

Abstract
Background and aims. The popularity of playing games among adolescents has increased during the last decades, possibly affecting the prevalence of problematic gaming behavior. The current study aimed to compare country-level prevalence rates of adolescents' problematic gaming behavior in five countries and identify cross-cultural similarities and differences in the relationship between problematic gaming and well-being (life satisfaction, psychological complaints, and peer support). Methods. Cross-national data from the Health Behavior in School-aged Children (HBSC) study were used. The sample comprised 14,398 gamers (61% boys) aged 11 to 16 (average age between 13.31 and 13.85) from Azerbaijan, England, Serbia, Slovenia, and the Netherlands. Results. The findings showed that the prevalence of problematic gaming differs between countries. The highest prevalence of problematic gaming was seen in Azerbaijan (16.1%) and the lowest in the Netherlands (4.3%). In contrast, Azerbaijan reported the lowest gaming intensity, whereas the Netherlands and England showed the highest gaming intensity. Additional analyses revealed that problematic gaming was associated with lower life satisfaction, more psychological complaints, and lower peer support in all countries, although the strength of these associations varied between countries. Discussion and conclusions. The current study's results are consistent with the assumption that problematic gaming negatively affects adolescents' social and mental well-being. These findings are further discussed in light of the normalization theory which suggests that cultural gaming norms (i.e., the percentage of gamers per country) would influence the strength of the relationship between problematic gaming and adolescents' well-being. The present findings highlight the need for adequate prevention strategies aiming at problematic gaming among youngsters.
Keywords: problematic gaming, cross-national, peer support, life satisfaction, psychological complaints
Introduction
Gaming as an addiction
Digital games continue to be one of the most popular forms of entertainment. According to European data, 79% of children (6 to 14-years old) play games regularly (ISFE, 2020). Similar numbers are reported in North American surveys, with 70% of children and adolescents under 18 playing games regularly (ESA, 2020). These numbers illustrate that games have been adopted into households and integrated into the youth culture worldwide. However, the popularity of playing games among adolescents is accompanied by increased parental concern about the amount of time their adolescents spend on games. Studies have shown that playing games for several hours a day is not necessarily problematic (Brunborg et al., 2013, 2014; Király, Sleczka, et al., 2017; Spekman, Konijn, Roelofsma, & Griffiths, 2013; Van Den Eijnden, Koning, Doornwaard, Van Gurp, & Ter Bogt, 2018). For instance, Van Den Eijnden et al. (2018) show that number of hours spent gaming has no negative effect among adolescents when controlling for problematic gaming symptoms. For some outcomes, hours spent gaming may even be beneficial, for instance for perceived social competence.
However, a small proportion of youth struggle with keeping their gaming behavior under control, even when they experience negative consequences due to their gaming. These adolescents have developed addictive-like gaming behavior, referred to as problematic gaming. Problematic gaming is characterized by symptoms similar to other substance or behavioral addictions, such as conflict with family members, unsuccessful attempts to stop gaming and problems in school- or work-related contexts (Pontes & Griffiths, 2015).
Definition of problematic gaming in an international context
The prevalence of problematic gaming varies greatly across countries (Mihara & Higuchi, 2017). For example, the prevalence rates of problematic gaming range between 0.7% in a Norwegian study and 27.5% in a French study (Mihara & Higuchi, 2017). However, no strong inferences can or should be made based on these previous data, as there are large discrepancies between used samples (e.g., age, education level), research designs, and operationalizations of problematic gaming. As far as we know only one study compared self-perceived gaming problems between countries. More specifically, the European School Survey Project on Alcohol and Other Drugs (ESPAD; ESPAD Group, 2020) measured 3 self-perceived problems with gaming amongst 15- to 16-year-old European students (Colasante et al., 2022). The conceptualization of gaming problems in this study, however, was not based on diagnostic criteria for gaming addiction, and can only be interpreted as a self-perceived risk of problematic gaming. Because of these methodological and conceptual inconsistencies, it is currently impossible to draw conclusions about cross-country differences in the prevalence of problematic gaming.
The inconsistent conceptualizations of problematic gaming result, to a large extent, from a lack of scientific and diagnostic consensus. Whereas the Diagnostic Statistical Manual (DSM-5, 2013) does not officially recognize Internet Gaming Disorder yet and describes it as a condition warranting more clinical research before it can be considered a formal disorder, the World Health Organization (WHO) has already recognized Gaming Disorder as a formal diagnosis in the 11th revision of the International Classification of Diseases (ICD-11) in 2018 (World Health Organization, 2018). Moreover, whereas the DSM-5 describes nine criteria, of which at least five criteria should be met to classify someone as suffering from Internet Gaming Disorder, the ICD-11 provides a general definition of Gaming Disorder as a pattern of gaming behavior characterized by impaired control over gaming, increasing priority given to gaming over other activities to the extent that gaming takes precedence over other interests and daily activities, and continuation or escalation of gaming despite the occurrence of negative consequences.
