68, 84, 102, 105, 114, 148, 152, 154–156, 158, 160, 162–167, 171]. Six interventions, with 12 evaluations targeted the organisational, community and policy domains [73, 115, 128, 147, 149–151, 153, 157, 159, 161, 182]. There were 14 study reports that provided moderator analysis or interaction effects that were relevant to assessing equity harms [54, 65, 69–71, 101, 122, 126, 130, 133, 140, 142, 170, 182].
There was one partial economic evaluation, which estimated the relative costs and consequences of a new intervention compared to the estimated costs of usual care [173].
Discussion
The CHIMES systematic review aimed to synthesise international evidence on interventions targeting the mental health and wellbeing of care-experienced children and young people. The first phase of the review, an evidence map of the available literature, is reported presently.
Mapping interventions by the socio-ecological domain targeted, the main cluster was intrapersonal and interpersonal approaches, often targeting children and young people’s skills and knowledge, or carers’ parenting practices. Some of these also combined organisational and community facing activities to optimise functioning and implementation. As identified in a range of systematic and practitioner reviews of parenting interventions for care-experienced children and young people [187–190], a couple of interventions were dominant in the map. These were the USA originated Multidimensional Treatment Foster Care (MTFC) [51–53, 58, 76, 78, 90, 128, 129] and its derivative Keeping Foster and Kinship Parents Supported and Trained (KEEP) [53, 71, 62, 79, 106, 140, 141, 149, 161], which provide intensive parenting training for foster and kinship carers, embedded in a wider system of support services. Overall, these interventions were under-described and under-theorised, but where specified they often draw on theories related to social modelling and prosocial developmental contexts [179, 181].
In contrast, there was a clear gap in structural-level interventions targeting organisational, community and policy drivers. This is significant given that risk factors for poor mental health in this population include a constellation of family and child welfare system-level factors, which are embedded in a wider context of community-level challenges, such as economic opportunity and socio-economic deprivation [191]. Equally, structural interventions were identified as a priority area for stakeholders who informed the scope and focus of the CHIMES review.
The map identified a wealth of interventions targeting mental health, behavioural and neurodevelopmental disorders, specifically total social, emotional and behavioural problems. Conversely, there was a dearth of interventions targeting subjective wellbeing and suicide-related outcomes, despite care-experienced young people reporting relative adversity in these areas compared to the general population [7, 8]. This reflects wider findings in the research evidence, with a recent review of suicide prevention interventions for children involved in child protection services also identifying a paucity of evidence-based approaches [192]. New interventions might be developed to target these outcomes, or existing approaches adapted if theoretically appropriate. To this end, there is a need to further develop the operationalisation of these constructs and understand the causes that should be targeted to leverage the most change [193]. The extant evidence base, while limited, suggests potential drivers of wellbeing that might be targeted. Primarily operating within the interpersonal domain, these include positive relationships with teachers and family [7, 194], and having available supports, notably material support [194]. Causal mechanisms for suicide-related outcomes are less evident, with current research tending to focus on identifying socio-demographic risk profiles within this population (e.g. age, ethnicity and maltreatment exposure) [6].
The evidence map has implications for future research. Presently the weight of available evidence is focused on outcome evaluation, although only a limited number consider the potential for equity harms [195]. Methodological guidance related to the development, adaptation and evaluation of interventions recommends the integration of outcome data with a clear understanding of the underpinning theory, explication of context, implementation and acceptability through process evaluation, and economic evaluation [39, 40, 196].
As indicated, there remains a lack of description of interventions’ programme theory, with less than a fifth of included interventions reporting a theoretical basis. This is imperative in knowing how interventions interact with system conditions in the generation of outcomes. Given that the evidence base is predominantly located in the USA to date, this means that there is currently a lack of knowledge about the implementation of different approaches in diverse contexts, cultures and countries. Understanding how programme theories function in the USA evaluation context can offer insight into the potential replicability of effects elsewhere. It can then support efforts to adapt interventions to different settings or population subgroups, or to identify where transportation may not be suitable and new approaches need to be developed [39].
Equally, while there continues to be expansion in the conduct of process evaluations, these tend to be conceptually and empirically thin, providing rudimentary summaries of reach and delivery. This is reflected in systematic reviews that currently synthesise process evaluation data, which largely detail barriers and facilitators to implementation [26]. Understanding of wider contextual characteristics, through conceptually and empirically rich process evaluation, is important from a complex systems perspective, which emphasises that intervention’s functioning is dependent on its interaction with both proximal and distal system characteristics [30–34].
There is also a paucity of economic evaluations, which reflects a wider issue identified in children’s social care research [197]. Failing to attend to the cost-effectiveness of interventions is a particular concern given extant issues around escalating costs across social care systems [14].
Beyond implications for evaluation research, there are also some initial suggestions for enhancing systematic reviews in the area of care-experienced populations. It is important that interventions are more comprehensively described in evaluations, preferably with the use of reporting guidance such as the TIDIeR Framework for intervention descriptions [47]. Systematic description of the complex system in which interventions are delivered, using frameworks such as the Context and Implementation of Complex Interventions (CICI) framework [198], will be particularly helpful in supporting future syntheses. In regard to the review process, future reviews of intervention evaluations might aim to map and synthesise all relevant types of evidence [47], particularly in relation to theory, equity and economic outcomes. This will help to identify where gaps continue and where good practice is emerging. Finally, reviews might take advantage of methodological progress in integrating complex systems perspectives into systematic reviews, to help understand the interaction of interventions with system features more fully [34, 199].
Review limitations
There are five central limitations associated with the evidence map. First, the literature around care-experienced populations can be challenging to identify, largely due to extensive international variations in terminology. As such, while the review searches were designed and tested to be sensitive, some study reports may have been missed. Second, the review was limited to studies conducted in higher-income countries, as classified by the Organisation for Economic Co-operation and Development (OECD). As a result, the review has limited generalisability to middle- and lower-income countries, and potentially higher-income countries that do not fall within this classification. Third, there was limited reporting of interventions and associated evaluations, which provided challenges in the cataloguing and mapping of study reports. There were further issues due to the under-specification of interventions’ programme theory. Fourth, study reports were aggregated to chart overarching evidence gaps and clusters. As a result, some of the diversity between interventions and countries is not fully described. Fifth, at the stage of evidence mapping, we did not quality appraise study reports. As such reporting of evidence clusters only reflects the quantity of interventions and evaluations.
Conclusion
The present evidence map describes intervention and evidence clusters and gaps in relation to mental health and wellbeing interventions for care-experienced children and young people. With the predominance of intrapersonal and interpersonal interventions from the USA, future development and adaptation might focus on structural-level theories and components, paying attention to how they function in different contexts. They might also focus on subjective wellbeing and suicide-related outcomes. Intervention research needs to integrate theory, outcome, process and economic evaluation to strengthen the evidence base.
Acknowledgements
The CHIMES review acknowledges the support of the Project Advisory Group, participants of stakeholder consultations, Dr Asmaa El-Banna, Dr Helen Morgan, Lindsey Allan, Clare Olsen, Payton Ramsey, Rohen Renold, Lorna Stabler and Rachel Vaughan.
Authors’ contributions
Dr RE conducted the conception of study design; screening of study reports; extracting and appraising of study reports; review synthesis; stakeholder consultation; drafting of the publication; confirming of the publication. Dr SM conducted the screening of study reports; extracting and appraising of study reports; review synthesis; conducting of stakeholder consultation; confirming of the publication. Dr RT conducted the screening of study reports; extracting and appraising of study reports; review synthesis; confirming of the publication. Professor G.J.M-T conducted the conception of the study design; screening of study reports; extracting and appraising of study reports; review synthesis, notably the meta-analysis; confirming of the publication. Professor MR conducted the conception of the study design: review synthesis; confirming of the publication. SW (Systematic Reviewer) conducted the conception of the search strategy; conducting of searches for study reports; conducting of all related information specialist tasks; screening of study reports; extracting and appraising of study reports; confirming of the publication. MB conducted the stakeholder consultations; confirming of the publication. CW conducted the stakeholder consultations; confirming of the publication. SV conducted the screening of study reports; extracting and appraising of study reports; confirming of the publication. Professor JN conducted the conception of the study design; review synthesis; drafting of the publication; confirming of the publication.
Funding
This work was supported by the NIHR-PHR grant number NIHR129113. This work was supported by The Centre for Development, Evaluation, Complexity and Implementation in Public Health Improvement (DECIPHer) funded by Welsh Government through Health and Care Research Wales. The Centre for Trials Research receives funding from Health and Care Research Wales and Cancer Research UK.
Availability of data and materials
Data extraction, analysis and synthesis are available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
The CHIMES review was exempted from ethical approval from Cardiff University’s School of Social Sciences Research Ethics Committee.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.United Nations . Guidelines for the Alternative Care of Children New York: UN. 2010. [Google Scholar]
- 2.Harwin J, Alrouh B, Golding L, McQuarrie T, Broadhurst K, Cusworth L. The contribution of supervision orders and special guardianship to children’s lives and family justice. Lancaster: Final report to the Nuffield Foundation, Lancaster University; 2019. [Google Scholar]
- 3.Stein M. Supporting young people from care to adulthood: international practice. Child Fam Soc Work. 2019;24(3):400–405. doi: 10.1111/cfs.12473. [DOI] [Google Scholar]
- 4.Desmond C, Watt K, Saha A, Huang J, Lu C. Prevalence and number of children living in institutional care: global, regional, and country estimates. Lancet Child AdolescHealth. 2020;4(5):370–377. doi: 10.1016/S2352-4642(20)30022-5. [DOI] [PubMed] [Google Scholar]
- 5.Ford T, Vostanis P, Meltzer H, Goodman R. Psychiatric disorder among British children looked after by local authorities: comparison with children living in private households. Br J Psychiatry. 2018;190(4):319–325. doi: 10.1192/bjp.bp.106.025023. [DOI] [PubMed] [Google Scholar]
- 6.Engler AD, Sarpong KO, Van Horne BS, Greeley CS, Keefe RJ. A systematic review of mental health disorders of children in foster care. Trauma Violence Abuse. 2022;23(1):255–264. doi: 10.1177/1524838020941197. [DOI] [PubMed] [Google Scholar]
- 7.Long SJ, Evans RE, Fletcher A, Hewitt G, Murphy S, Young H, et al. Comparison of substance use, subjective well-being and interpersonal relationships among young people in foster care and private households: a cross sectional analysis of the School Health Research Network survey in Wales. BMJ Open. 2017;7(2). [DOI] [PMC free article] [PubMed]
- 8.Evans R, White J, Turley R, Slater T, Morgan H, Strange H, et al. Comparison of suicidal ideation, suicide attempt and suicide in children and young people in care and non-care populations: Systematic review and meta-analysis of prevalence. Child Youth Serv Rev. 2017;82:122–129. doi: 10.1016/j.childyouth.2017.09.020. [DOI] [Google Scholar]
- 9.Bronsard G, Alessandrini M, Fond G, Loundou A, Auquier P, Tordjman S, et al. The prevalence of mental disorders among children and adolescents in the child welfare system: a systematic review and meta-analysis. Medicine. 2016;95(7):e2622-e. doi: 10.1097/MD.0000000000002622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Murray ET, Lacey R, Maughan B, Sacker A. Association of childhood out-of-home care status with all-cause mortality up to 42-years later: Office of National Statistics Longitudinal Study. BMC Public Health. 2020;20:1–10. doi: 10.1186/s12889-020-08867-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.James S. Why do foster care placements disrupt? An investigation of reasons for placement change in foster care. Soc Serv Rev. 2004;78(4):601–627. doi: 10.1086/424546. [DOI] [Google Scholar]
- 12.Rubin DM, Alessandrini EA, Feudtner C, Mandell DS, Localio AR, Hadley T. Placement stability and mental health costs for children in foster care. Pediatrics. 2004;113(5):1336–1341. doi: 10.1542/peds.113.5.1336. [DOI] [PubMed] [Google Scholar]
- 13.Rock S, Michelson D, Thomson S, Day C. Understanding foster placement instability for looked after children: a systematic review and narrative synthesis of quantitative and qualitative evidence. Br J Soc Work. 2015;45(1):177–203. doi: 10.1093/bjsw/bct084. [DOI] [Google Scholar]
- 14.Holmes L. Children’s social care cost pressures and variations in unit costs. 2021. [Google Scholar]
- 15.Luke N, Sinclair I, Woolgar M, Sebba J. What works in preventing and treating poor mental health in looked after children. London: NSPCC; 2014. [Google Scholar]
- 16.Everson-Hock ES, Jones R, Guillaume L, Clapton J, Goyder E, Chilcott J, et al. The effectiveness of training and support for carers and other professionals on the physical and emotional health and well-being of looked-after children and young people: a systematic review. Child Care Health Dev. 2012;38(2):162–174. doi: 10.1111/j.1365-2214.2011.01247.x. [DOI] [PubMed] [Google Scholar]
- 17.Hambrick EP, Oppenheim-Weller S, N'Zi AM, Taussig HN. Mental health interventions for children in foster care: a systematic review. Child Youth Serv Rev. 2016;70:65–77. doi: 10.1016/j.childyouth.2016.09.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kerr L, Cossar J. Attachment interventions with foster and adoptive parents: a systematic review. Child Abuse Rev. 2014;23(6):426–439. doi: 10.1002/car.2313. [DOI] [Google Scholar]
- 19.O'Higgins A, Ott EM, Shea MW. What is the impact of placement type on educational and health outcomes of unaccompanied refugee minors? A systematic review of the evidence. Clin Child Fam Psychol Rev. 2018;21(3):354–365. doi: 10.1007/s10567-018-0256-7. [DOI] [PubMed] [Google Scholar]
- 20.Marsh D. A systematic review and meta-analysis of randomized clinical trials of evidence-based practices through measured change of behavior for children in foster care. 2017. [Google Scholar]
- 21.Solomon DT, Niec LN, Schoonover CE. The impact of foster parent training on parenting skills and child disruptive behavior. Child Maltreat. 2017;22(1):3–13. doi: 10.1177/1077559516679514. [DOI] [PubMed] [Google Scholar]
- 22.Sullivan AL, Simonson GR. A systematic review of school-based social-emotional interventions for refugee and war-traumatized youth. Rev Educ Res. 2016;86(2):503–530. doi: 10.3102/0034654315609419. [DOI] [Google Scholar]
- 23.Bergström M, Cederblad M, Håkansson K, Jonsson AK, Munthe C, Vinnerljung B, et al. Interventions in foster family care: a systematic review. Res Soc Work Pract. 2019;30(1):3–18. doi: 10.1177/1049731519832101. [DOI] [Google Scholar]
- 24.Greeson JKP, Garcia AR, Tan F, Chacon A, Ortiz AJ. Interventions for youth aging out of foster care: a state of the science review. Child Youth Serv Rev. 2020;113:105005. doi: 10.1016/j.childyouth.2020.105005. [DOI] [Google Scholar]
- 25.Barnett ER, Concepcion-Zayas MT, Zisman-Ilani Y, Bellonci C. Patient-centered psychiatric care for youth in foster care: a systematic and critical review. J Publ Child Welfare. 2019;13(4):462–489. doi: 10.1080/15548732.2018.1512933. [DOI] [Google Scholar]
- 26.Excellence NIfHaC . Looked-after children and young people: interventions to promote physical, mental, and emotional health and wellbeing of lookedafter children, young people and care leavers. NICE guideline NG205. 2021. [PubMed] [Google Scholar]
- 27.Turner W, Macdonald G. Treatment foster care for improving outcomes in children and young people: a systematic review. Res Soc Work Pract. 2011;21(5):501–527. doi: 10.1177/1049731511400434. [DOI] [PubMed] [Google Scholar]
- 28.Åström T, Bergström M, Håkansson K, Jonsson AK, Munthe C, Wirtberg I, et al. Treatment foster care oregon for delinquent adolescents: a systematic review and meta-analysis. Res Soc Work Pract. 2020;30(4):355–367. doi: 10.1177/1049731519890394. [DOI] [Google Scholar]
- 29.Hawe P. Minimal, negligible and negligent interventions. Soc Sci Med. 2015;138:265–268. doi: 10.1016/j.socscimed.2015.05.025. [DOI] [PubMed] [Google Scholar]
- 30.Moore GF, Evans RE. What theory, for whom and in which context? Reflections on the application of theory in the development and evaluation of complex population health interventions. SSM - Population Health. 2017;3:132–135. doi: 10.1016/j.ssmph.2016.12.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Moore GF, Evans RE, Hawkins J, Littlecott H, Melendez-Torres GJ, Bonell C, et al. From complex social interventions to interventions in complex social systems: Future directions and unresolved questions for intervention development and evaluation. Evaluation. 2018;25(1):23–45. doi: 10.1177/1356389018803219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hawe P, Shiell A, Riley T. Theorising interventions as events in systems. Am J Community Psychol. 2009;43(3):267–276. doi: 10.1007/s10464-009-9229-9. [DOI] [PubMed] [Google Scholar]
- 33.McGill E, Er V, Penney T, Egan M, White M, Meier P, et al. Evaluation of public health interventions from a complex systems perspective: a research methods review. Soc Sci Med. 2021;272:113697. doi: 10.1016/j.socscimed.2021.113697. [DOI] [PubMed] [Google Scholar]
- 34.Petticrew M, Knai C, Thomas J, Rehfuess EA, Noyes J, Gerhardus A, et al. Implications of a complexity perspective for systematic reviews and guideline development in health decision making. BMJ Glob Health. 2019;4(Suppl 1):e000899. doi: 10.1136/bmjgh-2018-000899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Educ Q. 1988;15(4):351–377. doi: 10.1177/109019818801500401. [DOI] [PubMed] [Google Scholar]
- 36.Bronfenbrenner U. The ecology of human development: experiments by nature and design. Cambridge: Harvard university press; 1979.