In addition, previous studies have used very different measurement instruments to assess problematic gaming behavior, such as the Internet Gaming Disorder Test (IGD-20 Test; Pontes, Király, Demetrovics, & Griffiths, 2014), the Ten-Item Internet Gaming Disorder Test (IGDT-10; Király, Sleczka, et al., 2017), the Internet Gaming Disorder Scale–Short Form (IGDS9-SF; Pontes & Griffiths, 2015), and several others (for a more extensive summary, see Pontes et al., 2021). The current study aimed to address this methodological problem by administering the same measurement instrument, i.e., the IGD scale (Lemmens, Valkenburg, & Gentile, 2015) based on DSM-5 criteria, in five different countries. Moreover, the same sampling techniques and inclusion criteria were used in these five countries to reach and include a representative sample of adolescents to obtain more reliable estimates of differences in cross-country prevalence rates of problematic gaming. The IGD scale is a valid and reliable measure of problematic gaming behavior (Lemmens et al., 2015) but should not be used as a diagnostic instrument for clinical use.
Consequences of problematic gaming
Despite an ongoing scholarly debate about the conceptualization of problematic gaming, evidence that problematic gaming is associated with negative outcomes for healthy youth development is increasing. Cross-sectional studies have linked problematic gaming with negative outcomes, such as feeling down, irritability, exhaustion (Brunborg et al., 2013), and depression (Männikkö, Billieux, & Kääriäinen, 2015). Recent meta-analyses have shown that problematic gaming correlates with psychological problems (Cheng, Cheung, & Wang, 2018; Dullur, Krishnan, & Diaz, 2020; Männiko et al., 2020), difficulties in social functioning (Cheng et al., 2018) and impulsivity (Şalvarlı & Griffiths, 2019). Moreover, longitudinal findings suggest that problematic gaming predicts lower life satisfaction and a lower perceived social competence over time (Van Den Eijnden et al., 2018), as well as anxiety and school-related problems (Gentile et al., 2011). The negative consequences of problematic gaming may, thus, severely affect and hinder adolescents' development.
Normalization theory
The implications of problematic gaming should be seen in light of cross-cultural differences. According to the normalization theory, risk behaviors that most people in a certain culture or society accept become normalized and are no longer viewed as problematic (Boer et al., 2020; Haskuka, Arenliu, & Kelmendi, 2018). The normalization theory originally focused on substances use but has since been shown to be applicable to other behaviors as well (Boer et al., 2020). It may be that the cultural or societal acceptance of gaming influences whether young gamers experience certain gaming behaviors as problematic and may, consequently, influence the relationship between reported symptoms of problematic gaming and the well-being of individual gamers. Considering the abovementioned, we assume that in countries where gaming is a mainstream part of the youth culture, i.e., the percentage of gamers is high, the strength of associations between problematic gaming and negative well-being outcomes will be lower than in countries where gaming is less common.
The current study
The current study had three aims. First, cross-country differences in the prevalence of problematic gaming were investigated in five European countries. Second, the overall relationship between problematic gaming and three mental and social well-being indicators (life satisfaction, psychological complaints, and peer support) was tested. Third, possible cross-country differences in the associations between problematic gaming and mental and social well-being were examined. Additionally, we tested whether these country-level associations depend on the national gaming context, specifically on the country's prevalence rates of (problematic) gaming behavior, as suggested by the normalization theory.
Methods
Sample and procedure
We used cross-national data from the 2017/2018 HBSC study. This school-based study monitored adolescent health and well-being in several countries across Europe, North America, and the Middle East.
The current study included five of the eight countries that applied the optional package for gaming questionnaires. Turkey was excluded as the gaming data were only obtained from participants with a limited age range, Georgia was excluded due to the absence of data on problematic gaming and Estonia had no data on gaming intensity and was therefore excluded.
The analyzed sample consisted of 14,398 adolescent gamers (61% boys; meanage = 13.47, standard deviationage = 1.61). Sampling methods, data collection, and questionnaires were standardized using a standard protocol (Inchley, Currie, Cosma, & Samdal, 2018). This protocol included sampling, data collection and data management procedures. Sampling procedures may vary per country, but generally aim to provide a nationally representative sample. Data was collected through self-administered questionnaires in classrooms. Researchers translated questionnaires from English to the native language of the respective countries. These translations were back-translated into English and compared to the original. A specialized translation team inspected each item and corrected inconsistencies to ensure minimal measurement variation across countries. Research has validated the questionnaires in each of the participating countries (Heinz et al., 2022). Participation was voluntary and anonymous. Verbal or written consent was obtained from both the child and the parents before participation.
Measures
Problematic gaming
Symptoms of problematic gaming behavior were measured using the dichotomous 9-item Internet Gaming Disorder Scale (Lemmens et al., 2015) which was based on the nine Internet Gaming Disorder criteria described in the appendix of the DSM-5 (APA, 2013). With these nine items, participants indicated whether they experienced symptoms such as conflict with parents, preoccupation, or loss of control (for a full list, see Lemmens et al., 2015). Responses were either 1) yes or 0) no. Higher scores indicate more problematic gaming symptoms. In line with the DSM-5 definition, participants who indicated to be experiencing five or more IGD symptoms were considered as problematic gamers (Lemmens et a., 2015). The scale's internal consistency was good (Cronbach's α = 0.81).
Life satisfaction
Using the Cantril Ladder (Cantril, 1965), the participants rated their overall life satisfaction on a scale ranging from 0) worst possible life to 10) best possible life. A previous study showed good reliability of this measure and good convergent validity with other well-being measures (Levin & Currie, 2014). Higher scores indicate higher life satisfaction.
Psychological complaints
As part of the HBSC Symptoms Checklist (HBSC-SCL; Haugland & Wold, 2001), the participants indicated the extent to which they experienced the following psychological complaints: feeling low, irritability, nervousness, and difficulty sleeping. Answers ranged from 0) about every day to 5) rarely or never. Means were calculated after the items were rescaled, so higher scores represented more psychological complaints. The internal consistency of this scale was good (Cronbach's α = 0.77).