- 37.O’Cathain A, Croot L, Sworn K, Duncan E, Rousseau N, Turner K, et al. Taxonomy of approaches to developing interventions to improve health: a systematic methods overview. Pilot Feasib Stud. 2019;5(1):1–27. doi: 10.1186/s40814-019-0425-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.O'Cathain A, Croot L, Duncan E, Rousseau N, Sworn K, Turner KM, et al. Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open. 2019;9(8):e029954. doi: 10.1136/bmjopen-2019-029954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Moore G, Campbell M, Copeland L, Craig P, Movsisyan A, Hoddinott P, et al. Adapting interventions to new contexts—the ADAPT guidance. BMJ. 2021;374:n1679. doi: 10.1136/bmj.n1679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. Framework for the development and evaluation of complex interventions: gap analysis, workshop and consultation-informed update. Health Technol Assess. 2021;25(57):1–132. doi: 10.3310/hta25570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Miake-Lye IM, Hempel S, Shanman R, Shekelle PG. What is an evidence map? A systematic review of published evidence maps and their definitions, methods, and products. Syst Rev. 2016;5(1):28. doi: 10.1186/s13643-016-0204-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Evans R, Boffey M, MacDonald S, Noyes J, Melendez-Torres G, Morgan HE, et al. Care-experienced cHildren and young people’s Interventions to improve Mental health and wEll-being outcomes: systematic review (CHIMES) protocol. BMJ Open. 2021;11(1):e042815. doi: 10.1136/bmjopen-2020-042815. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Noyes J, Booth A, Moore G, Flemming K, Tunçalp Ö, Shakibazadeh E. Synthesising quantitative and qualitative evidence to inform guidelines on complex interventions: clarifying the purposes, designs and outlining some methods. BMJ Glob Health. 2019;4(Suppl 1):e000893. doi: 10.1136/bmjgh-2018-000893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Clapton J, Rutter D, Sharif N. SCIE Systematic mapping guidance. London: SCIE; 2009. [Google Scholar]
- 45.Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018;169(7):467–473. doi: 10.7326/M18-0850. [DOI] [PubMed] [Google Scholar]
- 46.UNICEF . The United Nations Convention on the Rights of the Child. London: UNICEF; 1989. [Google Scholar]
- 47.van Vliet P, Hunter SM, Donaldson C, Pomeroy V. Using the TIDieR Checklist to Standardize the Description of a Functional Strength Training Intervention for the Upper Limb After Stroke. J Neurol Phys Ther. 2016;40(3):203–208. doi: 10.1097/NPT.0000000000000133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Tancred T, Melendez-Torres GJ, Paparini S, Fletcher A, Stansfield C, Thomas J, et al. Public Health Research. Interventions integrating health and academic education in schools to prevent substance misuse and violence: a systematic review. Southampton (UK): NIHR Journals Library 2019. [PubMed]
- 49.Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5(1):69. doi: 10.1186/1748-5908-5-69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Bachi K, Terkel J, Teichman M. Equine-facilitated psychotherapy for at-risk adolescents: The influence on self-image, self-control and trust. Clin Child Psychol Psychiatry. 2012;17(2):298–312. doi: 10.1177/1359104511404177. [DOI] [PubMed] [Google Scholar]
- 51.Chamberlain P. The Oregon Multidimensional Treatment Foster Care Model: features, outcomes, and progress in dissemination. Cogn Behav Pract. 2003;10(4):303–312. doi: 10.1016/S1077-7229(03)80048-2. [DOI] [Google Scholar]
- 52.Chamberlain P, Leve Leslie D, Smith DK. Preventing behavior problems and health-risking behaviors in girls in foster care. Int J Behav Consult Ther. 2006;2(4):518–530. doi: 10.1037/h0101004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Chamberlain P, Roberts R, Jones H, Marsenich L, Sosna T, Price JM. Three collaborative models for scaling up evidence-based practices. Adm Policy Ment Health. 2012;39(4):278–290. doi: 10.1007/s10488-011-0349-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.DeGarmo DS, Reid John B, Fetrow Becky A, Fisher Philip A, Antoine KD. Preventing child behavior problems and substance use: the pathways home foster care reunification intervention. J Child Adolesc Subst Abuse. 2013;22(5):388–406. doi: 10.1080/1067828X.2013.788884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Farmer Elizabeth MZ, Lippold MA. The need to do it all: exploring the ways in which treatment foster parents enact their complex role. Child Youth Serv Rev. 2016;64:91–99. doi: 10.1016/j.childyouth.2016.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Fisher PA, Ellis BH, Chamberlain P. Early intervention foster care: a model for preventing risk in young children who have been maltreated. Child Serv Soc Policy Res Pract. 1999;2(3):159–182. [Google Scholar]
- 57.James S, Meezan W. Refining the evaluation of treatment foster care. Fam Soc J Contemp Human Serv. 2002;83(3):233–244. doi: 10.1606/1044-3894.24. [DOI] [Google Scholar]
- 58.Leve LD, Fisher PA, Chamberlain P. Multidimensional treatment foster care as a preventive intervention to promote resiliency among youth in the child welfare system. J Pers. 2009;77(6):1869–1902. doi: 10.1111/j.1467-6494.2009.00603.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Mezey G, Meyer D, Robinson F, Bonell C, Campbell R, Gillard S, et al. Developing and piloting a peer mentoring intervention to reduce teenage pregnancy in looked-after children and care leavers: an exploratory randomised controlled trial. Health Technol Assess. 2015;19(85):1–139. doi: 10.3310/hta19850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Nilsen W. Fostering futures: a preventive intervention program for school-age children in foster care. Clin Child Psychol Psychiatry. 2007;12(1):45–63. doi: 10.1177/1359104507071055. [DOI] [PubMed] [Google Scholar]
- 61.Pithouse A, Hill-Tout J, Lowe K. Training foster carers in challenging behaviour: a case study in disappointment? Child Fam Soc Work. 2002;7(3):203–214. doi: 10.1046/j.1365-2206.2002.00249.x. [DOI] [Google Scholar]
- 62.Price JM, Chamberlain P, Landsverk J, Reid J. KEEP foster-parent training intervention: model description and effectiveness. Child Fam Soc Work. 2009;14:233-42. 10.1111/j.1365-2206.2009.00627.x.
- 63.Southerland Dannia G, Mustillo Sarah A, Farmer Elizabeth MZ, Stambaugh Leyla F, Murray M. What’s the relationship got to do with it? Understanding the therapeutic relationship in therapeutic foster care. Child Adolesc Soc Work J. 2009;26(1):49–63. doi: 10.1007/s10560-008-0159-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Taussig H, Weiler L, Rhodes T, Hambrick E, Wertheimer R, Fireman O, et al. Fostering healthy futures for teens: adaptation of an evidence-based program. J Soc Soc Work Res. 2015;6(4):617–642. doi: 10.1086/684021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Taussig Heather N, Culhane Sara E, Garrido E, Knudtson Michael D, Petrenko Christie LM. Does severity of physical neglect moderate the impact of an efficacious preventive intervention for maltreated children in foster care? Child Maltreat. 2013;18(1):56–64. doi: 10.1177/1077559512461397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Taussig Heather N, Culhane Sara E, Hettleman D. Fostering healthy futures: an innovative preventive intervention for preadolescent youth in out-of-home care. Child Welfare. 2007;86(5):113–131. [PMC free article] [PubMed] [Google Scholar]
- 67.Van H, Frank. Vanschoonlandt F, Vanderfaeillie J. Evaluation of a foster parent intervention for foster children with externalizing problem behaviour. Child Fam Soc Work. 2017;22(3):1216–26. doi: 10.1111/cfs.12338. [DOI] [Google Scholar]
- 68.Vanschoonlandt F, Vanderfaeillie J, Van H, De M, Vanschoonlandt F, Vanderfaeillie J, et al. Development of an intervention for foster parents of young foster children with externalizing behavior: theoretical basis and program description. Clin Child Fam Psychol Rev. 2012;15(4):330–344. doi: 10.1007/s10567-012-0123-x. [DOI] [PubMed] [Google Scholar]
- 69.Weiler LM, Lee S-K, Zhang J, Ausherbauer K, Schwartz Sarah EO, Kanchewa Stella S, et al. Mentoring children in foster care: examining relationship histories as moderators of intervention impact on children’s mental health and trauma symptoms. American Journal of Community Psychology. 2021;n/a(n/a). [DOI] [PMC free article] [PubMed]
- 70.M WL, Taussig Heather N. The moderating effect of risk exposure on an efficacious intervention for maltreated children. J Clin Child Adolesc Psychol. 2019;48:S194–S201. doi: 10.1080/15374416.2017.1295379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Chamberlain P, Price J, Leve LD, Laurent H, Landsverk JA, Reid JB, et al. Prevention of behavior problems for children in foster care: outcomes and mediation effects. Prev Sci. 2008;9(1):17–27. doi: 10.1007/s11121-007-0080-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Alderson H, Kaner E, Brown R, et al. Behaviour change interventions to reduce risky substance use and improve mental health in children in care: the SOLID three-arm feasibility RCT. Southampton (UK): NIHR Journals Library; 2020. (Public Health Research, No. 8.13.) Available from: https://www.ncbi.nlm.nih.gov/books/NBK562036/. [PubMed]
- 73.Izzo Charles V, et al. Improving relationship quality in group care settings: the impact of implementing the CARE model. Child Youth Serv Rev. 2020;109:104623. doi: 10.1016/j.childyouth.2019.104623. [DOI] [Google Scholar]
- 74.Aventin A, Houston S, Macdonald G. Utilising a computer game as a therapeutic intervention for youth in residential care: some preliminary findings on use and acceptability. Child Youth Serv Rev. 2014;47(Part 3):362–9. doi: 10.1016/j.childyouth.2014.10.012. [DOI] [Google Scholar]
- 75.Baginsky M. The New Orleans Intervention Model: Early Implementation in a London Borough Evaluation report. London. 2017. [Google Scholar]
- 76.Biehal N, Dixon J, Parry E, Sinclair I, Green J, Roberts C, et al. The Care Placements Evaluation (CaPE) Evaluation of Multidimensional Treatment Foster Care for Adolescents (MTFC-A). London: Department for Education; 2012.
- 77.Blair K, Topitzes J, Mersky JP. Brief, group-based parent-child interaction therapy: Examination of treatment attrition, non-adherence, and non-response. Child Youth Serv Rev. 2019;106.
- 78.Brown CH, Chamberlain P, Saldana L, Padgett C, Wang W, Cruden G. Evaluation of two implementation strategies in 51 child county public service systems in two states: results of a cluster randomized head-to-head implementation trial. Implement Sci. 2014;9:134. doi: 10.1186/s13012-014-0134-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Buchanan R, Chamberlain P, Price Joseph M, Sprengelmeyer P. Examining the equivalence of fidelity over two generations of KEEP implementation: a preliminary analysis. Child Youth Serv Rev. 2013;35(1):188–193. doi: 10.1016/j.childyouth.2012.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Callaghan J, Young B, Richards M, Vostanis P. Developing new mental health services for looked after children: a focus group study. Adopt Foster. 2003;27(4):51–63. doi: 10.1177/030857590302700408. [DOI] [Google Scholar]
- 81.Chamberlain P, Price J, Reid J, Landsverk J. Cascading Implementation of a Foster and Kinship Parent Intervention. Child Welfare. 2008;87(5):27–48. [PMC free article] [PubMed] [Google Scholar]
- 82.Conn A-M, Szilagyi Moira A, Alpert-Gillis L, Webster-Stratton C, Manly Jody T, Goldstein N, et al. Pilot randomized controlled trial of foster parent training: a mixed-methods evaluation of parent and child outcomes. Child Youth Serv Rev. 2018;89:188–197. doi: 10.1016/j.childyouth.2018.04.035. [DOI] [Google Scholar]
- 83.Dorsey S, Conover KL, Revillion C. Improving foster parent engagement: using qualitative methods to guide tailoring of evidence-based engagement strategies. J Clin Child Adolesc Psychol. 2014;43(6):877–89. doi: 10.1080/15374416.2013.876643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Furlong M, McLoughlin F, McGilloway S. The incredible years parenting program for foster carers and biological parents of children in foster care: a mixed methods study. Child Youth Serv Rev. 2021;126:106028. doi: 10.1016/j.childyouth.2021.106028. [DOI] [Google Scholar]
- 85.Haight W, Black J, Sheridan K. A mental health intervention for rural, foster children from methamphetamine-involved families: experimental assessment with qualitative elaboration. Child Youth Serv Rev. 2010;32(10):1446–1457. doi: 10.1016/j.childyouth.2010.06.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Hall Seventy F, Semanchin J, Annette Implementation of intensive permanence services: a trauma-informed approach to preparing foster youth for supportive relationships. Child Adolesc Soc Work J. 2018;35(6):587–98. doi: 10.1007/s10560-018-0550-8. [DOI] [Google Scholar]
- 87.Hutchings J, Bywater T. Delivering the Incredible Years parent programme to foster carers in Wales: reflections from group leader supervision. Adopt Foster. 2013;37(1):28–42. doi: 10.1177/0308575913477075. [DOI] [Google Scholar]
- 88.Briskman J, Castle J, Blackeby K, Bengo C, Slack K, Stebbens C, Leaver W, Scott S. Randomised controlled trial of the fostering changes programme K.s.C.L. National Academy for Parenting Research, Department for Education. London: Department for Education; 2012.