Peer support
Peer support was assessed using four items that were part of a subscale of the Multidimensional Scale of Perceived Social Support (MSPSS; Zimet, Dahlem, Zimet, & Farley, 1988). An example question is, “My friends really try to help me.” Items were measured on a scale from 0) very strongly disagree to 7) very strongly agree, with higher scores indicating more perceived peer support. The internal consistency of this scale was good (Cronbach's α = 0.91).
Control variables
The analyses controlled for age, gender, social and economic status (SES), and gaming intensity. SES was measured using the third version of the HBSC Family Affluence Scale (FAS III). This scale included six items measuring the material possessions of participants' families, home characteristics (e.g., number of bedrooms and bathrooms), and family holidays. These items were used to create a percentile score for each participant relative to their country. These scores were categorized into the lowest 20%, middle 60%, and highest 20%.
Gaming intensity was measured with two items. Participants indicated the average number of days and hours per day they spent playing games during a week. Responses ranged from 1) (almost) never to 6) (almost) every day and from 1) one to two h to 5) 8 h or more, respectively. Next, the answer categories were recoded to represent average days h−1 spent playing games. These two recoded variables were multiplied to indicate the weekly gaming hours.
Statistical analyses
Missing data
The total HBSC sample consisted of 24,970 adolescents. Participants who indicated they had (almost) never played games had the option (but were not required) to skip any subsequent gaming-related questions. This resulted in a relatively large number of non-responses on the gaming items. Therefore, participants who had (almost) never played games were coded as non-gamers and excluded from the analyses (N = 5,913; see Table 1 for a distribution of non-gamers per country). After exclusion, the remaining 14,398 made up the analysis sample.
Table 1.
Descriptive statistics for the analysis sample
| Netherlands | Slovenia | Serbia | England | Azerbaijan | |
| Non-gamers1 | 1,207 (26%) | 1,417 (28%) | 1,106 (30% | 391 (14%) | 1,792 (44%) |
| Gamers | 3,479 (74%) | 3,622 (72%) | 2,591 (70%) | 2,429 (86%) | 2,277 (66%) |
| Life satisfaction2 | 7.84 | 7.98 | 8.28 | 7.51 | 8.30 |
| Psychol. Complaints3 | 2.09 | 2.16 | 2.04 | 2.45 | 1.75 |
| Peer support4 | 5.70 | 5.12 | 5.35 | 4.49 | 5.08 |
| Gaming intensity5 | 12.49 | 10.14 | 12.36 | 13.90 | 6.71 |
| Gender (boys %) | 61% | 62% | 61% | 58% | 54% |
| Age | 13.32 | 13.53 | 13.85 | 13.36 | 13.31 |
Note. 1 These participants were excluded from all analyses.
2 Measured on a scale from 1 to 10, with higher scores indicate more life satisfaction.
3 Measured on a scale from 0 to 5, with higher score indicating more psychological complaints.
4 Measured on a scale from 0 to 7, with higher scores indicating more experienced peer support.
5 Average hours spent gaming per week.
Analysis strategy
The statistical analyses were performed using SPSS. First, descriptive statistics of all study variables were analyzed for each country. Next, country-prevalence rates of problematic gaming were calculated. For these prevalence rates, problematic gaming was dichotomized based on the defined cut-off point for the IGD scale (Lemmens et al., 2015). The country-prevalence gaming rates were calculated as the percentage of participants who indicated playing games at least once a week. Next, Pearson correlations were computed between the variables of interest. To measure the differences between the countries' problematic gaming, an ANOVA with post-hoc test was used.
Due to the small number of countries in the sample, it was impossible to apply multilevel models at the country level, as a small number of groups may cause the estimates of group-level effects to be unreliable (Bryan & Jenkins, 2016; Hox, 2010). Therefore, to test the associations between problematic gaming and well-being, hierarchical regression analyses were performed with problematic gaming as a (continuous) predictor of the three mental and social well-being indicators (life satisfaction, psychological complaints, peer support) while controlling for age, gender, SES, and gaming intensity. Age, gender, and SES can be expected to influence problematic gaming (Stevens, Dorstyn, Delfabbro, & King, 2021) and/or adolescents' well-being (Quon & McGrath, 2014); therefore, they were used as control variables. As mentioned previously, although high gaming intensity often correlates with problematic gaming, it may not lead to problematic behavior (Brunborg et al., 2013, 2014; Király, Sleczka, et al., 2017; Spekman et al., 2013; Van Den Eijnden et al., 2018). Moreover, to confirm that problematic gaming behavior rather than the high intensity of gaming is associated with well-being, gaming intensity was added as a confounding variable to all analyses that included problematic gaming.
In the hierarchical regression analyses, the control variables were entered in the first step, and problematic gaming was entered in the second step. Next, to test the normalization hypothesis, country-prevalence rates of gaming and interaction terms between problematic gaming and country-prevalence rates of gaming were entered in the third step. Due to the large sample size of this study, a significance level of p < 0.001 was adopted. Finally, a graph was plotted to illustrate how the problematic gaming and well-being relationship relates to country prevalence rates of (problematic) gaming.
Ethics
This study was done in accordance with the Declaration of Helsinki. As per the HBSC protocol (Inchley et al., 2018), all participants were informed about the study and parental consent was obtained.
Results
Descriptive statistics
Sample descriptives
Table 1 shows descriptive statistics for the analyzed sample. As expected, the sample of gamers in each country consisted of more boys than girls (54.2%–62.3%). The mean age was similar across countries, ranging from 13.31 to 13.85. Differences in social and mental well-being per country were analyzed using an ANOVA, which is described in Appendix A. For gaming intensity, the average hours spent gaming per week ranged from 6.71 h in Azerbaijan to 13.90 in England.
Correlations
Table 2 shows the bivariate correlations between all variables of interest. Problematic gaming and gaming intensity were moderately positively correlated (r = 0.27). Problematic gaming was associated with lower life satisfaction (r = −0.11), more psychological complaints (r = 0.12), and less peer support (r = −0.13). Similarly, gaming intensity was associated with lower life satisfaction (r = −0.10), more psychological complaints (r = 0.10) and less peer support (r = −0.08), although the correlations were slightly weaker.
Table 2.
Correlations between all study variables
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | |
| 1. Problematic gaming | |||||||
| 2. Life satisfaction | −0.11* | ||||||
| 3. Psychological complaints | 0.12* | −0.40* | |||||
| 4. Peer support | −0.13* | 0.15* | −0.13* | ||||
| 5. Gaming intensity | 0.27* | −0.10* | 0.10* | −0.08* | |||
| 6. Age | 0.03 | −0.19* | 0.14* | −0.03 | 0.08* | ||
| 7. Gender | 0.13* | 0.06* | −0.13* | −0.11* | 0.31* | 0.09* | |
| 8. Family SES | 0.03 | 0.12* | −0.02 | 0.03 | 0.01 | −0.00 | 0.02 |
Note. The effect is significant at *p < 0.001 (two-tailed).
Cross-national differences in problematic gaming
When applying the cut-off point of five or more symptoms, as indicated by the DSM-5 definition (Lemmens et al., 2015), problematic gaming was most prevalent among adolescents in Azerbaijan (16.1%), followed by England (12.3%), Serbia (8.7%), Slovenia (6.7%), and the Netherlands (4.3%). The ANOVA was statistically significant for problematic gaming symptoms, F (4, 13,662) = 187,50, p < 0.001, η2 = 0.05, implying differences in problematic gaming between countries. Differences between countries are shown in Table 3 and indicated with superscript. If two or more countries share a common superscript that means that these countries do not significantly differ from one another. Countries with a different superscript differ from each other.
Table 3.
Problematic gaming scores per country
| Nether-lands | Slovenia | Serbia | England | Azerbaijan | |
| % prob. gaming1 | 4.3% | 6.7% | 8.7% | 12.3% | 16.1% |
| Number symptoms2 | 1.23a | 1.43a | 1.74b | 2.09c | 2.71d |
Note. 1 Prevalence of problematic gaming. 2 Average number of reported symptoms of IGD. a-d Differences between countries were tested using Tukey's post-hoc. Different superscripts indicate significant differences between countries.
The relationship between problematic gaming and well-being: overall and country-level effects
Table 4 presents the overall results and the country-level differences in the relationship between problematic gaming and the three social and mental well-being factors. Age was a significant predictor of both life satisfaction (ß = −0.19, SD = 0.01, p < 0.001) and psychological complaints (β = 0.16, SD = 0.01, p < 0.001). Gender was a significant predictor of all three well-being indicators (β = 0.13, SD = 0.01, p < 0.001; B = −0.21, SD = 0.02, p < 0.001; β = −0.08, SD = 0.03, p < 0.001). Family SES was a significant predictor of life satisfaction (β = 0.12, SD = 0.02, p < 0.001) and peer support (β = 0.03, SD = 0.03, p < 0.001). Finally, gaming intensity was a significant predictor of both life satisfaction (β = −0.05, SD = 0.00, p < 0.001) and psychological complaints (β = 0.04, SD = 0.01, p < 0.001). These findings suggest that older adolescents, girls, adolescents with a lower SES, and intensive gamers report a lower level of well-being.
Table 4.
Relationships between problematic gaming and mental and social well-being
| Life satisfaction | Psychological complaints | Peer Support | |
| β (SD) | β (SD) | β (SD) | |
| Age | −0.19 (0.01)* | 0.16 (0.01)* | −0.02 (0.01) |
| Gender | 0.13 (0.01)* | −0.21 (0.02)* | −0.08 (0.03)* |
| SES | 0.12 (0.02)* | −0.01 (0.01) | 0.03 (0.03)* |
| Gaming intensity | −0.05 (0.00)* | 0.04 (0.00)* | 0.02 (0.00) |
| Problematic gaming | −0.15 (0.01)* | 0.19 (0.00)* | −0.16 (0.01)* |
| Netherlands | −0.18 (0.02)* | 0.26 (0.01)* | −0.14 (0.02)* |
| Slovenia | −0.19 (0.02)* | 0.23 (0.01)* | −0.13 (0.02)* |
| Serbia | −0.18 (0.02)* | 0.25 (0.01)* | −0.14 (0.02)* |
| England | −0.18 (0.02)* | 0.26 (0.01)* | −0.07 (0.02) |
| Azerbaijan | −0.10 (0.02)* | 0.12 (0.01)* | −0.13 (0.02)* |
Note. The effect is significant at *p < 0.001 (two-tailed). All analyses controlled for age, gender, family SES, and gaming intensity.