- 89.Jee SH, Couderc JP, Swanson D, Gallegos A, Hilliard C, Blumkin A, et al. A pilot randomized trial teaching mindfulness-based stress reduction to traumatized youth in foster care. Complement Ther Clin Pract. 2015;21(3):201–209. doi: 10.1016/j.ctcp.2015.06.007. [DOI] [PubMed] [Google Scholar]
- 90.Kirton D, Thomas C. A suitable case?: implementing multidimensional treatment foster care in an English local authority. Adopt Foster. 2011;35(2):5–17. doi: 10.1177/030857591103500202. [DOI] [Google Scholar]
- 91.Lee Bethany R, Phillips Danielle R, Steward Rochon K, Kerns Suzanne EU. Equipping TFC parents as treatment providers: findings from expert interviews. J Child Fam Stud. 2021;30(4):870–880. doi: 10.1007/s10826-020-01808-z. [DOI] [Google Scholar]
- 92.Lotty M, Bantry-White E, Dunn-Galvin A. The experiences of foster carers and facilitators of Fostering Connections: The Trauma-informed Foster Care Program: A process study. Child Youth Serv Rev. 2020;119:105516. 10.1016/j.childyouth.2020.105516.
- 93.McDermid S, Trivedi H, Holmes L, Boddy J. Foster carers’ receptiveness to new innovations and programmes: an example from the introduction of social pedagogy to UK Foster Care. Br J Soc Work. 2021.
- 94.Midgley N, Besser SJ, Fearon P, Wyatt S, Byford S, Wellsted D. The Herts and Minds study: feasibility of a randomised controlled trial of Mentalization-Based Treatment versus usual care to support the wellbeing of children in foster care. BMC Psychiatr. 2019;19(1). [DOI] [PMC free article] [PubMed]
- 95.Murray M, Culver T, Farmer E, Jackson Leslie A, Rixon B. From theory to practice: One agency's experience with implementing an evidence-based model. J Child Fam Stud. 2014;23(5):844–853. doi: 10.1007/s10826-013-9738-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Reddy Sheethal D, Negi Lobsang T, Dodson-Lavelle B, Ozawa-de Silva B, Pace Thaddeus WW, Cole Steve P, et al. Cognitive-based compassion training: a promising prevention strategy for at-risk adolescents. J Child Fam Stud. 2013;22(2):219–230. doi: 10.1007/s10826-012-9571-7. [DOI] [Google Scholar]
- 97.Schuurmans Angela AT, Nijhof Karin S, Rutger CMEE, Granic I. Using a Videogame intervention to reduce anxiety and externalizing problems among youths in residential care: an initial randomized controlled trial. J Psychopathol Behav Assess. 2018;40(2):344–354. doi: 10.1007/s10862-017-9638-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Silva IS, Gaspar MFF, Anglin JP. Webster-Stratton Incredible Years Basic Parent Programme (IY) in child care placements: Residential staff carers' satisfaction results. Child Fam Soc Work. 2016;21(2):198–208. doi: 10.1111/cfs.12129. [DOI] [Google Scholar]
- 99.Spencer R, Drew Alison L, Gowdy G, Horn JP. 'A positive guiding hand': a qualitative examination of youth-initiated mentoring and the promotion of interdependence among foster care youth. Child Youth Serv Rev. 2018;93:41–50. doi: 10.1016/j.childyouth.2018.06.038. [DOI] [Google Scholar]
- 100.Spielfogel Jill E, Leathers Sonya J, Christian E, McMeel LS. Parent management training, relationships with agency staff, and child mental health: Urban foster parents' perspectives. Child Youth Serv Rev. 2011;33(11):2366–2374. doi: 10.1016/j.childyouth.2011.08.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Taussig HN, Weiler LM, Garrido EF, Rhodes T, Boat A, Fadell M. A Positive Youth Development Approach to Improving Mental Health Outcomes for Maltreated Children in Foster Care: Replication and Extension of an RCT of the Fostering Healthy Futures Program. Am J Community Psychol. 2019;64(3-4):405-17. 10.1002/ajcp.12385. Epub 2019 Aug 30. [DOI] [PMC free article] [PubMed]
- 102.Triantafillou . Solution-focused parent groups: a new approach to the treatment of youth disruptive behavioural difficulties. 2002. [Google Scholar]
- 103.Turner-Halliday F, Kainth G, Young-Southward G, Cotmore R, Watson N, McMahon L, et al. Clout or doubt? Perspectives on an infant mental health service for young children placed in foster care due to abuse and neglect. Child Abuse Negl. 2017;72:184–195. doi: 10.1016/j.chiabu.2017.07.012. [DOI] [PubMed] [Google Scholar]
- 104.Turner-Halliday F, Watson N, Minnis H. Process evaluation of the New Orleans Intervention Model for infant mental health in Glasgow. Impact Evid Ser. 2016:69.
- 105.Vallejos Elvira P, Ball Mark J, Brown P, Crepaz-Keay D, Haslam-Jones E, Crawford P. Kundalini yoga as mutual recovery: a feasibility study including children in care and their carers. J Child Serv. 2016;11(4):261–282. doi: 10.1108/JCS-11-2015-0034. [DOI] [Google Scholar]
- 106.Walsh Natalia E Participant engagement in a foster parent training intervention. Diss Abstr Int B Sci Eng. 2017;77(12-B(E)):No-Specified. [Google Scholar]
- 107.Ziviani J, Darlington Y, Feeney R, Meredith P, Head B. Children with disabilities in out-of-home care: perspectives on organisational collaborations. Child Youth Serv Rev. 2013;35(5):797–805. doi: 10.1016/j.childyouth.2013.02.003. [DOI] [Google Scholar]
- 108.Alderson H, Kaner E, McColl E, Howel D, Fouweather T, McGovern R, et al. A pilot feasibility randomised controlled trial of two behaviour change interventions compared to usual care to reduce substance misuse in looked after children and care leavers aged 12–20 years: The SOLID study. PLoS ONE. 2020;15(9):e0238286. doi: 10.1371/journal.pone.0238286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Alderson H, McGovern R, Copello A, McColl E, Kaner E, Smart D, et al. Implementation factors for the delivery of alcohol and drug interventions to children in care: qualitative findings from the SOLID Feasibility Trial. Int J Environ Res Public Health. 2021;18(7). [DOI] [PMC free article] [PubMed]
- 110.Shklarski L. Understanding individual and organizational factors related to the implementation fidelity of the family finding intervention to support youth in foster care who are transitioning to independent living. Child Welfare. 2020;98(2):103–136. [Google Scholar]
- 111.Job AK, Ehrenberg D, Hilpert P, Reindl V, Lohaus A, Konrad K, et al. Taking Care Triple P for foster parents with young children in foster care: results of a 1-year randomized trial. J Interpers Violence. 2022;37(1–2):322–348. doi: 10.1177/0886260520909196. [DOI] [PubMed] [Google Scholar]
- 112.Dorsey S, Pullmann MD, Berliner L, Koschmann E, McKay M, Deblinger E. Engaging foster parents in treatment: a randomized trial of supplementing trauma-focused cognitive behavioral therapy with evidence-based engagement strategies. Child Abuse Negl. 2014;38(9):1508–1520. doi: 10.1016/j.chiabu.2014.03.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Geenen S, Powers Laurie E, Powers J, Cunningham M, McMahon L, Nelson M, et al. Experimental study of a self-determination intervention for youth in foster care. Career Dev Transit Except Individ. 2012;36(2):84–95. doi: 10.1177/2165143412455431. [DOI] [Google Scholar]