The significant main effect of problematic gaming on mental and social well-being in the entire sample (including all five countries) indicated that higher scores on problematic gaming are associated with decreased life satisfaction, more psychological complaints, and less peer support. After controlling for age, gender, SES, and gaming intensity, the independent variable problematic gaming explained 8% of the variance in life satisfaction (R2 = 0.08, R2change = 0.02, p < 0.000), 8% in psychological complaints (R2 = 0.08, R2change = 0.02, p < 0.000) and 4% in peer support (R2 = 0.04, R2change = 0.02, p < 0.001).
Country data analysis showed associations between problematic gaming and mental and social well-being in all countries (except for peer support in England).
Additional analyses
Although the associations were weak, the regression analyses in the total sample showed that gaming intensity was significantly related to two well-being indicators, life satisfaction and psychological complaints. Because these weak associations may also turn out to be significant because of the large sample size (N = 14,398), it is also important to test the relationships between gaming intensity and the well-being factors per country (see Appendix B). The results showed no significant relationship between gaming intensity and social and mental well-being, except for life satisfaction in Azerbaijan (β = −0.09, SD = 0.01, p < 0 .001).
Normalization theory
Finally, the normalization hypothesis was tested in the last step of the regression analysis. Three separate interaction effects were tested, i.e., interaction effects between problematic gaming and the country-prevalence of gaming on all three well-being indicators. Only one significant interaction term was found, which was inconsistent with the proposed hypothesis. Contrary to the normalization hypothesis, the strength of the relationship between problematic gaming and psychological complaints increased with higher country-prevalence rates of gaming (β = 0.05, p < 0.001). No interaction effects were found for life satisfaction or peer support.
To illustrate these findings, the effect sizes for the relationship between problematic gaming and the three well-being indicators were plotted against the prevalence of gamers in each country (see Fig. 1). If the normalization theory were applied to gaming, effect sizes would be expected to decrease with increasing countries' prevalence rates of gamers. The graph illustrates that this normalization pattern is not visible for any of the three mental and social well-being indicators.
Fig. 1.
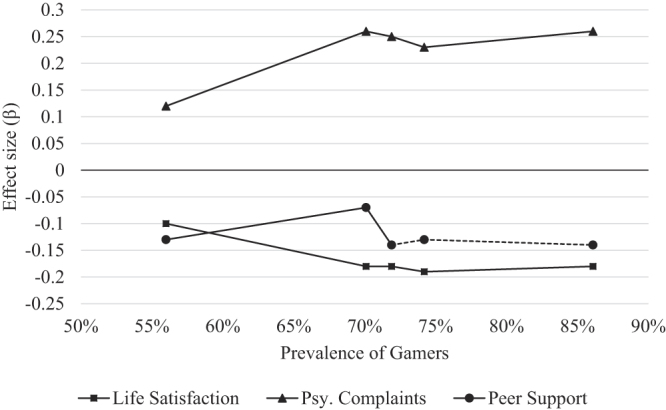
Relations Between Problematic Gaming and Mental and Social Well-being per Country's Gamer Prevalence. Note. Peer support in England (86%, indicated by the dotted line) was not significant
Discussion
There are several studies (Männiko et al., 2020) that highlighted the negative mental health outcomes of problematic gaming behavior. The present study added to the conception of problematic gaming behavior and its relationship with social and mental well-being in a cross-national sample of adolescents from five European countries that engaged in the 2017/2018 Health Behavior in School-aged Children (HBSC) study. The current findings are consistent with the results of previous studies that confirmed the significant associations between problem gaming behavior and psychosocial problems such as low life satisfaction, psychological complaints, and lack of peer support (Cheng et al., 2018; Dullur et al., 2020; Gentile et al., 2011; Männiko et al., 2020; Van Den Eijnden et al., 2018). Although some country-differences in the strength of these relationships are observed, negative associations between adolescents' problematic gaming and their social and mental well-being are seen in all five countries (except for peer support in England). Interestingly, additional analyses indicated no relationships between gaming intensity (i.e., time spent playing games) and social and mental well-being (except for life satisfaction in Azerbaijan). The findings of the current study substantiate previous studies suggesting that the amount of time adolescents spend on gaming does not necessarily relate to lower well-being in adolescents (Brunborg et al., 2013, 2014; Király, Sleczka, et al., 2017; Spekman et al., 2013; Van Den Eijnden et al., 2018). Thus, the distinction between time spent gaming and symptoms of problematic gaming is crucial for the conceptualization of problematic gaming, as well as to prevent heavy gamers to be labeled and treated as problematic gamers.
While most countries showed comparable results, Azerbaijan was one notable outlier in almost all analyses, showing weaker relationships between problematic gaming, life satisfaction, and psychological complaints compared to the other countries. At the country level, Azerbaijan had the lowest gaming intensity but the highest score on problematic gaming symptoms. One possible explanation for these findings may be that the relatively limited gaming opportunities in Azerbaijan (the prevalence of gaming and the time adolescents spent playing games were the lowest in Azerbaijan), compared to the other countries, may have elicited certain symptoms of problematic gaming. Feeling the desire or the urge to play games but not being able to do so may stimulate problematic thoughts (e.g., preoccupation with gaming) as well as conflicts with parents and siblings who also may want to use the available device(s) in the household. This is in line with previous research findings suggesting that extreme internet restrictions imposed by parents seem to stimulate symptoms of problematic internet use among adolescents (van Den Eijnden, Spijkerman, Vermulst, van Rooij, & Engels, 2010). Another explanation may be that adolescents in Azerbaijan may have overreported their gaming problems due to beginner's fascination, as gaming is less mainstream in Azerbaijan than in the other countries. Because of this, gamers in Azerbaijan, more than gamers from other countries, may also regard having gaming problems as cool. They may see problematic gaming as a badge of pride. However, empirical research would be required to verify these possible explanations.
Furthermore, the current study aimed to take account of the cultural context of gaming problems by exploring the results in light of the normalization theory, which proposed that risk behaviors that become more mainstream or ‘normalized’ tend to generate fewer negative consequences due to higher social acceptance of the behavior (Boer et al., 2020; Haskuka et al., 2018). The current study findings show no visible pattern suggesting that the relationship between problematic gaming and mental or social well-being is weaker in countries with higher prevalence rates of gamers. Thus, the current study does not support the normalization theory for problematic gaming behavior and suggests that the association between problematic gaming and adolescents' well-being does not necessarily depend on the country context. These findings seem to imply that problematic gaming negatively affects adolescents' well-being in all instances, regardless of country norms about gaming behavior. This finding is in line with a previous study that found no support for the normalization theory when it comes to problematic social media use (Boer et al., 2020), but that did find support for the normalization theory with regard to intensive social media use, which is much more normative behavior than problematic use. Future studies should investigate the specific conditions under which the normalization theory is applicable.
Strengths and limitations
The primary strength of this study was the large sample of young people and the similar set-up of the HBSC study across countries, allowing for cross-cultural comparisons of problematic gaming behavior and the well-being of young people in different European countries without the methodological inconsistencies of previous studies.
However, this study also had several limitations that we would like to address. First, the data were obtained using self-report questionnaires. Therefore, various biases might have affected responses to the problematic gaming measure (both over- and underreporting of gaming problems), and these biases may have differed between countries. Second, we cannot rule out that contextual factors, such as the country's availability of game options, may have affected the number of problematic gaming symptoms. Third, the study's cross-sectional design does not allow for causal inferences. The current study incorporated social and mental well-being as outcomes; however, poor social and mental well-being may also lead to more problematic gaming. For example, previous studies have found that adolescents who struggle with peer problems may use gaming as a substitute for social contact, leading to more problematic gaming (Peeters, Koning, & van den Eijnden, 2018). Additional longitudinal studies are required to better understand the direction of these associations.
Finally, the limited number of countries included in the study prevented us from performing multi-level analyses. Future studies should include more countries to conduct cross-national comparisons with better statistical methodologies.
Practical implications
The current study emphasizes the potential harm of problematic gaming, as problematic gaming was negatively associated with almost all well-being domains across all countries. Time spent gaming, on the other hand, was hardly related to adolescents' well-being. The present findings underline that time spent gaming and problematic gaming are very different concepts, that should be considered separately when investigating the relationship between gaming behavior and adolescents' well-being, but also when screening for problematic gamers. We believe it is time to shift the focus of current scholarly discussions on the definition of (Internet) Gaming Disorder to researching intervention efforts that may prevent problematic gaming and its negative consequences for the healthy upbringing of young people.
Conclusion
Despite cross-cultural differences in the prevalence of problematic gaming, gaming intensity, and well-being, the current study revealed a clear and consistent association between problematic gaming and adolescents' well-being. Moreover, the intensity of gaming was not associated with mental or social well-being, further confirming earlier research that indicates that more time spent gaming does not necessarily translate to problematic gaming (Brunborg et al., 2013, 2014; Király, Sleczka, et al., 2017; Spekman et al., 2013; Van Den Eijnden et al., 2018). In addition, the current study found no evidence to support that the normalization theory (Boer et al., 2020; Haskuka et al., 2018) applies to problematic gaming. Thus, the negative consequences of problematic gaming do not seem to diminish or disappear when gaming becomes more normative in the national context. Finally, future studies should identify why individuals in certain countries score higher on problematic gaming than individuals in other countries and which contextual risk factors are associated with these increased scores. The findings of this study contribute to the conceptualization of problematic gaming and highlight the need for adequate prevention strategies.
Funding sources
This study did not receive any financial support.
Authors’ contribution
DvdN was responsible for writing and editing the manuscript and performing statistical analyses. RvdE and MP contributed by supervising, reviewing and writing, and conceptualizing analyzing strategies. MBN, HJK, and LO contributed by reviewing and writing the discussion. All authors read and approved the final version of the paper.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
Health Behaviour in School-aged Children (HBSC) is an international study carried out in collaboration with WHO/EURO. The International Coordinator was Jo Inchley (University of Glasgow) for the 2017/2018 survey. The Data Bank Manager was Oddrun Samdal (University of Bergen). The 2017/2018 survey included in this study were conducted by the following principal investigators in 5 countries: Azerbaijan (Gahraman Hagverdiyev), England (Fiona Broks, Ellen Klemera), the Netherlands (Gonneke Stevens and Saskia van Dorsselaer), Serbia (Jelena Rakic), and Slovenia (Helena Jericek).
APPENDICES
Appendix A: Cross-national differences in mental and social well-being
Life satisfaction
England had the lowest (M = 7.51, SD = 1.78) and Azerbaijan had the highest average score on life satisfaction (M = 8.30, SD = 2.00). The ANOVA was statistically significant, F (4, 14,312) = 86.07, p < 0.001, η2 = 0.02. The Tukey post-hoc revealed that adolescents in Azerbaijan and Serbia reported the highest level of life satisfaction, followed by Slovenia, Serbia, the Netherlands, and England.