- 114.Leathers Sonya J, Spielfogel Jill E, McMeel Lorri S, Atkins MS. Use of a parent management training intervention with urban foster parents: a pilot study. Child Youth Serv Rev. 2011;33(7):1270–1279. doi: 10.1016/j.childyouth.2011.02.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Murphy K, Moore Kristin A, Redd Z, Malm K. Trauma-informed child welfare systems and children's well-being: a longitudinal evaluation of KVC's bridging the way home initiative. Child Youth Serv Rev. 2017;75:23–34. doi: 10.1016/j.childyouth.2017.02.008. [DOI] [Google Scholar]
- 116.Tullberg E, Vaughon W, Muradwij N, Kerker BD. Unpacking 'support': Understanding the complex needs of therapeutic foster parents. Child Youth Serv Rev. 2019;105:104420. doi: 10.1016/j.childyouth.2019.104420. [DOI] [Google Scholar]
- 117.Pasalich DS, Moretti MM, Hassall A, Curcio A. Pilot randomized controlled trial of an attachment- and trauma-focused intervention for kinship caregivers. Child Abuse Negl. 2021;120:105178. doi: 10.1016/j.chiabu.2021.105178. [DOI] [PubMed] [Google Scholar]
- 118.Maaskant Anne M, van R, Floor B, OverbeekGeertjan J, OortFrans J, Hermanns Jo MA. Parent training in foster families with children with behavior problems: follow-up results from a randomized controlled trial. Child Youth Serv Rev. 2016;70:84–94. doi: 10.1016/j.childyouth.2016.09.005. [DOI] [Google Scholar]
- 119.McMillen JC, Narendorf SC, Robinson D, Havlicek J, Fedoravicius N, Bertram J, et al. Development and piloting of a treatment foster care program for older youth with psychiatric problems. Child Adolesc Psychiatr Mental Health. 2015;9(1). [DOI] [PMC free article] [PubMed]
- 120.Adkins T, Reisz S, Hasdemir D, Fonagy P. Family Minds: A randomized controlled trial of a group intervention to improve foster parents’ reflective functioning. Dev Psychopathol. 2022;34(3):1177-91. [DOI] [PubMed]
- 121.Akin BA, Lang K, Yan YQ, McDonald TP. Randomized trial of PMTO in foster care: 12-month child well-being, parenting, and caregiver functioning outcomes. Child Youth Serv Rev. 2018;95:49–63. doi: 10.1016/j.childyouth.2018.10.018. [DOI] [Google Scholar]
- 122.Akin Becci A, Lang K, McDonald Thomas P, Yan Y, Little T. Randomized trial of PMTO in foster care: six-month child well-being outcomes. Res Soc Work Pract. 2019;29(2):206–222. doi: 10.1177/1049731516669822. [DOI] [Google Scholar]
- 123.Betzalel N, Shechtman Z. Bibliotherapy treatment for children with adjustment difficulties: a comparison of affective and cognitive bibliotherapy. J Creat Ment Health. 2010;5(4):426–439. doi: 10.1080/15401383.2010.527816. [DOI] [Google Scholar]
- 124.Bittman B, Dickson L, Coddington K. Creative musical expression as a catalyst for quality-of-life improvement in inner-city adolescents placed in a court-referred residential treatment program. Adv Mind Body Med. 2009;24(1):8–19. [PubMed] [Google Scholar]
- 125.Clark Hewitt B, Prange Mark E, Lee B, Boyd LA, McDonald Beth A, Stewart ES. Improving adjustment outcomes for foster children with emotional and behavioral disorders: early findings from a controlled study on individualized services. Special Ser Center Mental Health Serv Res Proj. 1994;2(4):207–218. [Google Scholar]
- 126.Dozier M, Peloso E, Lindhiem O, Gordon MK, Manni M, Sepulveda S, et al. Developing evidence-based interventions for foster children: an example of a randomized clinical trial with infants and toddlers. J Soc Issues. 2006;62(4):767–785. doi: 10.1111/j.1540-4560.2006.00486.x. [DOI] [Google Scholar]
- 127.Farmer EMZ, Burns BJ, Wagner HR, Murray M, Southerland DG. Enhancing 'usual practice' treatment foster care: findings from a randomized trial on improving youths' outcomes. Psychiatr Serv. 2010;61(6):555–561. doi: 10.1176/ps.2010.61.6.555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Green JM, Biehal N, Roberts C, Dixon J, Kay C, Parry E, et al. Multidimensional Treatment Foster Care for Adolescents in English care: randomised trial and observational cohort evaluation. Br J Psychiatry. 2014;204(3):214–221. doi: 10.1192/bjp.bp.113.131466. [DOI] [PubMed] [Google Scholar]
- 129.Jonkman Caroline S, Schuengel C, Oosterman M, Lindeboom R, Boer F, Lindauer Ramon JL. Effects of Multidimensional Treatment Foster Care for Preschoolers (MTFC-P) for Young Foster Children with Severe Behavioral Disturbances. J Child Fam Stud. 2017;26(5):1491–1503. doi: 10.1007/s10826-017-0661-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Linares LO, Montalto D, Li M, Oza VS. A promising parenting intervention in foster care. J Consult Clin Psychol. 2006;74(1):32–41. doi: 10.1037/0022-006X.74.1.32. [DOI] [PubMed] [Google Scholar]
- 131.Lipscomb ST, Pratt ME, Schmitt SA, Pears KC, Kim HK. School readiness in children living in non-parental care: Impacts of Head Start. J Appl Dev Psychol. 2013;34(1):28–37. doi: 10.1016/j.appdev.2012.09.001. [DOI] [Google Scholar]
- 132.Maaskant Anne M, van R. Floor B, OverbeekGeertjan J, OortFrans J, Arntz M, et al. Effects of PMTO in foster families with children with behavior problems: a randomized controlled trial. J Child Fam Stud. 2017;26(2):523–39. doi: 10.1007/s10826-016-0579-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Marquis R. The gender effects of a foster parent-delivered tutoring program on foster children's academic skills and mental health: a randomized field trial. Diss Abstr Int A Humanit Soc Sci. 2014;75(1-A(E)):No-Specified. [Google Scholar]
- 134.Mersky Joshua P, Topitzes J, Grant-Savela Stacey D, Brondino Michael J, McNeil CB. Adapting parent-child interaction therapy to foster care: outcomes from a randomized trial. Res Soc Work Pract. 2016;26(2):157–167. doi: 10.1177/1049731514543023. [DOI] [Google Scholar]
- 135.Messer EP, Greiner MV, Beal SJ, Eismann EA, Cassedy A, Gurwitch RH, et al. Child adult relationship enhancement (CARE): a brief, skills-building training for foster caregivers to increase positive parenting practices. Child Youth Serv Rev. 2018;90:74–82. doi: 10.1016/j.childyouth.2018.05.017. [DOI] [Google Scholar]
- 136.Minnis H, Pelosi AJ, Knapp M, Dunn J. Mental health and foster carer training. Arch Dis Child. 2001;84(4):302–306. doi: 10.1136/adc.84.4.302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Moody G, Coulman E, Brookes-Howell L, Cannings-John R, Channon S, Lau M, et al. A pragmatic randomised controlled trial of the fostering changes programme. Child Abuse Negl. 2020;108:104646. doi: 10.1016/j.chiabu.2020.104646. [DOI] [PubMed] [Google Scholar]
- 138.N'Zi A, Stevens ML, Eyberg SM. Child Directed Interaction Training for young children in kinship care: A pilot study. Child Abuse Negl. 2016;55:81–91. doi: 10.1016/j.chiabu.2016.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Oxford Monica L, Marcenko M, Fleming Charles B, Lohr Mary J, Spieker SJ. Promoting birth parents' relationships with their toddlers upon reunification: results from Promoting First Relationships home visiting program. Child Youth Serv Rev. 2016;61:109–116. doi: 10.1016/j.childyouth.2015.12.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Price JM, Roesch S, Walsh NE, Landsverk J. Effects of the KEEP Foster Parent Intervention on child and sibling behavior problems and parental stress during a randomized implementation trial. Prev Sci. 2015;16(5):685–695. doi: 10.1007/s11121-014-0532-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Price Joseph M, Roesch S, Burce CM. The effects of the KEEP foster parent training intervention on child externalizing and internalizing problems. Dev Child Welfare. 2019;1(1):5–21. doi: 10.1177/2516103218812092. [DOI] [Google Scholar]