Psychological complaints
The results indicated that adolescents in England scored the highest (M = 2.45, SD = 1.05), and those in Azerbaijan scored the lowest on psychological complaints (M = 1.74, SD = 1.00). The ANOVA was statistically significant, F (4, 14,246) = 157.79, p < 0.001, η2 = 0.04. The post-hoc test showed that psychological complaints were the highest in England, followed by the Netherlands, Serbia, Slovenia, and Azerbaijan.
Peer support
Lastly, peer support was the highest in the Netherlands (M = 5.70, SD = 1.33) and lowest in England (M = 4.49, SD = 2.12). The ANOVA was statistically significant, F (4, 14,259) = 167.96, p < 0.001, η2 = 0.05. The post-hoc revealed that peer support was the highest in the Netherlands, followed by Serbia, Slovenia, and Azerbaijan.
Appendix B: Additional analyses on gaming intensity and mental and social well-being
Table B1.
Relationships of game intensity with mental and social well-being per country
| Life satisfaction | Psychological complaints | Peer Support | |
| β (SD) | |||
| Intensity | |||
| Netherlands | 0.03 (0.00) | 0.02 (0.00) | −0.04 (0.00) |
| Slovenia | 0.02 (0.00) | 0.01 (0.00) | −0.02 (0.00) |
| Serbia | 0.00 (0.00) | 0.00 (0.00) | −0.04 (0.00) |
| England | −0.08 (0.00) | 0.04 (0.00) | 0.04 (0.00) |
| Azerbaijan | −0.09 (0.02)* | 0.03 (0.00) | −0.01 (0.01) |
Note. The effect was significant at *p < 0.001 (two-tailed). All analyses controlled for age, gender, family SES, and problematic gaming.
References
- Boer, M., Van Den Eijnden, R. J., Boniel-Nissim, M., Wong, S. L., Inchley, J. C., Badura, P., … Stevens, G. W. (2020). Adolescents' intense and problematic social media use and well-being in 29 countries. Journal of Adolescent Health, 66(6), S89–S99. 10.1016/j.jadohealth.2020.02.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brunborg, G. S., Mentzoni, R. A., & Frøyland, L. R. (2014). Is video gaming, or Video Game addiction, associated with depression, academic achievement, heavy episodic drinking, or conduct problems? Journal of Behavioral Addictions, 3(1), 27–32. 10.1556/jba.3.2014.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brunborg, G. S., Mentzoni, R. A., Melkevik, O. R., Torsheim, T., Samdal, O., Hetland, J., … Palleson, S. (2013). Gaming addiction, gaming engagement, and psychological health complaints among Norwegian adolescents. Media Psychology, 16(1), 115–128. 10.1080/15213269.2012.756374. [DOI] [Google Scholar]
- Bryan, M. L., & Jenkins, S. P. (2016). Multilevel modelling of country effects: A cautionary tale. European Sociological Review, 32(1), 3–22. 10.1093/esr/jcv059. [DOI] [Google Scholar]
- Cantril, H. (1965). The pattern of human concerns. Rutgers University Press. [Google Scholar]
- Cheng, C., Cheung, M. W. L., & Wang, H. Y. (2018). Multinational comparison of internet gaming disorder and psychosocial problems versus well-being: Meta-analysis of 20 countries. Computers in Human Behavior, 88, 153–167. 10.1016/j.chb.2018.06.033. [DOI] [Google Scholar]
- Colasante, E., Pivetta, E., Canale, N., Vieno, A., Marino, C., Lenzi, M., … Molinaro, S. (2022). Problematic gaming risk among European adolescents: A cross‐national evaluation of individual and socio‐economic factors. Addiction, 117(8), 2273–2282. 10.1111/add.15843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Den Eijnden, R. J., Spijkerman, R., Vermulst, A. A., van Rooij, T. J., & Engels, R. C. (2010). Compulsive Internet use among adolescents: Bidirectional parent–child relationships. Journal of Abnormal Child Psychology, 38(1), 77–89. 10.1007/s10802-009-9347-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dullur, P., Krishnan, V., & Diaz, A. M. (2020). A systematic review on the intersection of attention-deficit hyperactivity disorder and gaming disorder. Journal of Psychiatric Research, 133, 212–222. 10.1016/j.jpsychires.2020.12.026. [DOI] [PubMed] [Google Scholar]
- ESA (2020). 2020 essential facts about the video game industry. https://www.theesa.com/esa-research/2020-essential-facts-about-the-video-game-industry/. [Google Scholar]
- Gentile, D., Choo, H., Liau, A., Sim, T., Li, D., Fung, D., & Khoo, A. (2011). Pathological video game use among youths: A two-year longitudinal study. Pediatrics, 127(2), e319–e329. 10.1542/peds.2010-1353. [DOI] [PubMed] [Google Scholar]
- Haskuka, M., Arenliu, A., & Kelmendi, K. (2018). The relationship between substance use and suicidal behaviour among adolescents in selected European countries: A test of normalisation theory. Drugs: Education, Prevention and Policy, 25(5), 413–421. 10.1080/09687637.2017.1308468. [DOI] [Google Scholar]
- Heinz, A., Sischka, P. E., Catunda, C., Cosma, A., García-Moya, I., Lyyra, N., … Pickett, W. (2022). Item response theory and differential test functioning analysis of the HBSC-Symptom-Checklist across 46 countries. BMC Medical Research Methodology, 22(1), 1–24. 10.1186/s12874-022-01698-3. 36175865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hox, J. J. (2010). Multilevel analysis: Techniques and applications (2nd ed.) Routledge. [Google Scholar]
- Inchley, J., Currie, D., Cosma, A., & Samdal, O. (2018). Health Behaviour in School-aged Children (HBSC) study protocol: Background, methodology and mandatory items for the 2017/18 survey. St Andrews: CAHRU. [Google Scholar]
- ISFE (2020). Key facts 2020. https://www.isfe.eu/isfe-key-facts/. [Google Scholar]
- Király, O., Sleczka, P., Pontes, H. M., Urbán, R., Griffiths, M. D., & Demetrovics, Z. (2017). Validation of the ten-item internet gaming disorder test (IGDT-10) and evaluation of the nine DSM-5 internet gaming disorder criteria. Addictive Behaviors, 64, 253–260. 10.1016/j.addbeh.2015.11.005. [DOI] [PubMed] [Google Scholar]
- Lemmens, J. S., Valkenburg, P. M., & Gentile, D. A. (2015). The Internet gaming disorder scale. Psychological Assessment, 27(2), 567. 10.1037/pas0000062. [DOI] [PubMed] [Google Scholar]
- Levin, K. A., & Currie, C. (2014). Reliability and validity of an adapted version of the Cantril Ladder for use with adolescent samples. Social Indicators Research, 119(2), 1047–1063. 10.1007/s11205-013-0507-4. [DOI] [Google Scholar]
- Männikkö, N., Billieux, J., & Kääriäinen, M. (2015). Problematic digital gaming behavior and its relation to the psychological, social and physical health of Finnish adolescents and young adults. Journal of Behavioral Addictions, 4(4), 281–288. 10.1556/2006.4.2015.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Männikkö, N., Ruotsalainen, H., Miettunen, J., Pontes, H. M., & Kääriäinen, M. (2020). Problematic gaming behaviour and health-related outcomes: A systematic review and meta-analysis. Journal of Health Psychology, 25(1), 67–81. 10.1177/1359105317740414. [DOI] [PubMed] [Google Scholar]
- Mihara, S., & Higuchi, S. (2017). Cross‐sectional and longitudinal epidemiological studies of internet gaming disorder: A systematic review of the literature. Psychiatry and Clinical Neurosciences, 71(7), 425–444. 10.1111/pcn.12532. [DOI] [PubMed] [Google Scholar]
- Peeters, M., Koning, I., & van den Eijnden, R. (2018). Predicting internet gaming disorder symptoms in young adolescents: A one-year follow-up study. Computers in Human Behavior, 80, 255–261. 10.1016/j.chb.2017.11.008. [DOI] [Google Scholar]
- Pontes, H. M., & Griffiths, M. D. (2015). Measuring DSM-5 Internet gaming disorder: Development and validation of a short psychometric scale. Computers in Human Behavior, 45, 137–143. 10.1016/j.chb.2014.12.006. [DOI] [Google Scholar]
- Pontes, H. M., Király, O., Demetrovics, Z., & Griffiths, M. D. (2014). The conceptualisation and measurement of DSM-5 internet gaming disorder: The development of the IGD-20 test. Plos One, 9(10), e110137. 10.1371/journal.pone.0110137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pontes, H. M., Schivinski, B., Sindermann, C., Li, M., Becker, B., Zhou, M., & Montag, C. (2021). Measurement and conceptualization of gaming disorder according to the World health organization framework: The development of the gaming disorder test. International Journal of Mental Health and Addiction, 19(2), 508–528. 10.1007/s11469-019-00088-z. [DOI] [Google Scholar]
- Quon, E. C., & McGrath, J. J. (2014). Subjective socioeconomic status and adolescent health: A meta-analysis. Health Psychology, 33(5), 433. 10.1037/a0033716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Şalvarlı, Ş. İ., & Griffiths, M. D. (2019). The association between internet gaming disorder and impulsivity: A systematic review of literature. International Journal of Mental Health and Addiction, 1–27. 10.1007/s11469-019-00126-w. [DOI] [Google Scholar]
- Spekman, M. L., Konijn, E. A., Roelofsma, P. H., & Griffiths, M. D. (2013). Gaming addiction, definition and measurement: A large-scale empirical study. Computers in Human Behavior, 29(6), 2150–2155. 10.1016/j.chb.2013.05.015. [DOI] [Google Scholar]
- Stevens, M. W., Dorstyn, D., Delfabbro, P. H., & King, D. L. (2021). Global prevalence of gaming disorder: A systematic review and meta-analysis. The Australian and New Zealand Journal of Psychiatry, 55(6), 553-568. 10.1177/000486742096285. [DOI] [PubMed] [Google Scholar]
- Van Den Eijnden, R., Koning, I., Doornwaard, S., Van Gurp, F., & Ter Bogt, T. (2018). The impact of heavy and disordered use of games and social media on adolescents’ psychological, social, and school functioning. Journal of Behavioral Addictions, 7(3), 697–706. 10.1556/2006.7.2018.65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zimet, G. D., Dahlem, N. W., Zimet, S. G., & Farley, G. K. (1988). The multidimensional scale of perceived social support. Journal of Personality Assessment, 52(1), 30–41. 10.1207/s15327752jpa5201_2. [DOI] [PubMed] [Google Scholar]