- 142.Smith Dana K, Leve Leslie D, Chamberlain P. Preventing internalizing and externalizing problems in girls in foster care as they enter middle school: impact of an intervention. Prev Sci. 2011;12(3):269–277. doi: 10.1007/s11121-011-0211-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Sprang G. The efficacy of a relational treatment for maltreated children and their families. Child Adolesc Mental Health. 2009;14(2):81–88. doi: 10.1111/j.1475-3588.2008.00499.x. [DOI] [Google Scholar]
- 144.Taussig HN, Culhane SE. Impact of a mentoring and skills group program on mental health outcomes for maltreated children in foster care. Arch Pediatr Adolesc Med. 2010;164(8):739–746. doi: 10.1001/archpediatrics.2010.124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Van H, Frank. Vanderfaeillie J, Omer H, Vanschoonlandt F. Training in nonviolent resistance for foster parents: a randomized controlled trial. Res Soc Work Pract. 2018;28(8):931–42. doi: 10.1177/1049731516662915. [DOI] [Google Scholar]
- 146.Vandivere S, Malm KE, Allen TJ, Williams SC, McKlindon A. A randomized controlled trial of family finding: a relative search and engagement intervention for youth lingering in foster care. Eval Rev. 2017;41(6):542–567. doi: 10.1177/0193841X17689971. [DOI] [PubMed] [Google Scholar]
- 147.Bellamy J. The benefits of outpatient mental health services for children in long-term foster care. Mental Health Services for Vulnerable Children and Young People: Supporting Children Who are, or Have Been, in Foster Care. 2013. pp. 21–36. [Google Scholar]
- 148.Bronz Kimberly D. Effects of a therapeutic playgroup intervention on the social competence and executive functioning of young children in foster care. Diss Abstr Int A Humanit Soc Sci. 2004;65(6-A):2082. [Google Scholar]
- 149.Greeno Elizabeth J, Lee Bethany R, Uretsky Mathew C, Moore Jessica E, Barth Richard P, Shaw TV. Effects of a foster parent training intervention on child behavior, caregiver stress, and parenting style. J Child Fam Stud. 2016;25(6):1991–2000. doi: 10.1007/s10826-015-0357-6. [DOI] [Google Scholar]
- 150.Hayduk I. The Effect of Kinship Placement Laws on Foster Children's Well-Being. BE J Econ Anal Policy. 2017;17(1).
- 151.Izzo CV, Smith EG, Holden MJ, Norton CI, Nunno MA, Sellers DE. Intervening at the Setting Level to Prevent Behavioral Incidents in Residential Child Care: Efficacy of the CARE Program Model. Prev Sci. 2016;17(5):554–564. doi: 10.1007/s11121-016-0649-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152.Kessler RC, Pecora PJ, Williams J, Hiripi E, O'Brien K, English D, et al. Effects of enhanced foster care on the long-term physical and mental health of foster care alumni. Arch Gen Psychiatry. 2008;65(6):625–633. doi: 10.1001/archpsyc.65.6.625. [DOI] [PubMed] [Google Scholar]
- 153.Leloux-Opmeer H, Kuiper C, Swaab H, Scholte E. Similarities and differences in the psychosocial development of children placed in different 24-h settings. J Child Fam Stud. 2018;27(4):1299–1310. doi: 10.1007/s10826-017-0955-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Leon Scott C, Saucedo Deborah J, Jachymiak K. Keeping it in the family: The impact of a Family Finding intervention on placement, permanency, and well-being outcomes. Child Youth Serv Rev. 2016;70:163–170. doi: 10.1016/j.childyouth.2016.09.020. [DOI] [Google Scholar]
- 155.Livheim F, Tengström A, Andersson G, Dahl J, Björck C, Rosendahl I. A quasi-experimental, multicenter study of acceptance and commitment therapy for antisocial youth in residential care. J Contextual Behav Sci. 2020;16:119–127. doi: 10.1016/j.jcbs.2020.03.008. [DOI] [Google Scholar]
- 156.Lotty M, Dunn-Galvin A, Bantry-White E. Effectiveness of a trauma-informed care psychoeducational program for foster carers - Evaluation of the Fostering Connections Program. Child Abuse Neglect. 2020;102. [DOI] [PubMed]
- 157.McCrae Julie S, Lee Bethany R, Barth Richard P, Rauktis ME. Comparing three years of well-being outcomes for youth in group care and nonkinship foster care. Child Welfare. 2010;89(2):229–249. [PubMed] [Google Scholar]
- 158.Muela A, Balluerka N, Amiano N, Caldentey Miguel A, Aliri J. Animal-assisted psychotherapy for young people with behavioural problems in residential care. Clin Psychol Psychother. 2017;24(6):O1485–O1494. doi: 10.1002/cpp.2112. [DOI] [PubMed] [Google Scholar]
- 159.Portwood Sharon G, et al. A comparison of outcomes for children and youth in foster and residential group care across agencies. Child Youth Serv Rev. 2018;85:19–25. doi: 10.1016/j.childyouth.2017.11.027. [DOI] [Google Scholar]
- 160.Pozo-Breen A. The effectiveness of individualized and rehabilitative therapies for children in foster care. Diss Abstr Int B Sc Eng. 2018;79(1-B(E)):No-Specified. [Google Scholar]
- 161.Price Joseph M, Roesch S, Walsh NE. Effectiveness of the KEEP Foster Parent Intervention during an implementation trial. Child Youth Serv Rev. 2012;34(12):2487–2494. doi: 10.1016/j.childyouth.2012.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162.Rivard Jeanne C, Bloom Sandra L, Abramovitz R, Pasquale Lina E, Duncan M, McCorkle D, et al. Assessing the implementation and effects of a trauma-focused intervention for youths in residential treatment. Psychiatr Q. 2003;74(2):137–154. doi: 10.1023/A:1021355727114. [DOI] [PubMed] [Google Scholar]
- 163.Scholte EM, van der P, J D Residential treatment of adolescents with severe behavioural problems. J Adolesc. 2006;29(4):641–54. doi: 10.1016/j.adolescence.2005.05.010. [DOI] [PubMed] [Google Scholar]
- 164.Silva Ana D, Coelho P, do Ceu T. Effectiveness of a career intervention for empowerment of institutionalized youth. Vulnerable Child Youth Stud. 2017;12(2):171–81. doi: 10.1080/17450128.2017.1282070. [DOI] [Google Scholar]
- 165.Timmer Susan G, Urquiza Anthony J, Zebell N. Challenging foster caregiver–maltreated child relationships: The effectiveness of parent–child interaction therapy. Child Youth Serv Rev. 2006;28(1):1–19. doi: 10.1016/j.childyouth.2005.01.006. [DOI] [Google Scholar]
- 166.Williams Nathaniel J, Sherr ME. Children's psychosocial rehabilitation: Clinical outcomes for youth with serious emotional disturbance living in foster care. Child Adolesc Soc Work J. 2009;26(3):225–234. doi: 10.1007/s10560-008-0160-y. [DOI] [Google Scholar]
- 167.Wood JN, Dougherty SL, Long J, Messer EP, Rubin D. A pilot investigation of a novel intervention to improve behavioral well-being for children in foster care. J Emot Behav Disord. 2019;27(1):3–13. doi: 10.1177/1063426617733715. [DOI] [Google Scholar]
- 168.Pereira AI, Ferreira C, Oliveira M, Evangelista ES, Ferreira J, Roberto MS, et al. Effectiveness of a combined surf and psychological preventive intervention with children and adolescents in residential childcare: a randomized controlled trial. Revista de Psicología Clínica con Niños y Adolescentes. 2020;7(2):22–31. doi: 10.21134/rpcna.2020.07.2.3. [DOI] [Google Scholar]
- 169.Suomi A, Lucas N, McArthur M, Humphreys C, Dobbins T, Taplin S. Cluster randomized controlled trial (RCT) to support parental contact for children in out-of-home care. Child Abuse Negl. 2020;109:104708. doi: 10.1016/j.chiabu.2020.104708. [DOI] [PubMed] [Google Scholar]
- 170.Yan Y, De Luca S. Heterogeneity of treatment effects of PMTO in foster care: a latent profile transition analysis. J Child Fam Stud. 2021;30(1):17–28. doi: 10.1007/s10826-020-01798-y. [DOI] [Google Scholar]
- 171.Johnson S, Pryce J. ZM. The role of therapeutic mentoring in enhancing outcomes for youth in foster care. Child Welfare. 2010;90(5):51–69. [PubMed] [Google Scholar]
- 172.Mersky JP, Topitzes J, Janczewski CE, Lee C-TP, McGaughey G, McNeil CB. Translating and Implementing Evidence-Based Mental Health Services in Child Welfare. Adm Policy Mental Health ServRes. 2020;47(5):693–704. doi: 10.1007/s10488-020-01011-8. [DOI] [PubMed] [Google Scholar]
- 173.Boyd KA, Balogun MO, Minnis H. Development of a radical foster care intervention in Glasgow Scotland. Health Promotion Int. 2016;31(3):665–673. doi: 10.1093/heapro/dav041. [DOI] [PubMed] [Google Scholar]
- 174.Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348:g1687. doi: 10.1136/bmj.g1687. [DOI] [PubMed] [Google Scholar]
- 175.Baginsky M, Moriarty J, Manthorpe J, Ougrin D, Middleton K. Evaluation of the Early Implementation of the New Orleans Intervention Model in a London Borough. London: Department for Education; 2017. [Google Scholar]
- 176.Tullberg E, Vaughon W, Muradwij N, Kerker BD. Unpacking 'support': Understanding the complex needs of therapeutic foster parents. Child Youth Serv Rev. 2019;105:104420. doi: 10.1016/j.childyouth.2019.104420. [DOI] [Google Scholar]
- 177.Maden M, Cunliffe A, McMahon N, Booth A, Carey GM, Paisley S, et al. Use of programme theory to understand the differential effects of interventions across socio-economic groups in systematic reviews—a systematic methodology review. Syst Rev. 2017;6(1):266. doi: 10.1186/s13643-017-0638-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 178.Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. bmj. 2021;374. [DOI] [PMC free article] [PubMed]
- 179.Waid J, Uhrich M. A scoping review of the theory and practice of positive youth development. Br J Soc Work. 2020;50(1):5–24. [Google Scholar]
- 180.Bowlby J, Ainsworth M. The origins of attachment theory. Attach Theory Soc Dev Clin Perspect. 2013;45(28):759–775. [Google Scholar]
- 181.Bandura A, Walters RH. Social learning theory: Englewood cliffs Prentice Hall. 1977. [Google Scholar]
- 182.Biehal N, Dixon J, Parry E, Sinclair I, Green J, Roberts C, et al. The Care Placements Evaluation (CaPE) Evaluation of Multidimensional Treatment Foster Care for Adolescents (MTFC-A) 2012. [Google Scholar]
- 183.Isrctn. The Fostering Changes programme. http://www.whoint/trialsearch/Trial2aspx?TrialID=ISRCTN58581840. 2011.
- 184.Mezey G, Meyer D, Robinson F, Bonell C, Campbell R, Gillard S, et al. Developing and piloting a peer mentoring intervention to reduce teenage pregnancy in looked-after children and care leavers: an exploratory randomised controlled trial. Health Technol Assess. 2015;19(85). [DOI] [PMC free article] [PubMed]
- 185.Kirton D, Thomas C. A Suitable Case?: Implementing Multidimensional Treatment Foster Care in an English Local Authority. Adopt Foster. 2011;35:5–17. doi: 10.1177/030857591103500202. [DOI] [Google Scholar]
- 186.Lotty M, Bantry-White E, Dunn-Galvin A. The experiences of foster carers and facilitators of Fostering Connections: The Trauma-informed Foster Care Program: a process study. Child Youth Serv Rev. 2020;119:105516. doi: 10.1016/j.childyouth.2020.105516. [DOI] [Google Scholar]
- 187.National Institute for Health and Care Excellence. Looked-after children and young people: interventions to promote physical, mental, and emotional health and wellbeing of lookedafter children, young people and care leavers. NICE guideline. NG205.: Public Health England; 2021. [PubMed]
- 188.Wu Q, Zhu Y, Ogbonnaya I, Zhang S, Wu S. Parenting intervention outcomes for kinship caregivers and child: a systematic review. Child Abuse Negl. 2020;106:104524. doi: 10.1016/j.chiabu.2020.104524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 189.Bergström M, Cederblad M, Håkansson K, Jonsson AK, Munthe C, Vinnerljung B, et al. Interventions in foster family care: a systematic review. Res Soc Work Pract. 2020;30(1):3–18. doi: 10.1177/1049731519832101. [DOI] [Google Scholar]
- 190.Tarren-Sweeney M. A narrative review of mental and relational health interventions for children in family-based out-of-home care. J Fam Ther. 2021;43(3):376–391. doi: 10.1111/1467-6427.12341. [DOI] [Google Scholar]
- 191.Barth RP, Berrick JD, Garcia AR, Drake B, Jonson-Reid M, Gyourko JR, et al. Research to consider while effectively re-designing child welfare services. Res Soc Work Pract. 2021;32(5):483–498. doi: 10.1177/10497315211050000. [DOI] [Google Scholar]
- 192.Russell DH, Trew S, Higgins DJ. Vulnerable yet forgotten? A systematic review identifying the lack of evidence for effective suicide interventions for young people in contact with child protection systems. Am J Orthopsychiatry. 2021;91:647–659. doi: 10.1037/ort0000555. [DOI] [PubMed] [Google Scholar]
- 193.Ranzato E, Austerberry C, Besser SJ, Cirasola A, Midgley N. A qualitative analysis of goals set by foster carers seeking support for their child’s emotional well-being. Adopt Foster. 2021;45(1):7–21. doi: 10.1177/0308575921991951. [DOI] [Google Scholar]
- 194.Evans R, Katz CC, Fulginiti A, Taussig H. Sources and types of social supports and their association with mental health symptoms and life satisfaction among young adults with a history of out-of-home care. Children. 2022; 9(4). [DOI] [PMC free article] [PubMed]
- 195.O'Neill J, Tabish H, Welch V, Petticrew M, Pottie K, Clarke M, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol. 2014;67(1):56–64. doi: 10.1016/j.jclinepi.2013.08.005. [DOI] [PubMed] [Google Scholar]
- 196.Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ : British Medical Journal. 2015;350:h1258. doi: 10.1136/bmj.h1258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 197.El-Banna A, Petrou S, Yiu HHE, Daher S, Forrester D, Scourfield J, et al. Systematic review of economic evaluations of children’s social care interventions. Child Youth Serv Rev. 2021;121:105864. doi: 10.1016/j.childyouth.2020.105864. [DOI] [Google Scholar]
- 198.Pfadenhauer LM, Gerhardus A, Mozygemba K, Lysdahl KB, Booth A, Hofmann B, et al. Making sense of complexity in context and implementation: the Context and Implementation of Complex Interventions (CICI) framework. Implement Sci. 2017;12(1):21. doi: 10.1186/s13012-017-0552-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 199.Booth A, Moore G, Flemming K, Garside R, Rollins N, Tunçalp Ö, et al. Taking account of context in systematic reviews and guidelines considering a complexity perspective. BMJ Glob Health. 2019;4(Suppl 1):e000840. doi: 10.1136/bmjgh-2018-000840. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data extraction, analysis and synthesis are available from the corresponding author on reasonable request.